
Abstract
Background
The acute onset of Marchiafava-Bignami disease (MBD) is difficult to capture, and its clinical manifestations are overlapped. Magnetic resonance imaging (MRI) is very useful in the diagnosis of acute MBD.
Purpose
To investigate the MRI features and clinical outcomes of acute MBD.
Materials and Methods
Sagittal T2-weighted (T2W) or T1-weighted (T1W) imaging, axial T1W and T2W imaging, and axial FLAIR and diffusion-weighted imaging (DWI) sequences were performed in 17 patients with acute MBD on 1.5-T MR. According to the different ranges of callosal restricted diffusion, MBD was divided into Type I (n = 7, the completely involved), Type II (n = 5, the mostly involved), and Type III (n = 5, the partly involved). The MRI findings and outcomes of each type were retrospectively analyzed.
Results
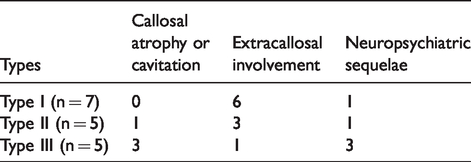
With the reduced range of the callosal restricted diffusion, the callosal atrophy or cavitation was more common: no case of Type I; 1 (20%) case of Type II; and 3 (60%) cases of Type III. With the increased range of callosal restricted diffusion, the extracallosal involvement was more common: 6 (86%) cases of Type I; 3 (60%) cases of Type II; and 1 (20%) case of Type III. During the follow-up, five cases had neuropsychiatric sequelae: 1 (14%) case of type I; 1 (20%) case of Type II; 3 (60%) cases of Type III.
Conclusion
The MRI findings and clinical outcomes of acute MBD are regular. The extensive restricted diffusion of acute MBD may present the curable condition. Callosal heterogeneity may affect the outcome of acute MBD.
Introduction
Marchiafava-Bignami disease (MBD), also known as primary degeneration of the corpus callosum, is a rare alcohol-associated demyelinating disease of the corpus callosum, which can be divided into acute, subacute, and chronic stages according to the clinical process (1). Its acute onset is difficult to capture, and its clinical manifestations are overlapped. Magnetic resonance imaging (MRI) is very useful in the diagnosis of acute MBD (2). In the past, the description of acute MBD was mainly based on case reports, making it difficult to describe its MRI features comprehensively.
Seventeen cases of clinically confirmed acute MBD were included in the present study. The aim of the present study was to analyze the MRI findings in order to provide new insights into the outcomes of acute MBD.
Material and Methods
Clinical data
This retrospective study was approved by the institutional ethics board. Seventeen patients with acute MBD admitted to our hospital from February 2015 to July 2019 were included. All of them were male (median age = 51 years; age range = 33–68 years). They were hospitalized for acute onset of symptoms such as conscious disturbance, limb hypermyotonia, dysarthria, among others. All 17 patients had a history of drinking for 12–45 years, mainly Chinese liquor, with an average daily intake of approximately 250–500 mL, and each of them had had a recent (within 1–2 days) drunken experience before the visit. On admission, their routine biochemical indexes (including routine blood and urine tests, liver and kidney function tests, electrolyte tests, etc.) were all within the normal range.
MRI examinations
By using a 1.5-T MR system (Achieva, Philips Electronics Inc., Netherlands), sagittal T2-weighted (T2W) or T1-weighted (T1W) imaging, axial T1W and T2W imaging, and axial fluid attenuated inversion recovery (FLAIR) and diffusion-weighted imaging (DWI) sequences were performed. Parameters were as follows: spin echo (SE) T1W imaging: TR = 380–500 ms, TE = 8–16 ms; fast spin echo (FSE) T2W imaging: TR = 4200–4500 ms, TE 87.6–98.6 ms; FLAIR: TR = 9002 ms, TE = 133 ms, TI = 2200 ms; DWI adopted SE/EPI sequence scanning: b values = 0 and 1000 s/mm2, TR = 3000–6600 ms, TE = 74–100 ms. The field of view was in the range of 200–240 mm. Slice thickness was 7.0 mm, the interslice gap was 1.5 mm, and the matrix size was 512 × 512 or 256 × 256.
Results
MRI findings of acute MBD
The MRI examinations of the 17 patients displayed the different ranges of restricted diffusion in the corpus callosum and extracallosum, showing hyperintensity on DWI and hypointensity on the apparent diffusion coefficient (ADC) map (Figs. 1a and b, 3a and b). The lesions of the corpus callosum mainly involved the central portion, sparing the ventral and dorsal layers, showing hyperintensity on T2W imaging (Figs. 1d and 2a). Symmetrical restricted diffusion was also detected in the extracallosum, involving the bilateral hemispheric white matter, internal capsule (Fig. 1a–c), and frontotemporal cortices. No significant mass effect was found.
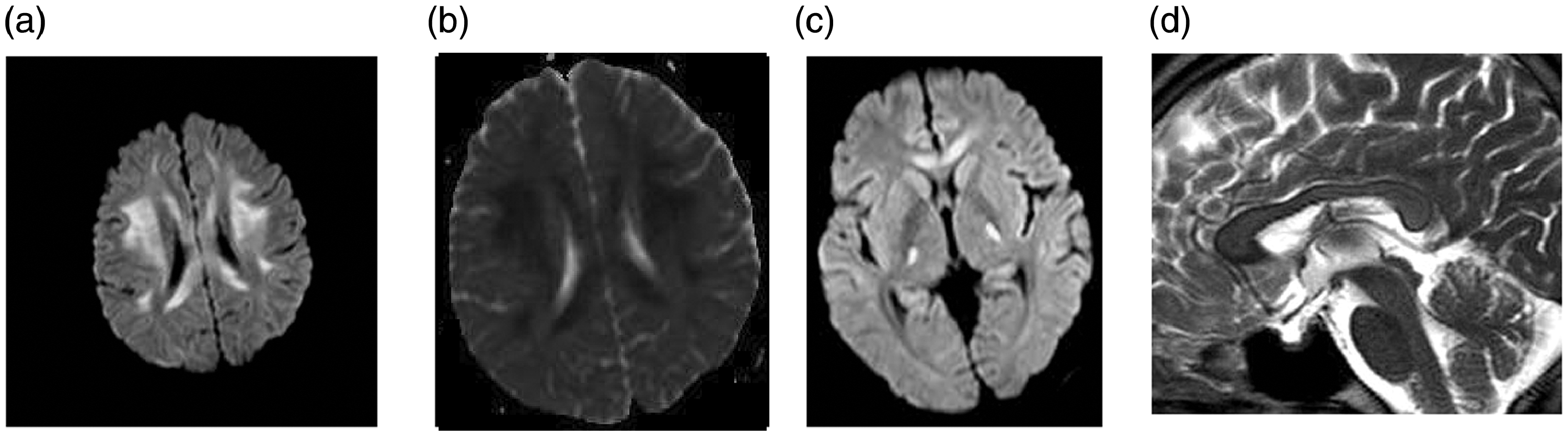
Type I of acute MBD. Axial MRI scans show diffuse swelling of the corpus callosum, with marked hyperintensity on DWI (a) and hypointensity on ADC map (b). The similar lesions are also observed in the bilateral hemispheric white matter (a) and internal capsule (c). Sagittal T2W imaging shows the slight hyperintensity in the central portion of corpus callosum, sparing the ventral and dorsal layers (d). ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; MBD, Marchiafava-Bignami disease; MRI, magnetic resonance imaging; T2W, T2-weighted.
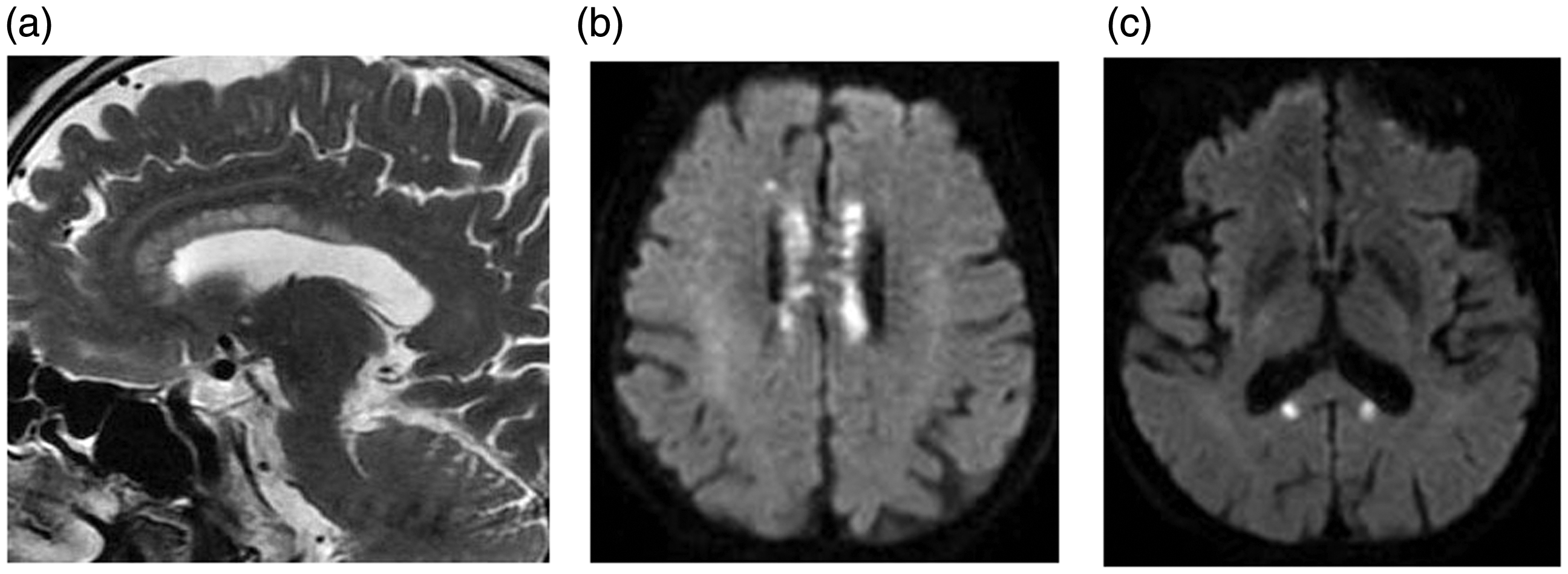
Type II of acute MBD. The genu and body of corpus callosum show the extensive hyperintensity on sagittal T2W imaging (a) and axial DWI (b). Axial DWI also shows the symmetrical punctate hyperintense lesions in the splenium (c). DWI, diffusion-weighted imaging; MBD, Marchiafava-Bignami disease; T2W, T2-weighted.
Classification of acute MBD
According to the different ranges of the callosal restricted diffusion, 17 patients with acute MBD were divided into three types: Type I (n = 7, restricted diffusion involved the entire corpus callosum; Fig. 1); Type II (n = 5, restricted diffusion involved at least two parts of the corpus callosum; Fig. 2); and Type III (n = 5, restricted diffusion involved the single part of the corpus callosum; Fig. 3). With the reduced range of callosal restricted diffusion, callosal atrophy or cavitation was more common (Fig. 3a–c): no case of Type I; 1 (20%) case of Type II; and 3 (60%) cases of Type III. With the increased range of callosal restricted diffusion, extracallosal involvement was more common and more extensive (Fig. 1a–c): 6 (86%) cases of Type I; 3 (60%) cases of Type II; and 1 (20%) case of Type III. The detailed MRI findings of the three types are shown in Tables 1 and 2.
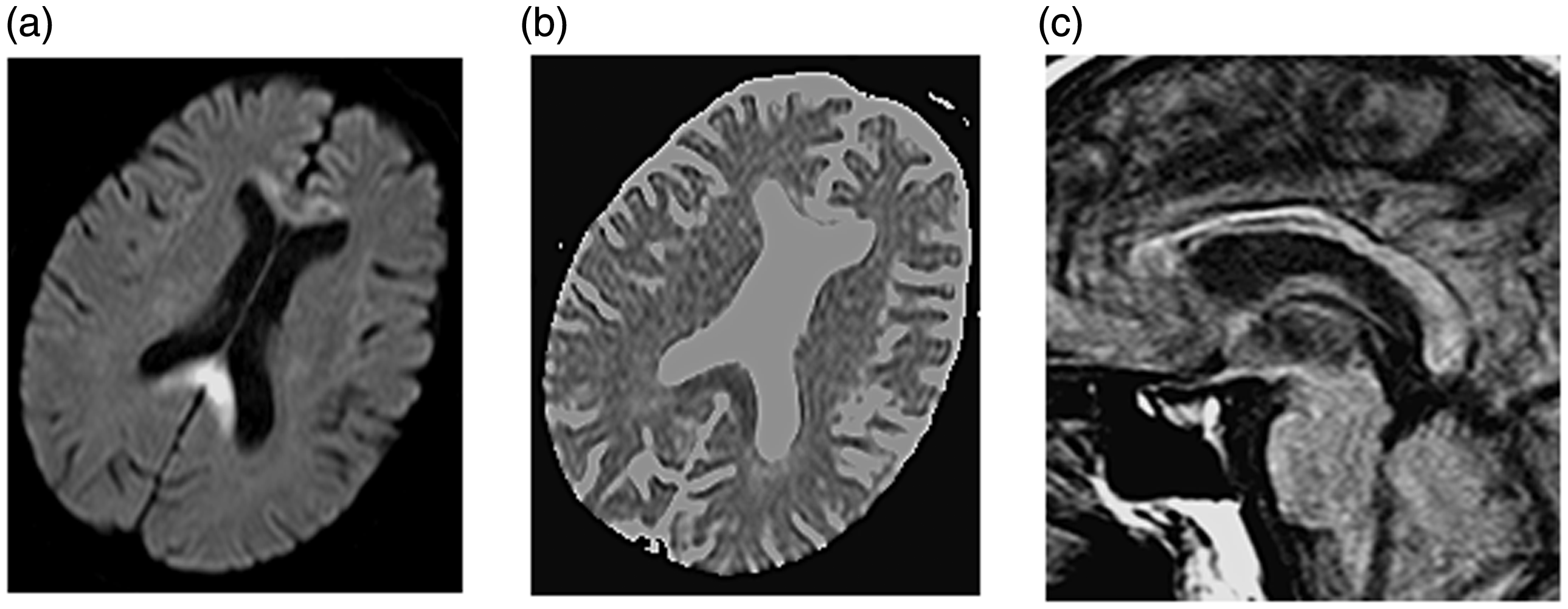
Type III of acute MBD. Axial DWI shows localized hyperintensity in the splenium of corpus callosum (a) with corresponding hypointensity on ADC map (b). In addition, the cavitation in the genu shows iso-hyperintensity on DWI (a) and hyperintensity on ADC map (b). Sagittal T1W imaging shows the callosal atrophy and cavitation, especially in the genu and body of corpus callosum (c). ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; MBD, Marchiafava-Bignami disease; T1W, T1-weighted.
MRI findings and the outcomes of the three types of acute Marchiafava-Bignami disease.
Extracallosal restricted diffusion of the three types of acute Marchiafava-Bignami disease.

*The involvement of bilateral hemispheric matter and internal capsule coexists in Types I and II.
Treatment and prognosis
The diagnosis of acute MBD was determined by the history, clinical manifestations, and MRI findings. All 17 patients met the diagnostic criteria of acute MBD (3,4). After admission, thiamine and methylprednisolone pulse therapies were performed first, followed by prednisone and administration of B complex vitamins. After 2–3 weeks, the 17 patients were significantly improved and discharged from the hospital. All patients were given abstinence measures and clinical follow-up (time range = 1–6 months). Twelve patients had no relapse or sequelae. Five patients still had neuropsychiatric symptoms such as slow reactions, apathy, uncoordinated movement, etc. Among them, three patients were type III with callosal atrophy or cavitation, one patient was type II with callosal atrophy, and one patient was type I with extracallosal lesions. The detailed outcomes of the three types are shown in Table 1.
Discussion
Acute MBD is characterized by an acute onset of conscious disturbance, ataxia, and epileptic seizures. Its etiology and pathogenesis are still inconclusive (5). It is generally believed that nutritional and metabolic disorders caused by chronic alcoholism are the pathogenic basis of MBD, while the onset of acute MBD is likely related to the direct neurotoxicity of the alcohol (6). All 17 patients in this group had a long history of alcohol consumption and had had drunken experiences before the visit. Therefore, on the basis of their long-term drinking histories, the recent drunkenness may have triggered the acute onset of MBD. MBD is one of the cytotoxic lesions of the corpus callosum (CLOCCs), which can cause restricted diffusion of water molecules, myelin swelling, and demyelination (7). According to the different courses of MBD, intramyelinic or cytotoxic edema may play an important role in the early stage. In the later stages, demyelination and necrosis may follow (8,9). The MRI findings of this group are consistent with the pathological manifestation of acute MBD.
According to the clinical symptoms, imaging findings, and prognosis, Heinrich et al. (10) proposed the clinicoradiologic subtypes of MBD in 2004. Type A is characterized by conscious disturbance, seizures and pyramidal signs, with diffuse edema of the entire corpus callosum and poor prognosis. Type B is characterized by cognitive impairment, dysarthria, gait disturbance, signs of interhemispheric disconnection, with partial involvement of the corpus callosum and favorable prognosis. Both types can be subdivided into acute, subacute, and chronic stages. However, the clinical symptoms, imaging findings, and prognosis of MBD are not completely consistent with each other; therefore, this classification is not absolute in this group. First, with the improvement of healthcare, more Type A patients could have a good prognosis (11), just as in this group. Furthermore, the extent of callosal involvement is sometimes difficult to define. For example, in this group, the genu and body of the corpus callosum were diffusely involved, while the splenium of the corpus callosum was localized involvement. Therefore, according to the different ranges of the callosal restricted diffusion, 17 cases of acute MBD were classified into three types. It is more in line with the actual situation in this group.
Alcohol has a direct neurotoxic effect on the brain and results in different degrees of metabolic disorders of the myelin (12). The most abundant amount of myelin is found in the corpus callosum, so it is more vulnerable to MBD, showing selective involvement of the central portion of corpus callosum, with sparing of the ventral and dorsal layers (13). The extent of callosal restricted diffusion were different in this group: Type I cases involved the entire corpus callosum; Type II cases involved at least two parts of the corpus callosum; and Type III cases involved the single part of the corpus callosum.
With the increased ranges of callosal restricted diffusion, the extracallosal restricted diffusion became more common and more extensive. Extracallosal involvement was most extensively in Type I cases, mainly involving the bilateral hemispheric white matter and internal capsule. Type II was next, mainly involving the bilateral hemispheric white matter. Type III was localized involvement, mainly involving the bilateral frontotemporal cortices. This is thought to be the extracallosal involvement of cytotoxic edema via the corpus callosum (14). The corpus callosum is the largest commissural fiber tract, connecting the corresponding cortical areas through callosal radiation, and can intermingle with the bilateral projecting fibers (15). Therefore, extracallosal involvement may depend on the callosal changes. In addition, the extracallosal involvement may be associated with the extrapontine myelinolysis or Morel’s laminar sclerosis (16).
The curative effect of Type I is the best in this group, suggesting that the extensive restricted diffusion is not directly related to the poor outcome (17). Instead, it may present curable conditions. The early cytotoxic edema of MBD has not caused structural damage, so it has potential reversibility. The timing of treatment is the key (18,19). Callosal atrophy or cavitation are more common in Type III cases. It is possible that the old lesions lead to callosal heterogeneity and poor outcome. Moreover, cortical involvement may be another reason (9,19). The outcome of Type II is somewhere in between, just like its MRI findings. We can speculate that the Type I is the pure acute MBD with the extensively homogeneous changes and better outcome, while the Type II and Type III cases are the ones with acute onset on the chronic or subacute basis with the callosal heterogeneity and poorer outcomes, especially the Type III cases. It is possible that MBD is a recurrent and dynamic pathological process that can eventually cause permanent callosal damage, which in turn affects the outcome.
The MRI findings of acute MBD should be differentiated from corpus callosal infarction, Wernicke’s encephalopathy, posterior reversible encephalopathy syndrome (PRES), and multiple sclerosis (MS). Corpus callosal infarction is consistent with the blood supply and the corpus callosum is partly involved. Wernicke’s encephalopathy is also associated with alcoholism, which mainly involves the bilateral medial thalamus, periaqueductal areas, and mammillary bodies (20). PRES is also symmetrical and reversible, but its pathological basis is the vasogenic edema in the areas of posterior circulation (21). MS is characterized by multifocal, multiphasic demyelination. The “vertical sign of lateral ventricle” is typical (22).
In conclusion, MBD may be a dynamic pathological process with the different MRI features and outcomes. The morphological and signal changes of the corpus callosum are characteristic for acute MBD. Additionally, the callosal and extracallosal involvements also have certain regularity. Understanding the diversity of MRI findings of acute MBD is helpful for the early diagnosis and timely treatment. Because of the short follow-up period and small sample size of this group, further study is needed.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.