
Abstract
Background
Hypoxia-inducible factor (HIF)-1α plays a key role in hypoxic adaptation of tumor cells. Overexpression of HIF-1α is associated with tumor aggressiveness and worse prognosis in several malignancies. Presumably, expression of HIF-1a may be reflected by positron emission tomography with 2-deoxy-2 [fluorine-18] fluoro-D-glucose (18F-FDG PET). There are inconsistent data about relationships between FDG PET and HIF-1α.
Purpose
To provide evident data about associations between maximum standardized uptake value (SUVmax) and HIF-1α expression in solid tumors.
Material and Methods
MEDLINE, SCOPUS, and EMBASE databases were screened for relationships between SUV and HIF-1α up to August 2019. Overall, 21 studies with 1154 patients were identified. The following data were extracted from the literature: authors; year of publication; number of patients; and correlation coefficients.
Results
Correlation coefficients between SUVmax and HIF-1α were in the range of −0.51–0.71. The pooled correlation coefficient was 0.27 (95% confidence interval [CI] = 0.14–0.41). Furthermore, correlation coefficients for some tumor entities were calculated. For this sub-analysis, data for primary tumors with >2 reports were included. The calculated correlation coefficients in the analyzed subgroups were as follows: head and neck squamous cell carcinoma: ρ = 0.25 (95% CI = 0.07–0.42); non-small lung cell cancer: ρ = 0.27 (95% CI = −0.14–0.67); uterine cervical cancer: ρ = −0.09 (95% CI = −0.89–0.71); thymic tumors: ρ = 0.39 (95% CI = 0.04–0.58).
Conclusion
SUVmax of FDG PET correlated weakly with expression of HIF-1α both in overall sample and tumor subgroups. Therefore, FDG PET cannot be used for prediction of hypoxia in clinical practice.
Introduction
Positron emission tomography (PET) with 2-deoxy-2 [fluorine-18] fluoro-D-glucose (18F-FDG PET) is well established for diagnosing and staging in different malignant tumors. Besides diagnostic potential, 18F-FDG PET parameters can also predict histologic and biologic characteristics such as tumor stage and grade (1–3). For example, in breast cancer, invasive carcinomas have higher uptake than lower-grade tumors (1). Furthermore, PET can also be used for monitoring of treatment response (4). Finally, PET can predict prognosis in several tumors. So far, it has been shown that high metabolic activity determined by the standardized uptake value (SUV) was associated with poor survival in squamous cell carcinoma of the head and neck region (5).
These effects may be related to possible associations between PET parameters, particularly SUVmax, with underlying histopathology. In fact, some reports confirmed this hypothesis (6–8). For example, Cochet et al. (8) suggested that SUVmax correlated strong with expression of proliferation marker Ki 67 in breast cancer.
Besides proliferation activity, other histopathological biomarkers play an important role in different malignancies. One of them is hypoxia-inducible factor (HIF)-1α. According to the literature, hypoxia-inducible factors, particularly HIF-1α, play a key role in the adaptation of tumor cells to hypoxic and nutrient-deprived conditions by upregulating the transcription of several pro-oncogenic genes (9). Overexpression of HIF-1α is significantly associated with increase of mortality risk and worse prognosis in several malignancies (10–12).
Previously, some authors analyzed associations between PET parameters and expression of HIF-1α in several tumors with controversial results (13–20). While some authors identified significant correlations between the parameters, others did not (13,18,19). Furthermore, most reports investigated small samples of patients.
The aim of the present meta-analysis was to provide evident data regarding possible relationships between SUV retrieved from FDG PET and HIF-1α.
Material and Methods
Data acquisition
The endpoint of the present meta-analysis was the assumption that SUVmax derived from FDG PET may have strong correlations with expression of HIF-1α.
For this analysis, MEDLINE, EMBASE, and SCOPUS databases were screened for associations between PET (SUVmax) and expression of HIF-1α up to July 2019. The strategy of data acquisition is shown in Fig. 1.
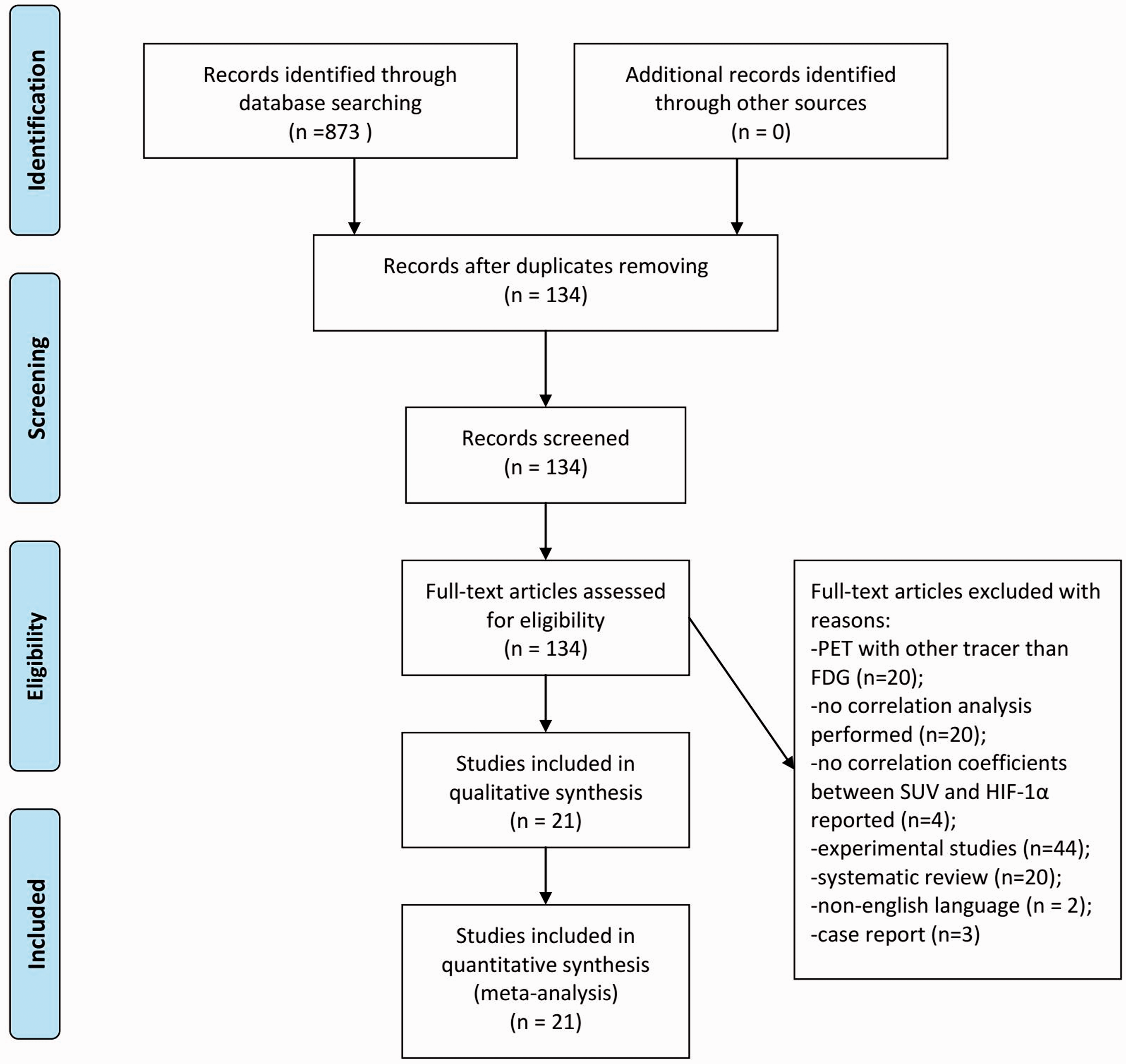
Flow chart of the data acquisition.
The following search words were used: PET (or) positron emission tomography (or) SUV (or) standardized uptake value AND HIF-1α (or) HIF1α (or) HIF 1α (or) HIF-1 alpha (or) HIF1 alpha (or) hypoxia-inducible factor (or) hypoxia inducible factor. Secondary references were also recruited. The primary search identified 873 records. After exclusion of duplicate articles (n = 739), abstracts of the remaining 134 articles were checked. Exclusion criteria were: review articles, experimental animals and in vitro studies, case reports, and non-English publications. Overall, 93 articles were excluded after checking of abstracts. Thereafter, full texts of the remaining 41 articles were retrieved and analyzed. Inclusion criteria were: original articles; studies investigating humans; reported correlation coefficients between SUVmax derived from FDG PET and expression of HIF-1α; in the English language. Articles that did not contain correlation coefficients between PET/SUV and HIF-1α were also excluded (n = 20). Therefore, 21 studies were included into the present analysis (13–33). The following data were extracted from the literature: authors; year of publication; diagnosis; number of patients; and correlation coefficients. In all studies, Spearman’s correlation coefficient for correlations between SUVmax and HIF-1α was reported. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement (PRISMA) was used for the research (34).
Meta-analysis
First, the methodological quality of the acquired 21 studies was checked by one observer (AS) using the Quality Assessment of Diagnostic Studies (QUADAS 2) instrument (35). Fig. 2 shows the results of QUADAS proving. Of the involved studies, 5 (24%) were prospective, 8 (38%) retrospective, and in 8 (38%) studies the design was unclear.
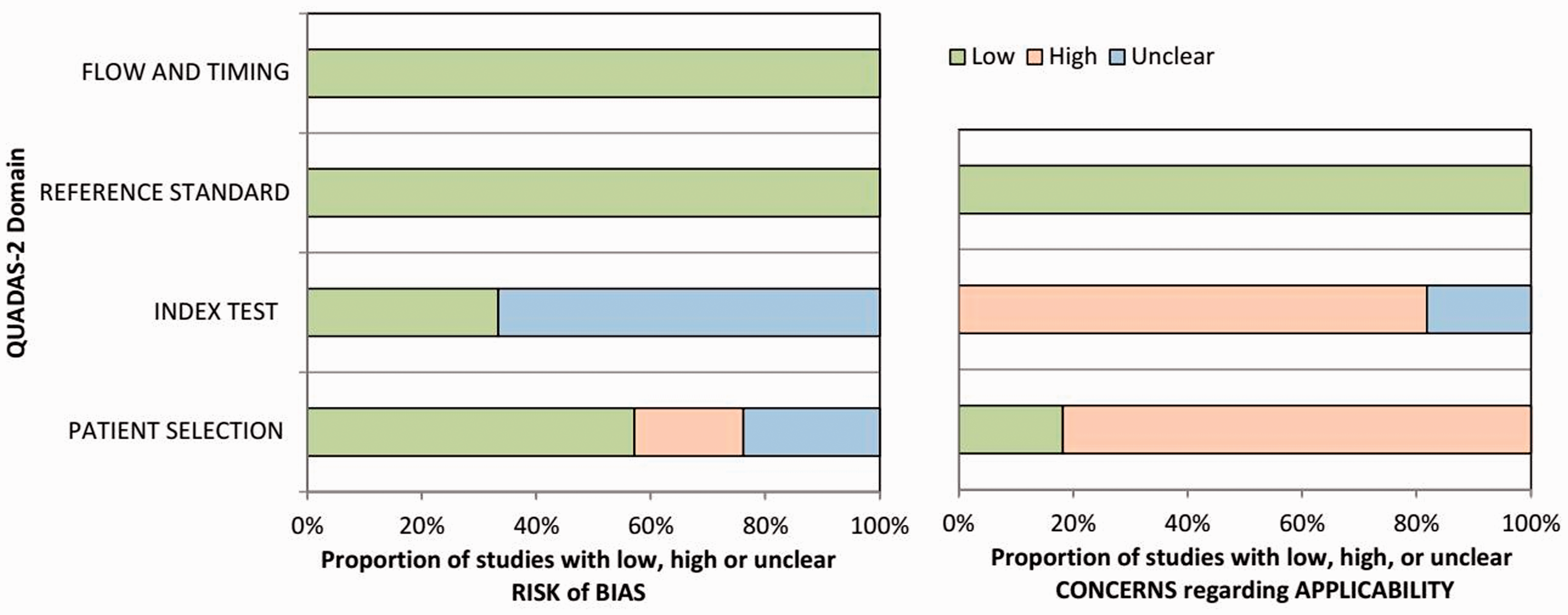
Methodological quality of the involved 21 studies according to the QUADAS 2 criteria.
Second, the meta-analysis was undertaken by using RevMan 5.3 (Computer program, version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014). Heterogeneity was calculated by means of the inconsistency index I2 (36,37).
Third, DerSimonian and Laird random-effects models with inverse-variance weights were performed without any further correction (3).
Results
Overall, the acquired 21 studies comprised 1154 patients with different malignant tumors (Table 1). They were predominantly non-small cell lung cancer (NSCLC; 28.3%) and head and neck squamous cell carcinomas (HNSCC; 10.8%).
Included studies and primary tumors.
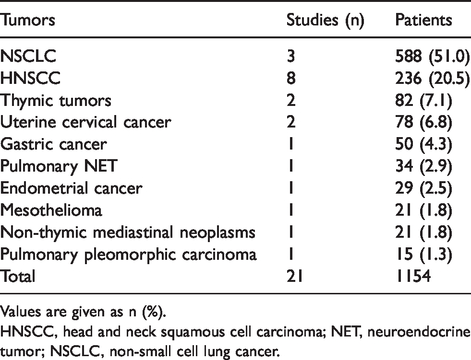
Values are given as n (%).
HNSCC, head and neck squamous cell carcinoma; NET, neuroendocrine tumor; NSCLC, non-small cell lung cancer.
The correlation coefficients between SUVmax and HIF-1α were in the range of −0.51–0.71 (Fig. 3). The pooled correlation coefficient was 0.27 (95% confidence interval [CI] = 0.14–0.41).
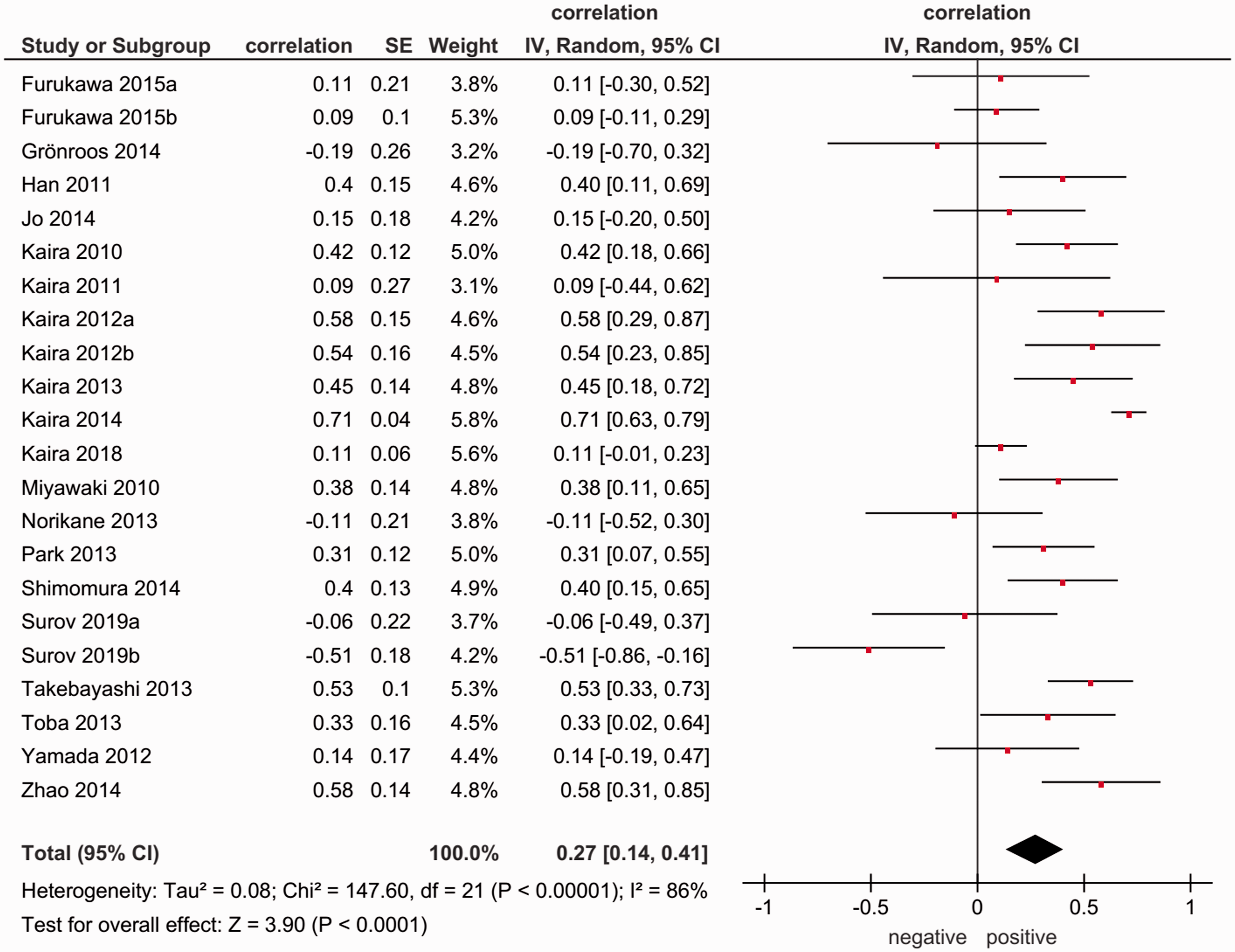
Forest plots of correlation coefficients between SUVmax derived from 18F-FDG PET and expression of HIF-1α in all involved studies/malignancies.
On the next step, correlation coefficients for every tumor entity were calculated. For this sub-analysis, data for primary tumors with more than two reports were included.
The calculated correlation coefficients in the analyzed subgroups were as follows: HNSCC: ρ = 0.25 (95% CI = 0.07–0.42); NSCLC: ρ = 0.27 (95% CI = −0.14–0.67); uterine cervical cancer: ρ = −0.09 (95% CI = −0.89–0.71); thymic tumors: ρ = 0.39 (95% CI = 0.04–0.58) (Fig. 4).
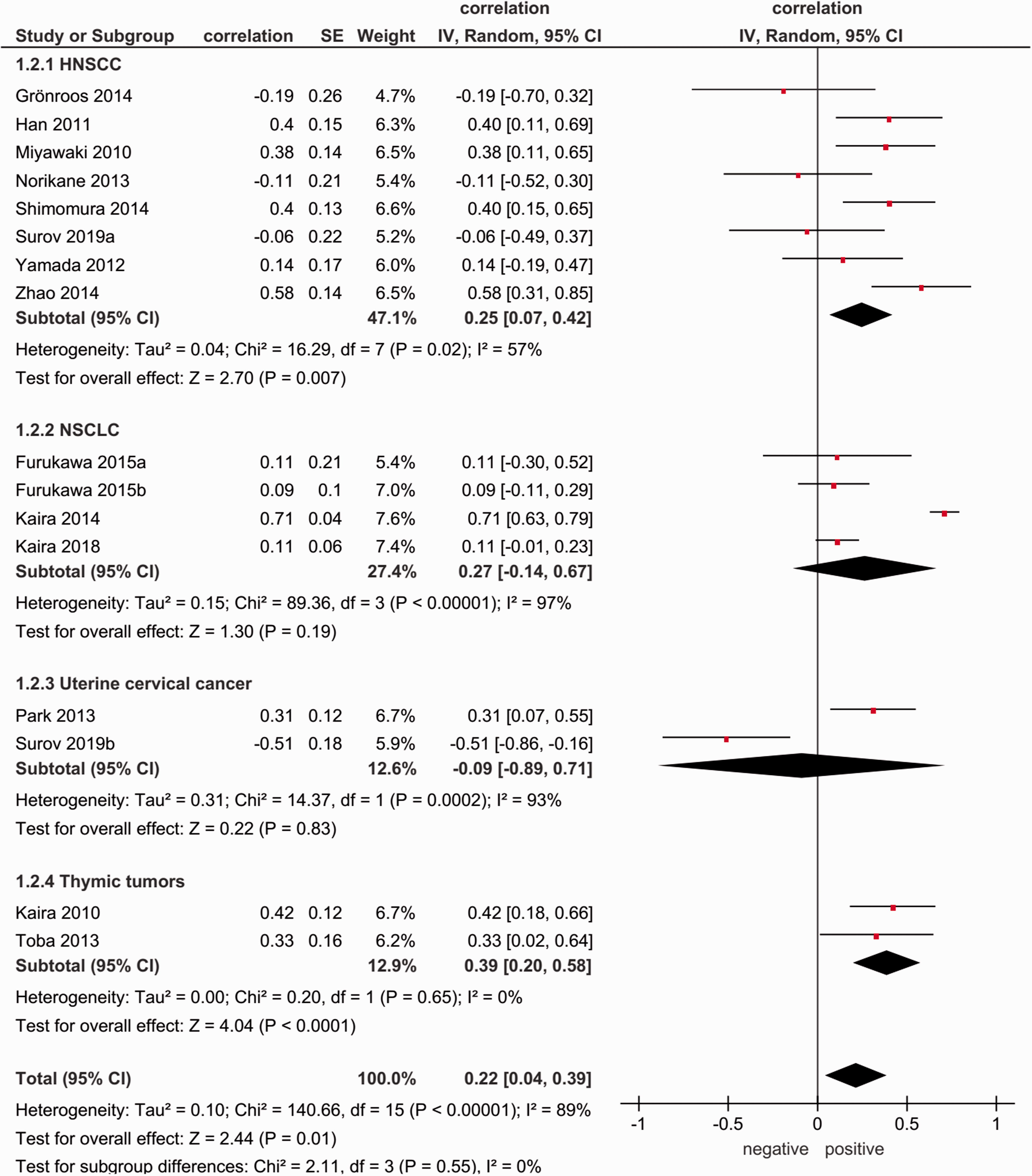
Forest plots of correlation coefficients between SUVmax derived from derived from 18F-FDG PET and expression of HIF-1α in different primary tumors.
Discussion
It is well-known that uncontrolled growth of cancer cells results in imbalance between oxygen demand and angiogenesis. This causes tumor hypoxia, which provokes activation of cellular adaptation mechanisms. HIF-1α plays a key role in hypoxic adaptation of tumor cells. HIF-1α is overexpressed in hypoxia and initializes a cascade including transcription of a network of genes that control several aspects of tumor biology (39–41). So far, HIF-1α induces transcription of vascular endothelial growth factor (VEGF) to promote endothelial cell proliferation and blood vessel formation (40–43). Furthermore, HIF-1α stimulates glucose metabolism of cancer cells via upregulation of glucose transporter (GLUT) 1 and 3 (40–43). Moreover, other relevant factors such as erythropoietin, inducible nitric oxide synthase, and different matrix metalloproteinases are also activated by HIF-1α (39–42). Overall, these mechanisms result in aggressiveness, increase metastatic potential, and promote tumor progression (39–42). In fact, previously, numerous studies identified a significant role of HIF-1α in several malignancies. It has been shown that overexpression of HIF-1α was associated with increased mortality and worse prognosis of HNSCC (10). In lung cancer, patients with positive HIF-1α expression in tumor tissues had lower overall survival rate than patients with negative HIF-1α expression (12). Similar results were reported for uterine cervical cancer (11). In addition, HIF-1α predicts resistance to anticancer therapy (9–11). Therefore, visualization of tumor hypoxia may be of great importance. Some novel tracers were proposed to reflect tumor hypoxia HIF-1α. They showed promising preclinical and clinical results (44). However, they are not widely available and, therefore, cannot be used in daily clinical routine. In contrast, the FDG is available in clinics worldwide. Therefore, the possibility to predict on imaging, which is widely used in clinical setting, expression of HIF-1α is very important. In fact, if metabolic parameters of FDG PET are associated with expression of HIF-1α, FDG PET can be used as surrogate biomarker for tumoral hypoxia. Hence, tumor behavior can also be predicted. Theoretically, metabolic activity measured by FDG PET may reflect expression of HIF-1α. As mentioned above, HIF-1α induces upregulation of GLUT 1 and 3, which are main cellular mediators for FDG (40–43). Presumably, parameters of FDG PET like SUVmax may well correlate with expression of HIF-1α. Some experimental investigations supported this hypothesis (45,46). Previously, only few clinical studies investigated this question. Some authors reported promising data about relationships between FDG PET and HIF-1α. However, because of the small number of participants, the reported results cannot apply as evident. The present meta-analysis is the first report based on a large sample including different tumors. Our results did not confirm the hypothesis about possible associations between SUVmax derived from FDG PET and expression of HIF-1α. A wide spectrum of correlation coefficients was identified and the pooled coefficient was 0.27. This finding indicates that FDG PET is only weakly associated with tumoral hypoxia. Furthermore, in the tumor subgroups, namely NSCLC, HNSCC, uterine cervical cancer, and thymic tumors SUVmax correlated weakly with HIF-1α. These findings are difficult to ascertain. Presumably, the HIF-1α processes only a small part of all glucose metabolisms. It is also possible that other hypoxia factors, such as hexokinase IX, may be stronger associated with glucose metabolism/FDG PET. Furthermore, the FDG uptake might be influenced by a complex interaction of several histopathological features such as intratumoral inflammatory cells, extracellular matrix, and other factors. These might be some of the reasons for the identified results in the present analysis.
The present meta-analysis identified some problems. To date, there are no reports analyzing associations between SUVmax and expression of HIF-1α in frequent and less frequent solid malignancies such as breast cancer, colonic cancer, esophageal carcinoma, different sarcomas, pancreatic cancer, hepatocellular carcinoma, and cholangiocellular carcinoma. Further investigations are needed.
Furthermore, we found significant heterogeneities among the studies investigating the same tumors. So far, in HNSCC, Grönroos et al. (14) observed an inverse correlation between SUVmax and expression of HIF-1α (−0.194), but in the study by Zhao et al. (33), the correlation coefficient was 0.577. Moreover, the same work group of Kaira et al. (17,23) identified different correlations between SUVmax and expression of HIF-1α in NSCLC, namely 0.71 and 0.11. This finding is difficult to ascertain. The identified variations of the published correlation coefficients might be related to different ratio of tumor subtypes, or different analysis methods of HIF-1α expression. Finally, for uterine cervical cancer and thymic tumors, the number of patients was small, namely 78 and 82, respectively. This fact relativizes the estimated correlation coefficients.
The present analysis also identified some methodological problems in the acquired studies. Most of the acquired reports were retrospective or the study design was not given. Furthermore, according to the QUADAS criteria, most included studies showed index test bias. Some reports also had patient selection bias. In addition, the included studies used different HIF-1α antibodies and different methods of estimation of staining intensity. Finally, only correlation coefficients between SUVmax and HIF-1α were included into the present meta-analysis. However, associations between these parameters may be of non-linear character. Therefore, tumors with high expression of HIF-1α may also have higher SUV values, but this relationship cannot be displayed by a correlation analysis. Moreover, real association between FDG uptake and HIF-1α is mainly based on the absence of evidence and this is not evidence of absence. Clearly, further prospective studies with well-defined inclusion and exclusion criteria and homogeneous methodology are needed.
In conclusion, the present meta-analysis based on the current literature showed that SUVmax of FDG PET correlated weakly with expression of HIF-1α in both the overall sample and tumor subgroups. Therefore, FDG PET cannot be used for prediction of hypoxia in clinical practice.
Authors' note
Alexey Surov is currently affiliated with Department of Radiology and Nuclear Medicine, Otto-von-Guericje University Magdeburg, Magdeburg, Germany.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.