
Abstract
Background
The inferior phrenic artery (IPA) is the most common extrahepatic feeder for hepatocellular carcinoma (HCC) during transhepatic arterial chemoembolization (TACE).
Purpose
To compare the incidence of diaphragmatic weakness in patients with HCC after TACE of the right IPA conducted using either N-butyl cyanoacrylate (NBCA) or gelatin sponge particles.
Material and Methods
Medical records of 111 patients who underwent TACE of the right IPA using NBCA were retrospectively reviewed and compared with data from 135 patients with IPA embolization using gelatin sponge particles.
Results
The incidence of diaphragmatic weakness after the initial TACE procedure did not significantly differ between the groups (NBCA group 16.2%; gelatin sponge group 20.7%; P = 0.458). Five patients in the NBCA group and 11 in the gelatin sponge group showed spontaneous resolution of diaphragmatic weakness after a mean period of 3.5 months. Diaphragmatic weakness developed after the initial follow-up visit in 17 patients from the gelatin sponge group due to repeated TACE of the right IPA (mean 2.4 sessions; range 2–4 sessions), while it spontaneously developed without additional TACE procedures in one patient from the NBCA group. Permanent diaphragmatic weakness was less common in the NBCA than in the gelatin sponge group (12.6% and 25.2%, respectively; P = 0.017). The complete response rate did not significantly differ between the groups (NBCA group 16.2%; gelatin sponge group 25.9%; P = 0.065).
Conclusion
Use of NBCA rather than gelatin sponge particles for TACE of the right IPA resulted in a lower incidence of permanent diaphragmatic weakness.
Keywords
Introduction
Extrahepatic collateral vessels play an important role in maintaining the presence of residual hepatocellular carcinoma (HCC); this can limit the effectiveness of transcatheter arterial chemoembolization (TACE) (1–4). The right inferior phrenic artery (IPA) is the most common source of the extrahepatic collateral blood supply to HCCs (5). TACE of the IPA using gelatin sponge particles with an emulsion of iodized oil and a chemotherapeutic agent can improve control of HCCs, especially in the bare area of the liver (6,7).
The IPA supplies most of the undersurface of the diaphragm. This vessel can communicate with the internal mammary artery, the intercostal artery, and other systemic vessels of the thorax (8,9). However, despite the collateral arterial supply to the diaphragm, ischemic injury of the IPA after TACE can cause diaphragmatic weakness (7–10). Shin et al. (7) reported that TACE of the IPA can induce ipsilateral diaphragmatic weakness; this most likely results from ischemic damage due to the occlusion of the feeding artery, as well as muscle necrosis induced by the toxic anticancer agent.
N-butyl cyanoacrylate (NBCA) has been used for many years as a liquid embolic agent (11–14). While the success rate of occlusion with NBCA is relatively high, it can be difficult to handle precisely (11). Previous studies have investigated the embolization of central nervous system tumors using liquid materials such as Onyx or NBCA (15–17), and a limited number of studies have used NBCA for TACE of the hepatic artery in the treatment of HCC (18). However, we are not aware of any studies investigating the use of NBCA for embolization of the right IPA during TACE sessions.
The aim of the present study was to assess clinical outcomes following TACE of the right IPA using NBCA, focusing on the frequency of diaphragmatic weakness, and to draw comparisons with outcomes in patients who underwent TACE of the right IPA using gelatin sponge particles.
Material and Methods
Patient population
This single-center study was approved by the institutional review board, and informed patient consent was waived due to its retrospective nature. Between February 2016 and October 2017, 321 patients with unresectable HCC underwent TACE of the right IPA at our study center. All patients had no hepatic lesions other than HCC. We excluded 75 patients for the following reasons: previous TACE of the right IPA (n = 51) or of bilateral IPAs (n = 11); pre-existing right pleural effusion (n = 8) or pleural calcification due to previous pleuropulmonary disease (n = 3); or loss to follow-up due to early death after TACE (n = 2). The present study therefore involved 246 patients. Of these, 111 received treatment with NBCA between December 2016 and October 2017. Their records were compared with those of 135 patients who underwent TACE using gelatin sponge particles between February 2016 and November 2016. Demographic and clinical characteristics are summarized in Table 1.
Patent characteristics.
Values are given as n (%), mean (range), or mean ± SD.
*Old pulmonary tuberculosis (n = 13), active pulmonary tuberculosis (n = 2), emphysema (n = 11), bronchiectasis (n = 5), pulmonary thromboembolism (n = 2), interstitial lung disease (n = 3), pneumonectomy state (n = 1).
HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; LC, liver cirrhosis; NBCA, N-butyl cyanoacrylate; NBNC, non-B non-C; SD, standard deviation; TACE, transcatheter arterial chemoembolization.
TACE technique
TACE was performed by eight interventional radiologists with 10–32 years of experience. Among the eight intervention radiologists, one used NBCA and the others used gelatin sponge particle for IPA embolization. All the operators have performed the TACE procedure in the same center for more than 10 years with almost the same techniques, and the patients are randomly distributed for the TACE procedure. Before TACE, selective digital angiography of the superior mesenteric and celiac or common hepatic arteries was performed with a 5-F angiographic catheter (Rösch hepatic catheter; Cook, Bloomington, IN, USA) to assess the vascular anatomy, the extent and vascularity of tumors, and portal vein patency. In most patients, conventional TACE was performed using cisplatin (2 mg/kg) or doxorubicin (25–50 mg). In some patients, if clinically indicated, TACE was performed using drug-eluting beads (HepaSphere; Merit Medical, South Jordan, UT, USA).
In patients treated with cisplatin, this drug was infused into segmental or lobar hepatic arteries using microcatheters (Progreat Alpha; Terumo, Tokyo, Japan or Veloute; Asahi Intec Co. Ltd., Nagoya, Japan), and then an emulsion of cisplatin in iodized oil (Lipiodol; Guerbet, Roissy, France) was manually infused into the segmental branches or the more peripheral branches of hepatic arteries. In patients treated with doxorubicin, an emulsion of doxorubicin in iodized oil was directly infused into the feeding branches. After infusion of the chemotherapeutic agent and iodized oil, the feeding arteries were then embolized with a slurry of gelatin sponge particles (CaliGel; Alicon, Zhejiang, China; 150–350 µm) until stasis of blood flow was achieved.
When drug-eluting beads were used, tumor-feeding arteries were super-selected and then drug-eluting beads loaded with a maximum dose of 50 mg doxorubicin were slowly injected at the level of the subsegmental arteries until stasis of blood flow was achieved. If feeding vessels were still visible, additional embolization was then performed using gelatin sponge particles.
After TACE of the hepatic artery, angiography of extrahepatic collateral vessels was performed in the same session according to tumor location, especially in patients with no or insufficient tumor blush on the hepatic angiogram in spite of a visible tumor on computed tomography (CT) scans or magnetic resonance imaging (MRI). A collateral supply of a hepatic tumor via the right IPA was suspected if the following findings were observed: hepatic tumors abutting the bare area of the liver; visualization of a hypertrophied IPA; a peripheral defect in iodized oil retention within the tumor seen on follow-up CT; local recurrence at the periphery of the treated tumor during follow-up; no definitive tumor blush on routine hepatic angiography; or injury to the hepatic artery after multiple TACE sessions.
Selective digital subtraction angiography of the right IPA was performed using a 5-F angiographic catheter or a microcatheter. If tumor blush was visible on the right IPA angiogram, TACE of the right IPA was performed. In some patients, according to the operator’s judgement, 5–10 mL of lidocaine (Lidocaine hydrochloride 1%, Jeil Pharmaceutical, Daegu, Republic of Korea) was injected before embolization to reduce pain.
When gelatin sponge particles were used for IPA embolization, approximately 2–5 mL of iodized oil mixed with 4–10 mL of a chemotherapeutic agent was carefully injected until complete accumulation of iodized oil in the tumor was seen, while paying careful attention to reflux into non-target branches. Gelatin sponge particles were used to achieve complete embolization of the right IPA.
When NBCA was used for IPA embolization, a 1:8–1:10 mixture of NBCA with iodized oil was slowly injected by hand after flushing the microcatheter with 5% dextrose. The dilution of NBCA varied depending on differences in arterial flow and the operator’s preference. In patients with visible pulmonary shunting or mediastinal branches seen on the right IPA angiogram, the iodized oil emulsion was infused super-selectively into each feeding branch before embolization of the IPA using NBCA. When drug-eluting beads were used for TACE, beads loaded with doxorubicin were infused before embolization of the right IPA using NBCA. If super-selective embolization of each feeding branch was impossible, only NBCA was used for embolization.
Evaluation of diaphragmatic weakness and other complications
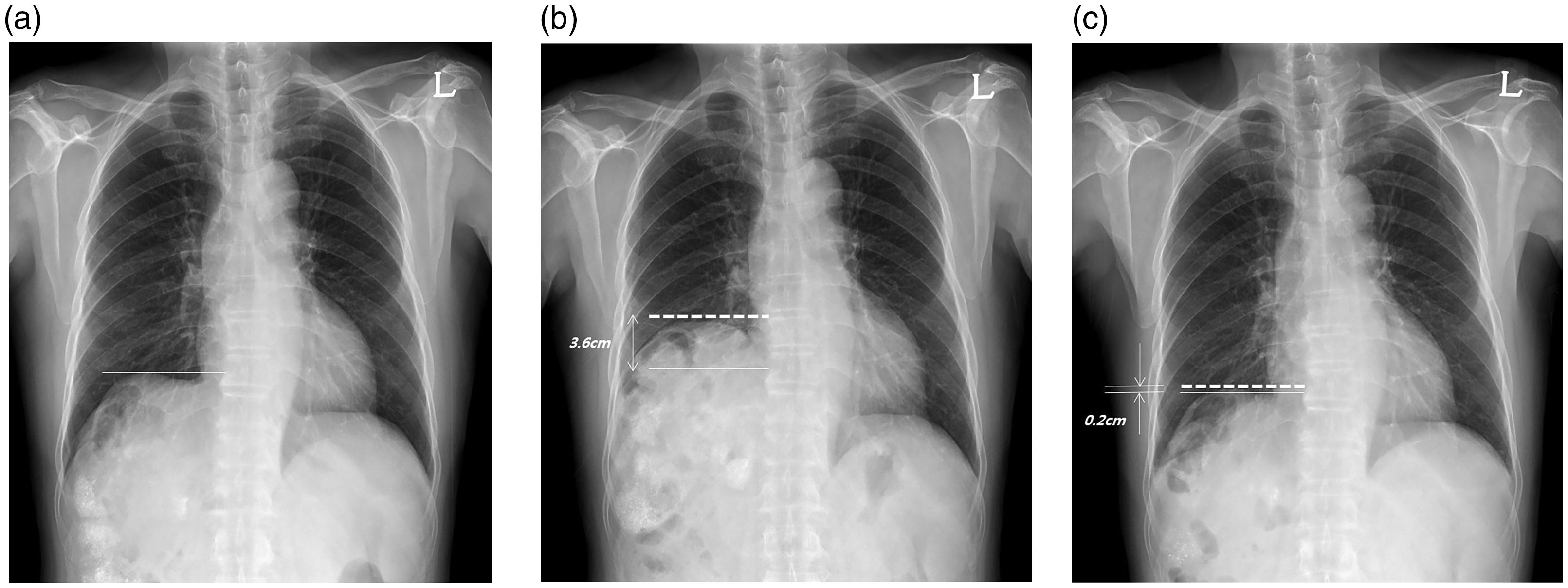
Chest radiography was performed for all patients before TACE and within six weeks afterwards. We analyzed chest radiographs and fluoroscopy images for evidence of diaphragm elevation and abnormal diaphragmatic movement. Patients whose right diaphragmatic dome was elevated > 2 cm after TACE of the right IPA, as determined by comparison of the post-TACE and pre-TACE chest radiographs, were considered to have diaphragmatic weakness (Fig. 1) (19).
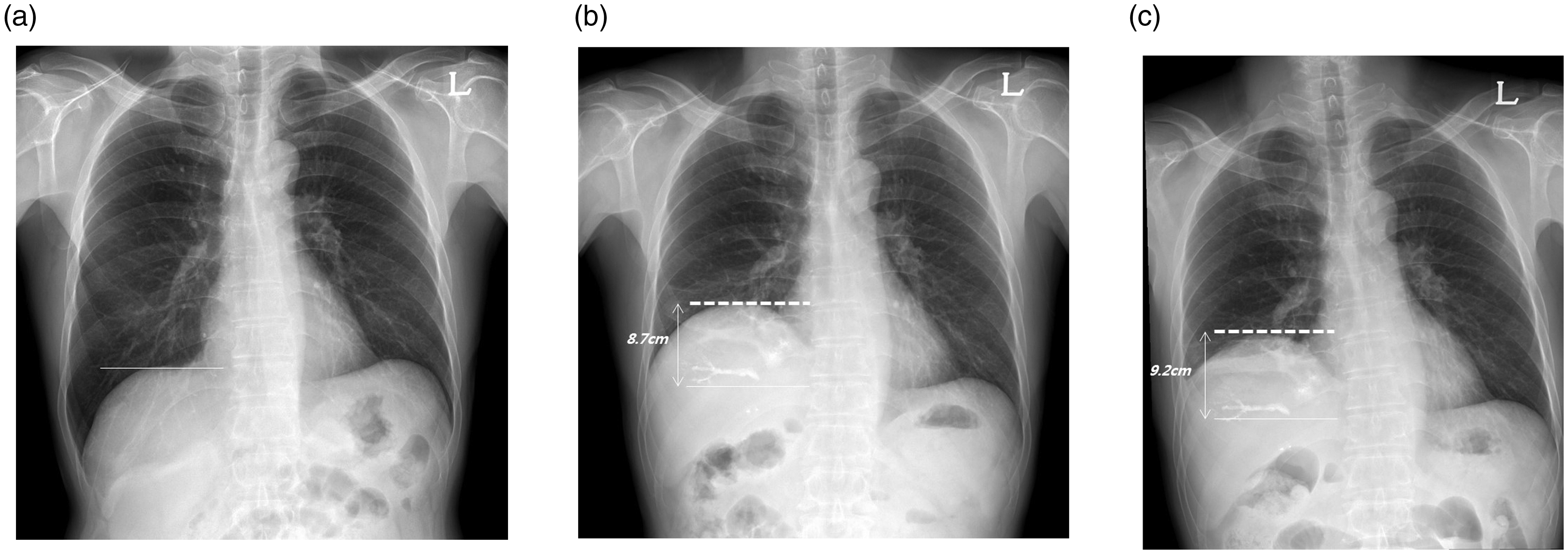
Assessment of diaphragmatic weakness using chest radiography. Chest radiographs were obtained before (a) and two weeks after (b) embolization of the right inferior phrenic artery. Solid lines indicate the level of the right hemidiaphragmatic dome on the initial chest radiograph. The dotted line indicates the level at follow-up. The right hemidiaphragm was elevated >2 cm on the follow-up chest radiograph (b). (c) Diaphragmatic weakness had not resolved at the four-week follow-up; it was therefore classified as permanent.
Chest fluoroscopy was performed in 51 patients in the NBCA group, both before the initial TACE session and at the first follow-up, over at least two respiratory cycles including deep inspiration and deep expiration. Fluoroscopy was not performed in the gelatin sponge group. Paradoxical or decreased movement (>50% decrease) of the affected hemidiaphragm during chest fluoroscopy was considered to indicate diaphragmatic weakness (Fig. 2a and b) (8). Although chest fluoroscopy was only performed for 51 of 118 patients (43.2%) in the NBCA group, the findings from follow-up chest radiography and fluoroscopy corresponded well (Fig. 2c). Thus, we used chest radiography as the main tool for diagnosing diaphragmatic weakness. We continued to monitor for the development of diaphragmatic weakness during the follow-up period with repeated TACE procedures, even in patients without initial diaphragmatic weakness.
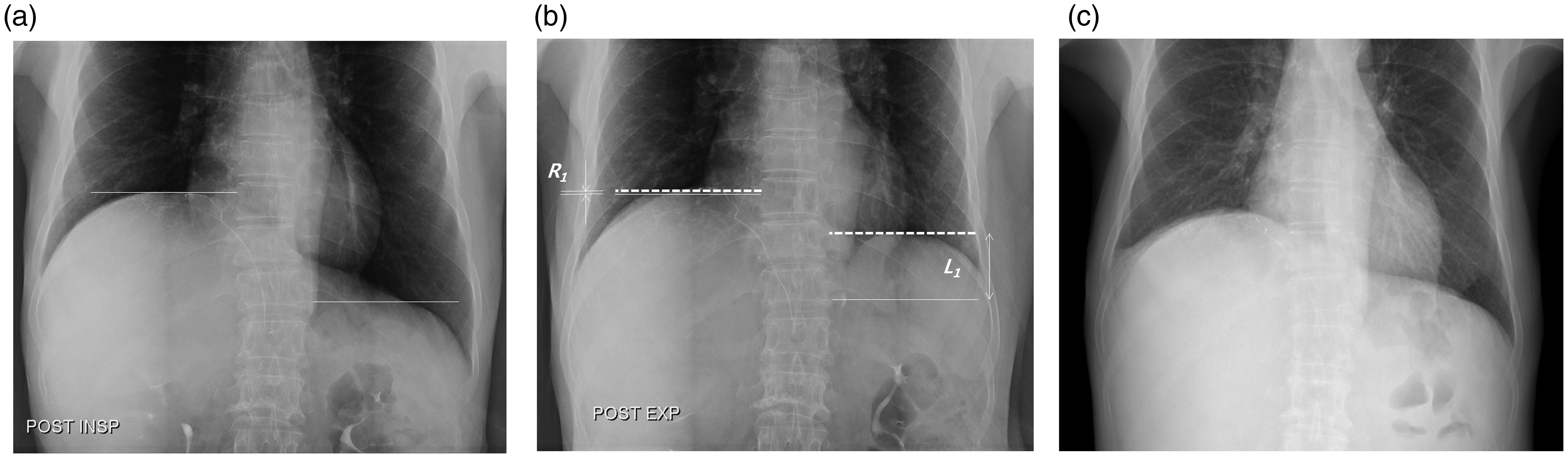
Assessment of diaphragmatic weakness using chest fluoroscopy and radiography. Inspiratory (a) and expiratory (b) chest fluoroscopy images were obtained after embolization of the right inferior phrenic artery. Solid lines indicate the level of each hemidiaphragmatic dome in the inspiratory phase, while dotted lines signify the levels in the expiratory phase. R1 and L1 indicate the movement of the right and left hemidiaphragms. (c) The one-week follow-up chest radiograph with full inspiration shows that the level of each hemidiaphragm was consistent with the fluoroscopy findings, which reflects that the radiograph can be used for evaluation of diaphragmatic weakness when the fluoroscopy is not available.
Complications were classified as major or minor, according to the Society of Interventional Radiology Standards of Practice Committee guidelines (20).
Local tumor response and survival outcomes
Local response of the tumor fed by the IPA was evaluated using three-month post-treatment imaging, according to the modified Response Evaluation Criteria in Solid Tumors (mRECIST). Thorough assessment of both CT/MRI and angiographic images was performed (21,22). The disease control rate was defined as the percentage of patients who achieved a complete response, partial response, or stable disease on the three-month follow-up imaging study (23,24). Local tumor recurrence was defined as any recurrence abutting the tumor supplied by the IPA observed on follow-up angiography and CT/MRI. Overall survival was calculated from the date of initial embolization of the IPA to the date of death or the last follow-up (23). Serum levels of alpha-fetoprotein (AFP) and protein induced by vitamin K absence-II (PIVKA-II) were measured before and three months after the procedure.
NBCA is a permanent embolic material; this raises the concern that after the IPA is occluded in the initial TACE procedure, the recurred or residual tumor could be supplied by other extrahepatic collaterals such as the internal thoracic artery, the intercostal artery, or other systemic arteries at subsequent TACE sessions. Therefore, we aimed to actively perform angiography for extrahepatic collaterals and to treat vessels with positive tumor staining in cases of recurrence. Even if angiography for the suspected parasitic supply was not performed, we considered the newly developed hypertrophied vessels seen on follow-up CT or MRI to be potential feeder vessel candidates for recurred/residual tumors.
Statistical analysis
Continuous variables were compared between the two groups using the t-test or Mann–Whitney U test, while categorical variables were compared using the chi-square test or Fisher’s exact test. The overall survival rate was analyzed with the Kaplan–Meier method. All statistical analyses were performed using SPSS software (version 20.0; SPSS, Chicago, IL, USA), with P values < 0.05 considered to be statistically significant.
Results
TACE of the right IPA
In the NBCA group, TACE of the right IPA was technically successful in all patients. There was no non-target embolization. TACE using only NBCA was performed in 40 patients, while iodized oil emulsion was infused before NBCA embolization (Fig. 3) in 63 patients, and drug-eluting beads were infused in eight patients. TACE through both the anterior and posterior branches of the right IPA was performed in 110 patients. One patient underwent TACE through a single anterior branch of the right IPA. All 111 patients underwent one session of IPA embolization.
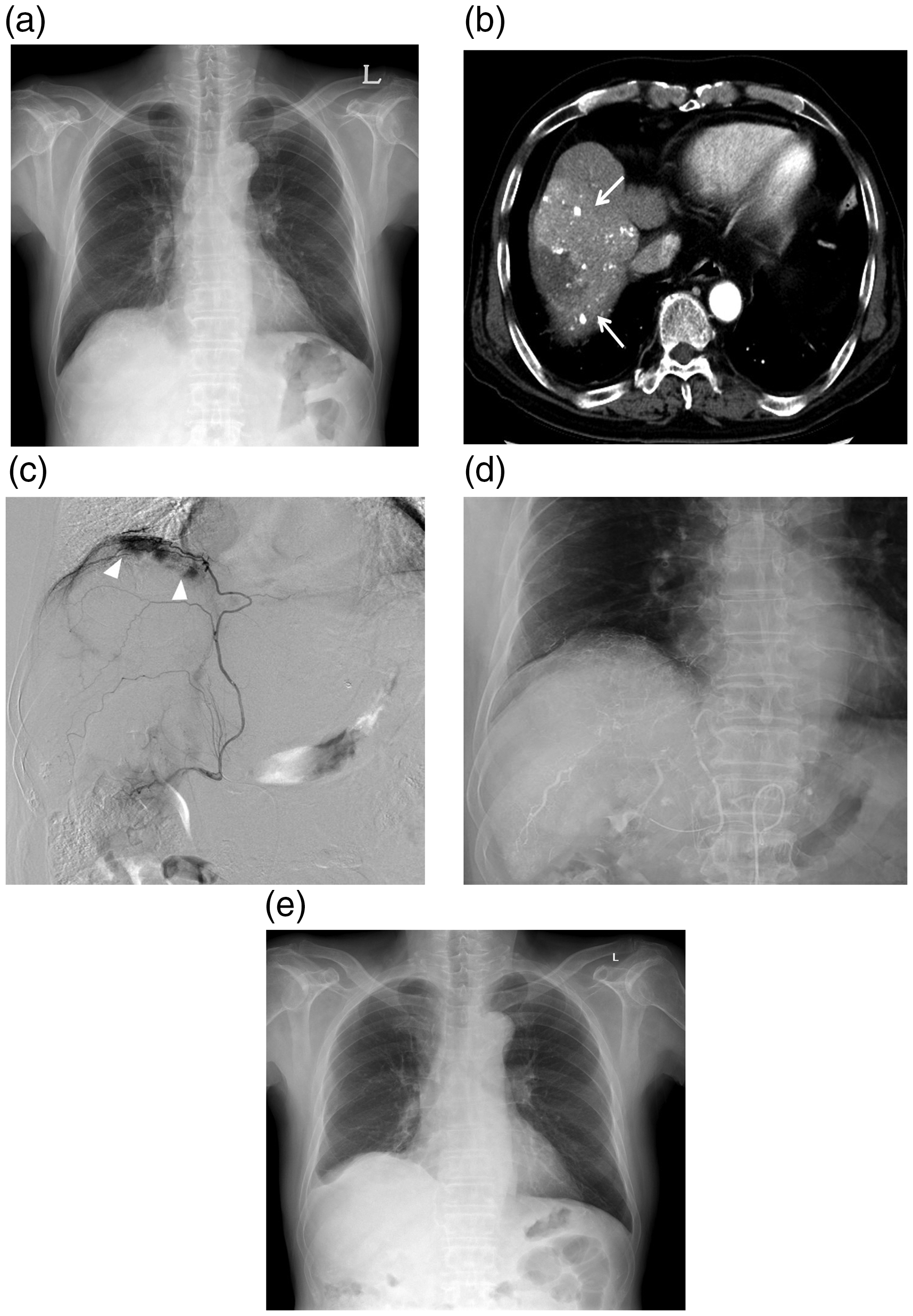
A 68-year-old male with underlying alcoholic liver cirrhosis who presented with residual HCC. (a) Chest radiography was performed before the TACE procedure. (b) An arterial phase axial CT image shows a viable hepatocellular carcinoma with partial iodized oil uptake in the right hepatic dome (arrows). (c) On selective right IPA angiography, there is hypervascular tumor staining in the right hepatic dome; the tumor is fed by an anterior branch (arrowheads). (d) The right IPA was embolized with N-butyl cyanoacrylate and iodized oil at a ratio of 1:10. (e) The follow-up chest radiograph shows elevation of the right hemidiaphragm, which did not resolve during follow-up. CT, computed tomography; IPA, inferior phrenic artery; TACE, transcatheter arterial chemoembolization.
In the gelatin sponge group, 15 patients underwent TACE through a single branch of the right IPA: the anterior and posterior branches in seven and eight patients, respectively. TACE through both the anterior and posterior branches was performed in the remaining 120 patients. Sixty-seven patients underwent one TACE session for IPA embolization, 33 underwent two sessions, 15 underwent three, 13 underwent four, six underwent five, and one underwent six (mean = 2 sessions).
Diaphragmatic weakness
No patients had clinical symptoms of diaphragmatic weakness. The results regarding diaphragmatic weakness are summarized in Table 2 and the patient selection flow chart is shown in Fig. 4. Diaphragmatic weakness after the initial TACE procedure occurred in 18 of 111 patients (16.2%) in the NBCA group and in 28 of 135 patients (20.7%) in the gelatin sponge group; these rates were not significantly different (P = 0.458). The mean diaphragmatic elevation was 28 mm (range = 21–40 mm) in the NBCA group and 34 mm (range = 21–70 mm) in the gelatin sponge group. Among the 46 patients who developed diaphragmatic weakness after TACE, 13 from the NBCA group and 17 from the gelatin sponge group had permanent diaphragmatic weakness. Five patients in the NBCA group and 11 in the gelatin sponge group experienced spontaneous resolution of diaphragmatic weakness during follow-up after a mean period of 3.5 months (range = 1–13 months) (Fig. 5).
Diaphragmatic weakness in NBCA and gelatin sponge group.
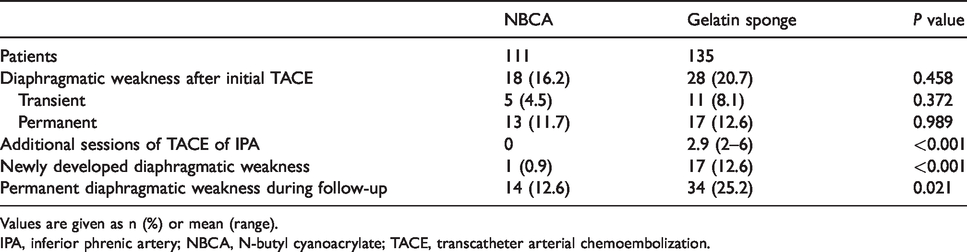
Values are given as n (%) or mean (range).
IPA, inferior phrenic artery; NBCA, N-butyl cyanoacrylate; TACE, transcatheter arterial chemoembolization.
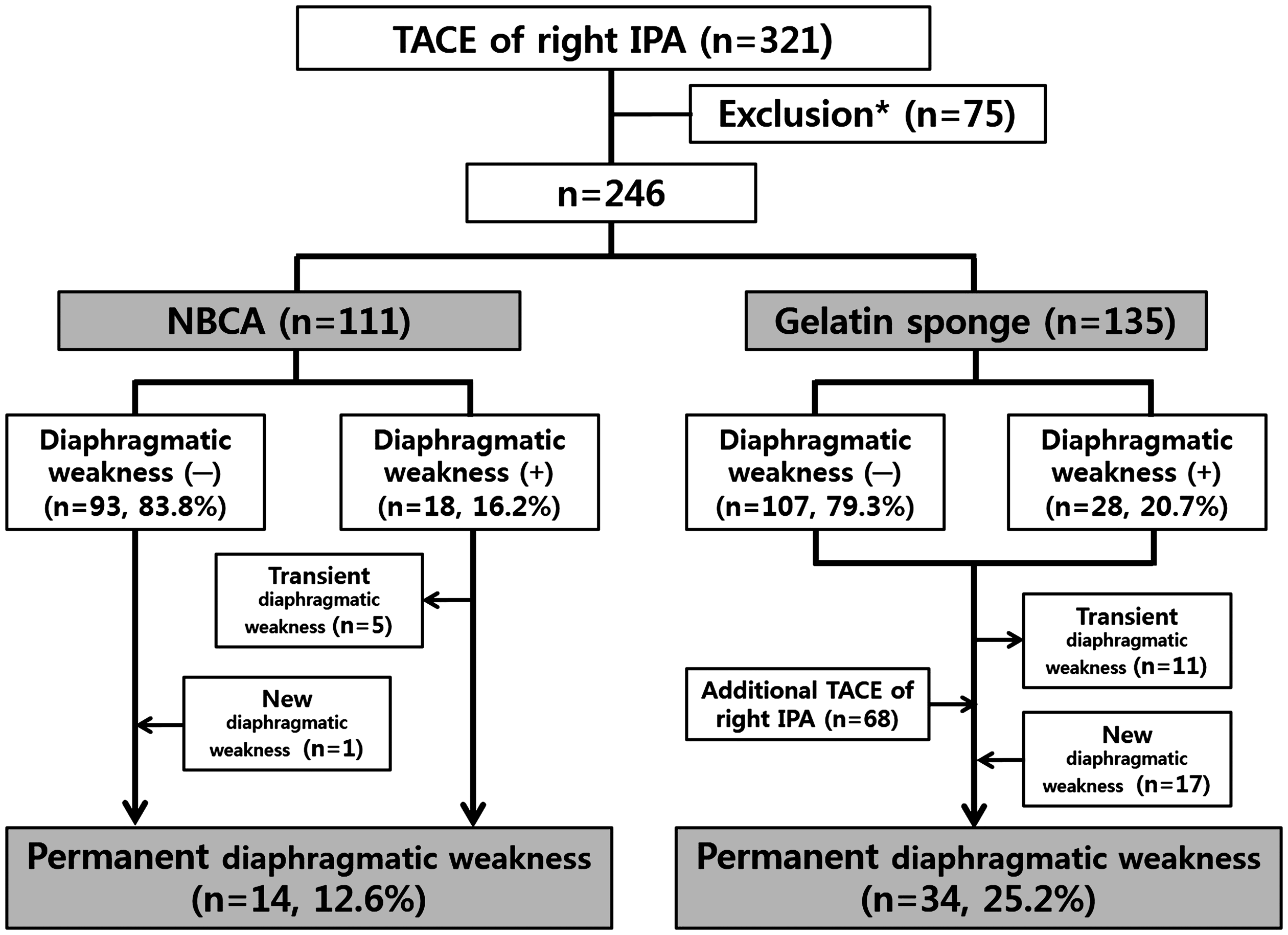
Flow chart showing the selection of the study patients. Exclusion criteria: previous TACE of the right IPA (n = 51) or TACE of both IPAs (n = 11), the presence of a right pleural effusion (n = 8) or pleural calcification due to previous pleuropulmonary disease (n = 3), and loss to follow-up due to early death after TACE (n = 2). IPA, inferior phrenic artery; TACE, transcatheter arterial chemoembolization.
Assessment of diaphragmatic weakness using chest radiography: transient diaphragmatic weakness. Chest radiographs were obtained before (a), one month after (b), and 18 months after (c) embolization of the right inferior phrenic artery. Solid lines indicate the level of the right hemidiaphragmatic dome on the initial chest radiograph. Dotted lines indicate the level at follow-up. (b) The right hemidiaphragm was elevated > 2 cm in comparison to the pre-procedural chest radiograph. (c) The difference was decreased on the 18-month follow-up radiograph, and this was therefore classified as transient diaphragmatic weakness.
During the follow-up period (mean duration =354 days; range = 17–914 days), 68 patients in the gelatin sponge group underwent repeated TACE of the right IPA with a mean of 2.9 sessions (range = 2–6 sessions). Newly developed diaphragmatic weakness after the initial follow-up was observed in 18 patients (one in the NBCA group and 17 in the gelatin sponge group). One patient in the NBCA group experienced spontaneous diaphragmatic weakness two months after initial TACE of the right IPA. All 17 patients with newly developed diaphragmatic weakness in the gelatin sponge group had undergone repeat TACE of the right IPA, with a mean of 2.4 additional sessions (range = 2–4 sessions).
The overall incidence of permanent diaphragmatic weakness was significantly lower in the NBCA group (12.6%, 14/111 patients) than the gelatin sponge group (25.2%, 34/135 patients; P = 0.021) (Table 2). Among the 14 patients in the NBCA group who developed permanent diaphragmatic weakness, five were from the group of 40 patients who underwent only NBCA embolization, and nine were from the group of 71 patients who underwent NBCA embolization following the infusion of iodized oil emulsion (n = 63) or drug-eluting beads (n = 8). There was no significant difference in the rate of permanent diaphragmatic weakness between patients who received only NBCA and those who received NBCA embolization following iodized oil or drug-eluting beads infusion (P = 0.072). All of the 14 patients in the NBCA group who developed permanent diaphragmatic weakness underwent one TACE session. Of the 34 patients who developed permanent diaphragmatic weakness in the gelatin sponge group, 17 underwent one TACE session, 13 underwent two, two underwent three, and two underwent four (mean = 1.7 sessions).
Efficacy and survival outcomes
The median follow-up period was 33.2 months. The disease control rate according to the mRECIST criteria did not significantly differ between the two groups. The complete response rate was 16.2% in the NBCA group and 25.9% in the gelatin sponge group (P = 0.065). The objective response rate (complete response rate plus partial response rate) showed a tendency to be higher in the gelatin sponge group, though the difference between the groups was not significant (NBCA group = 56.8%; gelatin sponge group = 67.4%; P = 0.086) (Table 3).
Disease control rate and recurrence.
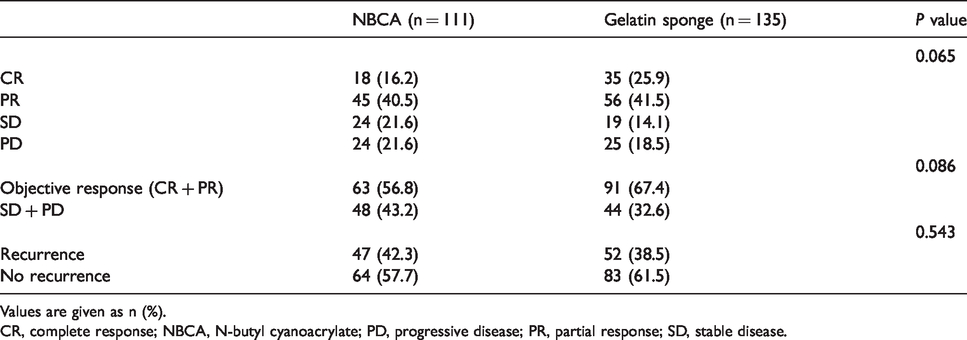
Values are given as n (%).
CR, complete response; NBCA, N-butyl cyanoacrylate; PD, progressive disease; PR, partial response; SD, stable disease.
The recurrence rate did not significantly differ between the two groups (NBCA group = 42.3%; gelatin sponge group = 38.5%; P = 0.543) (Table 3). The one-year overall survival rate also showed no significant difference: 55.4% in the NBCA group and 61.5% in the gelatin sponge group (P = 0.311) (Fig. 6). The differences in pre- and post-treatment levels of AFP and PIVKA-II were not significantly different between the two groups (P = 0.088 and 0.702, respectively) (Table 4).
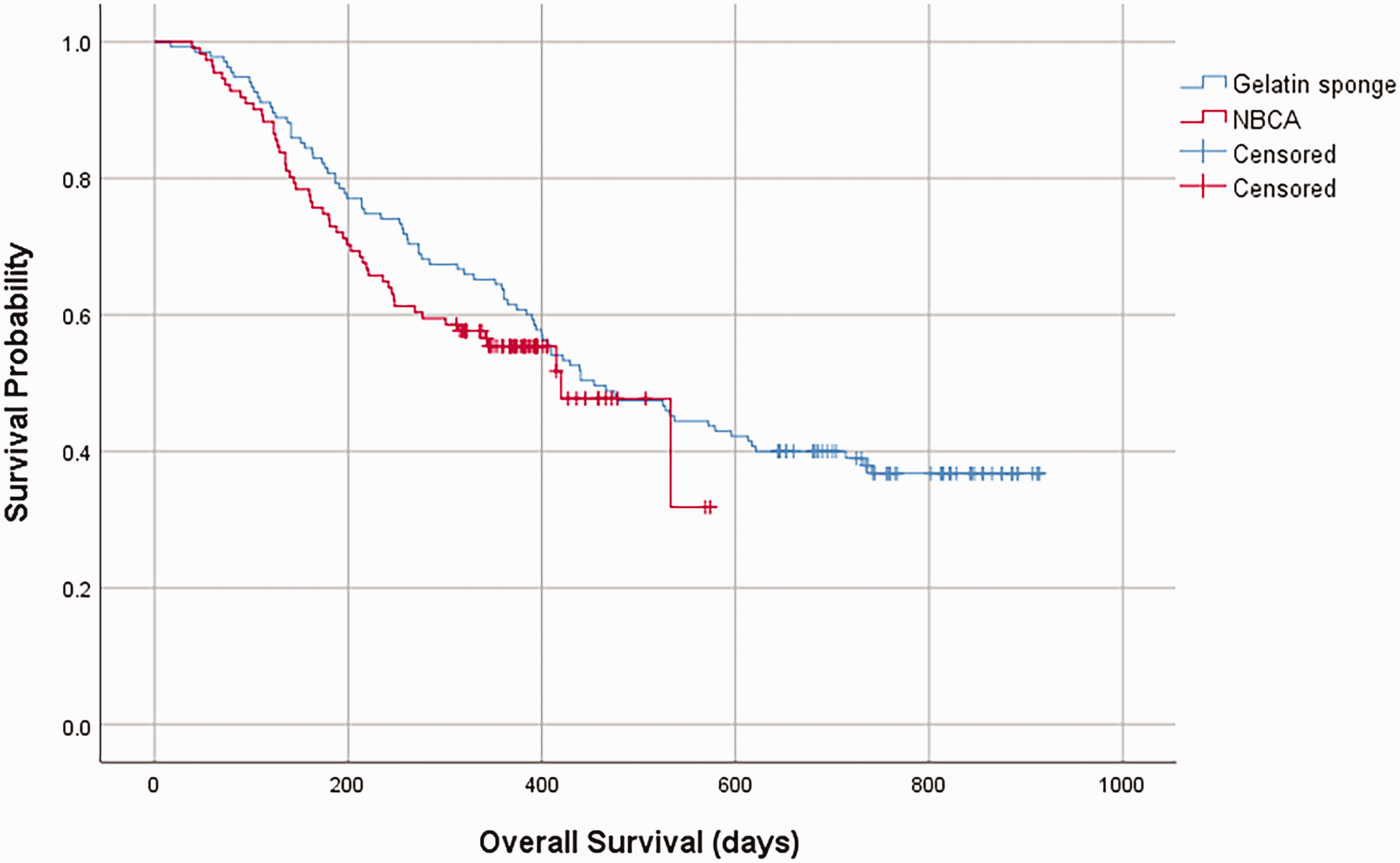
Overall survival
Pre and post AFP and PIVKA.
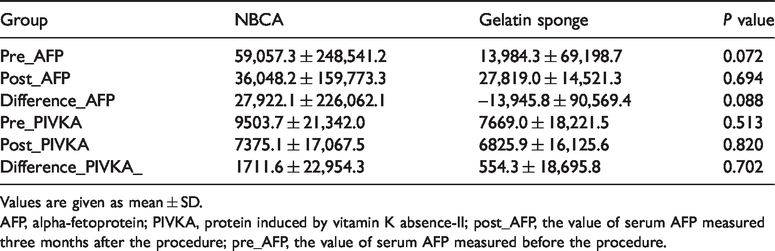
Values are given as mean ± SD.
AFP, alpha-fetoprotein; PIVKA, protein induced by vitamin K absence-II; post_AFP, the value of serum AFP measured three months after the procedure; pre_AFP, the value of serum AFP measured before the procedure.
Of the 246 patients, 99 experienced local recurrence. The percentage of newly developed extrahepatic feeding vessels for the previously treated IPA-fed tumor was 19.1% in the NBCA group and 42.3% in the gelatin sponge group (P = 0.013). The types of these extrahepatic collaterals are shown in Table 5.
Tumor feeding vessels in recurred patients.
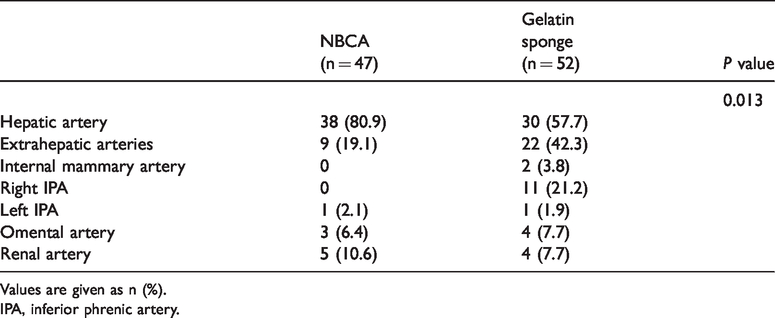
Values are given as n (%).
IPA, inferior phrenic artery.
Clinical findings and complications after TACE of the right IPA
Shoulder pain was observed in some cases, with a significantly higher incidence in the NBCA group (50 patients) than the gelatin sponge group (36 patients; P = 0.004). However, shoulder pain was managed supportively and lasted for an average of two days, and no patients experienced persistent symptoms during hospitalization.
Complications other than diaphragmatic weakness occurred in 4 of 246 patients (1.6%): one in the NBCA group (1/111, 0.9%) and three in the gelatin sponge group (3/135, 2.2%). The minor complication of transient pleural effusion occurred in three patients: one in the NBCA group and two in the gelatin sponge group. The major complication of cerebral iodized oil embolism occurred in one patient in the gelatin sponge group. The overall complication rate did not significantly differ between the two groups (P = 0.598).
Discussion
In the present study, TACE of the right IPA using NBCA was technically successful in all patients. No non-target embolization was observed because the parent catheter was kept in the orifice or the proximal portion of the right IPA. Traditionally, there have been concerns about using NBCA as an embolic agent due to the risk of ischemic injury and the difficulty in handling the material (11,25–28).
Although the incidence of diaphragmatic weakness at the first follow-up visit after initial TACE of the right IPA did not significantly differ between the two groups, the incidence of permanent diaphragmatic weakness was significantly lower in the NBCA group than the gelatin sponge group (12.6% vs. 25.2%; P = 0.017). Previous studies have found the incidence of diaphragmatic weakness to be in the range of 18%–40% after using a similar technique with gelatin sponge particles (7,8).
In the present study, no patient in the NBCA group underwent repeated IPA embolization at the following TACE sessions. Only one patient spontaneously developed diaphragmatic weakness two months after the initial treatment, without further TACE procedures. Thus, although NBCA induced occlusive changes in the right IPA, the lower incidence of permanent diaphragmatic weakness in the NBCA group might be associated with a lesser interruption of the collateral pathways. Shin et al. (7) suggested that liquid chemo-embolic agents may travel relatively far peripherally to reach the anastomotic point of various collateral arteries. This could interrupt potential collateral pathways and cause ischemic damage to the diaphragm. In the NBCA group, the incidence of permanent diaphragmatic weakness was not significantly different in the group treated with NBCA embolization only and the group that received NBCA embolization after the infusion of iodized oil emulsion or drug-eluting beads. Hence, the characteristics of the embolic material might be a more important factor than the prior use of these infusions in inducing permanent diaphragmatic weakness.
As the IPA can be recanalized, repeated embolization is needed in successive TACE sessions when using gelatin sponge particles. However, this can completely block collateral pathways and cause permanent diaphragmatic weakness. In the present study, among the 34 patients with permanent diaphragmatic weakness in the gelatin sponge group, 17 (50%) newly developed diaphragmatic weakness after the initial follow-up due to repeat TACE of the right IPA. Similarly, Lee et al. (8) found that 4 of 11 patients (36.4%) with diaphragmatic weakness underwent more than two TACE sessions for the right IPA. We therefore suggest that repeated TACE of the right IPA might induce occlusive changes and interrupt potential collateral pathways, thus increasing the likelihood of permanent diaphragmatic weakness
In the present study, persistent dyspnea was not observed in any patient. Unilateral diaphragmatic weakness after TACE of the right IPA may not be clinically significant; indeed, most patients with unilateral diaphragmatic weakness are asymptomatic (8). However, unilateral diaphragmatic weakness can initiate or aggravate pulmonary symptoms during later stages of the disease. Moreover, patients with a compromised cardiopulmonary reserve due to co-morbidities can report exertional breathlessness, orthopnea, or sleep disturbances (29,30). It is important to bear in mind that diaphragmatic weakness can cause serious problems in patients with poor collaterals of the IPA (i.e. the internal mammary artery or intercostal artery), contralateral diaphragmatic weakness, or underlying pulmonary disease (5,8). Although the clinical implications of unilateral diaphragmatic weakness after TACE of the right IPA are not clear, using NBCA is effective in reducing the incidence of diaphragmatic weakness and avoiding repeated TACE treatments of the IPA.
We found that the rate of procedure-related complications other than diaphragmatic weakness was only 1.6% in the entire study population. Cerebral Lipiodol embolism was the only major procedure-related complication observed; this occurred in one patient in the gelatin sponge group. In general, patients with advanced liver disease are likely to have a pulmonary arteriovenous shunt, and a right-to-left shunt from the IPA to the pulmonary vasculature is a possible cause of this rare but severe complication (31–33).
There has been limited research investigating the use of NBCA in oncology. In this study, complete and objective response rates, rate of local recurrence, and overall survival rate did not significantly differ between the two treatment groups. In addition, there was no significant difference in the pre- and post-procedural levels of tumor markers between the two groups. Therefore, we postulate that NBCA itself does not compromise tumor control when used as an embolic agent in extrahepatic tumor-feeding vessels.
The present study has some limitations. First, its retrospective design and the derivation of data from a single center limits its clinical significance; however, this is the largest study of its type to date. Second, when measuring diaphragmatic weakness, chest fluoroscopy was not performed on all patients. However, according to a previous report, the sensitivity of using plain chest radiography to detect unilateral diaphragmatic paralysis is as high as 90% (34). We obtained equivalent results from follow-up chest radiography and fluoroscopy; thus, we assumed that follow-up chest radiography was sufficient to diagnose diaphragmatic weakness. Third, we had limited tools for the diagnosis of diaphragmatic weakness without access to electromyography and a pulmonary function test. Previous reports have raised concerns over the use of chest radiography and fluoroscopy in diagnosing diaphragmatic weakness because of their false-positive and false-negative rates (7,35,36). Fourth, we did not perform internal mammary and intercostal artery angiography; however, these arteries may supply the diaphragm when the IPA is occluded. Thus, diaphragmatic blood supply from the internal mammary artery and intercostal artery can influence the development of diaphragmatic weakness. Fifth, a lack of consistency in terms of evaluating newly developed extrahepatic collaterals at the follow-up treatment session after IPA embolization could be a concern. However, we attempted to perform the procedure as consistently as possible despite the involvement of several operators.
In conclusion, TACE of the right IPA using NBCA resulted in a significantly lower incidence of permanent diaphragmatic weakness than TACE using gelatin sponge particles, which could have an effect on patients with poor cardiopulmonary function. In addition, this technique can prevent the need for repeat embolization of the right IPA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.