
Abstract
Background
Fibular flaps have been widely used for mandibular and maxillary reconstructions. On occasion, anatomical variants of fibular arteries (FA) will be encountered.
Purpose
Although anatomical variants of FA during fibular harvest have been reported, controversy exists regarding whether simple color Doppler ultrasonography (CDU) and physical examinations (PE) are sufficient for early preoperative detection.
Material and Methods
A 10-year retrospective analysis in our department was performed to find the patients with various FA anomalies confirmed by computed tomography angiography (CTA) or intraoperative findings.
Results
A total number of 19 FA anomalies were found either pre- or intraoperatively in 16 patients, in whom three cases were with bilateral FA variants. Type IIIC variants, also called arteria peronea magna (great peroneal artery), were confirmed in two legs, while the majority (13 legs) had type IIIA hypoplastic/aplastic posterior tibialis arteries (PTA). Four legs had new type IIID (low FA and PTA bifurcations). Preoperative CDU and PE only suspected anomalies in two legs. Six cases proceeded with using the affected fibulas, within whom vascular grafts were used in half of them for lengthening the FA pedicle. Local ischemia, partial soleus muscle necrosis, and claudication were reported in one.
Conclusions
Routine CTA before every fibular harvest, rather than simple PE and CDU, should be added for screening contraindications and ensuring safety for fibular flap harvest.
Introduction
Fibular flaps have been used as a workhorse flap for jaw reconstructions (1). During the fibular flap transfer procedures, the fibular artery (FA) is routinely transected for subsequent anastomosis to another artery at the cervical recipient site (1,2). The FA is one of the principal three sources of the arterial supply of the leg, along with the anterior tibial artery (ATA) and the posterior tibial artery (PTA) (2). In general, after fibular harvest, the donor leg can be solely vascularized by ATA and PTA. However, some congenital and acquired abnormalities, such as hypoplastic or aplastic infra-popliteal arteries, may preclude the use of the fibular flap for a potential risk of pedal ischemia or necrosis (3). Though rare, this is the most feared donor-site complication after fibular flap harvest (4). Therefore, a proper evaluation of the infra-popliteal arteries is essential before harvest. Despite the awareness of several anatomical variants of FA, ATA, and PTA, however, routine preoperative imaging evaluations before fibular harvest remain controversial (5–7). Some still rely solely on physical examinations (PE) or color Doppler ultrasonography (CDU), while others advocate preferred evaluations by computed tomography (CT) or magnetic resonance (MR) angiography (8,9).
Although there is currently no universal consensus on this topic, surgeons are now more likely to be confronted with such vascular variants as the number of fibular transfers increase every year. In order to summarize the change of practice, and the lessons learned from encountering various FA variants in the last 10 years, the aim of the present study was to present our experiences and justify the routine use of CT angiography (CTA) in identifying cases with such contraindications to avoid iatrogenic mistakes.
Material and Methods
A retrospective analysis with a focus on FA vascular abnormalities was performed by searching chart records and imaging data in our department from October 2009 to September 2019. All the included cases had received fibular harvest operations or had unimplemented plans of fibular harvest due to unfavorable imaging information. The incidence among all candidates for fibular flaps were calculated. The recorded parameters were age, sex, co-morbidities, diagnosis, types of preoperative vascular assessment, donor-site choices, and complications. Co-morbidities before fibular flap harvest were collected with an emphasis on diabetes mellitus or cardiovascular or hematological diseases. Methods of preoperative vascular assessment varied on a team-to-team basis with a dichotomous division of using solely physical and CDU examinations, or using all physical, CDU, and CTA examinations. For the analyses of vascular abnormalities, we used the classic Kim–Lippert classification (Table 1) for records of different infra-popliteal arterial branching patterns (7). According to the Kim–Lippert classification, type IA was considered the normal branching, while types IB and IC were regarded as normal-level branching variations. Type II was generally regarded as a higher origin (or division above tibial plateau) of popliteal artery branching. These two types (types I and II), with normal distal branching, were not relevant to the topic of fibular harvest safety. Therefore, we, like other studies, focused on type III variations as these variations encompassed the hypoplastic ATA and/or PTA situations, which might pose a threat to the plantar circulation if FA was planned to be dissected (10,11). In addition to the Kim–Lippert classification, we for the first time identified four cases with low distal bifurcation (in the middle of the leg) dividing PTA and FA. To the best of our knowledge, there have been no reports so far on such important types of variants. Thus, we named this type of vascular anomalies type IIID (Fig. 1), in its relation to potential shorter pedicle length during fibular harvest. We also collected some other acquired FA abnormalities in the Department of Vascular Surgery in our institution, though most of these patients were unquestionably contraindicated for fibular harvests due to severe symptomatic peripheral vascular diseases.
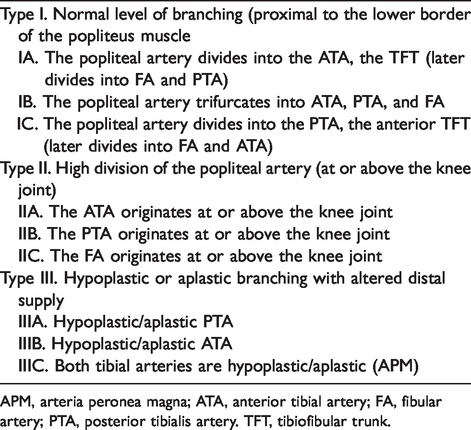
APM, arteria peronea magna; ATA, anterior tibial artery; FA, fibular artery; PTA, posterior tibialis artery. TFT, tibiofibular trunk.

Type III variants of infra-popliteal arterial branching patterns, with IIID as the new subtype:
CDU examinations were performed by the ultrasound practitioners at our institution. As for the methods of PE, simple clinical palpating of the dorsalis pedis and posterior tibial arteries pulses was used. The PE, CDU, and CTA protocols were as follows.
PE protocol
A general visual inspection of lower extremities from above the knee to the heel was made in every patient planned for fibular harvest. The movement, texture, and skin color of both legs and feet were checked for normality. The dorsalis pedis artery was palpated and pulse blood oxygen saturation was examined in the big toe for preoperative evaluation of crural circulation. The blood oxygen saturation of the big toe was also examined by pressing on the dorsalis pedis artery for 5 min.
CDU protocol
The ultrasound equipment used was a GE Healthcare (Voluson E8, Boston, USA) with a 5–7-MHz transducer. Considering the vascular anatomy in the popliteal regions, the evaluation of the FA and PTA started from the medial side of the popliteal fossa in order to identify the bifurcation point. The calibers of the FA, PTA, and ATA arteries were then recorded. The hemodynamic parameters were also recorded at the same time.
CTA protocol
A 128-row CT scanner (Brilliance iCT, Philips Healthcare, Cleveland, OH, USA) was used. Scan parameters in using unenhanced spiral acquisitions were as follows: tube voltage = 120 kVp; tube current =200 mA; detector collimations = 0.625 mm; pitch =0.75; rotation time = 0.75s; matrix = 512 × 512). The scanning field ranged approximately 5 cm above the anterior superior iliac spine (ASIS) in a cranial-to-caudal direction up to heel. A standard bolus of 100 mL of intravenous Omnipaque 350 (GE Healthcare) was used as a contrast medium. After injecting the contrast medium, we monitored the distal abdominal aorta for the enhancement up to a 15-s delay until most of the medium concentrated in the abdominal aorta. Raw data of images were calculated using imaging reconstruction (iDose4 standard) at intervals of 0.7 mm and a thickness of 0.7 mm. The images were reformatted into maximum-intensity projection and three-dimensional volume-rendered reconstructions using available software (Runoff, Philips Healthcare, Cleveland, USA). Anatomical features of the FAs were documented, along with the branching patterns of the PTAs. The pedal circulations were also recorded in the imaging data.
The scanning technique used in the present study was initially based on a protocol used for CTA of the FA from literature review, and we did some pre-tests and modifications in order to acquire the best parameters. The crural/plantar circulations, especially the dorsalis pedis artery and medial and lateral plantar arteries, were also assessed in the CTA for patency.
The surgical procedures and plan changes were recorded and compared. Lastly, the postoperative donor-site complications were also documented.
Results
Over the last 10 years (from October 2009 to September 2010), a total of 683 fibular flaps were harvested in our department. The surgical records revealed that eight cases were found with FA vascular anomalies during the harvest. In addition, the preoperative changes of surgical plans were recorded in another eight patients according to the CTA results. In these 16 patients, 19 legs were found with FA abnormalities. In our series, the incidence of the FA vascular variants in all the patients reached 2.8%. The detailed demographic and clinical information is presented in Table 2. The median age of these patients was 50 years; 2 (11.1%) patients had diabetes, 4 (22.2%) had hypertension, and 2 (11.1%) had anemia. One patient (patient 9) was suspected of having acquired a vascular anomaly during their long-term diabetic history and calcified plantar circulations, while the others were regarded as congenital ones (Table 2).
Detailed characteristics of the cases with FA anomalies who planned fibular reconstructions for mandibular defects.

*The documented anomalies were verified intraoperatively or via CTA. For the cases with intraoperative anomalies, the other leg was not examined postoperatively.
†Preoperative crural-pedal circulations were evaluated by CTA for the patency or calcification in crural or pedal arteries.
‡Surgical procedures were for recorded for cases with FA anomalies. Vessel grafts = continuing using the affected fibular flap with additional vessel grafts.
§Vessel grafts for lengthening the shorter pedicle.
AJV, anterior jugular vein; CDU, color Doppler ultrasound; CTA, computed tomography angiography; EJV, external jugular vein; FA, fibular artery; FaA, facial artery; N/A, not applicable; PE, physical examination; SCC, squamous cell carcinoma; TCA, transverse cervical artery.
Regarding the eight cases with intraoperative confirmation of FA abnormalities, the PE and preoperative CDU results were unfortunately all false negatives. On the other hand, for the other eight cases with preoperative changes of harvest plans, only two CDU reports showed suspicions of FA abnormalities, which were later corroborated via means of CTA.
Among all these cases, three were found with bilateral FA anomalies from preoperative CTA results (Fig. 2). Arteria peronea magna (APM; great peroneal artery) (type IIIC, single dominant FA), based on the Senior’s finding, was confirmed in two legs (Fig. 3), while the majority (13 legs) had type IIIA (hypoplastic/aplastic PTA); the other four legs had type IIID (lower-than-normal bifurcations of FA and PTA) (Fig. 4) (12). The imaging and videos of plantar circulation relating to these variants are also shown in the Supplemental Material.
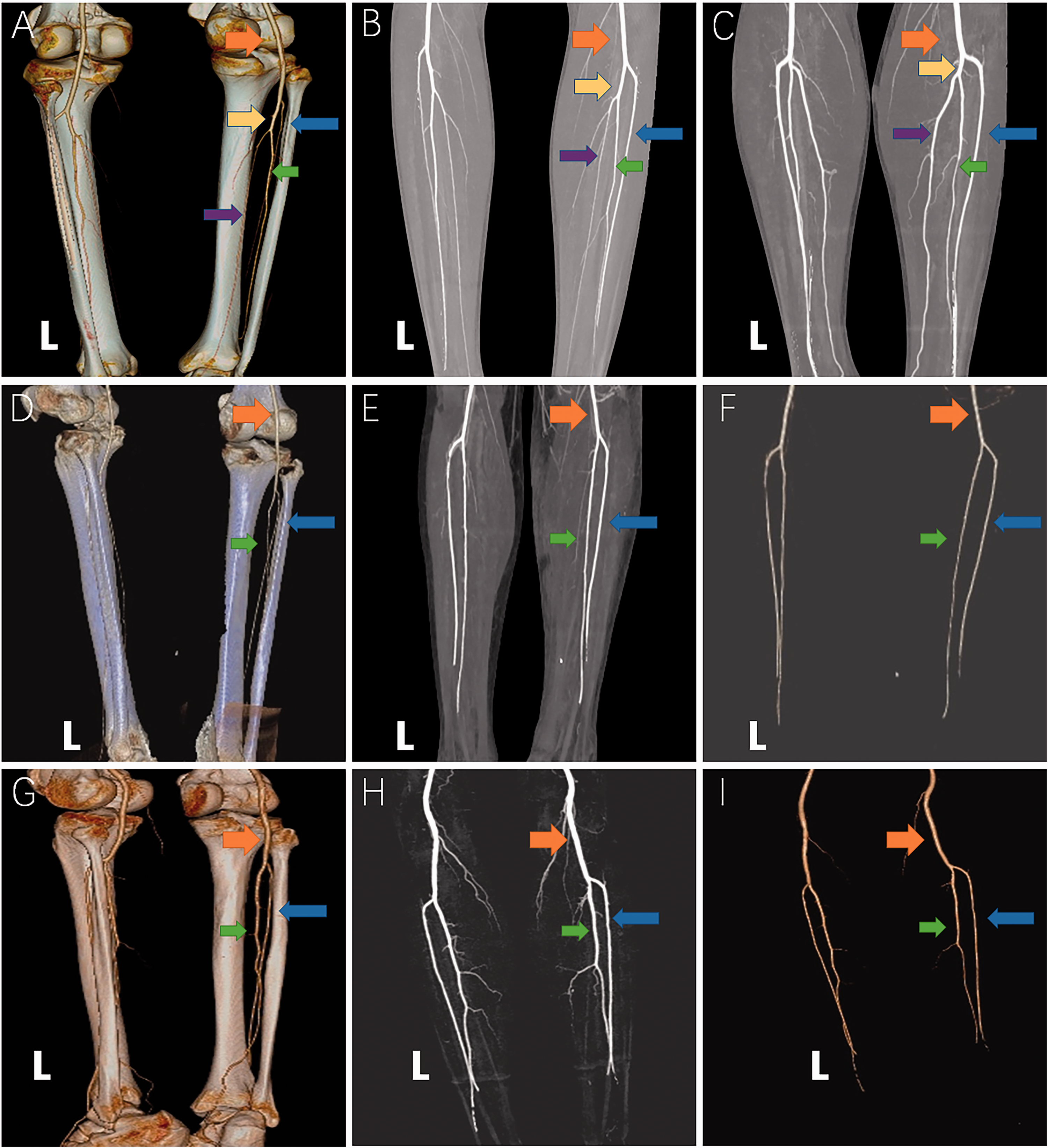
Normal and bilateral infra-popliteal arterial branching anomalies in CTA results. (a–c) Normal branching; (d–f) patient 1; (g–i) patient 4. (a) Normal infra-popliteal arterial branching (type IA) into ATA, tibio-fibular trunk, which later divides into PTA and FA. (b) MIP of a patient with normal type IA branching (the same patient in a). (c) MIP of another patient with normal type IA branching. (d) Reconstructive CTA images with bones in patient 1 with bilateral type IIIA branching variants (with aplastic PTA). (e) MIP of patient 1 with bilateral type IIIA branching variants. (f) VR of patient 1 with bilateral type IIIA branching variants. (g) Reconstructive CTA images with bones in patient 4 with bilateral type IIIA branching variants (with aplastic PTA). (h) MIP of patient 4 with bilateral type IIIA branching variants. (i) VR of patient 4 with bilateral type IIIA branching variants. Orange arrow = popliteal artery; yellow arrow = tibiofibular trunk; green arrow = FA; blue arrow = ATA; purple arrow = PTA. ATA, anterior tibial artery; CTA, computed tomography angiography; FA, fibular artery; MIP, maximum-intensity projection; PTA, posterior tibialis artery; VR, volume-rendering.
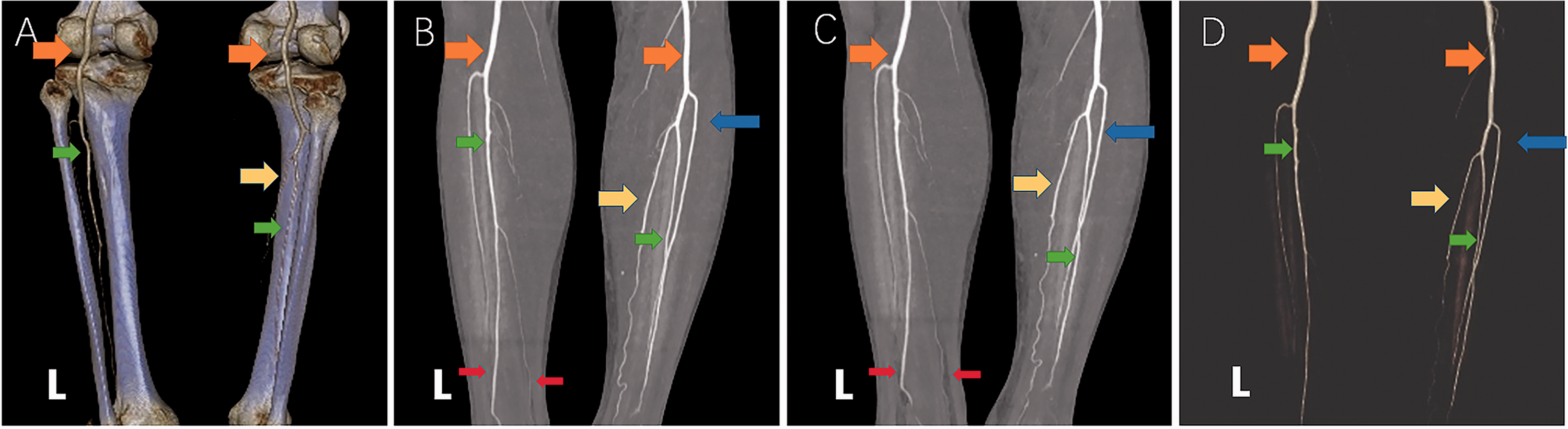
Patient 10 with left-sided APM (type IIIC) variant with dominant FA, hypoplastic ATA and aplastic PTA. (a) Reconstructive CTA images with bones in patient 10 with type IIIC branching variants in right leg. (b) MIP of patient 10 with type IIIC branching variants. ATA ended in the lower third of the leg while APM branched to provide blood supply of the left foot. (c) MIP of patient 10 with type IIIC branching variants. ATA ended in the lower third of the leg while APM branched to provide blood supply of the left foot. (d) VR of patient 10 with type IIIC branching variants. Orange arrow: popliteal artery; yellow arrow = PTA; green arrow = FA; blue arrow = ATA; red arrow = APM branching. APM, arteria peronea magna; ATA, anterior tibial artery; CTA, computed tomography angiography; FA, fibular artery; MIP, maximum-intensity projection; PTA, posterior tibialis artery; VR, volume-rendering.
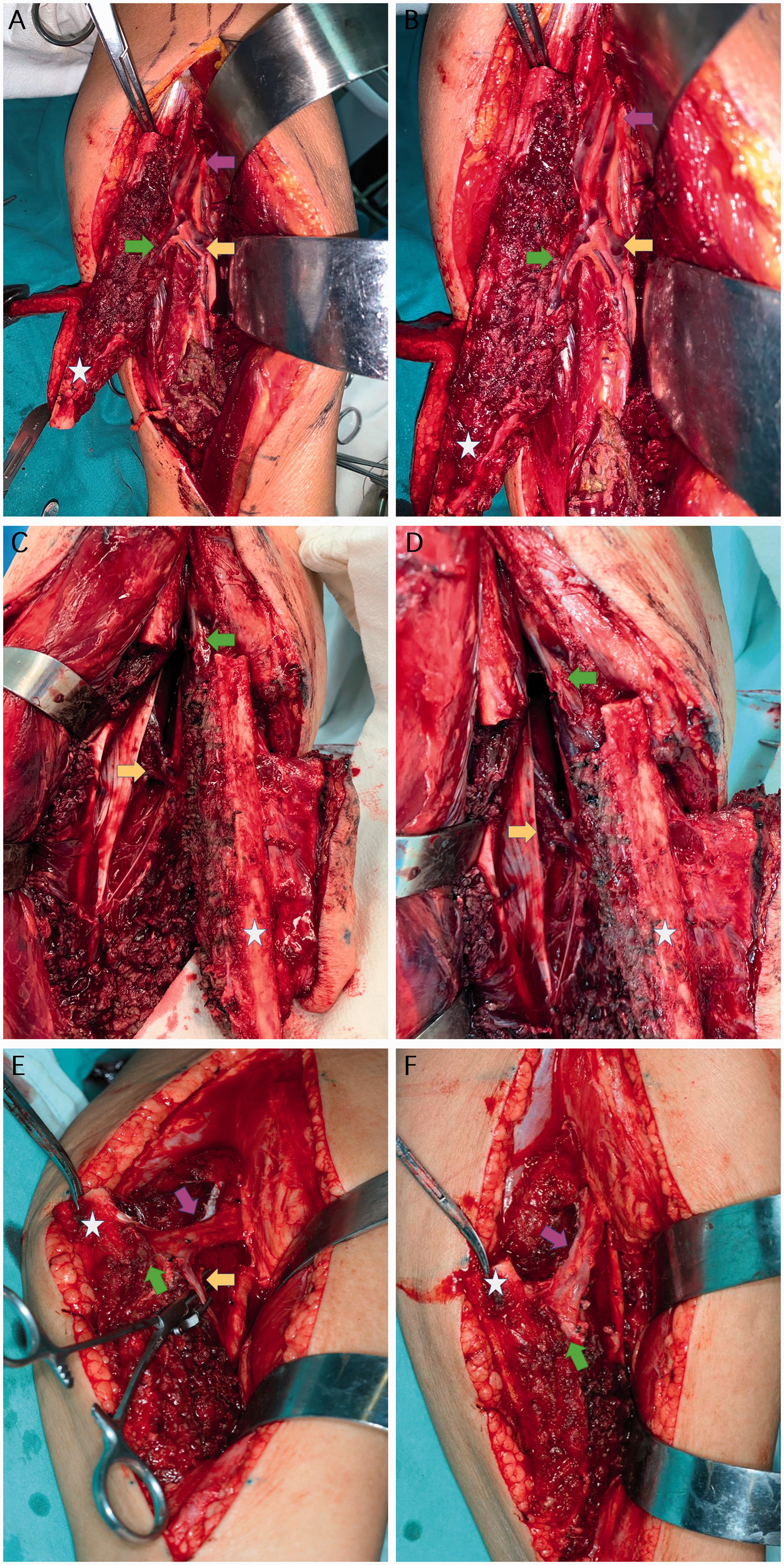
Presentation of cases with type IIID branching variants (low bifurcation of PTA/FA) with intraoperative findings. (a, b) Patient 2: the tibiofibular trunk divided into FA and PTA in the middle of the leg. (c, d) Patient 6: division of FA and PTA in the middle of the leg. (e, f) Patient 13: division of FA and PTA in the middle of the leg. (d) Preparation of ligation of PTA; (f) post-ligation of PTA (FA for fibular flap harvest). Purple arrow = tibiofibular arterial trunk; green arrow = FA; yellow arrow = PTA; white star = fibular bone. All images were in the head-to-toe direction. ATA, anterior tibial artery; CTA, computed tomography angiography; FA, fibular artery; MIP, maximum-intensity projection; PTA, posterior tibialis artery; VR, volume-rendering.
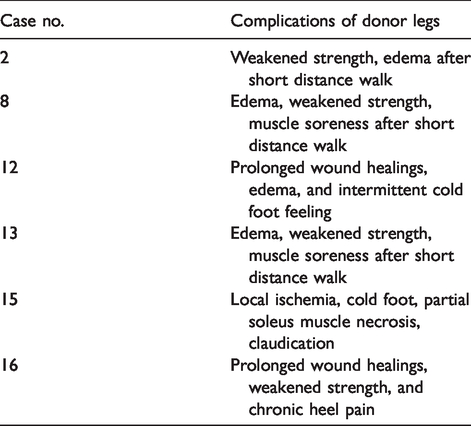
Furthermore, in our series, these vascular variants of FAs influenced the surgical procedures and plans. For the eight patients who underwent surgical fibular flap harvest, none of them had received any tests of lower-extremity CTAs before the operations. According to the surgical records, the surgical harvest still proceeded in six patients using the affected FAs, among whom vascular grafts (facial artery [4 cm] and external jugular vein [6 cm] for patient 2; transverse cervical artery [6 cm] and external jugular vein [7.5 cm] for patient 8; facial artery [4.5 cm] and anterior jugular vein [5 cm] for patient 13) were used in 3 (18.8%) cases for lengthening the pedicles for anastomoses (detailed information regarding vascular grafts is shown in Table 2). On the contrary, the harvest was aborted in the other two cases with the fibulas plated back and conversion to raising soft tissue flaps instead. Local ischemia, partial soleus muscle necrosis, and subsequent claudication were reported in one patient. Further, prolonged wound healings were reported in two patients while five of these eight cases reported persistent edema or cold limbs after three months of the harvest. Weakened leg strength was reported in four cases (Table 3). On the other hand, based on the preoperative CTA results, reconstructive plan alternatives were changed preoperatively for the other eight cases, with replacement of soft tissue free flaps, iliac bone flaps, or adjacent flaps for five, two, and one cases, respectively (Table 2).
Donor leg complications after affected fibular harvest in patients with fibular artery variants.
Discussion
Fibular flaps have been widely used for the reconstruction of large maxillary and mandibular defects (1). In the context of fibular flap harvest, vascular variations that may complicate, or even compromise, the flap harvest should be identified beforehand (13). Although the prevalence of such vascular variants involving the infra-popliteal or leg arterial trunks are at no more than 8%–9%, unawareness of these variants may result in ischemia of the foot and even limb loss (2,14). According to the study by Kil and Jung (15) of 1242 extremities, 1108 (89.2%) had normal branching, 63 (5.1%) had hypoplastic or aplastic PTA with replacement of enlarged fibular artery (FA), while hypoplastic or aplastic ATA were found in 21 (1.7%) extremities. Peroneal artery magna (with both hypoplastic or aplastic PTA and ATA) was found in 10 (0.8%) extremities. In the review by Kropman et al. (16), after the analysis of 7671 limbs, all types of variations in infra-popliteal artery branching were found in almost 10% of limbs, while the type III (hypoplastic or aplastic PTA) variations were confirmed in 1%–8.3% of limbs. In our series, the incidence of specific FA vascular variants in all the patients reached 2.8%, which was close to the results of the studies by both Kil and Jung, and Kropman et al. Although the chance of encountering such variations was not high, our iatrogenic lessons of insufficient evaluations were still alarming to the microvascular practitioners who were planning fibular flap reconstructions.
According to previous studies, normal-level (type I) or higher-origin (type II) variations were not closely relevant to microsurgical fibular flap harvest of our topic; instead these types were more relevant to other clinical scenarios during peripheral vascular interventions (11). Therefore, we focused on type III variations as these variations encompassed the hypoplastic ATA and/or PTA situations, which might pose a threat to the crural-plantar circulation if FA was to be dissected (Table 1).
Anatomically speaking, the vascular supply of the leg originates from popliteal artery, which usually bifurcates into the ATA and PTA at the inferior border of the popliteus muscle. The PTA continues shortly as the clinically recognized tibiofibular trunk and subsequently gives off FA (10,11). For the type IIIA variant, PTA is hypoplastic or aplastic and a large (dominant) FA instead replaces the role of providing both the posterior circulation of the leg and the heel. ATA hypoplasia or aplasia is generally found in type IIIB, with FA and PTA as the dominant arteries. Finally, in the extreme situation of type IIIC, both ATA and PTA are hypoplastic or absent, a single FA provides all the vascular supply for the foot and is regarded as the absolute contraindication to fibular flap harvest. APM (type IIIC) was first defined in 1919 as the presence of a single large peroneal artery that traverses the posterior crural region and enters the sole (12). Later, an enlarged APM (without the PTA) accompanied with a hypoplastic (smaller) ATA was also categorized as a type IIIC branching pattern of infra-popliteal arteries (hypoplastic–aplastic posterior and anterior tibial arteries) (17). As for type IV, FA hypoplasia or aplasia is very rare according to most studies (1,3,18). Aside from the Kim–Lippert classification, we found four cases of lower-than-normal-level bifurcations of FA and PTA, thus naming such type of variants as type IIID (Fig. 1). We have checked the classical works from Quain (19) and Dubreil-Chambardel (20) and there were no reports or descriptions on such variations. To be specific, the arterial bifurcation points in our series were found in the middle or even bottom third of the leg instead of the normal position right below the popliteal fossa (21). For the sake of fibular flap harvest, pedicle and bone length will be greatly affected when encountered with such variants, resulting in aborted or, at best, shorter than usual flaps or pedicles, as opposed to the original reconstructive plans. For uncompromising the foot circulation, vessel grafts, such as those used in our series, also need to be prepared to make up for shorter pedicles due to such type IIID variants, as is shown in our series. Bilateral FA anomalies were mentioned in other studies, with an incidence of 28%–50% out of all those with infra-popliteal vascular anomalies (14,22,23). We also reported 3 (18.8%) cases of bilateral FA variants, of which two were with bilateral type IIIA variants. According to the classical study by Kil and Jung, most of the bilateral anomalies were found to be bilateral type IIIAs, which is consistent with our results (15). In each of these anatomical variations, removal of FAs during harvesting will probably jeopardize the vascular supply of the donor leg, the flap, or both (24).
In addition to the congenital variants of FA, the acquired anomalies of FA, especially for those with long-term diabetes or dialysis, should always be kept in mind when considering fibular flap reconstructions. Peripheral arterial occlusive diseases (PAOD), caused by aging, diabetes, and dialysis, are characterized by a gradual reduction in blood to the extremities secondary to atherosclerosis (25,26). PAOD preferentially affects the infra-popliteal arteries, which generally present cumulative segmental or total thrombotic deposits or calcifications (26,27). CTA is an indispensable evaluation method before any vascular interventions, as segmental or atypical PAOD in FA, PTA, or ATA could be found in either symptomatic or asymptomatic patients (28). Although most of the cases in our series were with congenital vascular anomalies, some exemplary infra-popliteal PAOD cases were also shared by the vascular surgeons in our institutions (Supplemental data). Therefore, we considered that precautions for direct preoperative CTA screening in diabetic or dialytic candidates for fibular flaps should be taken; however, so far no absolute contraindications were given in these clinical situations.
Negligence of preoperative FA evaluations will result in iatrogenic disasters. Serious consequences have been reported recently when encountering such anatomical anomalies during fibular harvest operations. In 2005, Rosson and Singh (29) found devascularization of the donor leg with type IIIC variant after a fibular flap harvest. Fortunately, limb salvage procedures were carried out by insetting a vascular bypass with reversed the saphenous vein. In 2014, another case of foot ischemia after fibular harvest was salvaged again with a saphenous vein graft and repeated subsequent debridement (4). However, in many other studies, it was claimed that the donor leg wounds in patients who had fibular harvests with vascular anomalies healed without visible ischemic complications during perioperative hospitalizations (6). Despite these contradictory results, during the follow-up, we found a high donor-site morbidity rate of persistent edema or cold limbs when the fibular harvests proceeded in these affected donor legs. In addition, in our cases, one patient developed partial soleus muscle necrosis and managed with debridement; however, claudication still occured due to local tissue ischemia and contraction. Therefore, as far as we were concerned, precautions should be taken in the continuation of fibular harvests when FA anomalies are inadvertently identified intraoperatively, as either short-term or long-term leg complications were formidable and hard to resolve. A plan B should be decided preoperatively as there are many other viable reconstructive alternatives to choose from instead of gambling with these affected legs without a second thought.
Undoubtedly, the attendant risks or hazards with FA variants call for thorough preoperative screening. The ideal method of evaluation for the donor limb vessels has long been debated with the unsolved question of whether angiography should be applied routinely. Lutz et al. (5) and Disa and Cordeiro (6) considered the routine use of preoperative angiogram was not justified based on their experiences. Conversely, Lorenz and Esclamado (3) found that a simple PE by distal pedal palpation was not reliable. In our opinion, screening with simple PE palpation may not guarantee the safety of fibular harvest, as opposed to the Allen palpation assessment for radial forearm flap. On the other hand, CDU or pencil Doppler has also been an option for preoperative evaluations. Some even considered CDU to be as accurate as CTA in the detection of vascular fibular anomalies (30). However, the precision of CDU was recently questioned as the catastrophic outcomes ensued after false negative CDU results in the case by Saydam et al. (4). Though CDU has the advantages of being non-invasive and radiation-free, it is still highly investigator-dependent and non-reproducible. Besides, CDU is quite probe-dependent, and does not directly present the entire arterial anatomy of the lower extremity.
From our perspective, imaging techniques, especially angiography, are still indispensable parts of the preoperative evaluation methods before fibular flap harvest. Historically speaking, multiple imaging modalities have been attempted for predicting the presence of vascular anomalies, including digital subtraction angiography (DSA), CTA, and magnetic resonance angiography (MRA) (2–7,30). The use of DSA has been obsolete for preoperative detection due to its invasive nature and accompanying risks, such as hematoma and vascular occlusion (3). In comparison, CTA has been shown to be equally effective and less invasive in the detection of peripheral vascular anomalies, while avoiding complications caused by invasive arterial catheterization, cheaper, requiring less time, and with less radiation exposure (7,22). The reconstructive views of CTA, like ours, unambiguously revealed the entire branching courses of FAs and PTAs. Similarly, MRA, like CTA, enables reliable and visible preoperative information concerning leg vessels, but with no radiation load. Though it has the disadvantages of lengthy scanning time and increased costs, MRA represents a useful preoperative evaluation before fibula harvesting (30,31). As for virtual surgical planning, the role of CT/CTA in assisting preoperative virtual surgical planning (for bone flaps) has so far not been replaced by MRA. All in all, for the safety of the patient’s donor leg, we consent to the idea that performing routine preoperative CTA or MRA of the leg for all candidates who are planning free fibula flaps (2,3,7,23). Though this will add minor cost burden, the benefits outweigh the costs, in avoiding terrible situations of intraoperative flap changes or potential donor-site limb harm or loss.
The present study has some limitations. This is a retrospective single institutional study incorporating a limited number of cases with FA vascular variants of legs. We acknowledge the possible acquired causes for FA anomalies in aged patients, as most of our cases were with congenital causes. Besides, unlike studies using cadavers, the cases with intraoperative encountered FA anomalies do not guarantee normal branching of FAs or TPAs in the contralateral legs, which had only been checked by PE and CDU. The possibilities of other overlapping variants types could not be excluded.
In conclusion, adequate preoperative imaging angiography of the lower limb is significant for assessing the indication and suitability of a candidate for a fibular flap. It is indispensable and may minimize potential ischemic complications caused by vascular anomalies.
Supplemental Material
sj-jpg-1-acr-10.1177_0284185120980001 - Supplemental material for Standardize routine angiography assessment of leg vasculatures before fibular flap harvest: lessons of congenital and acquired vascular anomalies undetected by color Doppler and physical examinations
Supplemental material, sj-jpg-1-acr-10.1177_0284185120980001 for Standardize routine angiography assessment of leg vasculatures before fibular flap harvest: lessons of congenital and acquired vascular anomalies undetected by color Doppler and physical examinations by Chunyue Ma, Lei Wang, Zhuowei Tian, Xingjun Qin, Dan Zhu, Jinbao Qin and Yi Shen in Acta Radiologica
Supplemental Material
sj-pdf-5-acr-10.1177_0284185120980001 - Supplemental material for Standardize routine angiography assessment of leg vasculatures before fibular flap harvest: lessons of congenital and acquired vascular anomalies undetected by color Doppler and physical examinations
Supplemental material, sj-pdf-5-acr-10.1177_0284185120980001 for Standardize routine angiography assessment of leg vasculatures before fibular flap harvest: lessons of congenital and acquired vascular anomalies undetected by color Doppler and physical examinations by Chunyue Ma, Lei Wang, Zhuowei Tian, Xingjun Qin, Dan Zhu, Jinbao Qin and Yi Shen in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is supported by Science and Technology Commission of Shanghai Municipality, Grant Number: 19ZR1430000; Hospital Innovation Project, Grant Number: CK2019004; Hospital Cross-Multidisciplinary Project, Grant Number: JYJC201911, Fundamental research program funding of Ninth People’s Hospital Affiliated to Shanghai Jiao Tong University School of Medicine (No. JYZZ050).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.