
Abstract
Background
Neuroschistosomiasis is not commonly encountered and is probably underrecognized. We hope these findings can help clinicians and radiologists to raise awareness of this disabling disorder.
Purpose
To demonstrate the magnetic resonance imaging (MRI) findings of cerebral schistosomiasis and correlate it with pathological findings.
Material and Methods
We identified seven patients with cerebral schistosomiasis from radiology and pathology archives of our hospital. Of the seven patients, six were pathologically confirmed. The remaining patient had pathologically confirmed spinal schistosomiasis with MRI findings of cerebral involvement. MRI and pathological findings of these patients were analyzed and correlated.
Results
Multiple enhancing nodules at varying size were found in all patients. Prominent leptomeningeal or choroidal veins were found in six patients, four at the center of the foci and two at the periphery. Hemorrhage was identified in two patients. Histology revealed granulomas around ova in six patients. A prominent vein with ova in the lumen and wall of a vein was found in one patient and perivascular ova deposition was found in one patient.
Conclusion
Multiple enhancing nodules with central or peripheral veins in a circumscribed brain area are important signs to the diagnosis of cerebral schistosomiasis. The inflamed veins involved may be the route taken by the ova to spread to the brain tissue.
Introduction
Schistosomiasis is a helminthic infection caused by blood flukes of the genus Schistosoma. Five species infect human beings: Schistosoma mansoni, Schistosoma haematobium, and Schistosoma japonicum are the most widely distributed; and Schistosoma mekongi and Schistosoma intercalatum occur in restricted areas. More than 200 million people are infected across Africa, Asia, and South America, and close to 800 million are at risk of infection (1). The majority of S. haematobium, S. mansoni, and S. intercalatum infections are found in sub-Saharan Africa. S. mansoni remains endemic in parts of Brazil, Venezuela, and the Caribbean. S. japonicum infection still occurs in China, Indonesia, and the Philippines (2,3).
Despite major advances in control and substantial decreases in morbidity and mortality, schistosomiasis continues to spread to new geographic areas and re-emerges in previously endemic regions (4,5). Almost all reported cases of schistosomiasis involving the central nervous system are caused by infection with S. mansoni, S. haematobium, or S. japonicum (6). S. mansoni and S. haematobium usually affect the spinal cord, while S. japonicum mostly leads to encephalic diseases (7). Cerebral schistosomiasis can develop at any stage of infection (6). Although rare by comparison with the high prevalence of hepatointestinal and urinary tract diseases, neuroschistosomiasis is not uncommon, and is probably underrecognized (6). The aim of the present study was to report magnetic resonance imaging (MRI) findings of seven patients with cerebral schistosomiasis and correlate these findings with pathological data. We hope these findings can help clinicians and radiologists to raise awareness of this disabling disorder.
Material and Methods
We searched the radiology and pathology archives in our hospital for patients diagnosed with cerebral schistosomiasis within 10 years. We identified seven patients (4 male, 3 female; mean age = 22.1 years; age range = 8–35 years) with MR images before the diagnosis has been made. Among the seven patients, six patients had pathologically confirmed cerebral schistosomiasis by surgical resection or biopsy. The remaining patient had pathologically confirmed spinal schistosomiasis; MRI of the patient showed cerebral involvement.
MRI was performed on a 1.5-T scanner with standard head coil. All examinations comprised an axial T2-weighted (T2W) fast spin-echo sequence (TR/TE = 4100/93 ms), an axial FLAIR sequence (TR/TE/TI = 10,000/90/2500 ms), and an axial T1-weighted (T1W) spin-echo sequence (TR/TE = 450/9 ms). Except for one patient, axial, coronal, and sagittal T1W enhanced images were obtained after intravenous injection of gadopentetate dimeglumine (0.2 mmol/kg). The section thickness was 6 mm with an acquisition matrix of 256 × 256 and a field of view of 240 mm.
Results
Clinical and laboratory findings
The duration of symptoms ranged from 10 days to six months. All patients were natives of endemic regions in southwest China. Seven patients presented with headache, three with seizures, and three with vomiting. Two patients suffered from functional impairment of the kidney and liver. Eosinophilia was present in six patients. Serology for S. japonicum using the circumoval precipitin reaction test (COPT) was positive in six patients and negative in one patient.
Imaging findings
All lesions were located at the cortex and subcortical white matter in a circumscribed area. Cerebellar lesions were found in two patients, posterior temporal, occipital, and parietal lesions were found in four patients, and the one was found in the frontal lobe. Multiple enhanced nodules measuring in the range of 1–10 mm surrounded by vasogenic edema were presented in all patients. Smaller nodules measuring 1–3 mm were found in seven patients, manifesting as rim enhancement with central isointensity or hyperintensity on T2W imaging and isointensity on T1W imaging (Fig. 1). Larger nodules in the range of 5–10 mm were found in one patient, manifesting as rim enhancement with central hyperintensity on T2W imaging and hypointensity on T1W imaging (Fig. 2).

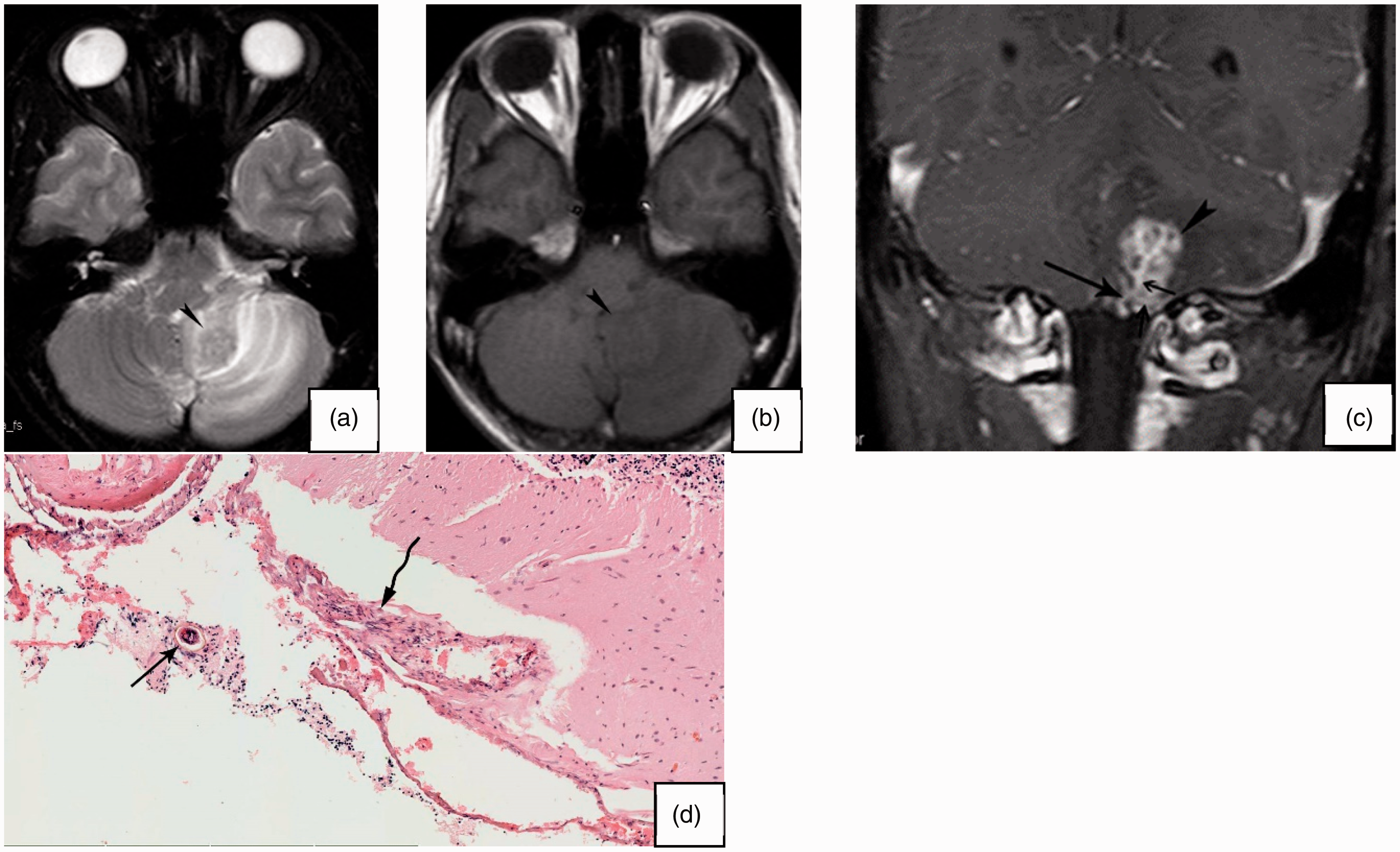
Case 6. T2W image (a), T1W image (b), and contrast-enhanced coronal T1W image (c) demonstrate multiple enhancing nodules with hypointensity on T2W imaging and isointensity on T1W imaging (thick arrows) surrounded by vasogenic edema. Hyperintensity on T1W imaging and hypointensity on T2W imaging is seen in right occipital cortex (arrowheads), which may be hemorrhage. A prominent enhancing leptomeningeal vein is seen at the center of the focus (thin arrow); another vein of adjacent focus is also seen (wavy arrow). (d) Histological photomicrograph (10 × 10) with H&E staining reveals productive granulomas (arrowheads), inflamed vein (thin arrows), and neutrophil infiltration (thick arrows). H&E, hematoxylin and eosin; T1W, T1-weighted; T2W, T2-weighted.

Case 3. T2W image (a), T1W image (b), and contrast-enhanced T1W image (c) show multiple enhancing nodules with hyperintensity on T2W imaging and hypointensity on T1W imaging (arrowheads). The choroidal plexus of right ventricular antrum is at the periphery of the focus and intimately attached to it (arrow). T1W image (d) slightly cephalad to (b) demonstrates hemorrhage (arrow). (e) Histological photomicrograph (1 × 10) with H&E staining shows an inflamed vein. (e) The inset (5 × 10), with a magnification of the marked area on the vein, shows perivascular inflammation (wavy arrows) and ova in the lumen (arrowheads) and wall (arrows). (f) Histological photomicrograph (5 × 10) also displays necrotic granulomas with neutrophil infiltration. H&E, hematoxylin and eosin; T1W, T1-weighted; T2W, T2-weighted.
Prominent leptomeningeal vein was present in six patients, which cannot be definitely identified in the remaining one patient because of lack of orthogonal images. Two patterns of leptomeningeal vein were identified in the six patients, a central pattern and a peripheral pattern (Fig. 2). In the central pattern, the vein and the nodules together appeared either as an arborization or a blooming flower (Figs. 1 and 3).
Case 1. T2W image (a), T1W image (b), and contrast-enhanced coronal T1W image (c) show multiple enhancing nodules with hypointensity on T2W imaging and isointensity on T1W imaging (arrowheads). An arborizing leptomeningeal vein is seen at the center of the lesion (arrow). (d) Histological photomicrograph (10 × 10) with H&E staining shows an ovum intimately related to the vein (arrow) and perivascular inflammation (wavy arrow). H&E, hematoxylin and eosin; T1W, T1-weighted; T2W, T2-weighted.
Subacute hemorrhage was found in two patients (Figs. 2 and 4). In another patient, curvilinear cortical hyperintensity on T1W imaging surrounded by vasogenic edema was identified (Fig. 1).

Case 4. T1W image (a) shows subacute hemorrhage (arrowhead). Contrast-enhanced T1W image (b) demonstrates enhancing nodules (arrow) and a vein (wavy arrow) at the periphery of the lesion. Sagittal T2W image (c) and T1W image (d) reveal epidural hematoma compressing the spinal cord (arrowheads), which is caused by spinal schistosomiasis. T1W, T1-weighted; T2W, T2-weighted.
Pathological findings
Cerebral histology was available in six patients and spinal histology in another patient. Granulomatous reaction around ova (referring to cerebral schistosomiasis eggs) was found in all cases. No adult worm was found in any of the seven patients. The majority of the granulomas were productive granulomas, in which inflammatory reaction around the egg consists of a variable number of epithelioid and multinuclear giant cells of the foreign-body type surrounded by lymphocytes and plasmocyte (Fig. 1). Prominent necrotic granulomas were found in one patient (Fig. 2). Prominent neutrophil and eosinophil infiltration were found in two cases (Figs. 1 and 2). A prominent vein with ova in the lumen and wall of a vein was found in one patient (Fig. 2). In another patient, a prominent leptomeningeal vein with perivascular ova deposition was identified. Perivascular inflammation of veins was shown in three patients (Fig. 3).
The clinical, laboratory, MRI, and pathological findings are listed in Table 1.
Clinical, laboratory, MRI, and pathological findings.
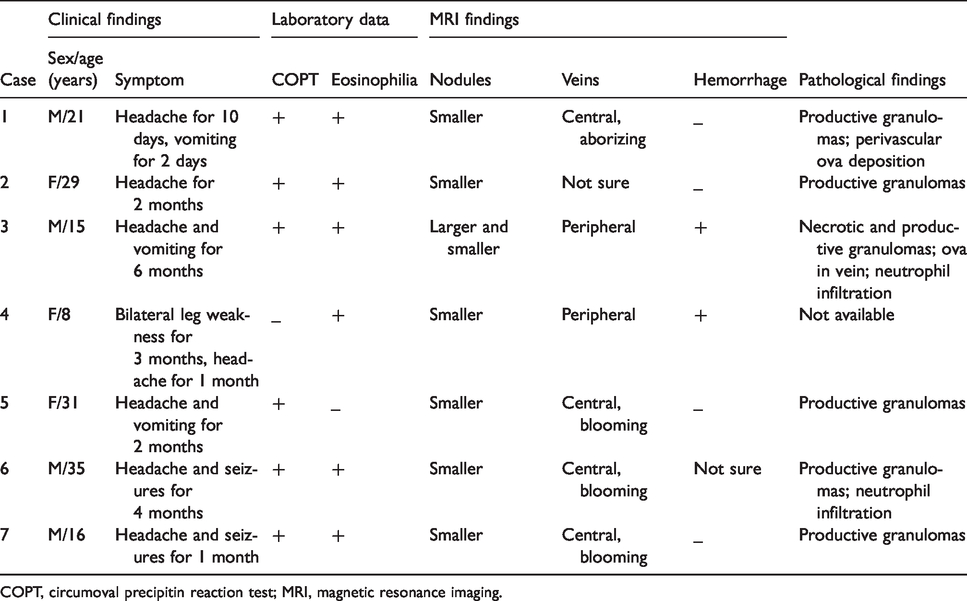
COPT, circumoval precipitin reaction test; MRI, magnetic resonance imaging.
Discussion
Schistosomes feed on blood and globulins through anaerobic glycolysis. The eggs of schistosomes are excreted in the urine or feces. On contact with water, the egg releases the miracidium, which later penetrate freshwater snail and multiply asexually in the snail into multicellular sporocysts. After migrating to the lymph vessels around the hepatopancreas of the snail, the secondary sporocysts change into cercariae. On finding a host, the cercariae penetrate the skin, migrate in the blood via the lungs to the liver, and transform into schistosomulae. These mature in the portal vein, mate, and migrate to their perivesicular (S. haematobium) or mesenteric (S. mansoni and S. japonicum) destination where the cycle starts again (8,9). Schistosomes may reach the brain in three possible ways: arterial embolization; retrograde venous flow via Batson’s epidural venous plexus; or in-situ egg deposition by anomalously migrating adult worm (8).
MRI findings of cerebral schistosomiasis have been reported sporadically (10–16). Enhanced multiple nodules of varying size are characteristic of cerebral schistosomiasis and some nodules may coalesce. In the present study, nodules measuring 0.1–1 cm were found. Larger nodules were hyperintense on T2W imaging and hypointense on T1W imaging, corresponding to necrosis in histology; while smaller nodules were iso- or hypointense on T2W imaging and isointense on T1W imaging, corresponding to productive changes. As in other organs, the granulomatous reaction in the brain has three stages: necrotic-exudative stage, productive stage, and healing by fibrosis stage and the granulomas in these stages become smaller and smaller as the disease progresses (8). MRI manifestations correlate well with these stages.
In the present study, we identified two patterns of leptomeningeal or choroidal vein in relation to the nodules. The central pattern manifested as central linear enhancement surrounded by multiple nodules, taking on an appearance of an arborization or blooming flower. In the peripheral pattern, a choroidal vein or a leptomeningeal vein was found at the periphery of the lesion. The central linear enhancement is thought by Sanelli et al. (14) to be the result of slow blood flow and local venous obstruction caused by the anomalous migration of the adult worm into the leptomeningeal veins. We did not identify signs of slow blood flow in patients with central linear enhancement in the present study. In the histological analysis, we found ova in the lumen and wall in an inflamed vein in one patient, and ova intimately related to veins in another patient. No adult worm was found in vessels or brain tissue in our series. Previous studies found ova either in the lumen of small arteries or around small arteries (8,17). We hypothesize that the central or peripheral vein represents the inflamed vein, through the wall of which the ova pierce to reach the brain tissue retrogradely through the Batson’s venous plexus. The patient with simultaneous spinal and cerebral involvement seemed to exemplify this. While we did not find ova in the arteries in the histological study, another possibility is that there may be a small arterial-venous shunt, through which the ova reach the vein antegradely.
We identified signs of intracranial hemorrhage in three patients and histological data was available in two of them. In histology, neutrophil and eosinophil infiltration was found in two patients and necrotic granulomas in one patient. While we did find inflammation in the venous wall, we failed to find necrotizing vascular lesions in the patients. In the third patient with confirmed spinal schistosomiasis, hemorrhage with a hyperintense vessel on T1W imaging at its periphery was found in the brain. Histology was unavailable in this patient. Whether the hyperintensity on T1W imaging of the peripheral leptomeningeal vein represented slow flow due to thrombosis is not clear. While intracranial hemorrhage may be present due to necrotizing vascular lesions or venous thrombosis (8,17), we cannot decide the cause of hemorrhage in these patients in the present study. In this study, it seems that intracranial hemorrhage is associated with prominent neutrophil and eosinophil infiltration, and necrotic-exudative granulomas, when immune response reaches maximum intensity. It is suggested that vasculitis mediated by eosinophils, immune complexes, or both has an important role in the pathogenesis of central nervous system involvement in the early phases of schistosomal infection (6,18).
Patients involved in the present study were at a chronic phase of schistosomal infection. Cerebral schistosomiasis rarely occurs during the acute phase of the disease, but when it does the neurological involvement differs from that in the chronic phase (8,19). Sporadic MRI reports of these patients show signs of border-zone infarctions or acute disseminated encephalomyelitis suggestive of vasculitis or small vessel thrombosis (20,21). It is suggested that systemic hypersensitivity reactions against the migrating schistosomula and early oviposition occur during the acute phase (6). Granulomatous reactions dominate in the chronic phase. The neurological involvement during the acute phase should be treated with corticosteroids, while that during chronic phase should be treated with praziquanel and sometimes surgery (6,7,19,20).
In conclusion, in patients with multiple enhancing nodules in the cortex and subcortical white matter of the brain, when the lesions are found in a circumscribed area, and prominent veins intimately related to the lesions are identified, cerebral schistosomiasis should be considered.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.