
Abstract
Background
Automated breast ultrasound (ABUS) is one of the first ultrasound devices which enables the de-coupling of image acquisition and interpretation. Another feature of ABUS is the coronal view, utilizing three-dimensional volume data reconstructed from two-dimensional transverse images acquired automatically.
Purpose
To assess the diagnostic performance of coronal view interpretation by comparing it with that of the transverse view.
Material and Methods
This was a retrospective, multi-case, observer study using a cancer-enriched dataset of ABUS images at a single institution with approval by an Institutional Review Board. The 100 scan datasets selected between October 2014 and January 2017 included 70 non-cancer cases and 30 malignancies. In the present observer study, two experienced physicians provided their confidence levels regarding the malignancy of each of the 100 scan datasets independently. The reading times for interpretation of coronal and transverse views were recorded.
Results
Area under the receiver operating characteristic curves for two observers with the transverse view (0.856) was improved by use of the coronal view (0.917, P = 0.036). The average reading times were 140.4 s with the coronal view and 148.5 s with the transverse view per scan dataset (P = 0.246).
Conclusion
It is conceivable that the accurate use of the coronal view will lead to improvement in diagnostic performance in breast cancer screening, although this needs to be confirmed with a larger prospective study.
Introduction
Conventional handheld ultrasound (HHUS) is limited by operator dependence and image reproducibility. In addition, HHUS requires simultaneous image acquisition and interpretation leading to psychophysical disturbance (1). The three-dimensional (3D) automated breast ultrasound system (ABUS), in comparison, is one of the first ultrasound devices which enables de-coupling of image acquisition and interpretation, similar to nearly all other conventional imaging modalities, such as X-ray, computed tomography (CT), and magnetic resonance imaging (MRI) (2,3). This technology allows the operators to concentrate on image acquisition, thereby reducing their burden. ABUS has made it possible to record reproducible whole breast data that are not affected by the skill of the operators, and the readers can access the data at any time, not just during the examination. Thus, ABUS offers a clear advantage over HHUS, potentially leading to improvement in the accuracy and efficiency of breast cancer screening.
In virtue of the recent rapid development of application software and other related technologies, automated scanning and management of the whole breast volume data have become faster and less costly. Another feature of 3D ABUS is the coronal view utilizing the 3D volume data reconstructed from the two-dimensional (2D) transverse images acquired automatically (4).
Our experience since installation of ABUS in 2014 led us to further explore the diagnostic performance of the coronal view and inspired us to pursue an independent evaluation of coronal view reading compared with transverse view reading. There have been no reports to date regarding the independent value of coronal view image interpretation. The aim of the present study was to assess the value of non-conventional coronal view image interpretation compared with image interpretation of the conventional transverse view.
Material and Methods
The present study was a retrospective, multi-case, observer study using a cancer-enriched dataset of ABUS images at a single institution after approval by an Institutional Review Board (IRB). Informed consent was waived by the IRB on the premise that the datasets were anonymized.
Material
The present study utilized 100 scan datasets selected from ABUS data at this institution between October 2014 and January 2017. The cases were independently and blindly selected by one of the authors (radiologic technologist) who did not take part in the interpretations. The 100 scan datasets included 70 non-cancer cases and 30 biopsy-proven malignancies. Cases were excluded if they were obtained from individuals who were noted to be extremely thin, for whom the use of ABUS was difficult, had mass lesions of ≥3 cm, and/or had undergone previous breast biopsy or surgery.
Scan datasets included 33/100 (33%) normal cases, 37/100 (37%) benign cases, and 30/100 (30%) malignant cases. Ultrasound-guided vacuum assisted needle biopsy (VAB; EnCore™, 10G, Bard, Murray Hill, NJ, USA) had been carried out in 46 of the selected cases, of which 1/46 (2.2%) were normal, 15/46 (32.6%) were benign, and 30/46 (65.2%) were malignant. The benign group consisted of 15 VAB-proven cases and 22 non-VAB cases that had been monitored for >1 year without any change.
Image acquisition
A radiologic technologist performed examinations using an Invenia™ ABUS (GE Healthcare, Sunnyvale, CA, USA). Each breast was imaged with an automated 15.3 cm 6–15-MHz linear-array transducer. Although three scans for one breast are recommended (anteroposterior [AP], lateral, and medial), smaller breasts were imaged with two scans per breast. Additional scans were taken as necessary to cover all breast tissues completely.
Image interpretation
Two physicians with 8 and 40 years of experience, respectively, in breast imaging participated in the observer study. Their experience with ABUS was six months and two years, respectively. Each of the observers had completed the Invenia™ ABUS Mastery Program (Physician’s Training) before participating in the present study. Images of the coronal view and transverse view were anonymized and presented to the observers in random order. Each observer interpreted 100 scan datasets (100 coronal view images and 100 transverse view images) independently without any personal information. The coronal images and transverse images were interpreted on different days, so that data from the same patient were not interpreted in both views on the same day. Observers were blinded to known pathology and to results of any previously interpreted view (coronal or transverse).
A “coronal comparison” panel was displayed for coronal view reading (Fig. 1), and a “T-C comparison” panel for transverse view reading (Fig. 2). The coronal views of the “T-C comparison” panel were fixed at the skin level to avoid mixed reading. The observer was asked to mark his or her confidence level regarding the malignancy of the case on a continuous rating scale from 0 to 1 corresponding to “definitely benign” and “definitely malignant,” respectively.
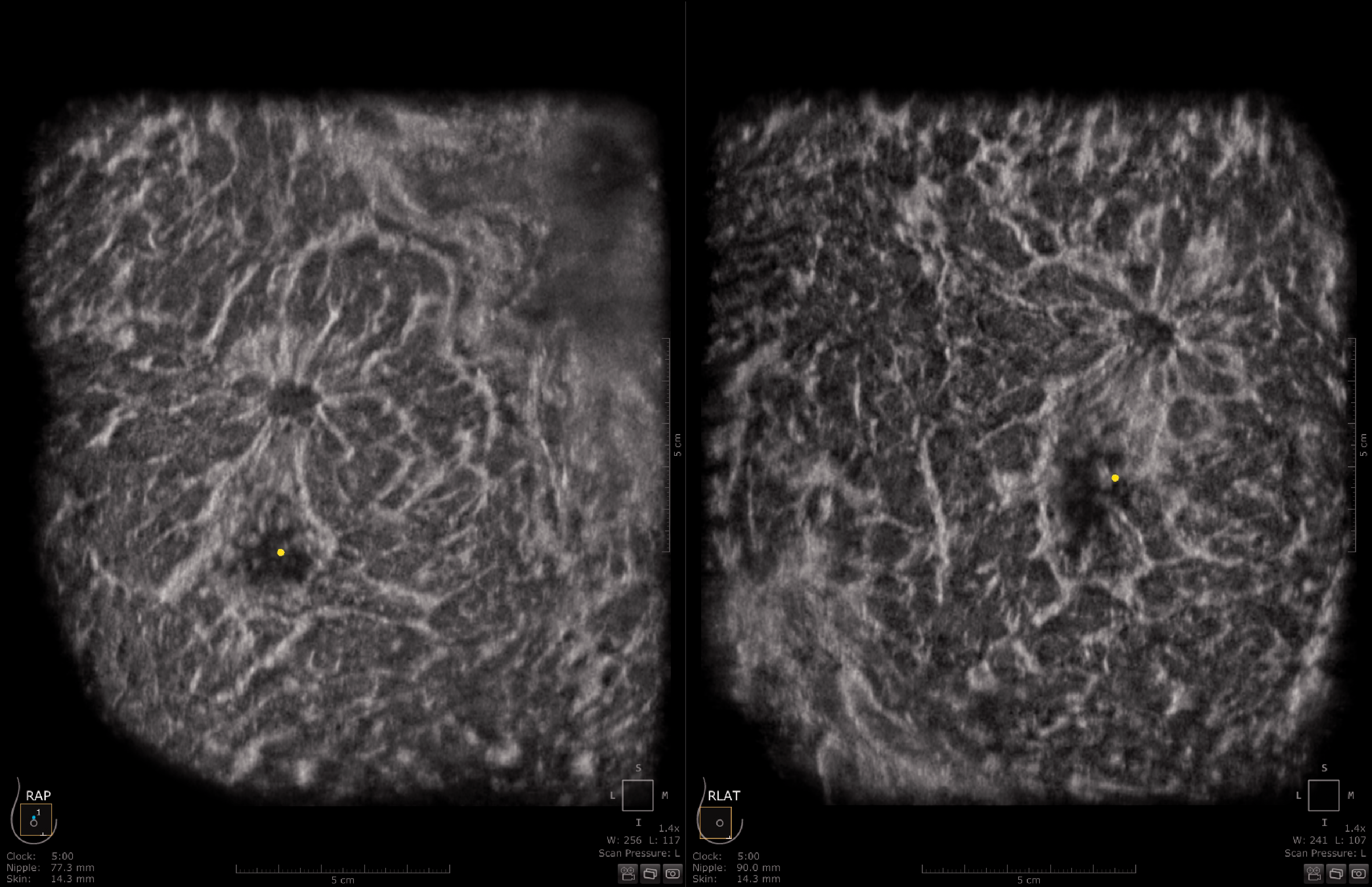
“Coronal comparison” panel showing the right breast (right: lateral; left: anteroposterior). The yellow dots indicate the positions of the nipple.

“T-C comparison” panel showing the right breast (left: coronal view; right: transverse view; top: anteroposterior; bottom: lateral). The yellow dots indicate the positions of the nipple.
The reading time was recorded, and the total amount of reading time per day was limited to 1 h in order to avoid the influence of fatigue.
Statistical analysis
Receiver operating characteristic (ROC) analysis using the method for continuously distributed test results was performed to compare the diagnostic accuracy between coronal view and transverse view. The areas under the ROC curve (AUC) and the 95% confidence intervals (CI) were obtained with a quasi-maximum-likelihood estimation of binormal distribution by use of DBM MRMC software developed by the University of Iowa and the University of Chicago (17,18). The average reading time of each dataset was analyzed for the coronal and transverse views, and the results were compared using the paired t-test. A P value < 0.05 was considered to indicate a significant difference.
Results
Characteristics
A total of 100 breast volume scan datasets for 69 female patients was selected (mean age = 53.2 years; age range = 24–81 years). The mean number of scans per breast was 2.35. Patient age, number of scans, and type of examination for malignant and benign/normal lesions were not significantly different (Table 1).
Description of the study sample
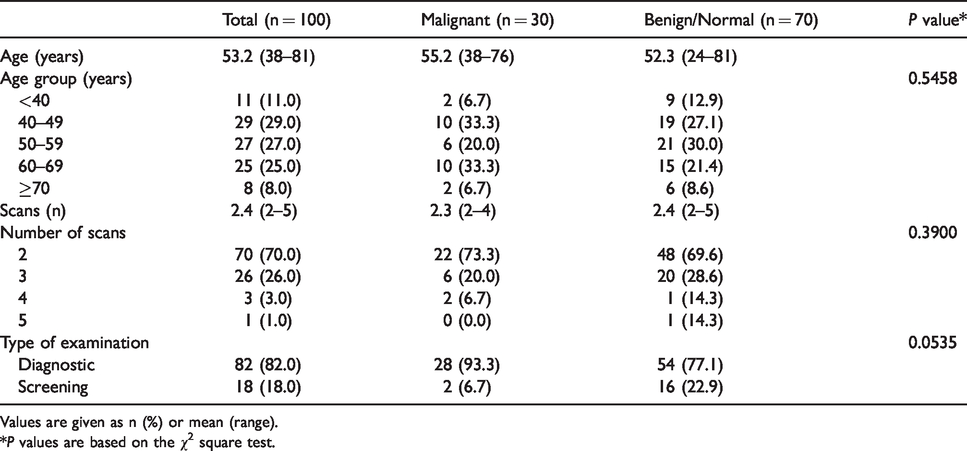
Values are given as n (%) or mean (range).
*P values are based on the χ2 square test.
The number of mass/non-mass lesions and size of mass for malignant and benign lesions were not significantly different (Tables 2 and 3).
The number of mass and non-mass lesions.
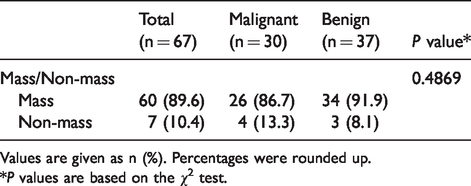
Values are given as n (%). Percentages were rounded up.
*P values are based on the χ2 test.
The size of the mass.
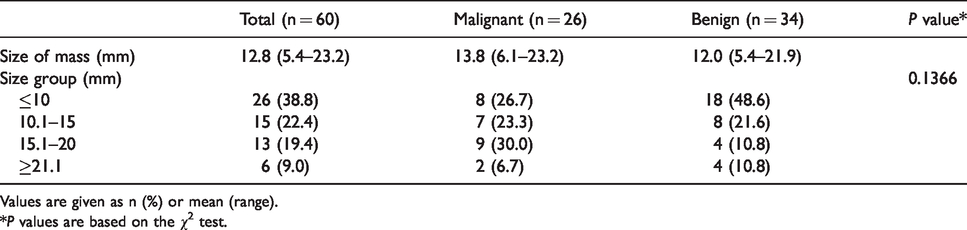
Values are given as n (%) or mean (range).
*P values are based on the χ2 test.
Diagnostic performance
AUC values for coronal view and transverse view respectively were: Reader A = 0.912 and 0.846 (P = 0.137); and Reader B = 0.922 and 0.866 (P = 0.170). The average AUC for two readers for the coronal view (0.917) was significantly greater than that for the transverse view (0.856, P = 0.036) (Fig. 3). The reading time for the coronal view and transverse view respectively were: Reader A = 118.8 s and 123.6 s; and Reader B = 162.0 s and 173.4 s per scan dataset. The average reading time for the coronal view and the transverse view was 140.4 s and 148.5 s, respectively, per scan dataset (P = 0.246). Although the coronal view tended to be superior with respect to shorter reading time, no statistical differences were observed.
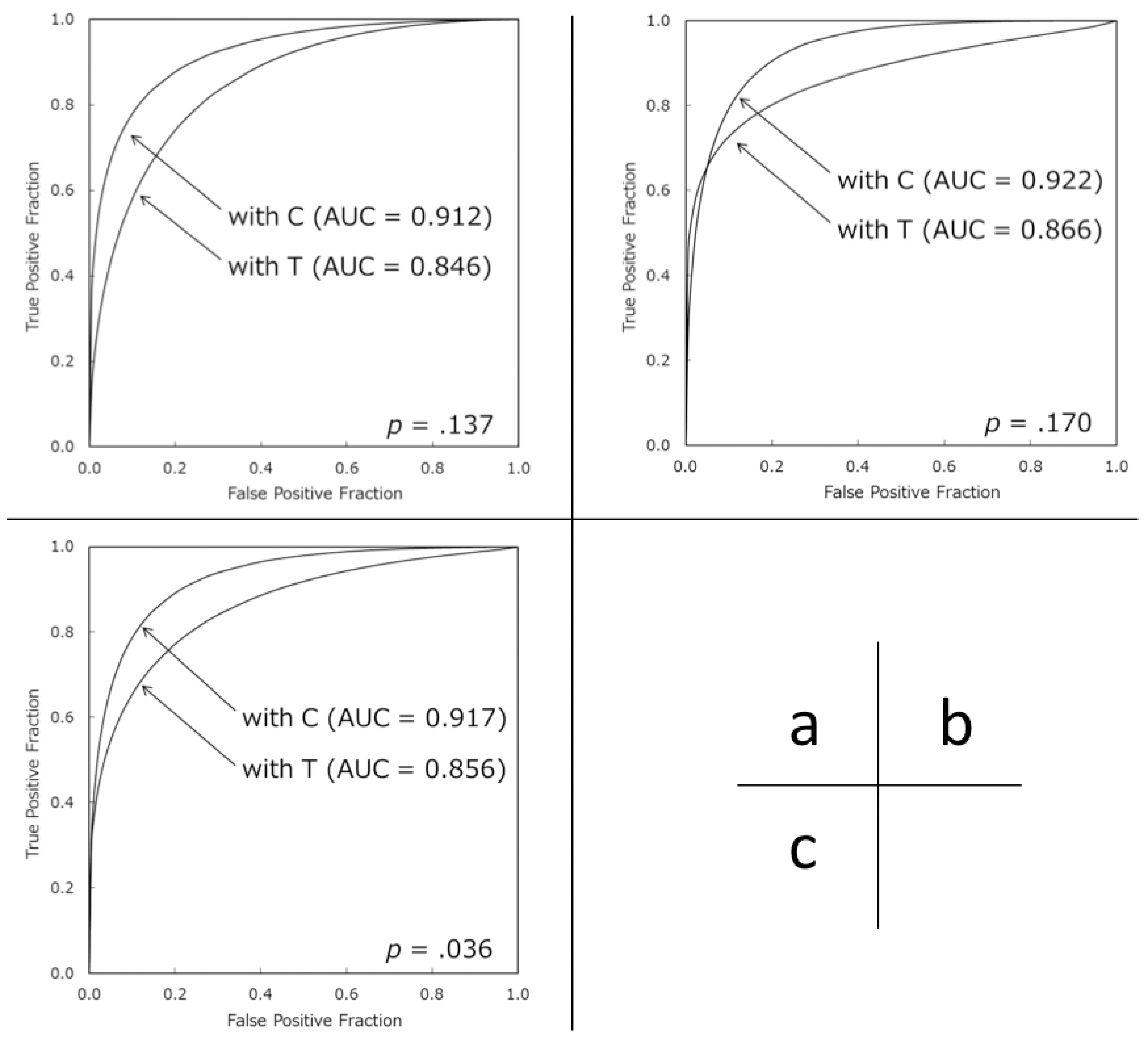
Comparison of ROC curves. (a) ROC curves for Reader A; (b) ROC curves for Observer B; (c) Average ROC curves for the two observers. ROC, receiver operating characteristic.
Discussion
Breast ultrasound is most commonly used as an adjunct to screening mammography in women with radiographically dense breasts. HHUS following mammography has proven to produce a significant increase in the detection of small (5,6), node-negative invasive breast cancers, especially in women with dense breasts (6). However, significant challenges exist with HHUS including operator dependence, time associated with obtaining and interpreting images, exam reproducibility, and the significant psychophysical burden on the operator. In contrast to HHUS, 3D ABUS has overcome many of these challenges, and produced, for the first time in the history of ultrasound imaging, complete division of image acquisition and interpretation, as found in nearly all other imaging modalities. Recent clinical studies have demonstrated considerable agreement in the assessment of breast lesions by ABUS and HHUS (3,7,8). Additionally, the use of 3D ABUS combined with mammography has been shown to increase the detection rate (9–12) for early stage invasive breast carcinoma in women with dense breasts (13,14).
Multiple advantages have been reported with the use of ABUS compared to HHUS. For instance, ABUS allows for shorter scanning times (8) as well as operator independence (7). Additionally, with regard to interpretation, Wojcinski et al. (15) described how utilizing ABUS for 3D planning of the surgical procedure helped in better defining the margins for resection. Finally, Lin et al. (7) demonstrated how ABUS had better correlation with pathological maximum diameters of lesions than HHUS.
As described above, our study specifically examined the coronal view, which is unique to ABUS. The coronal view is able to provide additional information for the detection and diagnosis of breast lesions (1,3,7,8,15). In the coronal view, multiple masses and large lesions can be displayed in one view with the location of these lesions accurately visualized. The higher diagnostic performance found with use of the coronal view can be explained by the fact that architectural distortion is clearly visualized (1,3,7). Kalmantis et al. (16) reported the retraction pattern was apparent in 88.7% of malignant cases (sensitivity = 0.89, specificity = 0.96, positive predictive value = 0.96, negative predictive value = 0.92). Architectural distortion is the imaging sign that led to the discovery of the tumor. Even a small mass can be easily detected if the distortion surrounding the lesion is identified, which leads to an increase in diagnostic performance. Lin et al. (7) reported ABUS could display the retraction phenomenon in the coronal view with a high sensitivity and high specificity in detecting breast cancer, and a high accuracy in discriminating malignant from benign lesions.
To evaluate the necessity for experience with ABUS, the same observer study was conducted with a physician possessing only one month of experience with ABUS. The AUC for this reader for the coronal view (0.815) was less than that for the transverse view (0.901, P = 0.068). Therefore, based on this limited evaluation, the experience reading coronal views is necessary to assess lesions accurately.
In terms of the reading time, it is conceivable that the coronal view was faster due to the small number of slices present between the chest wall and the skin, whereas with the transverse view, it was necessary to read slices from the bottom to the top of the breast.
The present study has some limitations. First, this was a retrospective study involving only a single institution and the number of readers was small. The main limitation, however, was that the design had a limited sample size of only 100 selected datasets. Additionally, the proportion of cases was not representative of the whole population. Unlike an actual screening setting, ABUS images were interpreted using either coronal view or transverse view alone. Therefore, the results of diagnostic accuracy cannot be applied to general breast cancer screening and must be carefully interpreted. Although the selection bias had an effect on the ROC results, it would not impact the comparison between the coronal view and the transverse view in the present study. Currently, we are planning a well-designed study involving multiple institutions for the purpose of a more comprehensive evaluation of coronal view.
In conclusion, in the present observer study, the average AUC for experienced observers using the coronal view was significantly greater than that with the transverse view. It is conceivable that the accurate use of the coronal view will lead to improvement in diagnostic performance in breast cancer screening. This should be confirmed with a larger prospective study to verify the trends seen here. We are conducting multi-center research that builds on the research presented here. Furthermore, it is hoped that computer-aided detection and artificial intelligence utilizing breast volume data and coronal view information will improve the early detection of breast cancer.
Footnotes
Acknowledgements
The authors thank the colleagues of Hokuto Hospital and GE Healthcare.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: RLS received consultant fee from QView Medical Inc., Los Altos, CA, USA. The supporting source had no involvement with the study and the author had no access to the study data.