
Abstract
Background
Although the effectiveness of percutaneous radiologic gastrojejunostomy (PRGJ) has been reported, a detailed description of the indications and clinical effectiveness of temporary PRGJ is still limited.
Purpose
To evaluate the clinical effectiveness and technical feasibility of temporary PRGJ using the modified Chiba-needle technique with single gastropexy.
Material and Methods
Temporary PRGJ using the modified Chiba-needle technique with single gastropexy was performed in 27 consecutive patients (19 men, 8 women; mean age = 61 years; age range = 32–77 years) for esophageal perforation (n = 18) or postoperative gastroparesis (n = 9). Outcomes analyzed included the technical and clinical success, procedure-related complications, and the tube indwelling period.
Results
Technical and clinical success was achieved in all 27 patients. All the tubes were electively removed 19–364 days (mean indwelling period = 104 days) after confirmation of the possibility of oral intake. Asymptomatic pneumoperitoneum occurred in 2/27 (7.4%) patients as minor complications and was resolved spontaneously by the time of the one-week follow-up. There were no major complications. During the follow-up period, a total of 11 tube changes were performed in seven patients for an elective tube change within a six-month interval (n = 5) or because of tube occlusion (n = 6).
Conclusion
Temporary PRGJ using the modified Chiba-needle technique with a single gastropexy was clinically effective and technically feasible in patients with esophageal perforation or gastroparesis. It can provide adequate enteral nutrition during its temporary placement.
Introduction
Percutaneous endoscopic and radiologic placement of gastrostomy, gastrojejunostomy, and jejunostomy tubes has been a traditionally standard option for nutritional support and enteric feeding for patients with inadequate oral intake (1–5). Percutaneous jejunostomy or gastrojejunostomy is preferred for patients with an abnormal gastric anatomy or surgically altered stomach (1,6). Since jejunal access using a jejunal tube was first described by Ponsky (7) in 1984, the use of fluoroscopically guided, transgastric jejunostomy, termed percutaneous radiologic gastrojejunostomy (PRGJ), has been increasingly reported as well as very effective for avoiding gastroesophageal reflux or aspiration (7–9). However, PRGJ tubes have more commonly been associated with tube obstruction, intussusception, and antegrade enteral tube migration and these complications may be associated with the duration of tube placement (10,11). Moreover, these complications may impair the quality of life in patients who undergo permanent PRGJ tube placement.
Temporary PRGJ tube placement may be possible in patients with gastroesophageal reflux disease, esophageal perforation, or respiratory-esophageal fistulas because temporary dysphagia by these causes may be reversible due to spontaneous and/or treatment-induced recovery, even in chronic stages (12–14). If nutrition and hydration needs are accomplished orally and no other contraindications exist, PRGJ tubes should be removed in order to prevent long-term complications. Although the effectiveness of PRGJ has been reported in many previous studies (10–14), a detailed description of the indications and clinical effectiveness of temporary PRGJ is still limited. Therefore, the aim of the present study was to evaluate the clinical effectiveness and technical feasibility of temporary PRGJ using the modified Chiba-needle technique with single gastropexy.
Material and Methods
Patient population
Our institutional review board approved this study and waived the requirement for informed consent. From January 2008 to January 2018, we retrospectively reviewed the medical records of 27 patients (19 men, 8 women; mean age = 61 years; age range = 32–77 years) who had undergone temporary PRGJ using the modified Chiba-needle technique with a single gastropexy. All the PRGJ tubes were intentionally removed after confirmation of patient oral intake.
The major indications for temporary PRGJ were esophageal perforation (EP) (n = 18) with/without esophagorespiratory fistula (ERF) after esophageal disease (n = 11), lung disease (n = 7), or gastroparesis after postoperative care (n = 9). The clinical information is summarized in Table 1.
Clinical information and results in 27 patients who underwent temporary PRGJ.
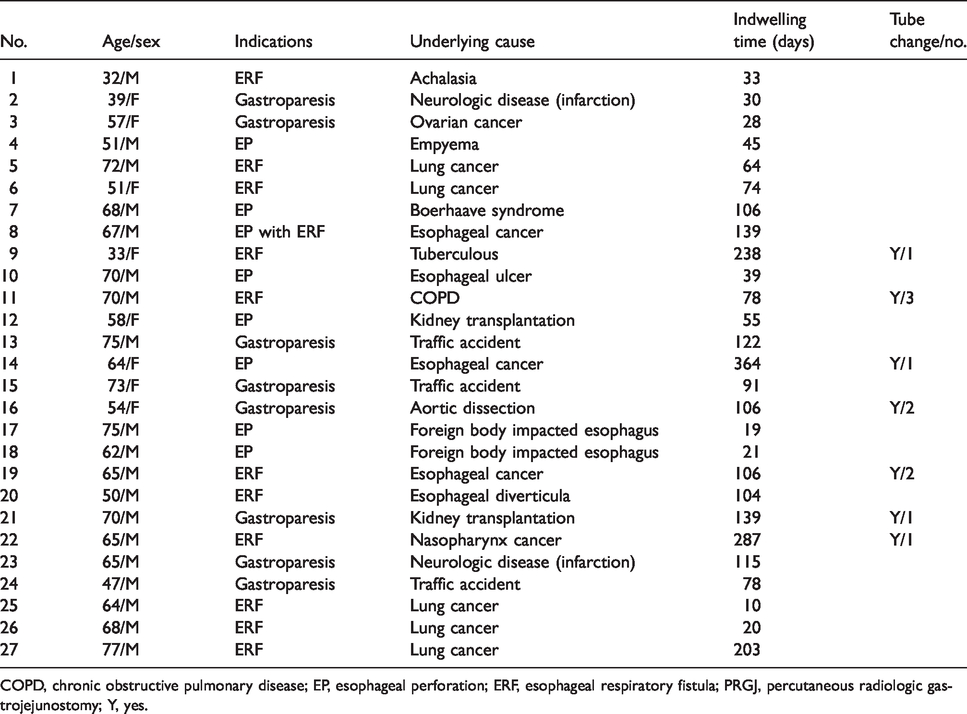
COPD, chronic obstructive pulmonary disease; EP, esophageal perforation; ERF, esophageal respiratory fistula; PRGJ, percutaneous radiologic gastrojejunostomy; Y, yes.
Technique
All the temporary PRGJ tubes were placed under fluoroscopic guidance with the patient under local anesthesia. An 8-Fr nasogastric tube was placed into the patient’s stomach one day before the PRGJ in order to decompress the stomach. Prophylactic antibiotics were routinely administered to prevent peristomal infection after the PRGJ. After intravenous administration of 20 mg of hyoscine butylbromide (Buscopan®; Boehringer, Ingelheim, Germany) to inhibit gastrointestinal motility, approximately 300–400 mL of air was then injected through the nasogastric tube in order to insufflate air into the stomach. Under fluoroscopic guidance, an appropriate puncture site was selected overlying the lower portion of the stomach. After local anesthesia, a 21-gauge, 15-cm-long Chiba needle (Cook, Bloomington, IN, USA) was advanced into the insufflated stomach toward the antrum. When we were able to confirm tenting of the anterior wall of the stomach, we then advanced the Chiba needle gently under fluoroscopic guidance in lateral projection of the C-arm.
After confirmation of the needle position by injection of contrast material, a 0.018-inch guide wire (Cope gastrointestinal Suture Anchor set, Cook) was passed into the stomach. The Chiba needle was then exchanged for a 6-Fr Neff percutaneous access sheath (Cook). A Cope suture anchor was then deployed into the stomach lumen through the Neff percutaneous access sheath using a 0.035-inch, 180-cm-long, hydrophilic guide wire (Terumo, Tokyo, Japan) for gastropexy. Pyloric catheterization was performed with the hydrophilic guide wire and a 5-Fr 65-cm Cobra catheter (C1, Cook). After cannulation of the proximal jejunum, the 0.035-inch hydrophilic guide wire was replaced with a 0.038-inch, 180-cm Amplatz stiff guide wire (Cook). Once the stomach was anchored to the abdominal wall, the puncture site was serially dilated over the stiff guide wire using 8-Fr, 10-Fr, 12-Fr, or 14-Fr dilators to allow placement of a 14-Fr, Cook-Cope type locking pigtail catheter (Cook).
Follow-up and data analysis
Patients underwent a contrast study via the tube 1–3 days and again one week after PRGJ tube placement in order to confirm the tube position, possible leakage, and the patency. Tube feeding was then started 1–3 days later if there were no complications related to the tube placement. The suture anchor was cut one week after the procedure. Further follow-up contrast studies via the tube were only performed if there were problems such as tube clogging, tract leakage, or tube dislodgement.
We evaluated the technical and clinical success, procedure-related complications, and the tube indwelling period. Temporary PRGJ was defined as transitory placement of a feeding tube in the jejunum until the end of treatment that is difficult to ingest. Technical success was defined as correct positioning of the feeding tube in the jejunum, and which was checked fluoroscopically at the end of the procedure. Clinical success was defined as successful feeding by the patient and without fever or pain after tube placement one week after PRGJ. Major complications were defined as hemorrhage requiring blood transfusion or other intervention, peritonitis, or other conditions necessitating surgery or intensive care. Minor complications were defined as self-limiting events or tube dislodgement.
Results
PRGJ using a modified Chiba-needle technique with single gastropexy under fluoroscopic guidance was technically successful in all 27 (100%) participants and with no procedure-related complications. A single puncture attempt was required in all patients. Catheterization of the pylorus was possible using a hydrophilic guide wire and a Cobra catheter after introduction of single anchor in all patients. Tube patency was noted without leakage on the immediate, post-procedure contrast study via the tube. Feeding was provided in all patients 1–3 days after the PRGJ. Clinical success was achieved in all patients with successful feeding without fever or pain at the time of the one-week follow-up contrast study (Fig. 1).
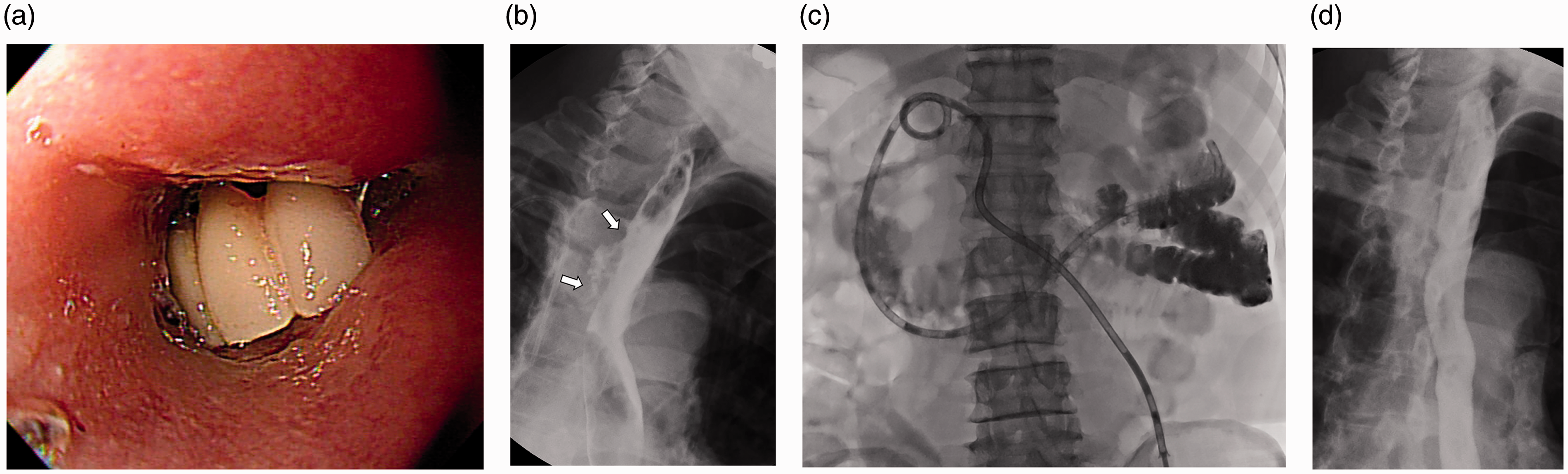
A 75-year-old man with esophageal perforation caused by a foreign-body impacted esophagus and who underwent temporary PRGJ for enteric nutrition. (a) Endoscopic image shows the denture impacted esophagus. (b) Esophagography obtained immediately after removal of the denture shows extraluminal contrast leakage at the impacted site (arrows). (c) Radiograph obtained immediately after PRGJ tube placement shows good passage of contrast medium though the tube and without leakage. (d) Esophagography obtained 19 days after PRGJ shows a well-healed esophageal perforation site with nutrition support via PRGJ. PRGJ, percutaneous radiologic gastrojejunostomy.
All tubes were electively removed 19–364 days after the PRGJ tube placement. The median indwelling period was 104 days after tube placement. All patients underwent contrast study, such as esophagography and/or an upper gastrointestinal series preceding tube removal in order to assess the possibility of oral intake or to confirm the healing of esophageal injuries such as perforation and/or ERFs. The tubes were removed seven days after starting oral feeding.
Two patients (7.4%) had minor complications in which a pneumoperitoneum was noted 1–3 days after tube placement. These two patients were asymptomatic, and the pneumoperitoneum had spontaneously resolved by the time of the one-week follow-up. Therefore, the complications were categorized as minor. There were no major complications or procedure-related mortality after the PRGJ tube placement.
During the follow-up period, a total of 11 tube changes were performed in seven patients, either for elective tube change within a six-month interval (n = 5) or due to tube occlusion (n = 6). All the replaced tubes were the same diameter catheter.
Discussion
The results of our retrospective study demonstrated that temporary PRGJ with a single gastropexy is technically feasible and safe. All the tubes were successfully removed and with only a few minor complications. Temporary PRGJ was highly effective for instant dysphagia relief and thus allowing adequate enteral nutrition while treating the dysphagia caused by esophageal injuries or gastroparesis. Malnutrition as a consequence of dysphagia is a well-known factor influencing the outcome of esophageal resection as well as affecting a patient’s recovery from surgery or illness and increasing the incidence and severity of infection (15–17). Given the fact that patients who opt for antibiotic medication are required to fast a minimum of several weeks during the treatment, temporary PRGJ allows sufficient enteral feeding via the tube and can serve as an effective bridge to various types of treatment for severe dysphagia.
The majority of patients requiring nutritional support will need it for less than one month, and nasoenteric tube feeding is by far the most commonly used route of access (17,18). The tubes are easy to insert, although there is a risk of esophageal or pulmonary perforation due to misplacement (19). Patients with a high risk of pulmonary regurgitation, such as those with gastroparesis and esophageal perforation with ERFs, are considered desirable to feed beyond the post-pyloric region in order to prevent gastroesophageal reflux. Placing nasoenteral feeding tubes can be difficult so as to have a transpyloric passage of the tube and there is a high risk of additional injuries to the damaged esophagus during the procedure (19,20). In the present study, temporary PRGJ provided successful enteral feeding for patients with esophageal injuries or gastroparesis and all of the tubes were removed safely after resuming oral feeding.
In the present study, gastric puncture with a 21-gauge Chiba needle for PRGJ is safe and technically feasible without any complications and is relatively easy because tenting of the stomach wall was clearly seen as the needle was gently advanced in all patients. Furthermore, there was less fear of vascular injury during the advancement of the Chiba needle due to its smaller diameter and which can thus avoid hemorrhagic complications. This finding is comparable to that in the report by Watkinson et al. (21) regarding the use of a 22-gauge Chiba needle for gastric puncture as they found no hemorrhagic complications in 100 cases of PRG and PRGJ.
Gastropexy with retention sutures has been used by many clinicians since its initial description because it can significantly reduce procedure-related complications (22). Theoretically, when the number of anchors increases, the fixation force of the anterior wall of the stomach to the abdominal wall also increases. Consequently, such risks as additional gastric catheter placement, leakage to the peritoneum, and peritonitis decrease; however, in parallel, the risk of bleeding or infection increases (23). Single gastropexy has advantages, such as a lower risk of bleeding or infection and a shorter procedure time. This technique consists of a single puncture of the stomach, thus creating a single tract for both an anchor and a guide wire over which dilatation and tube insertion can be performed. In our study, PRGJ was successfully performed in all patients, although pneumoperitoneum was observed without symptoms of peritonitis in two patients.
The principal limitations of the present study are its retrospective design and the relatively few patients collected over the 10-year period. In addition, as this was a single-center study, all the procedures were performed by clinically experienced interventional radiologists. As these results may not apply to other clinical practices, they need to be verified in larger multicenter studies.
In conclusion, temporary PRGJ using the modified Chiba-needle technique with single gastropexy was clinically effective and technically feasible in patients with esophageal perforation or gastroparesis. It can also provide adequate enteral nutrition during the treatment of dysphagia.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.