
Abstract
Background
Preoperative portal vein embolization (PVE) is performed to induce hypertrophy of the future liver remnant enabling major liver resection in patients with various types of liver tumors.
Purpose
To evaluate safety and effectiveness of PVE with n-butyl-cyanoacrylate (NBCA).
Material and Methods
All consecutive patients referred to our hospital for PVE between July 2006 and July 2017 were retrospectively reviewed. Volumetry was performed on computed tomography images before and after PVE, segmenting the total liver volume and the future liver remnant (FLR), i.e. liver segments I–III.
Results
PVE was performed in 46 patients (18 women, 28 men; mean age = 61 years) using local anesthesia. The ipsilateral technique was used in 45 patients. Adverse events were rare. The mean FLR volume increase was 56%, the degree of hypertrophy was 9.7%, and the kinetic growth rate was 2.1%/week. The median ± SD period between PVE and liver surgery was 7 ± 3 weeks. Forty-two patients (91%) had surgery; liver resection was performed in 37 (80%) patients. Three patients (7%) developed transient liver failure after surgery. There was no 90-day post-PVE or postoperative mortality.
Conclusion
PVE using NBCA through the ipsilateral approach in local anesthesia is safe and effective in inducing hypertrophy of the future liver remnant enabling surgery, and thereby increasing survival in patients with liver tumors.
Keywords
Introduction
Patients planned for potentially curative major liver resection due to primary or metastatic tumors may risk postoperative liver failure if the future liver remnant (FLR) is too small. First described in a human in 1986 (1), portal vein embolization (PVE) has since developed into a minimally invasive preoperative procedure (2). Several studies have proven PVE to be safe and effective for inducing hypertrophy, allowing patients with borderline resectability to become resectable (3–7). PVE induces similar volume increases regardless of underlying malignancy (8), decreasing the risk of postoperative liver insufficiency, the main cause of death after major hepatectomy (7,9–11).
Indication for PVE is an FLR volume ≤20% of the total liver volume (TLV) in patients with an otherwise normal liver, an FLR volume ≤30% of TLV in patients who have had preoperative chemotherapy, and an FLR volume ≤40% of TLV in patients with hepatic cirrhosis or fibrosis (7,12).
Several embolic agents have been used to increase the size of the FLR: n-butyl cyanoacrylate (NBCA); coils; polyvinyl alcohol; fibrin glue; microspheres; gelatin sponge; ethanol; and sclerosants (4). Percutaneous transhepatic access into the portal system can be achieved either through the part of the liver that is to be embolized (and future on resected), the ipsilateral technique, or through the part that is not embolized, i.e. the FLR, the contralateral technique. PVE is usually performed under sedation using local anesthesia or sometimes under general anesthesia (12).
The aim of the present study was to evaluate the effectiveness and safety of PVE using NBCA.
Material and Methods
Patient population and data
After approval from the regional ethical review board of Uppsala University (Etikprövningsmyndigheten, approval no. 2019-0097), all consecutive patients who were referred for PVE to our university hospital between July 2006 and July 2017 were identified. Written informed consent was obtained from patients who were alive, after which medical records, the radiology information system, abdominal computed tomography (CT) and magnetic resonance imaging (MRI) scans, and portal venography were retrospectively reviewed. The FLR was defined as segments I–III based on the preoperative planning of potential extended right-sided hemihepatectomy.
Liver volumetry
Liver volumetry was performed on contrast-enhanced CT or MRI images on all patients using the most recent scan before PVE, and the post-PVE scan closest to the date of surgery. The TLV and the FLR were manually traced on transversal images with a semi-automatic segmentation tool (Carestream Vue PACS Version 12.2.2.0105, Carestream, Rochester, NY, USA). The middle hepatic vein, the portal vein, the falciform ligament, and the gallbladder were used as markers to define the borders between the right and the left lobes of the liver and the borders of segment IV from segment II–III.
Hypertrophy response
The percentage FLR (FLR%) was calculated both from the absolute TLV using volumetry data for FLR and TLV, and from the total estimated liver volume (TELV) (4,13) using volumetry data for FLR and TELV calculated using the body surface area (BSA) according to Mosteller (14). All hypertrophy calculations were done based on both TLV and TELV.
FLR% volume increase was calculated as: FLR % volume increase = (FLR %post-PVE–FLR %pre-PVE)/(FLR %pre-PVE) *100 (4).
The degree of hypertrophy (DH) was calculated as: DH = FLR %post-PVE- FLR %pre-PVE.
The kinetic growth rate (KGR) was calculated as: DH/time elapsed since PVE in weeks.
PVE procedure
All patients were inpatients who had received oral pre-medication with analgesics and sedatives. PVE procedures were performed by experienced interventional radiologists under local anesthesia. Ultrasound-guided percutaneous transhepatic puncture of an ipsilateral portal vein branch was performed and a 5-Fr sheath was inserted. With fluoroscopic guidance, the right portal branches were catheterized with a 0.035-inch guidewire. Embolization was performed through a 4-Fr catheter. Procedure time was defined as the time from the first to the last portal venography, which was the only recorded time.
Statistics
Statistical analyses were performed using SPSS software version 23 (IBM SPSS Statistics for Windows, Version XX, IBM Corp., Armonk, NY, USA). Comparisons were performed using Pearson’s correlation for continuous data and the chi-square test for categorical data. The difference in survival between patients in whom surgical resection had, or had not, been performed was estimated using the independent Student’s t-test. Predictors of left lobe hypertrophy and of survival were searched for using logistic regression models. The significance level was set at 0.05 in all analyses.
Results
PVE was attempted in 47 patients. In one patient, PVE was not performed because of severe pain at first puncture and subsequently the treatment strategy was altered. Effectiveness and safety of PVE were studied in the remaining 46 patients (18 women, 28 men; mean age = 61 years; age range = 31–79 years). The median follow-up time after PVE was 38 months (range = 8 months–12 years). Patient characteristics are displayed in Table 1.
Patient characteristics.
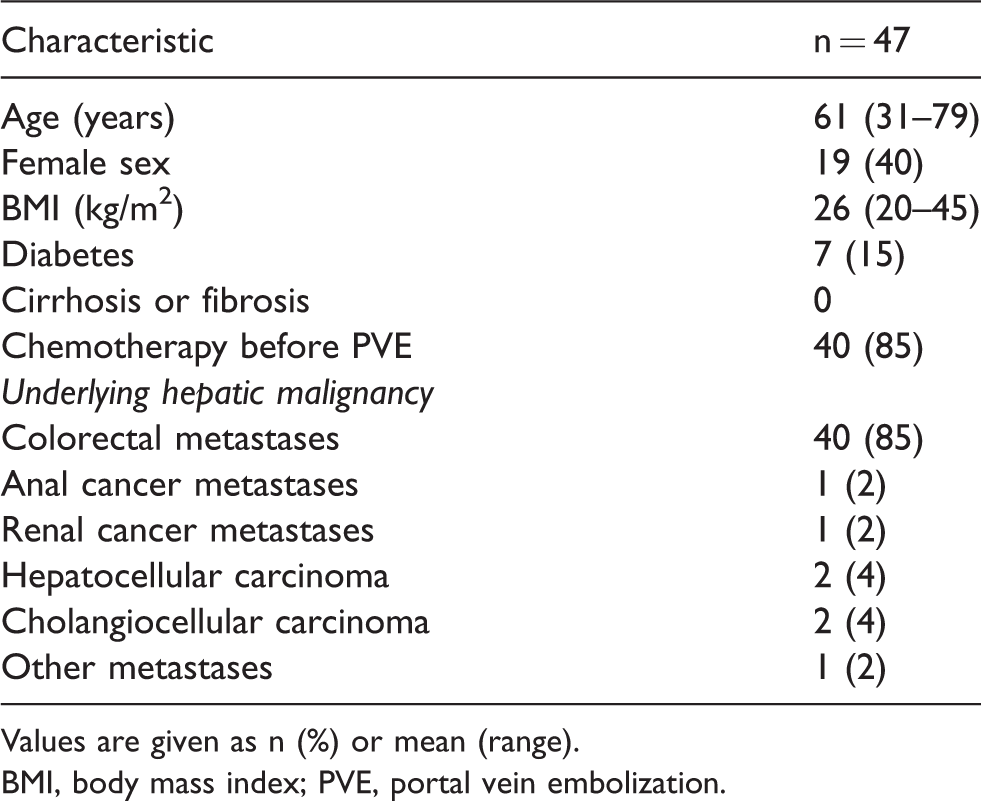
Values are given as n (%) or mean (range).
BMI, body mass index; PVE, portal vein embolization.
The mean pre-PVE volume of the FLR was 19% of TELV (Table 2). Three patients had biliary stasis before PVE, one of them had a drainage.
Volumetric data of the FLR.

Values are given as mean ± SD (range).
DH, degree of hypertrophy; FLR, future liver remnant; KGR, kinetic growth rate; PVE, portal vein embolization; TELV, estimated total liver volume; TLV, total liver volume.
PVE procedure
The ipsilateral approach was used in all cases except one where the entire right lobe consisted of tumor. All primary PVE procedures were performed using local anesthesia, targeting the right portal vein using the embolic agent NBCA mixed with Lipiodol. In two patients, coils were added. Reintervention was performed in one patient under general anesthesia. That patient had an anatomic variant where branches from the left portal vein supplied segments V and VIII. These were coiled at reintervention together with the branch to segment IV after which the patient could proceeded to surgery. In one more patient segment IV was embolized, also with coils.
The mean procedure time was 39 min (range = 12–96 min). On the post-PVE portal venography, all right portal branches were occluded in all patients.
Hypertrophy
The mean time interval between PVE and the follow-up CT scan was 4.7 weeks (range = 1–10 weeks). The liver volumetric data before and after PVE are presented in Table 2. Three patients were not included in the TLV calculations since there was a massive tumor burden in the right lobe making the calculations unreliable. One patient was not included in the TELV calculations since there were no weight measurement.
On follow-up CT, parts of the right portal vein were patent in 12 (26%) patients. In six of these, and in an additional two, embolic material had not reached all segments of the right liver lobe. There was no correlation between the DH and whether there was presence of open segments in the right lobe on the follow-up CT (P = 0.058).
Two patients were found to have new metastases in segment IV on follow-up CT but there was no significant increase in the size of the metastases in segment IV in the total cohort.
Liver surgery
Of the patients, 42 (91%) had liver surgery. Four patients were excluded from liver surgery: one who had progress of a thrombosis and an insufficient growth of the FLR and another three patients due to tumor progression.
The median period between PVE and liver surgery was 7 ± 3 weeks. The mean operation time was 3 h 34 min (range = 59 min–8 h 6 min). Five surgeries (12%) were aborted due to tumor progress. Two patients only had resection of segments VI–VII, one due to extensive chemotherapy-induced steatosis and one who had had a previous partial resection in the left lobe. Four patients had right-sided hemihepatectomy and the remaining 31 patients had extended right-sided hemihepatectomy.
Adverse events
PVE could not be performed in one patient because of severe pain at first puncture as mentioned above.
In another patient there was a periprocedural PVE complication: leakage of NBCA into the left portal branch causing a local thrombosis. This was treated with mechanical and pharmacological thrombectomy during the same procedure, and systemic anticoagulants after PVE. There was no thrombosis on follow-up CT and the patient underwent the planned liver surgery.
The post-PVE and postoperative complications are listed in Table 3.

Values are given as n (%) or mean hospitalization time.
PMV, portomesenteric vein; PVE, portal vein embolization; SIR, Society of Interventional Radiology; SMV, superior mesenteric vein.
The patient who had a subcapsular abscess after PVE was treated successfully with drainage and antibiotics. The patient who had a pleuropneumonia one week after the procedure was treated with antibiotics. The patient who got a partial portomesenteric vein thrombosis had a partial resection of segments VI–VII because of extensive chemotherapy-induced steatosis. The patient who had a small thrombosis of the superior mesenteric vein (SMV) before PVE that progressed to the main trunk of the portal vein after the procedure had an insufficient growth of the FLR and was excluded from surgery.
The patients who had postoperative pleural or abdominal fluid collections were successfully treated with drainages, the patient who had bile leakage was treated with percutaneous transhepatic cholangiography (PTC), and the patients who had bleedings or wound rupture had re-surgery.
Elevations in liver enzymes and S-bilirubin after PVE and surgery were transient. (Table 4) Three patients had transient postoperative liver failure defined according to the 50–50 criteria (15).
Laboratory parameters before and after PVE and liver surgery.

Values are given as mean (range).
*Significantly different from preoperative value.
†Data only available from nine patients.
AST, aspartate transaminase; ALT, alanine transaminase; INR, international normalized ratio; PT, prothrombin time; PVE, portal vein embolization.
Survival
There was no post-PVE or 90-day postoperative mortality. Patients in whom surgical resection was performed (n = 37) survived significantly longer (mean =42 months) than those in whom no surgery or only explorative laparotomy was performed (n = 9: mean survival = 17 months; P = 0.022). There was no correlation between the S-bilirubin, DH, or the KGR and overall survival.
The four patients who had PVE but no liver surgery had a mean survival of 10 months (range = 5–16 months) after PVE.
There were no sex-specific differences in the growth of the FLR or in whether liver resection was performed.
Discussion
Of the patients, 91% had enough FLR hypertrophy to undergo the planned liver surgery, consistent with previous reports (4,6,16–18) and guidelines (19). Three patients (7%) did not undergo liver surgery due to tumor progress on follow-up CT and surgery was aborted in another 5 (12%) patients due to perioperatively discovered tumor progress, consistent with previous studies (4,6,16,17). The frequency of liver failures (7%) in the present study is consistent with other reports (4%–10%) (16,17,20,21), and so is the frequency of major postoperative complications (4,6,16,22).
Of the adverse events after PVE, the minor complications were expected side effects (19). Major complications were rare and did not affect the patients’ planned surgery except for in one patient. In this patient, an already existing thrombus progressed, and the patient had an insufficient growth of the FLR and was excluded from surgery. Even though the thrombus was partial and had dissolved on ultrasound one month later, it may have reduced the blood flow to the FLR and thereby limited the hypertrophy. Generally, a small thrombus in the SMV is not considered a contraindication to PVE (5,23). However, anticoagulant medication and frequent follow-up might be needed. Another two patients in the present study had thrombotic events but their hypertrophy was sufficient for them to proceed to surgery.
The four patients who had PVE but no liver surgery had a mean survival of 10 months after PVE, consistent with expected survival on best supportive care (24,25). The observation that patients in whom surgical resection was performed survived twice as long as those in whom no surgery or only explorative laparotomy had been performed probably reflects different tumor biology and aggressivity. However, the observation that PVE did not entail any complications in the patients who for other reasons did not complete liver surgery supports the use of PVE to enhance the possibility of liver resection. Furthermore, a recent study reports that PVE is not associated with increased postoperative complications (26).
The mean FLR% volume increase varies between 38% in cohorts with varying embolic material (4) and 49%–52% when only NBCA as was used (6,27). This is consistent with the present study with a mean FLR% volume increase of 56%.
The mean DH of 9.7% (16,17,20,22,28) and KGR of 2.1%/week (16,20,28,29) in the present study is consistent with previous studies. No correlation was observed between DH and mortality in the present study, even though others have seen correlations with DH and post-hepatectomy outcomes (20). The patient who only had a DH of 0.5% mostly had hypertrophy of segment IV. Thus, in this patient segment IV was not resected and, except for the right-sided hemihepatectomy, only small resections made in segments II–III.
KGR < 2%/week has been reported to be a better predictor of postoperative morbidity and mortality than DH or FLR based on TELV (16). One study reports no liver failures in patients with KGR > 2.66%/week and suggests that KGR could be an early marker supporting surgery to be performed sooner than customary (20). This could not be confirmed by the results of the present study where the mean KGR was 2.1%/week, and the KGR was 2.6%/week in one of the patients who had transient liver failure. These observations could partly be explained by the rather long time interval (mean = 4.7 weeks) between PVE and the follow-up CT, since a recent study reports that KGR is highest the first week after portal vein occlusion and then decreases over time due to a non-linear pattern of growth of the FLR (30).
There are studies suggesting that previous chemotherapy has no significant effect on liver regeneration after PVE (31,32). This is supported by our observations since most patients in our cohort had chemotherapy before PVE and still 91% of the patients were accepted for liver surgery.
Because embolizing segment IV entails a higher risk of injuries and non-target embolization of the FLR, this is not routinely performed at our center (31,33). Despite that, there was enough hypertrophy of the FLR to proceed to surgery. In a recent retrospective study, there was no difference in survival between PVE patients in whom segment IV was or was not embolized, even though there was a significant increase in DH in those where segment IV had been embolized (17). In another recent study, they could not detect any increase in DH but an overall FLR% increase when embolizing segment IV compared to not embolizing it (28). Thus, segment IV might not need to be embolized routinely. Instead, a rapid evaluation of growth can be performed to detect patients in need of additional embolization. However, in patients with a very small FLR, embolization of segment IV could be considered at the primary PVE session.
A concern with PVE is that the tumors in the non-embolized segments would increase in size (34,35), even in patients where chemotherapy has been given (18,36). In our cohort, there was no significant increase in the size of the metastases in segment IV, although two patients were found to have new metastases in segment IV on follow-up CT.
The results of the present study confirm that PVE with NBCA results in adequate hypertrophy and resection rates with a low rate of PVE complications. The ipsilateral technique was used to minimize complications such as thrombosis or vascular injuries of the FLR (23). A few other studies have reported embolization with NBCA through an ipsilateral approach (4,29) and proved it safe and effective (29). All primary PVE procedures were performed in local anesthesia without any related complications. Local anesthesia was preferred because of its logistic advantage and to avoid any potential risks of general anesthesia and it was tolerated by the patients.
It has been reported that the use of NBCA as an embolic agent can increase operative technical difficulty due to the strong inflammatory reaction and development of fibrosis induced by the use of NBCA (6,37). However, in the present study, no surgery was aborted due to resection difficulties attributed to NBCA.
In conclusion, PVE using NBCA through the ipsilateral approach in local anesthesia is safe and effective in inducing hypertrophy of the FLR, enabling surgery, and thereby increasing survival in patients with liver tumors.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.