
Abstract
Background
MammaPrint is a 70-gene signature microarray assay that predicts the likelihood of recurrence of breast cancer and chemotherapeutic benefits.
Purpose
To investigate the association between mammography and ultrasound (US) features and MammaPrint results in patients with estrogen receptor (ER)-positive, HER2-negative, node-positive invasive breast cancer, and to identify the predictive factors for high risk of recurrence.
Material and Methods
This retrospective study included 251 patients with ER-positive, HER2-negative, 1–3 node-positive invasive breast cancer. Mammography and US findings were reviewed according to the BI-RADS criteria. The association between MammaPrint results and the clinicopathological and imaging features was evaluated. Logistic regression analysis was performed to identify independent predictors for high risk of recurrence.
Results
Of the patients, 143 (57.0%) and 108 (43.0%) had low and high risks for recurrence on MammaPrint, respectively. Young age (odds ratio [OR] 1.08; 95% confidence interval (CI) 1.04–1.12; P<0.001), posterior enhancement on US (OR 2.45; 95% CI 1.16–5.20; P = 0.019), absence of posterior shadowing on US (OR 3.19; 95% CI 1.17–8.62; P = 0.023), high histologic grade (OR 113.36; 95% CI 6.79–1893.53; P = 0.001), and high Ki-67 level (OR 4.90; 95% CI 2.62–9.17; P<0.001) were independently associated with high risk of recurrence on multivariate logistic regression analysis.
Conclusion
Posterior features in US may predict a high risk of recurrence in patients with ER-positive, HER2-negative, node-positive invasive breast cancer, which may be useful in enhancing the diagnostic value of MammaPrint and aid in the decision-making process regarding treatment.
Introduction
Breast cancer is a heterogeneous disease, and the treatment decisions differ according to the tumor characteristics. Women with early-stage breast cancer are often treated with adjuvant systemic therapy comprising endocrine therapy and chemotherapy. Accurate identification of the patient’s disease may prevent over-treatment with chemotherapy, and several gene expression profiling methods have been thus developed to aid in the decision-making process. For hormone receptor-positive, human epidermal growth factor 2 (HER2)-negative, early-stage breast cancer, Oncotype DX (1,2), MammaPrint (3–6), PAM50 (7), Breast Cancer Index (8,9), and EndoPredict (10,11) have been studied for their value in predicting the prognosis and improving disease management.
The MammaPrint® (Agendia, Amsterdam, The Netherlands) is a 70-gene signature microarray assay that categorizes patients as having high or low risks of recurrence, based on the risk of distant metastasis at 5 and 10 years after treatment (4,5). The prospective randomized MINDACT (Microarray in Node-negative and 1 to 3 positive lymph node Disease may Avoid Chemotherapy) trial validated the efficacy of MammaPrint; in this trial, 46% of the patients at high risk of distant recurrence based on the clinical factors were classified as genomically low-risk patients based on the MammaPrint results and did not receive adjuvant chemotherapy (3). Furthermore, the IMPACt (Impact of MammaPrint on Adjuvant and Neoadjuvant Treatment in Breast Cancer Patients: A Prospective Registry) trial reported that 88.5% of the treatment plans were concordant with the MammaPrint results, along with a 60% decrease in the treatment recommendation for patients whose clinical features indicated high risk but were deemed as low risk by MammaPrint (6).
Furthermore, several studies have used radiological imaging features in combination with the results of the multigene expression assays such as the Oncotype DX (12–16). Yepes et al. (15) demonstrated that the detection of a mass with pleomorphic micro-calcifications on mammography or the presence of posterior enhancement on ultrasound (US) may predict an intermediate-to-high recurrence score. A previous study identified parallel orientation and tumor roundness as independent variables for predicting a high risk of recurrence in patients undergoing Oncotype DX (12), and Dialani et al. (14) reported that a high recurrence score in Oncotype DX was correlated with the presence of a well-circumscribed oval mass on mammography, posterior enhancement and vascularity on US, and a lobulated mass on magnetic resonance imaging (MRI). Another study investigated the relationship between computer-extracted breast MRI phenotypes and multigene assays such as the MammaPrint, Oncotype DX, and PAM50, and reported that tumors with a high risk of recurrence tended to be large and showed more heterogeneous enhancement patterns (13). However, to the best of our knowledge, previous studies have not investigated the correlation between mammography and US characteristics of breast cancer patients and their MammaPrint results. We thus aimed to investigate the association between the mammography and US features and MammaPrint results in patients with ER-positive, HER2-negative, node-positive invasive breast cancer and to identify the predictive factors for high risk of recurrence.
Material and Methods
The institutional review board of Asan Medical Center approved this study, and waived the requirement for informed consent based on the retrospective nature of this study.
Study population
The study population included 271 patients with ER-positive, HER2-negative breast cancer with 1–3 positive lymph nodes who underwent MammaPrint at our institution between January 2018 and December 2019. Of the patients, the following patients were excluded: patients who underwent surgery elsewhere (n = 6); patients who underwent excisional biopsy at another hospital (n = 5); patients who received neoadjuvant chemotherapy (n = 3); patients with a history of breast cancer (n = 3); male patients (n = 2); and patients who did not have US images (n = 1). As a result, the study population comprised 251 women.
Mammography and US image acquisition
Mammography was performed using the full-field digital mammography system (Senographe Essential, GE Healthcare, Milwaukee, WI, USA; Selenia Dimensions, Hologic, Bedford, MA, USA; Mammomat Inspiration, Siemens Healthcare, Erlangen, Germany). Bilateral craniocaudal and mediolateral oblique views were routinely obtained. B-mode US was performed using high-resolution US equipment with a 5–12-MHz or 22–2-MHz linear array transducer (IU22 or EPIQ: Philips Medical Systems, Bothell, WA, USA) by 11 board-certified radiologists with 5–24 years of experience in breast imaging.
Image analysis
Two radiologists (H.S. and W.J.C., with 5 and 10 years of experience in breast imaging, respectively) independently reviewed the preoperative mammographic and US images according to the guidelines of the American College of Radiology Breast Imaging Reporting and Data System (BI-RADS), 5th edition (3). To reduce inter-observer variability, another radiologist joined the interpretation in case of a discrepancy between the two readers, and all three radiologists reached a consensus in describing the imaging findings. The radiologists were blinded to the clinicopathological findings. The mammographic breast densities were classified as either fatty (almost entirely fatty or with scattered areas of fibroglandular density) or dense (heterogeneously or extremely dense). Mammographic features (e.g. lesion type, mass shape, margin, density, and morphology and distribution of calcification) and US features (e.g. mass shape, orientation, margin, echo pattern, and posterior features) were also evaluated.
MammaPrint and pathological data analysis
Samples from surgically excised tumors were analyzed using the MammaPrint microarray assay (Agendia, Amsterdam, The Netherlands). We reviewed the MammaPrint results, which provide index scores in the range of –1.000 and 1.000, and categorized the tumors as having low (index score = 0.001–1.000) or high (index score = –1.000 to 0.000) risk of recurrence. By reviewing the postoperative pathological reports, we also assessed the pathological data including the histological tumor type, size, histologic grade, lymph node metastasis, lymphovascular invasion, expression of epidermal growth factor receptor (EGFR), cytokeratin (CK) 5/6, p53, and Ki-67 proliferation.
Statistical analysis
Statistical analyses were performed using the IBM SPSS Statistics for Windows, version 21 (IBM Corp., Armonk, NY, USA). P < 0.05 was considered statistically significant. The association between MammaPrint results and clinicopathological and imaging features was compared using Student’s t-test or Kruskal–Wallis test for continuous variables and chi-square test or Fisher’s exact test for categorical variables. Logistic regression analyses were performed to identify clinicopathological and imaging features that are independently associated with a high risk of recurrence with respect to the MammaPrint results. Variables with P < 0.05 in univariate analysis were included in the multivariate logistic regression analysis, with backward elimination. Receiver operating characteristic (ROC) analysis was performed to assess the diagnostic accuracy of the logistic model.
Results
Association of clinicopathological data and MammaPrint results
Of the 251 patients, 143 (57.0%) and 108 (43.0%) were at low and high risk of recurrence, respectively, based on the MammaPrint results. Table 1 summarizes the clinicopathological characteristics of the patients. The patients were aged 31–79 years (mean age = 51 years) and those in the high-risk group were significantly younger (P < 0.001). The mean tumor size was 2.3 cm (range = 0.4–6.5 cm) and the majority of the tumors were classified as invasive ductal carcinomas (n = 223, 88.8%), while the other histologic types included invasive lobular carcinoma (n = 19), mucinous carcinoma (n = 6), invasive micropapillary carcinoma (n = 2), and tubular carcinoma (n = 1). All patients presented with node-positive breast cancer with 1–3 positive lymph node metastases. In terms of histologic grade, 15 (6.0%), 220 (87.6%), and 16 (6.4%) tumors were of low, intermediate, and high histologic grade, respectively. The high-risk group was significantly associated with high histologic grade (P < 0.001), lymphovascular invasion (P = 0.001), and high levels of Ki-67 (P < 0.001) compared with the low-risk group.
Patient and tumor characteristics according to the risk of recurrence.

Values are given as n (%) or mean ± SD.
*Includes mucinous carcinoma, invasive micropapillary carcinoma, and tubular carcinoma.
CK, cytokeratin; EGFR, epidermal growth factor receptor; SD, standard deviation.
Association of imaging features and MammaPrint results
The mammographic and US findings based on the BI-RADS criteria are summarized in Tables 2 and 3. Twenty-three tumors (9.2%) were not detected on mammography, while 153 (61.0%) tumors appeared as masses, 15 (6.0%) tumors presented with only calcification, and 60 (23.9%) tumors appeared as masses with calcification. The high-risk group was significantly associated with dense breast tissue (P = 0.027) and indistinct mass margin (P = 0.021). No significant differences were observed between the low- and high-risk groups according to mass shape, density, and morphology and distribution of calcification on mammography. On US, all lesions appeared as masses, and the posterior features were significantly different according to the risk of recurrence (P < 0.001), whereas the mass shape, orientation, margin, and echo pattern in US did not significantly differ between the two groups. Representative images of patients in the low- and high-risk groups are shown in Figs. 1 and 2, respectively.
Mammography features according to the risk of recurrence.
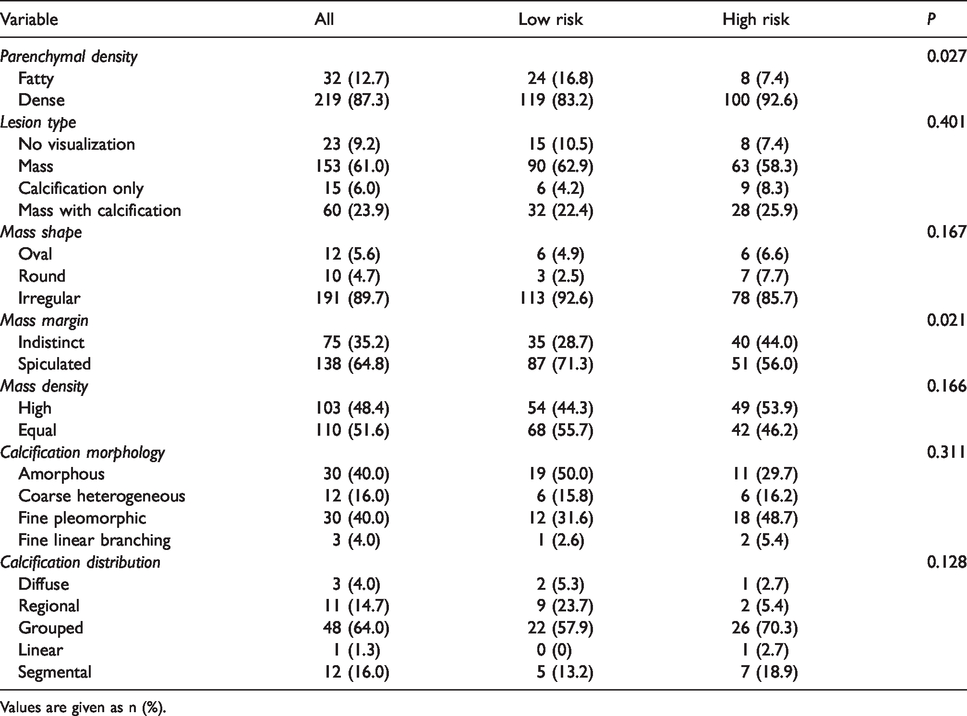
Values are given as n (%).
Ultrasound features according to the risk of recurrence.
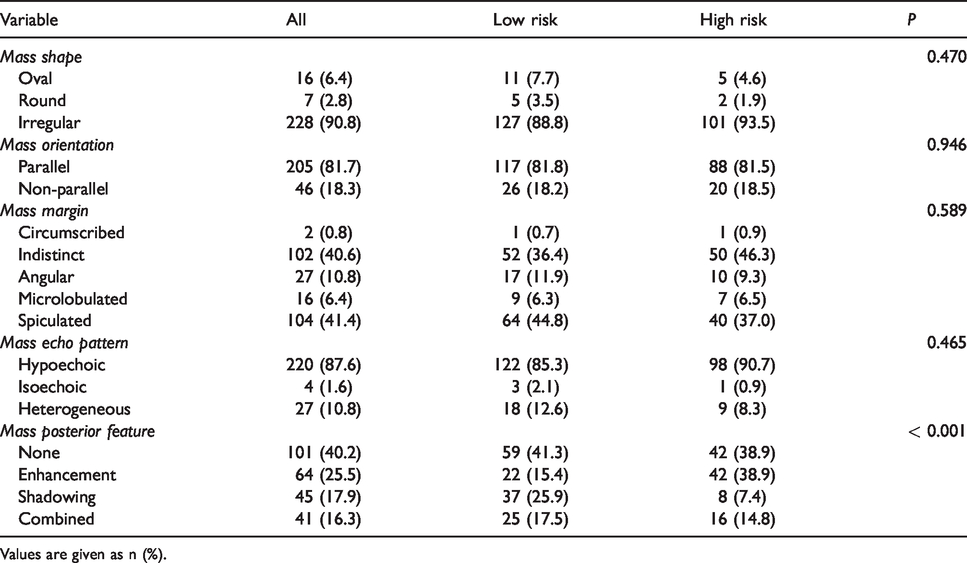
Values are given as n (%).

A 64-year-old woman with a MammaPrint result of 0.2 (low risk). (a) Mammography image showing spiculated irregular-shaped mass without calcification (arrow) in the scattered areas of fibroglandular density of the right breast. (b) Breast ultrasound image showing spiculated mass with no posterior feature (arrow).
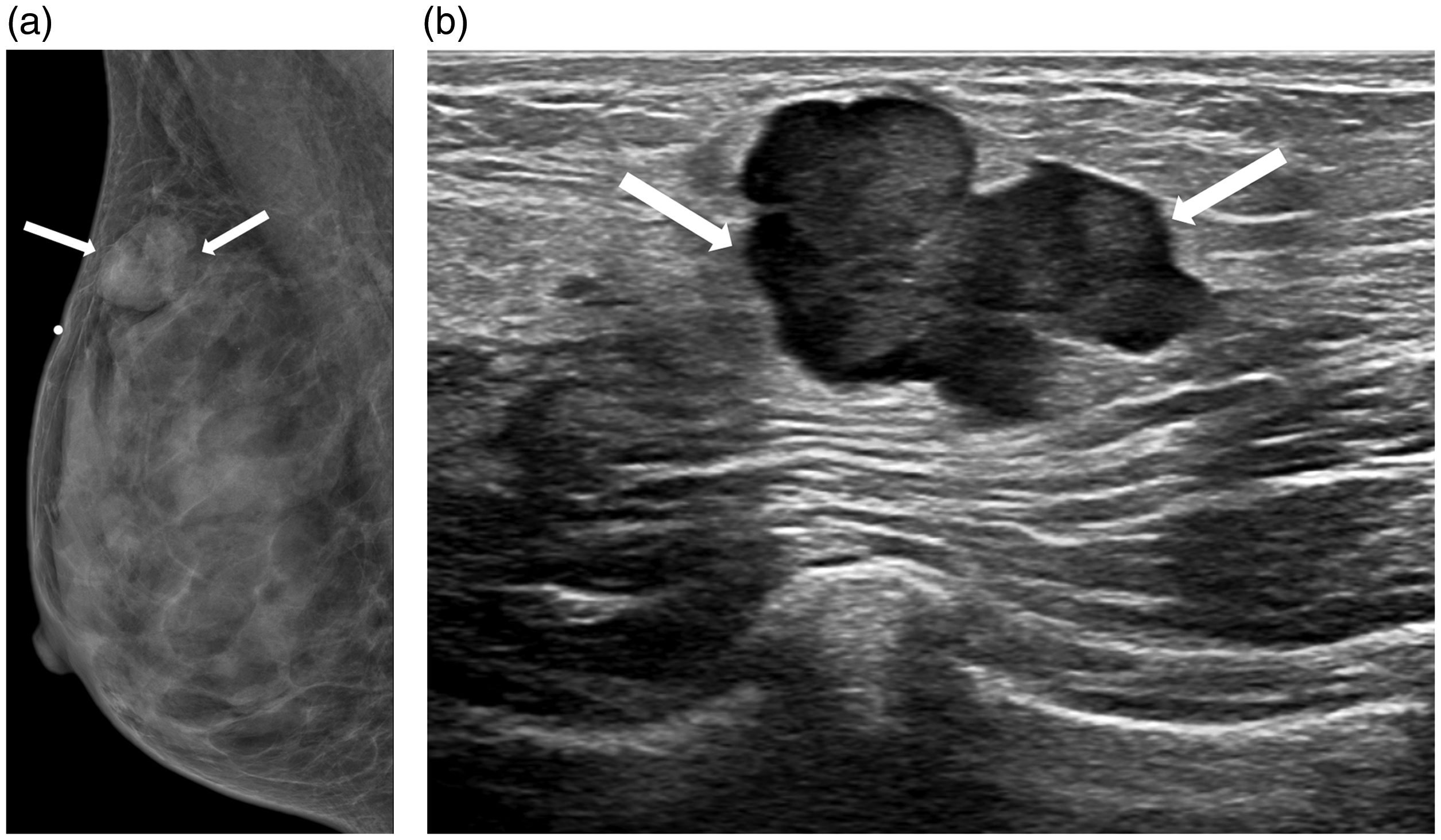
A 44-year-old woman with a MammaPrint result of –0.2 (high risk). (a) Mammography image showing indistinct irregular-shaped mass without calcification (arrow) in the extremely dense parenchymal tissues of the right breast. (b) Breast ultrasound image showing irregular mass with posterior enhancement (arrow).
Clinicopathological and imaging features associated with high risk of recurrence based on logistic regression analysis.
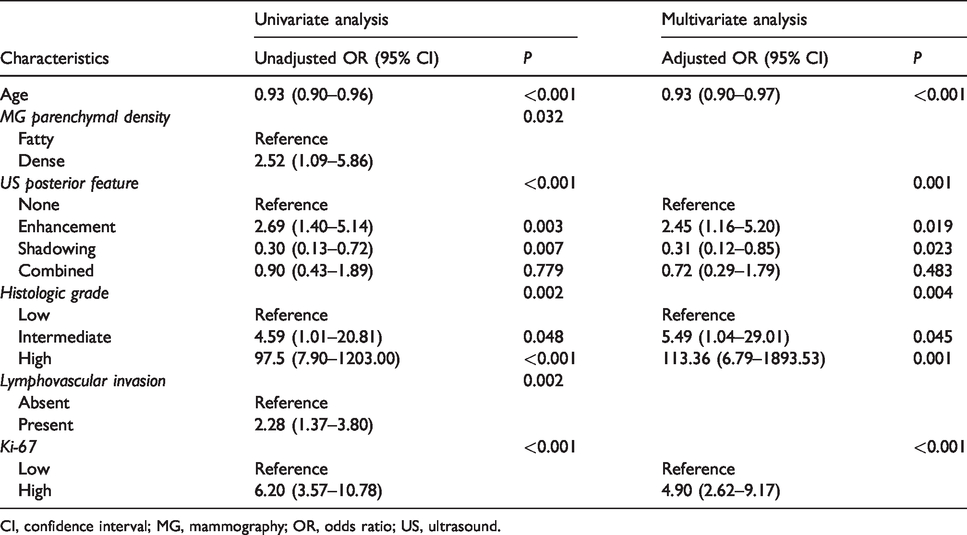
CI, confidence interval; MG, mammography; OR, odds ratio; US, ultrasound.
Logistic regression analysis
Univariate analyses showed that the high-risk group according to MammaPrint results was significantly associated with age (P < 0.001), mammographic parenchymal density (P = 0.032), posterior features in US (P < 0.001), histologic grade (P = 0.002), lymphovascular invasion (P = 0.002), and level of Ki-67 (P < 0.001). Multivariate logistic regression analysis showed that younger age (odds ratio (OR) = 1.08; 95% confidence interval (CI) = 1.04–1.12; P < 0.001), posterior enhancement on US (OR = 2.45; 95% CI = 1.16–5.20; P = 0.019), absence of posterior shadowing on US (OR = 3.19; 95% CI = 1.17–8.62; p = 0.023), high histologic grade (OR = 113.36; 95% CI = 6.79–1893.53; P = 0.001), and high levels of Ki-67 (OR = 4.90; 95% CI = 2.62–9.17; P < 0.001) were independent factors associated with high recurrence score. The Az values for age, posterior feature, histologic grade, and levels of Ki-67 were 0.67, 0.54, 0.60, and 0.71, respectively (Fig. 3). Also, the Az increased to 0.84 in the model in which all independent variables were used.
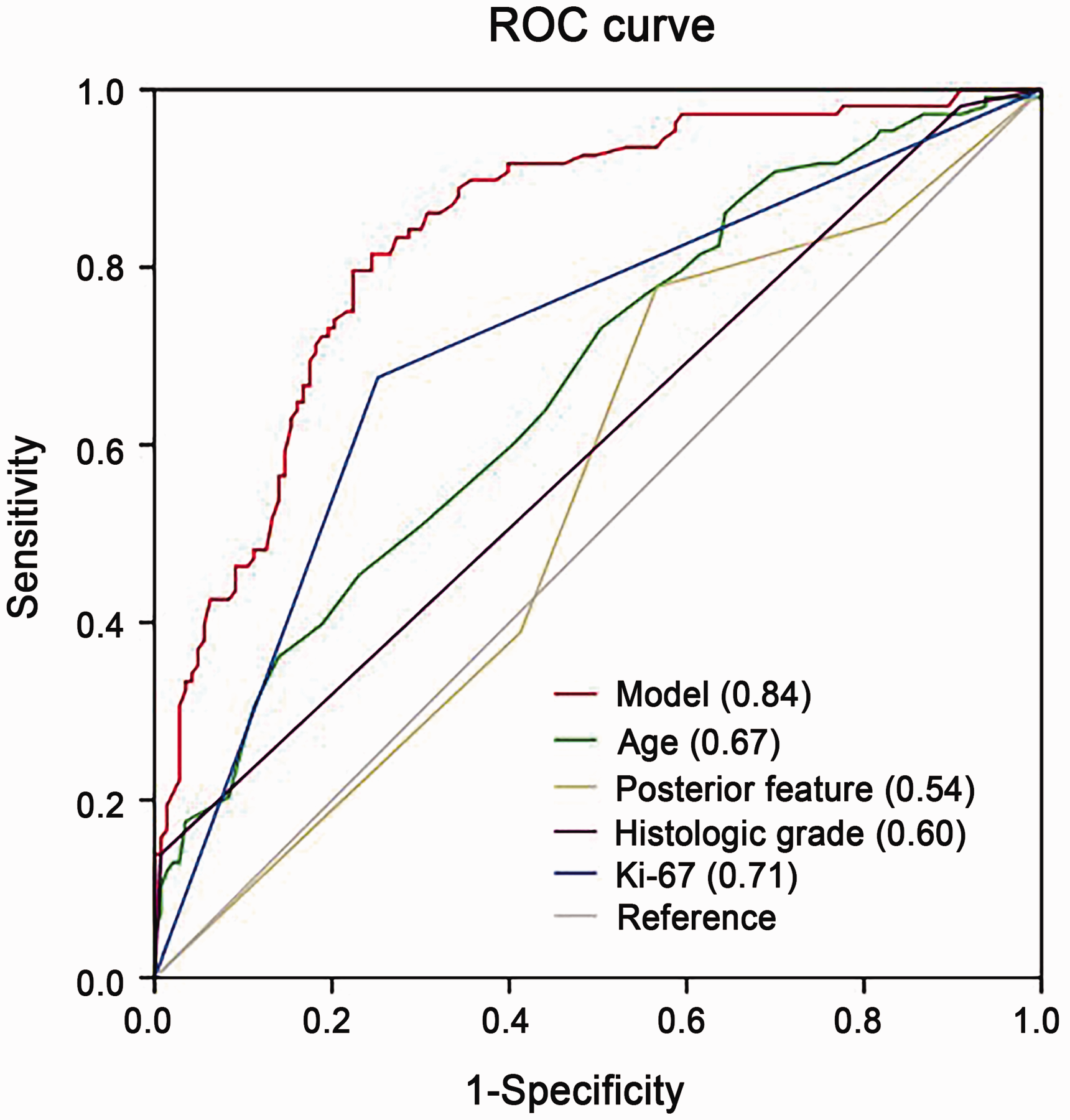
Receiver operating characteristic curve determined by multivariate logistic regression analysis for distinguishing high recurrence scores from low or intermediate recurrence scores. Data in parentheses indicate the Az values for each variable.
Discussion
Here, we observed that patients with ER-positive, HER2-negative, node-positive invasive breast cancer have different clinicopathological and imaging features according to the risk of recurrence as determined by the MammaPrint results. Posterior enhancement and absence of posterior shadowing in US images were independently associated with a high risk of recurrence. Additionally, young age, high histologic grade, and high levels of Ki-67 were more frequently observed in the high-risk group.
The posterior features in US images represent the attenuation characteristics of the mass. In our study, posterior enhancement (OR = 2.45; P = 0.019) and absence of posterior shadowing (OR = 3.19; P = 0.023) were identified as independent factors for the high-risk group. Posterior acoustic enhancement was reported to be associated with a high histological grade (17), and this finding corroborated the findings of previous studies in which posterior enhancement was correlated with the Oncotype DX results in the high-risk group (12,14,15). As high-grade tumors have higher mitotic rates and higher cellularity, they show less attenuation in the US waves, which leads to posterior enhancement. In contrast, low-grade tumors may show posterior shadowing as they are slow-growing and have lower mitotic rates, thus leading to marked differences in the acoustic impedance of tumor interfaces (18).
On mammography, the high-risk group showed significantly higher breast density (P = 0.027) and a higher number of masses with indistinct margins (P = 0.021), although these were not identified as independent predictive factors for high risk of recurrence in logistic regression analysis. Masses with indistinct margins are associated with a higher histologic grade and presence of extensive intraductal component (17). Woodard et al. (19) observed that while the indistinct mass margin had the highest Oncotype DX recurrence score, the breast density was inversely correlated with the Oncotype DX recurrence score. In our study, spiculated margins were associated with the low-risk group, which is consistent with the findings of a previous study in which spiculated margins were associated with low-grade breast tumors (20) and a more favorable prognosis (21). Increased breast density is a known risk factor for breast cancer (22), and although there is controversy regarding the association between breast density and breast cancer-specific survival, some studies have reported that dense breasts were associated with decreased breast cancer-specific survival (23,24).
Analysis of the relationships among imaging features, gene expression profiles, and patient outcomes may provide important information for individual patients. Moreover, the Oncotype DX assay has been widely used to predict the prognosis of patients with ER-positive, HER2-negative, early-stage breast cancer. However, while the recurrence score classifies tumors into low- (<18), intermediate- (18–30), or high-risk (≥31) groups, there is controversy regarding the intermediate-risk group with respect to the efficacy of adjuvant chemotherapy. Sparano et al. (25) reported similar efficacy of the adjuvant endocrine therapy and chemo-endocrine therapy in patients with mid-range Oncotype DX recurrence score, although limited benefits of chemotherapy were observed in some women aged ≤50 years.
The MammaPrint assay, as opposed to the Oncotype DX, classifies patients into low- or high-risk groups, and may aid clinicians in decision-making regarding additional treatment. The MammaPrint assay is a prognostic parameter in the St. Gallen and European Society of Medical Oncology (ESMO) guidelines (26,27). Mook et al. (28) demonstrated that the MammaPrint assay may be used to identify low-risk patients among those with 1–3 node-positive breast cancer, who are traditionally considered high-risk patients for recurrence based on the conventional histopathological evaluation; specifically, their study showed that the 70-gene signature was the most powerful predictor of breast cancer-specific survival even after adjustment for clinicopathological factors.
In the present study, clinicopathological variables such as age, histologic grade, and levels of Ki-67 were associated with the high-risk group. The high histologic grade variable had the highest OR for predicting the high-risk group in multivariate analysis. These results are consistent with those of previous studies in which the histologic grade was reported as a strong prognostic and predictive factor for the outcomes of patients with breast cancer (29,30). Ki-67 is a proliferation marker that serves as an independent prognostic factor (31) and was included in the Oncotype DX assay (2). Moreover, younger women with breast cancer may show aggressive tumors with worse prognoses (32).
The present study has several limitations. First, this was a retrospective study involving a limited number of patients from a single tertiary referral center. Second, US imaging analysis was based on static images and real-time evaluation was not possible. Finally, we only evaluated the relationship between imaging features and the MammaPrint result, and the actual tumor recurrence in patients was not evaluated. In a future study, correlating the imaging features with tumor recurrence and developing a model for predicting high recurrence scores may further aid in the decision for treatment.
In conclusion, we report that young age, posterior enhancement on US imaging, absence of posterior shadowing on US imaging, high histologic grade, and high levels of Ki-67 were independent predictors for high recurrence score in patients with ER-positive, HER2-negative, node-positive invasive breast cancer. The posterior features in US images may predict a high risk of recurrence in such patients, thus providing added diagnostic value and aiding in decision-making regarding additional treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.