
Abstract
Background
The rationale behind left renal vein division (LRVD) is the assumption that adequate collateral draining channels will develop.
Purpose
To describe computed tomography (CT) findings after LRVD during aortic surgery.
Material and Methods
Among 61 consecutive patients who underwent LRVD during aneurysm repair or revascularization for aortic occlusive disease between January 2003 and December 2017, 51 patients (40 men, mean age 71.4 ± 8.4 years) were enrolled. Contrast-enhanced CT images were analyzed to evaluate collateral drainage, patency, left renal vein diameter, and left renal parenchymal thickness. A total of 115 radiologic reports were reviewed to check whether these findings were accurately mentioned.
Results
The median time period of the first postoperative follow-up CT was 36 days (range 7–1351 days). The gonadal vein (n = 47) was the most common collateral draining channel, followed by the retroperitoneal veins (n = 42) and adrenal vein (n = 33). Thrombosis occurred in five patients between postoperative days 7 and 17 in the remnant renal vein (n = 3), remnant renal vein plus gonadal and adrenal veins (n = 1), and gonadal vein (n = 1). There was a significant decrease in renal vein diameter (–0.48 ± 2.12 mm, P = 0.006). There was no significant difference in parenchymal thickness (−0.25 ± 1.27 mm, P = 0.193). Neither LRVD nor any associated findings were correctly stated on radiologic reports.
Conclusion
Postoperative contrast-enhanced CT can delineate collateral draining channels and complications following LRVD. However, these findings tend to be either missed or misinterpreted.
Keywords
Introduction
The left renal vein usually runs between the aorta and superior mesenteric artery, connecting the left kidney and the inferior vena cava (IVC) (1,2). The approximate prevalence of circumaortic and retroaortic renal veins are 6% and 3%, respectively (1). When the patient has a pararenal or juxtarenal abdominal aortic aneurysm (AAA) or when the size of the aneurysm is large, surgical procedures become more technically challenging because the left renal vein obscures the surgeon’s field of view. Approximately 8%–20% of AAAs are found in a pararenal location or in both juxtarenal and suprarenal places (3–5). Accordingly, left renal vein division (LRVD) is not an uncommon surgical procedure and facilitates easy access to the aorta and the left renal artery (6–22).
One of the possible consequences after LRVD is a deterioration of venous drainage from the left kidney that can lead to venous hypertension, which manifests as renal dysfunction or hematuria. A number of clinical studies have demonstrated that LRVD can be safely performed, providing favorable short- and long-term clinical data (6–17). However, these studies focused on clinical outcomes by showing that renal function was preserved and both postoperative morbidity and mortality were not increased (12–17). The safety of LRVD is an assumption that potential collateral draining channels such as the adrenal vein, ascending lumbar vein, gonadal vein, and renal capsular vein might play a role. Nonetheless, few studies have dealt with postoperative radiologic findings of venous drainage from the left kidney (14).
The aim of the present study was to describe computed tomography (CT) findings related to LRVD and to check whether any of the associated findings were stated in radiologic reports.
Material and Methods
The institutional review board approved this retrospective single-center study and waived the requirement for written informed consent for the use of electronic medical records, imaging data, and radiologic reports.
Patients
The inclusion criteria were as follows: (i) LRVD performed during aortic surgery; and (ii) available preoperative and postoperative contrast-enhanced CT imaging data. Between January 2003 and December 2017, 61 consecutive patients underwent LRVD during aneurysm repair (n = 49) or revascularization for aortic occlusive disease (n = 12). Aortic repair surgeries for AAA and aortic occlusive disease were performed by three vascular surgeons. LRVD was performed when it was difficult to control the renal artery or expose the proximal aortic neck. The left renal vein was divided as close as possible to its confluence with the IVC to preserve the potential collateral draining channels. Nine patients who did not have postoperative CT images and one patient who underwent renal vein reconstruction at the time of surgery were excluded. Finally, 51 patients (40 men, 11 women, mean age = 71.4 ± 8.4 years) with AAA (n = 40) or aortic occlusive disease (n = 11) were included. Patients’ baseline characteristics are summarized in Table 1.
Patient demographics and baseline characteristics.

Values are given as n (%) or mean ± SD.
AAA, abdominal aortic aneurysm; AOD, aortic occlusive disease.
Analysis of CT findings after LRVD
The preoperative and first postoperative follow-up contrast-enhanced CT imaging datasets of each patient were compared by two radiologists (HNL and DH) to evaluate the development of collateral draining channels from the left renal vein, including the adrenal vein, gonadal vein, periureteral plexus, renal capsular vein, and retroperitoneal veins (lumbar, ascending lumbar, and hemiazygos veins). Postoperative dilatation of the collateral draining channels was stratified into dominant and codominant patterns. A dominant pattern was defined when one collateral draining channel was predominantly dilated over the others in terms of diameter. A co-dominant pattern meant that multiple collateral draining channels were dilated with no predominance.
The left renal parenchymal thickness and left renal vein diameter were measured at the level of the renal hilum in each patient, using Picture Archiving and Communication System (PACS) software (Fig. 1). If segmental confluence of the left renal vein occurred before entering the hilum, the diameter of the largest branch was measured. The changes in parenchymal thickness and renal vein diameter were calculated.
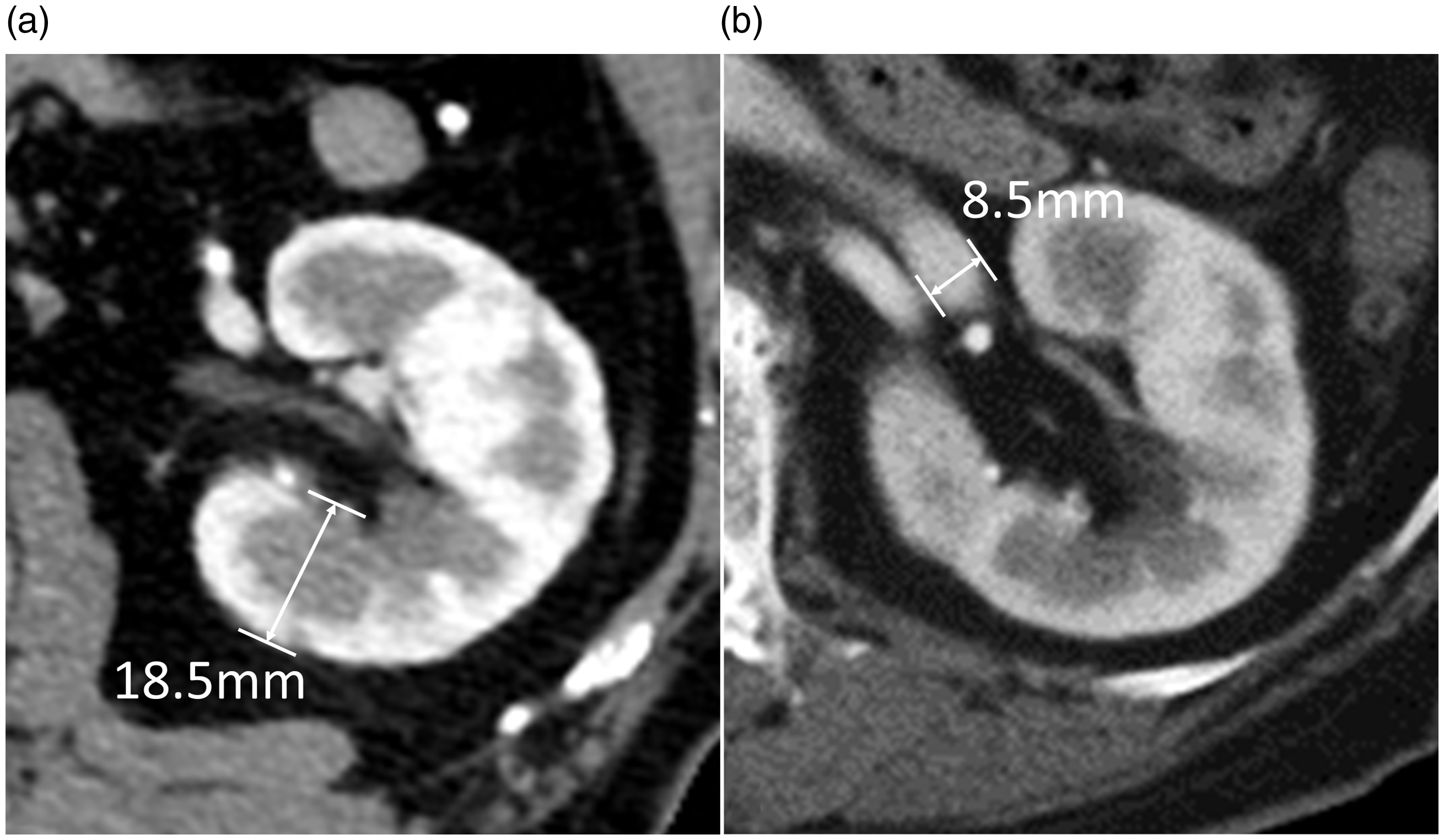
Measurement of renal parenchymal thickness and renal vein diameter. (a) Parenchymal thickness was measured perpendicular to the axis of the kidney on an axial image at the level of the hilum, from the renal capsule to the inner border of the medulla. (b) Renal vein diameter was measured at the level of the hilum on an axial image.
The presence of thrombus in the remnant renal vein or collateral draining channels was evaluated on postoperative follow-up contrast-enhanced CTs. Remnant renal vein thrombosis was classified into complete and partial thrombosis. Complete thrombosis was defined as no-vessel enhancement. Partial thrombosis was defined as the presence of both contrast enhancement and a low attenuation thrombus within the vessel lumen. In cases of partial or complete thrombosis, complications—including flank pain, hematuria, infarction, hemorrhage, and renal functional impairment—were also evaluated by reviewing electronic medical records. Clinical characteristics were compared between patients with and without thrombosis.
Evaluation of postoperative radiologic reports
Postoperative follow-up CT images were originally interpreted by radiologists who specialized in cardiovascular imaging. Preoperative CT images and past history were readily available from the electronic medical records and PACS software at the time of interpretation.
The radiologic reports were reviewed (HNL) to evaluate whether any of the following findings associated with LRVD were reported: discontinuity of the left renal vein, collateral draining channels for venous drainage, and any ancillary findings, including venous thrombosis.
Statistics
A computerized database was created and all clinical data were collected retrospectively. For descriptive statistics, numerical variables are presented as the mean ± SD, and categorical variables are presented as absolute and relative frequencies. Wilcoxon signed rank tests were used to compare the pre- and postoperative values of renal parenchymal thickness and renal vein diameter. For comparative analysis, the Mann–Whitney U test was used for continuous variables and Fisher’s exact test for categorical variables. A P value < 0.05 was considered statistically significant. The statistical analyses were executed using SPSS (version 25 software; IBM Corp., Armonk, NY, USA).
Results
A total of 123 CT scans were acquired for 51 patients during the follow-up period. The median time period of the first postoperative follow-up CT was 36 days (range = 7–1351 days). The number of follow-up CT examinations was in the range of 1–10 (mean = 2.4) per patient. The median duration of the entire follow-up period was 621 days (range = 7–3193 days).
Analysis of CT imaging findings after LRVD
The collateral draining channels demonstrated on postoperative CT images included the following, presented in descending order: gonadal vein (n = 47, 92.2%), retroperitoneal veins (n = 42, 82.4%), adrenal vein (n = 33, 64.7%), periureteral plexus (n = 31, 60.8%), and renal capsular vein (n = 23, 45.1%) (Fig. 2). A dominant pattern was observed in 31 of 51 patients (60.8%) and comprised 21 retroperitoneal veins and 10 gonadal veins. A co-dominant pattern was noted in 20 patients (39.2%) and included the retroperitoneal-gonadal (n = 12), retroperitoneal-gonadal-capsular (n = 5), and gonadal-capsular (n = 3) veins (Fig. 2).

Collateral draining channels on curved planar reformatted computed tomography images in patient with retroperitoneal-gonadal-capsular co-dominant pattern. (a) Phrenic vein (white arrowhead), adrenal vein (white arrow), renal capsular vein (double white arrows), gonadal vein (black arrow), retroperitoneal vein (double black arrows). (b) Renal capsular vein (double white arrows), periureteral plexus (white arrow).
Between postoperative days 7 and 17, five patients (9.8%) experienced thrombi in the following collateral draining channels: remnant renal vein (n = 3); remnant renal vein plus gonadal and adrenal veins (n = 1); and gonadal vein alone (n = 1). Among the four patients who had remnant renal vein thrombosis, three patients had partial thrombosis (n = 3), and the other patient had a complete thrombosis (n = 1). No patients received anticoagulation therapy during the follow-up period.
There were no significant differences in clinical characteristics between patients with and without thrombosis (Table 2). Among the five patients with thrombosis, complete resolution of the thrombosis was observed in four patients (Fig. 3), and thrombus-related complications did not occur. Only one patient with complete thrombosis in the remnant renal vein experienced gross hematuria and renal functional impairment. In this patient, abdominal compartment syndrome occurred and hematoma evacuation had to be performed on postoperative day 3. Since the patient’s renal function deteriorated rapidly over the following 17 days, subsequent contrast-enhanced follow-up CT could not be performed. Among the 46 patients without thrombosis, renal functional impairment occurred in 8 of 45 patients (17.8%) and hematuria in 3 of 30 patients (10%). One patient had no data on serum creatinine levels, and the development of hematuria could be evaluated in 30 patients.
Clinical characteristics of patients with and without thrombosis in the remnant renal vein or collateral draining channels.

Values are given as n (%) or mean ± SD.

A 63-year-old man with postoperative renal vein thrombosis. (a) An axial contrast-enhanced CT image acquired on postoperative day 35 demonstrates a thrombus (white arrow) extending from the proximal stump to the distal renal vein. (b) A contrast-enhanced axial CT image acquired on postoperative day 277 shows complete resolution of the thrombosis (black arrow). CT, computed tomography.
The parenchymal thicknesses and renal vein diameters before and after surgery are summarized in Table 3. There was no significant difference between pre- and postoperative parenchymal thickness (–0.25 ± 1.27 mm, P = 0.193) in the left kidney. Only one patient showed an increase of >3 mm. Renal vein diameter significantly decreased postoperatively (–0.48 ± 2.12 mm, P = 0.006). Only one patient who had complete thrombosis demonstrated an increase in diameter by >4 mm. In 35 of 51 patients (68.6%), segmental confluence of the left renal vein occurred before entering the hilum.
Left renal parenchymal thickness and left renal vein diameter before and after surgery.
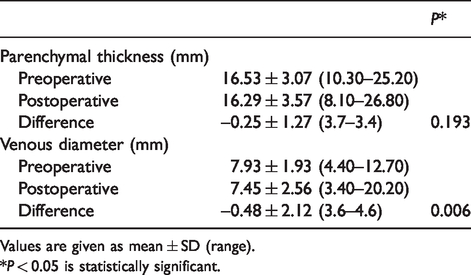
Values are given as mean ± SD (range).
*P < 0.05 is statistically significant.
Evaluation of postoperative radiologic reports
A total of 115 radiologic reports of 51 patients were reviewed. No radiologic report correctly stated the findings related to LRVD. In 10 radiologic reports of seven patients, LRVD-associated findings were detected but misinterpreted, as follows: remnant renal vein as an occlusion (n = 7) (Fig. 4) or extrinsic compression (n = 2) (Fig. 5); and collateral draining channel as a retroaortic left renal vein (n = 1) (Fig. 6). In five radiologic reports of two patients with renal vein thrombosis, thrombosis was described without mentioning of LRVD. In the remaining 100 radiologic reports of 42 patients, nothing was mentioned.
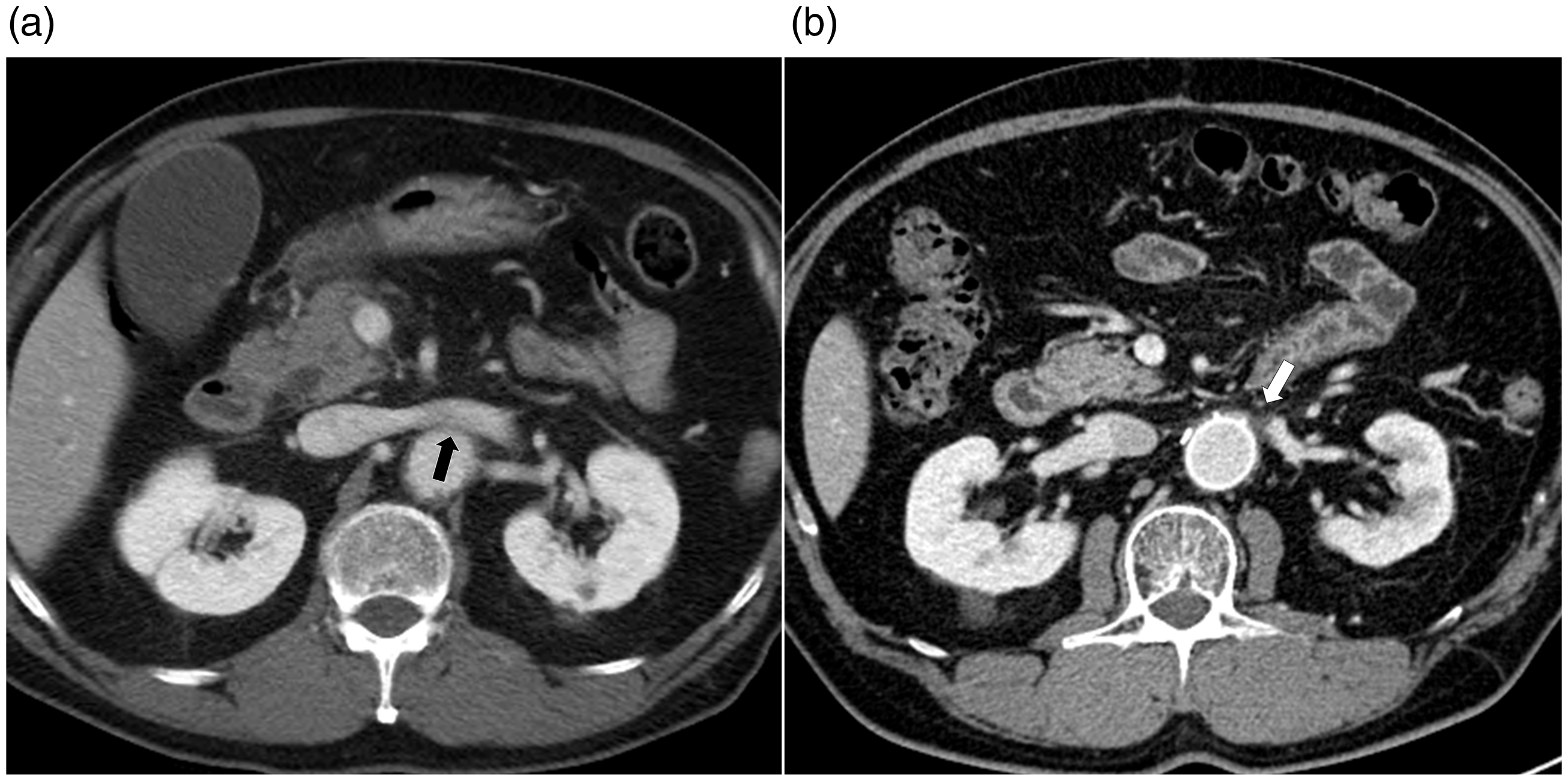
A case of a remnant renal vein misinterpreted as an “occlusion.” (a) A preoperative contrast-enhanced axial CT image shows left renal vein (black arrow) with a normal course between the abdominal aorta and superior mesenteric artery. (b) An axial contrast-enhanced CT image acquired on postoperative day 237 demonstrates a renal vein stump (white arrow) after LRVD. CT, computed tomography; LRVD, left renal vein division.

A case of a remnant renal vein misinterpreted as an “extrinsic compression.” (a) An axial preoperative contrast-enhanced CT image shows the left renal vein (black arrow), which crosses in front of the abdominal aortic aneurysm. (b) An axial contrast-enhanced CT image acquired on postoperative day 346 demonstrates the renal vein stump (white arrow). The division of the renal vein was mistaken for a collapsed vein by the aortic aneurysm. CT, computed tomography.

A case of a remnant renal vein misinterpreted as a “retroaortic renal vein.” (a) A preoperative contrast-enhanced CT image shows a patent left renal vein (black arrow) compressed by an aortic aneurysm. (b) A contrast-enhanced CT image acquired on postoperative day 862 demonstrated engorgement of the lumbar vein (double black arrows) misinterpreted as a retroaortic renal vein. The proximal renal vein stump near the inferior vena cava (white arrow) is also noted.
Discussion
LRVD was first described in 1961 by Clark and Leeds during resection of a retroperitoneal tumor without significant exacerbation of renal function (23). In 1967, Neal and Shearburn introduced this technique for AAA repair and reported that it was a safe and helpful surgical adjunct in complicated situations (7). Approximately 8%–20% of AAAs are pararenal, so that LRVD is often required to expose the aorta proximal to the renal artery during surgical repair (3–5). Accordingly, the left renal vein should be carefully divided. Critical venous collaterals from the left renal vein need to be preserved for future adequate venous drainage. To achieve this goal, it is technically important to divide the left renal vein as close as possible to the IVC.
Although the right renal vein has no accessory draining channels, the left renal vein has several candidates. Knowledge of these collateral draining channels from the left renal vein is important to prevent postoperative renal injury. Each tributary has a characteristic confluence point into the left renal vein. The left adrenal vein drains into the superior aspect of the proximal part of the left renal vein, typically 3–5 cm from the orifice of the renal vein, whereas the gonadal vein joins along the inferior aspect of the left renal vein just lateral to the adrenal vein. Almost always, the left inferior phrenic and capsular veins join the left adrenal vein before entering the renal vein. The left renal vein frequently communicates with the retroperitoneal veins. The retroperitoneal veins drain into the posterior aspect of the proximal left renal vein, just lateral to the aorta.
Although there have been many studies on the functional changes of the kidney after LRVD, we have limited information on the postoperative imaging findings and their clinical significance (6–22). Elsharawy et al. (14) reported gross morphologic changes on CT in patients who underwent LRVD during the management of aortic occlusive disease. They showed diffuse swelling and congestion of the left kidney on postoperative day 4 in four out of six patients who underwent LRVD, but this resolved by day 14. However, by analyzing the CT data of 51 patients, the current study revealed no significant change in left renal parenchymal thickness after surgery. This discrepancy might be explained by the long-term follow-up of our study. Acute renal congestion and a rapid rise in renal vein stump pressure induced by LRVD could be resolved after adequate development of accessory draining channels. The significant decrease in postoperative renal vein diameter in the current study also appears to reflect the development of sufficient venous drainage (24).
Regarding draining veins, engorgement of the accessory draining channels could be identified on CT in every patient after LRVD in the present study, and the gonadal (n = 47, 92.2%) and retroperitoneal (n = 42, 82.4%) veins were revealed to be the major draining channels. These imaging findings are partly in accordance with the results of previous animal and clinical studies. In an animal study with rats, division of both the left renal vein and adrenal vein resulted in acceptable renal function and histology. On the other hand, the gonadal vein should be preserved as a major draining channel (25). In a clinical study with patients undergoing LRVD as an adjunct to aortic surgery, postoperative spermatic venography demonstrated collateral drainage through various retroperitoneal veins in most cases (24). From the information about changes in left kidney size and collateral draining channels from existing studies, including ours, we can assume that it takes at least two weeks for physiological adaptation of a venous drain to occur after LRVD, and collateral draining channels, especially gonadal and retroperitoneal veins, play an important role.
Thrombotic complications after LRVD have never been properly investigated. The pathogenesis is not clear, but the most likely mechanisms include the following: (i) inadequate drainage capacity of tributaries; (ii) technical errors during the procedure; and (iii) underlying kidney disease such as glomerulopathy. None of the five patients with renal vein thrombosis had underlying chronic kidney disease or renal artery stenosis. In the present study, the majority of the patients (4/5, 80%) were asymptomatic and were diagnosed incidentally during the follow-up CT exam. However, renal vein thrombosis can cause severe passive congestion which causes the kidney to swell and become engorged, leading to degeneration of the nephrons, symptoms of flank pain and hematuria and deterioration of renal function. Concurrent involvement of tributaries may result in organ-specific complications such as adrenal hemorrhage, adrenal insufficiency or pelvic congestion syndrome (26–28). In this context, early diagnosis and anticoagulation therapy for patients with renal vein thrombosis are essential (27).
Although endovascular aneurysm repair has become the first-line treatment for AAA, open repair is still chosen when the anatomical factors are not favorable (29). However, radiologists seem to be unfamiliar with LRVD and its clinical significance. In the present study, none of the postoperative radiologic reports correctly mentioned the state of LRVD or the development of collateral draining channels. Patients with renal vein thrombosis were correctly diagnosed in 40% of the cases (2/5 cases). Considering that one case of a serious complication, a complete renal vein thrombosis, occurred in the present study, it is worth reporting the presence of thrombosis to help physicians manage patients in the postoperative period. The high percentage of missed interpretations (86.3%, 44/51) might arise from inappropriate acquisition timing of contrast-enhanced CT and unfamiliarity with LRVD-associated findings. Therefore, when radiologists interpret CT images following open repair, efforts should be made to evaluate the status of the left renal vein and collateral draining channels and the presence of thrombosis.
The present study has some limitations. First, because of its retrospective and single-center nature, there may be bias in the data collection and analyses. Regarding interpretation accuracy, a multicenter study is required to generalize our results. Second, because of the small number of events, the clinical significance of thrombosis in the remnant renal vein or collateral draining channels could not be fully elucidated. Finally, the postoperative follow-up CT period varied widely. This could influence the measurement data of the renal vein diameter and renal parenchymal thickness, and the incidence of thrombosis.
In conclusion, after LRVD, collateral draining channels (gonadal, adrenal, renal capsular, retroperitoneal veins, and periureteral plexus) and possible serious complications such as thrombosis are well delineated on postoperative contrast-enhanced CT images. However, these findings tend to be either missed or misinterpreted.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.