
Abstract
Background
Patients with talocalcaneal coalitions (TCC) often undergo computed tomography (CT). However, ultrasonography diagnosis of TCC has been seldom done according to the literature.
Purpose
To investigate the accuracy of ultrasonography in diagnosing TCC compared to CT.
Material and Methods
Ninety-seven consecutive patients with a clinical suspicion of TCC were included. Ultrasonography was used to assess the classification and complication of TCC. The main sonographic criteria for a positive diagnosis in cases of osseous coalition were the joint space between the medial surface of talar head and the underlying sustentaculum tali of calcaneus disappearing and being replaced by a continuous hyperechoic bony structure. In cases of fibrous coalition, ultrasonography revealed a reduced space of the joint associated with an irregular, angular appearance of its outline and hypoechoic fibrous tissue inside. These data were compared with CT findings. κ statistic was applied to determine the level of agreement. The sensitivity, specificity, positive and negative predictive values, accuracy, and Youden index of ultrasonography as a diagnostic method were assessed.
Results
Ultrasonography findings were positive in 20 of 97 patients with a clinical suspicion of TCC. The diagnosis was confirmed by CT in 21 patients. There were one false-positive result and two false-negative results by ultrasonography. The κ value was 0.907. The sensitivity, specificity, positive and negative predictive values, accuracy, and Youden index of ultrasonography were 90.5%, 98.7%, 95.0%, 97.4%, 96.9%, and 0.892, respectively.
Conclusion
Ultrasonography could be a reliable, accurate, and non-radioactive diagnostic imaging method in diagnosis of patients with suspected TCC.
Introduction
Talocalcaneal coalition (TCC) represents an abnormal osseous or fibrous connection between the talus and the calcaneus and is one of the main causes of medial ankle pain (1,2). The most common type of TCC involves the medial surface of the talar head and the underlying sustentaculum tali of the calcaneus, while TCC involving the posterior talocalcaneal joint is rarely seen (3). TCC was thought to be first described in 1750 by Buffon. The anatomical nature of TCC was then reported by Zuckerkandl (4). With the advent of X-ray, after Slomann observed tarsal coalition on X-ray in 1920 (5), the radiographic signs and properties of TCC were described in multiple literatures (6). The introduction of computed tomography (CT) and magnetic resonance imaging (MRI) improved the understanding of its anatomic characteristics, and CT/MRI have become the established standard to confirm the diagnosis of TCC (7–9).
High-frequency ultrasonography is a non-invasive, real-time imaging modality and its reliability of ankle examination is generally accepted (10,11). In addition, the value of ultrasonography as a diagnostic tool for ankle pain has been well documented. As far as we know, high-frequency ultrasonography diagnosis of TCC has been seldom done according to the literature. The aim of the present study was to investigate the accuracy of ultrasonography in the diagnosis of TCC compared to CT.
Material and Methods
Between June 2015 and December 2019, 97 consecutive patients (39 men, 58 women; age range = 18–55 years; mean age = 36.2 years) seen at Shandong Medical Imaging Research Institute with a clinical suspicion of TCC were included. The study protocol was approved by the ethics committee of the hospital and all methods were performed in accordance with the relevant guidelines and regulations. All patients enrolled in the study submitted informed consent for participation. All patients presented suspected symptoms and/or signs of the TCC: (i) symptoms: foot pain and discomfort around the hindfoot, with or without a traumatic history of the foot and ankle; and (ii) physical examination: flatfoot deformity with reduction or absence of subtalar motion. Swelling, tenderness, or prominence palpated inferior to the medial malleolus. Patients who had radiological investigation (radiographs, CT, or MRI) before ultrasonography were excluded from the present study.
All patients underwent high-frequency ultrasonography and CT.
The GE Vivid 7, GE Vivid 7 dimension, Philips EPIQ 5, Philips EPIQ 7 ultrasound systems were used in ultrasonography examination. A 18-5 MHz or 12–5 MHz broadband linear array probe was used for ankle examination. Musculoskeletal preset condition was used in all examinations. During the examination, a thick layer of coupling gel or an ultrasound gel pad was applied for better observation result. First, the linear array probe was put on the surface of the medial malleolus, both a static and a dynamic ultrasonography examination with longitudinal and axial sonograms were performed on the joint and periarticular tissues, mainly including coronal position examination over the middle facet of talocalcaneal joint in order to focus on the joint space between the middle facet of the talus and the underlying sustentaculum tali of calcaneus, the adjacent soft tissues including posterior tibial artery, tibial nerve and its branches, flexor hallucis longus tendon, flexor digitorum longus tendon and posterior tibial tendon, etc. Second, color Doppler ultrasound was used in all patients. The main sonographic criteria for a positive diagnosis in cases of osseous coalition were the joint space between the middle facet of the talus and the underlying sustentaculum tali of calcaneus disappearing and being replaced by a continuous hyperechoic bony structure. In cases of fibrous coalition, ultrasonography revealed a reduced space of the middle facet of the talocalcaneal joint associated with an irregular, angular appearance of its outline and hypoechoic fibrous tissue inside. Attention should be paid to determine their classification. Comparison scanning was performed on the contralateral ankle as the control.
CT images were acquired subsequently (SOMATOM Force, Siemens Medical Solution, Germany). The scanning parameters were as follows: slice thickness =1.0 mm; pitch = 0.8; collimation = 0.6 mm; and reconstruction interval = 0.7 mm. The axial, coronal, and sagittal reconstructed images focusing on the talocalcaneal joint and the adjacent soft tissues were evaluated via 3D reconstruction, including multiplanar reformation, maximum intensity projection, and volume rendering.
All the ultrasound examinations were performed by an experienced ultrasound expert with > 11 years of experience in ankle ultrasound examination. All the CT examinations were performed by a senior musculoskeletal technician who had 10 years of experience in CT.
Ultrasonography and CT images of the cases in the picture archiving and communication systems (PACS) system were all assessed by two musculoskeletal radiologists blinded to the clinical diagnosis independently, with more than 10 years of imaging diagnosing experience in interpreting ultrasound and CT examination results. Reference to original imaging reports was shielded to avoid bias.
The SPSS program (version 25.0, SPSS Inc., Chicago, IL, USA) was used for statistical analysis. The level of agreement between ultrasonography and CT was determined by kappa test. Sensitivity, specificity, positive and negative predictive values, accuracy, and Youden index of ultrasonography were obtained.
Results
The inferior medial surface of the talar head and the underlying sustentaculum tali of calcaneus form a part of the talocalcaneonavicular joint (12), which is often involved in TCC. Ultrasound can assess the medial outline and the space of the joint (13). A normal joint appears as a hyperechoic upside-down triangle, filled with adipose tissue inside the articular cavity. The borders of the inferior medial surface of the talar head and the sustentaculum tali of calcaneus are smooth and separated from each other. The joint space is clear and there is no bony or fibrous structure (Fig. 1).
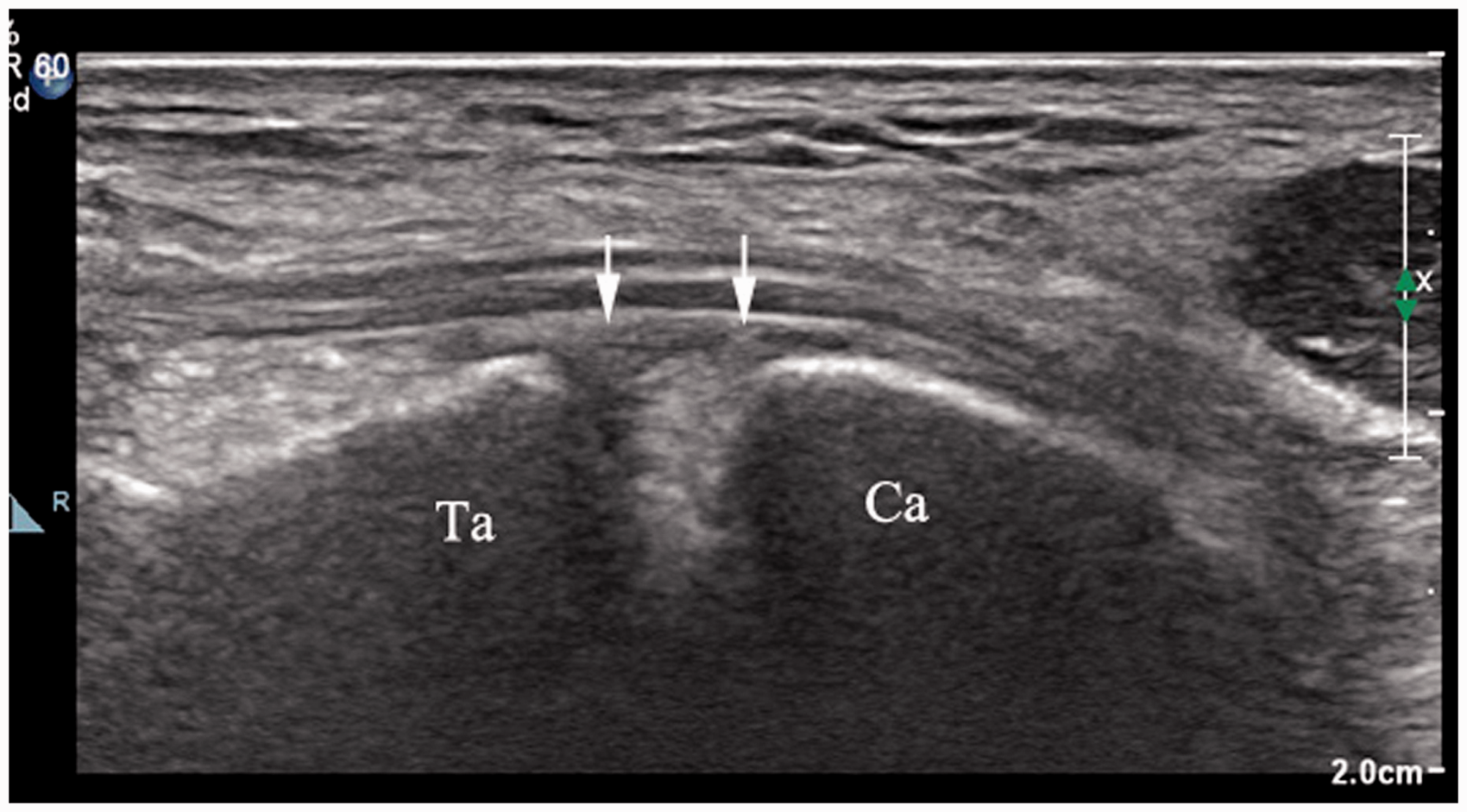
Normal talocalcaneonavicular joint. High-frequency ultrasonography image of the talar (Ta) and calcaneus (Ca) in the coronal plane. Note the hyperechoic adipose tissue inside the articular cavity. The borders of the inferior medial surface of the talar head and the sustentaculum tali of the calcaneus are smooth and separated from each other (arrow).
Of the 97 patients with a clinical suspicion of TCC in the present study, ultrasonography showed positive results for TCC in 20 patients and negative results in 77 patients. There were 15 patients with unilateral involvement and five patients with bilateral involvement (both sides were of the same type). In terms of type distribution, ultrasonography revealed 12 cases of osseous coalition and eight cases of fibrous coalition. In cases of osseous coalition, the joint space between the medial surface of the talar head and the underlying sustentaculum tali of calcaneus disappeared and was replaced by a smooth continuous hyperechoic bony structure, followed by acoustic shadow (Fig. 2). Among the 12 cases, five were complicated with local compression of tibial nerves or their branches (usually medial plantar nerves), which showed that the nerve was compressed and narrowed near the TCC. Ultrasonography also found that the proximal part of the nerve was thickened, the echo was decreased, and the structure of perineurium was not clear (Fig. 3). When the dynamic examinations were carried out in five patients, during both active and passive movements of the ankle or compression through the probe, local pain and plantar numbness occurred. In cases of fibrous coalition, the inferior medial surface of the talar head and the underlying sustentaculum tali of the calcaneus appeared as irregular and angular. Instead of a clearly joint space, ultrasonography revealed a reduced space of the joint and hypoechoic fibrous tissue inside (Fig. 4). There were two cases with tibial nerve compression among them. In addition, ultrasonography revealed compression and displacement of a flexor hallucis longus tendon and a flexor digitorum longus tendon, respectively. The involved tendon was thickened. The tendon sheath was hyperemia and contained a pathological amount of fluid, respectively.
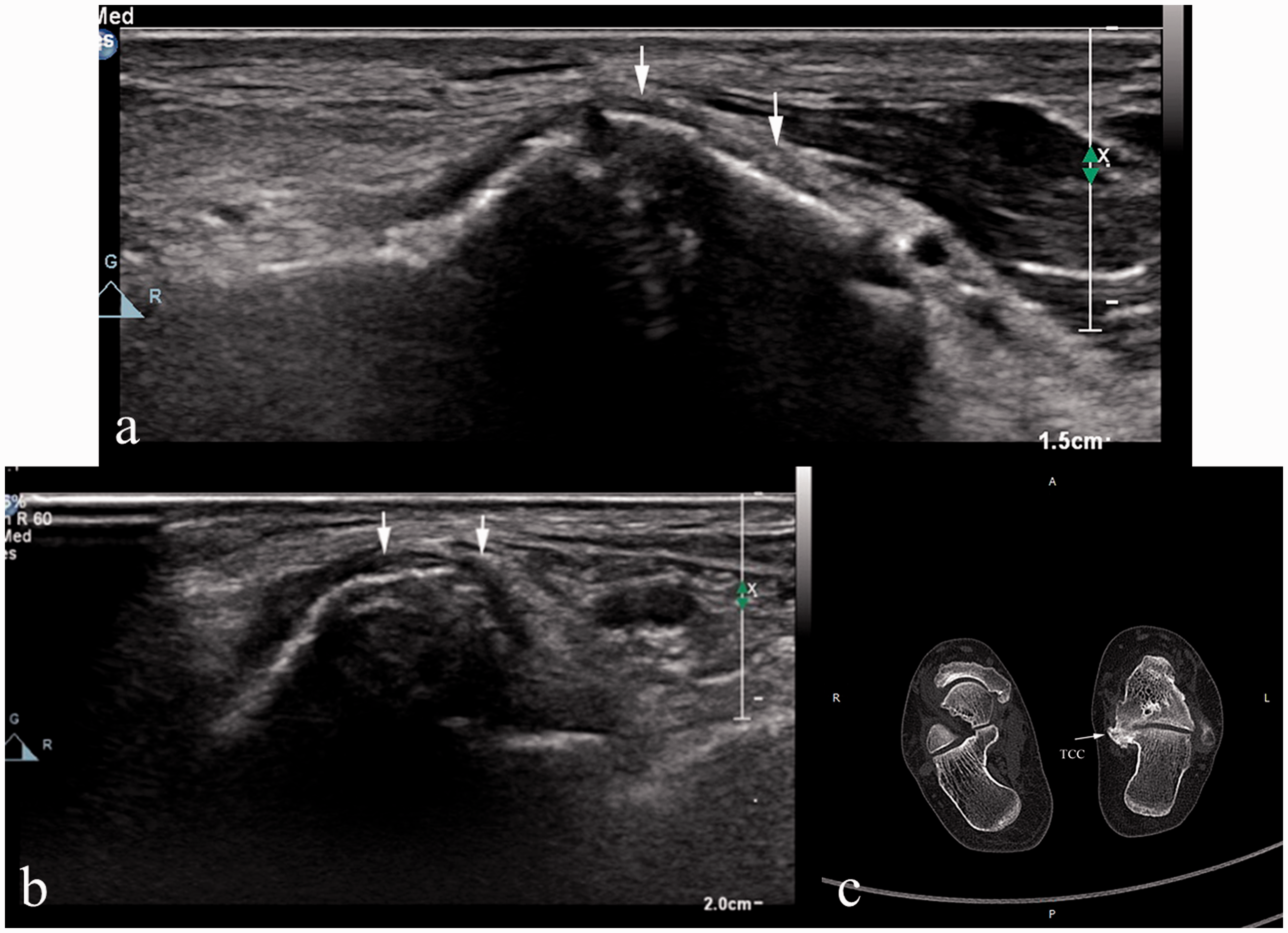
High-frequency ultrasonography image of an osseous TCC (arrow) in the longitudinal plane (a), transverse plane (b), and MPR (c). Ultrasonography shows the joint space between the medial surface of the talar head and the underlying sustentaculum tali of the calcaneus has disappeared and been replaced by a hyperechoic bony structure, followed by acoustic shadow, which is in line with the findings of the computed tomography image. MPR, multiplanar reformation; TCC, talocalcaneal coalition.
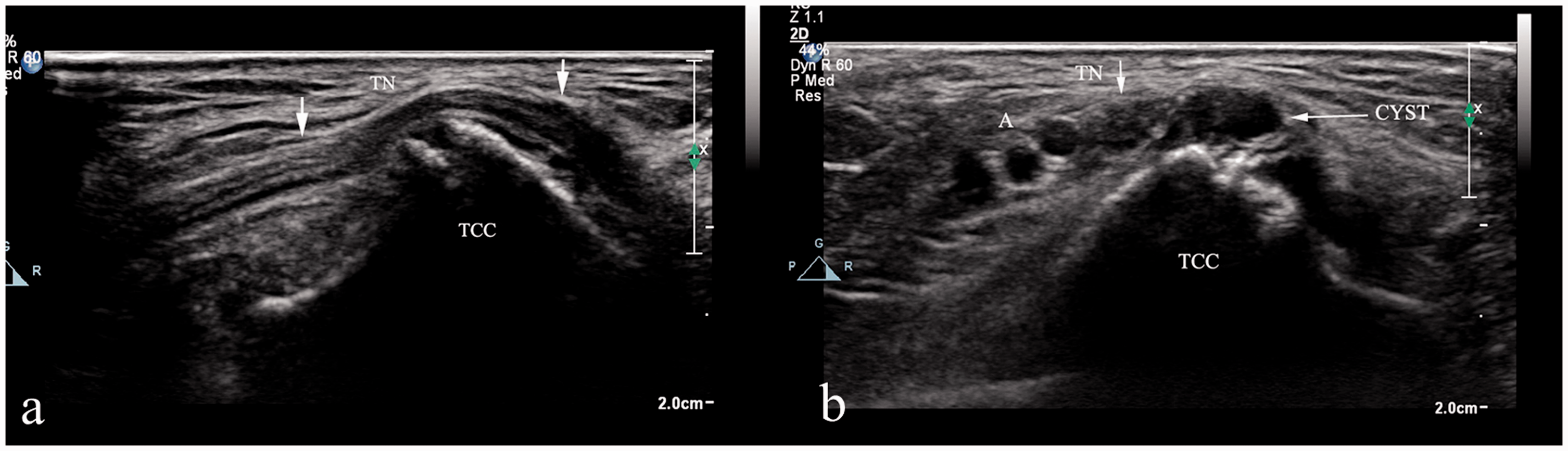
High-frequency ultrasonography image of an osseous TCC in the longitudinal plane (a) and transverse plane (b) with local compression of the TN. Ultrasonography shows the nerve is compressed and narrowed near the TCC and the proximal part of the nerve is thickened, the echo is decreased, and the structure of perineurium is not clear. In addition, ultrasonography also reveals a synovial cyst on the surface of the TCC. TCC, talocalcaneal coalition; TN, tibial nerve.
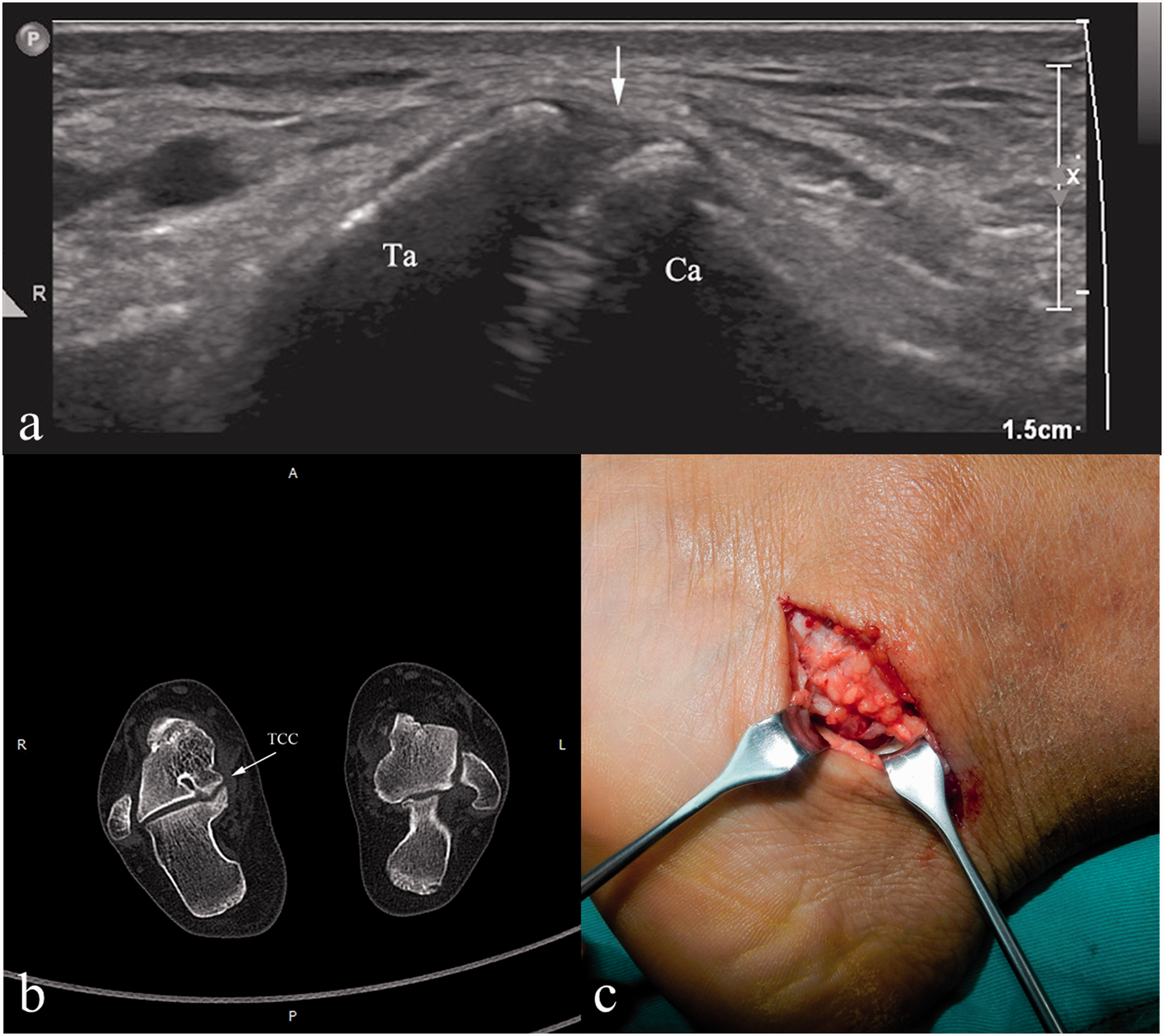
High-frequency ultrasonography image of a fibrous TCC in the longitudinal plane (a), MPR (b), and intraoperative findings (c). The inferior medial surface of the talar head and the underlying sustentaculum tali of the calcaneus appear as irregular and angular. Instead of a clearly joint space, ultrasonography reveals a reduced space of the joint and hypoechoic fibrous tissue inside, which is consistent with computed tomography and intraoperative findings. MPR, multiplanar reformation; TCC, talocalcaneal coalition.
Diagnosis using CT was positive for TCC in 21 patients and negative in 76 patients, with 16 patients with unilateral involvement and five patients with bilateral involvement (both sides were of the same type). As to the type distribution, CT found 12 cases of osseous coalition and nine cases of fibrous coalition. In addition, CT can obtain more details of TCC, such as the morphology and extent of TCC. In one patient (patient 17), CT diagnosed the medial talus fracture which was not found by ultrasonography.
Compared with CT, there were one false-positive result and two false-negative results by ultrasonography. Detailed ultrasonography findings in each patient are shown in Table 1. Results comparing CT and ultrasonography are shown in Table 2.
The ultrasonography examination results of talocalcaneal coalition.
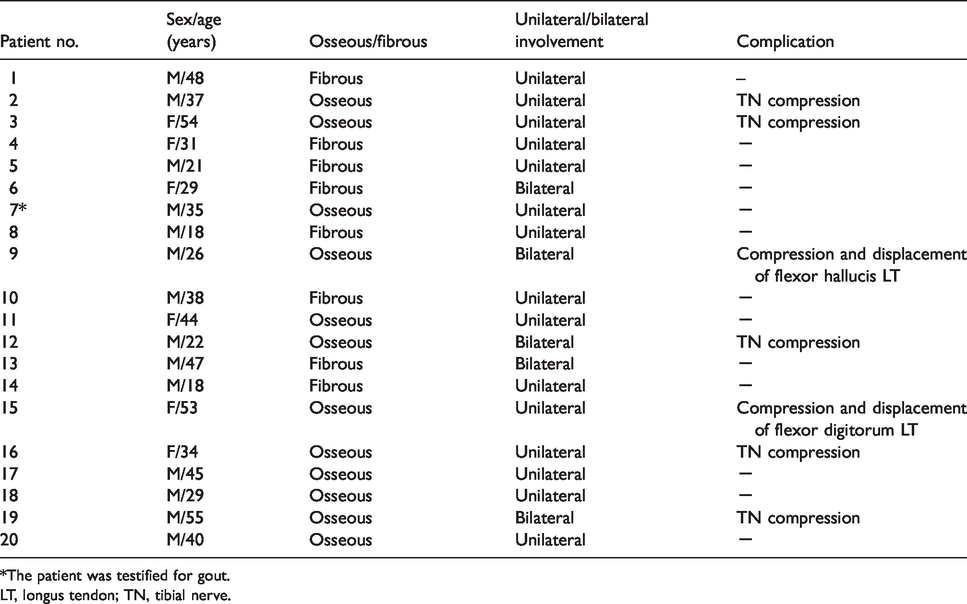
*The patient was testified for gout.
LT, longus tendon; TN, tibial nerve.
Comparison of results: ultrasonography and CT.
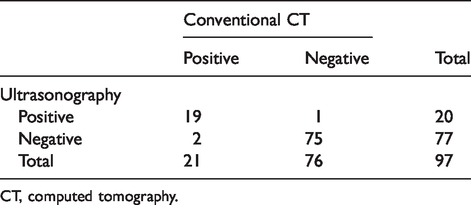
CT, computed tomography.
All patients with a negative ultrasonography diagnosis presented negative findings on CT except for two patients. The main reason lies in the inadequate understanding of the disease and the lack of accurate evaluation of the echo changes in the joint space, which were testified by CT. One patient (patient 7 in Table 1) with a positive diagnosis on ultrasound was finally proved to be gout, not TCC.
Analysis of internal validity parameters of ultrasonography as a diagnostic test for TCC showed a sensitivity of 90.5%, specificity of 98.7%, a positive predictive value of 95.0%, and a negative predictive value of 97.4%. The overall accuracy was 96.9%. The Youden index of ultrasonography was 0.892. The κ level of agreement between CT and ultrasonography for TCC was 0.907 (high level; Table 3).
κ statistics between conventional CT and ultrasonography.
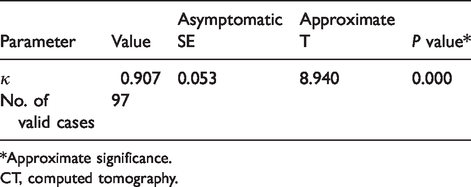
*Approximate significance.
CT, computed tomography.
Discussion
TCC refers to the abnormal connection between the talus and calcaneus with a prevalence of about 1%, which is underestimated according to the literature (14). All three talar surfaces for the calcaneus (anterior, middle, and posterior talar articular surfaces) may be affected. However, the medial surface of the talar head and the underlying sustentaculum tali of the calcaneus are the most commonly involved (15). There are two theories about the formation of TCC. One is that TCC is an embryogenetic defect characterized by failed segmentation of the primary mesenchyme or failed joint cleft development between calcaneus and talus (16). Another theory holds that it is an acquired disease and its main causes are traumatic fracture and infection, which lead to the injury of the joint, the formation of micro callus, and finally the formation of TCC. At present, the former theory is accepted by most scholars. TCC is usually associated with medial ankle pain that exacerbates with exercise. During the physical examination, flatfoot deformity with reduction or absence of subtalar motion is often found. Sometimes TCC may compress the tibial nerve and result in a positive Tinnel sign with paresthesia of the forefoot.
Various imaging techniques can be used in patients with a clinical suspicion of TCC, such as X-ray, ultrasonography, CT, and MRI. X-ray has been the first choice in the past. The C sign is the most commonly used sign for the diagnosis of TCC, according to the literature (6). However, Taniguchi et al. (7) reported the low sensitivity (49%) of the C sign for TCC, which indicated that an absence of the C sign does not negate a diagnosis of TCC. Nowadays, the evaluation of TCC can be made in detail when spiral CT is used. The axial, coronal, and sagittal reconstructed images and 3D reconstruction (multiplanar reformation, maximum intensity projection, and volume rendering) can provide valuable information regarding the type, morphology, and extent of TCC, which is helpful in its diagnosis and treatment (17). In addition to being able to show the shape of TCC, the advantage of MRI lies in its high signal sensitivity, which allow the sensitive evaluation of bone marrow and soft tissue, including bone marrow edema associated with TCC and tarsal tunnel soft-tissue abnormalities affecting TCC (the flexor hallucis longus tendon, flexor digitorum longus tendon and posterior tibial tendon, as well as the tibial nerve and its branches) (9). Although CT and MRI can visualize the type, morphology, and extent of TCC, CT is a radioactive examination and cannot evaluate the adjacent soft tissue, such as the compression of tibial nerve and the structure of perineurium, while MRI is time-consuming, stressful, and complicated. Ultrasonography is not only a radiation-free and convenient method of diagnostic imaging with excellent resolution of soft tissue from which confirmation can be obtained immediately, it also allows dynamic evaluation through active or passive movements of the subtalar joint or compression through the probe to trigger symptoms to get more concrete conclusions no other tests could. Furthermore, it is well-known that ultrasonography is a more affordable screening choice when compared to CT/MRI (18).
Nevertheless, ultrasonography had certain limitations. An unavoidable problem is operator dependence, which requires ultrasound doctors to strengthen the study of ankle anatomy and improve the understanding of the disease. Furthermore, due to the complexity of ankle anatomy, ultrasound can only display the partial section imaging of TCC and cannot provide information regarding the overall morphology and extent of TCC. Therefore, ultrasonography is inferior to CT in demonstrating the overall view and the accuracy of local bone structure abnormalities is lower than that of CT. Despite the above-mentioned limitations, the advantage of ultrasonography is that it is more sensitive and accurate in showing soft tissue compared to CT, such as when demonstrating the compression site and degree of tibial nerves or their branches. In addition, comparison scanning could also be performed on the contralateral side as a control. Moreover, under the guidance of ultrasound, we can make marks on the skin surface to determine the exact compression site, so as to provide help for accurate surgery. Last but not least, as ultrasonography is a less expensive examination and it can be used as a tool to monitor the changing process of patients with TCC adopting conservation treatments. Thus, it provides a reliable, non-radioactive, and convenient method of imaging in the diagnosis and follow-up of patients with TCC.
As to the treatment of TCC, asymptomatic patients only need close follow-ups as there is no evidence suggesting that asymptomatic TCC may lead to future problems, according to the literature (19). For symptomatic patients, clinical physicians recommend either conservative or surgical treatment mainly based on the type and severity of symptoms. The aim of conservative treatment is to limit range of motion of the subtalar joint so as to relieve or even eliminate pain. Conservative treatments include selection of suitable shoes, fixed in a neutral or slight varus position, and anti-inflammatory agents (20). Further, all symptomatic patients should receive a series of strict conservative treatment for at least six months before any surgical treatment (14). For patients with persistent pain, dysfunction, and failure of conservative treatment, surgery would be more appropriate (2). Surgical treatments include resection of the coalition and subtalar joint arthrodesis, among others (21).
Although the gold standard for diagnosis of TCC is CT, the present study has shown that ultrasonography is useful in diagnosing TCC because of its high accuracy as a diagnostic test (96.9%) compared with the accuracy of CT. There is also a high level of agreement between both tests (k = 0.907). Therefore, in patients with typical symptoms and positive ultrasonography findings, a reliable diagnosis can be reached.
In conclusion, high-frequency ultrasonography may provide important imaging evidence for the diagnosis, treatment, and follow-up in patients with TCC. To the best of our knowledge, this is the first study to identify the accuracy of ultrasonography in diagnosis of TCC. It is a reliable, accurate, and non-radioactive examination in the assessment of patients with suspected TCC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Shandong Provincial Key R&D Program (2019GSF108271), PR China; Shandong Provincial Natural Science Foundation (ZR2019PH086), PR China; and the Shandong Provincial Medical Science and Technology Development Program (2017WS609), PR China.