
Abstract
Background
There are no consensus and guidelines on the optimal interval of repeat epidural steroid injections (ESI) for patients with lumbar herniated intervertebral disc (HIVD) who respond to initial ESI.
Purpose
To evaluate the effectiveness of ESI in patients with HIVD under a “wait-and-see” policy, i.e. as-needed injections not on a predetermined schedule.
Material and Methods
A total of 592 patients with lumbar HIVD received spine injections between January and December 2017. After excluding patients with excellent (no pain) or poor (>70% residual symptoms) response in the two- or three-week pain assessment, the data of 141 responders were analyzed (60 men, 73 women; age = 50.55±17.25 years). We divided patients into wait-and-see (n=124) and early repeat-ESI (n=17) groups, who received repeat ESIs within three weeks. Evaluations of characteristics and outcomes were performed with the chi-square test or independent Student’s t-test.
Results
Six patients (4.8%) in the wait-and-see group and 1 (5.9%) in the early repeat-ESI group underwent operation within one year (P=0.85). A mean of 1.52±0.82 ESIs was performed in the wait-and-see and a mean of 2.29±0.47 ESIs in the early repeat-ESI group over one year (P<0.001). The time interval between the first and second ESIs was longer in the wait-and-see group than in the early repeat-ESI group (97.15 vs. 15.47 days, P<0.001). Seventy-eight patients (62.9%) in the wait-and-see group could control their pain with a single ESI.
Conclusion
A “wait-and-see” policy could be an effective pain management option for patients with lumbar HIVD who respond to initial ESI.
Keywords
Introduction
Epidural steroid injections (ESIs) may be the most common nonoperative treatment option to control radicular pain considered to be caused by mechanical irritation and inflammation in patients with lumbar herniated intervertebral disc (HIVD) (1–4). In the era of blind injection, technical errors could lead to treatment failure and repeat injections (3,5,6). However, since the introduction of fluoroscopy-guided ESI, most patients achieve good response with a single ESI session and repeat injection is not recommended in non-responders if the initial ESI is accurate and in complete responders. Conversely, in partial responders, repeat ESI can achieve clinical benefit providing better pain relief (2,3,7,8). In this regard, repeat fluoroscopy-guided ESI has been recommended and included in ESI protocols for responders after reassessment of the first injection outcome (9–14).
In clinical practice, there are two pain management options for determining the repeat-injection interval for partial responders: first, the use of prescheduled ESI sessions at predetermined intervals, usually 2–3 weeks after the first injection; and, second, a “wait-and-see” policy that has been employed at our institution since 2011. Repeated ESI was performed only when the first injection fails to maintain a favorable outcome and the patient’s pain aggravated after initial injection without prescheduled ESI. Based on our clinical experience, a wait-and-see policy would have a comparable outcome to that of prescheduled repeat ESIs on pain control and on postponing surgery.
Currently, however, there are no consensus and guidelines on the optimal interval of repeat ESIs for responders. Thus, the decision to repeat ESI is solely based on the clinician’s experience and preference and on patient demand. Therefore, the aim of the present study was to evaluate the effectiveness of ESI in patients with lumbar HIVD under a “wait-and-see” policy based on the one-year clinical outcome.
Material and Methods
Study cohort
The present study was approved by the institutional review board and the requirement for informed consent was waived. The population of the present study was extracted from a spine-injection cohort: 592 patients received spine injections for lumbar HIVD in our department from January 2017 to December 2017. The indications of lumbar spine injection were: (i) patients with low back and radicular pain; (ii) failure of conservative management; and (iii) radiological diagnosis of HIVD as shown on magnetic resonance imaging (MRI) or computed tomography.
We followed up these cohort patients for one year under a “wait-and-see” policy. The next step in the management protocol after the initial injection was the scheduled follow-up after one month or returning to the clinician who referred the patient to our outpatient clinic. We recommended that the patient return to the clinic immediately if symptoms recurred or were aggravated even earlier than the scheduled follow-up date. Additionally, it was recommended to postpone the scheduled follow-up date if the symptoms were tolerable, until symptoms recurred or became aggravated. On subsequent follow-up visits, patients who were unresponsive to the initial steroid injection or had a tolerable degree of pain were not subject to repeat injection. Only patients whose pain had deteriorated or those experiencing severe pain, although the pain was significantly reduced, were considered for a second injection. In exceptional cases, repeat injections were performed if the patient strongly demanded it. Clinicians also treated and referred patients in consensus based on the same policy as ours.
Two to three weeks after the initial injection, a researcher performed telephone interviews under the supervision of a radiologist to evaluate the current injection response using a 5-point patient satisfaction scale (no pain, much improved pain, slightly improved pain, unchanged pain, or aggravated pain), residual symptom percentage, and numeric rating scale (NRS) score. One year after the initial injection, a telephone interview was conducted to check the patient’s operation status and total number of injections during the year. Additionally, a retrospective review of the patients’ electronic medical records was conducted for age, sex, predominant symptom location, onset, NRS score for initial pain, imaging diagnosis, previous operation history, previous steroid injection history within six months, date of first follow-up after initial injection, date of repeat injection sessions, types of lumbar steroid injections, and total number of steroid injections and operations.
Study population
Among the 592 patients, we selected patients with a partial or good response based on the residual-pain assessment on the 2–3-week telephone interview or hospital visit after the initial ESI. Partial response was defined as 50%–70% of residual symptoms, and good response was defined as < 50% of residual symptoms after the initial ESI (15). Patients without pain relief after the initial ESI (n = 7) or patients who had not achieved satisfactory response and had residual symptoms > 70% (n = 107) were excluded. Patients who had complete response without residual pain (n = 5) were also excluded. Other exclusion criteria were: (i) history of steroid injection within six months (n = 219); (ii) facet joint injection (n = 31); (iii) simultaneous use of two different ESI approaches (n = 4); (iv) no pain improvement assessment through telephone interviews or hospital visits within three weeks (n = 77); (v) repeat ESI with presence of new cervical symptoms (n = 1). Finally, 141 patients (60 men, 81 women; mean age = 50.55 ± 17.25 years) with good or partial response after the initial ESI were enrolled.
To assess the sole clinical outcome and effectiveness of the wait-and-see policy, we separated the early repeat-ESI group, consisting of patients who received a second ESI within three weeks. We analyzed in detail the reasons why the wait-and-see policy was not applied in the early repeat-ESI group. The characteristics and clinical outcomes of the two subgroups (early repeat ESI vs. wait-and-see) were compared. Additionally, to evaluate differences according to initial-injection response, we divided each subgroup into two: the good-responder group and the partial-responder groups (Fig. 1).
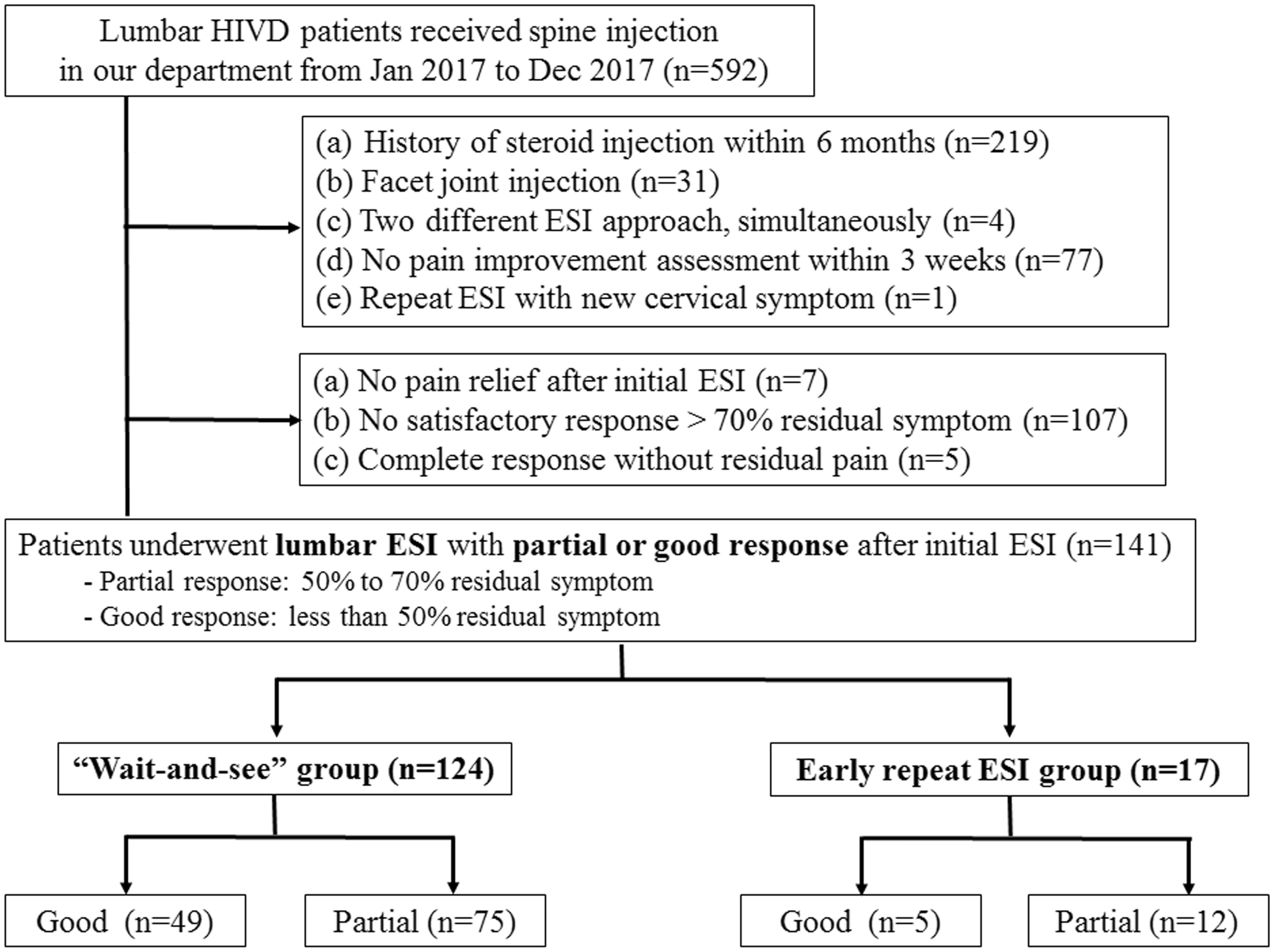
Flow chart schematizing cohort population and study patient selection. ESI, epidural steroid injection; HIVD, herniated intervertebral disc.
Lumbar ESI technique
Lumbar ESIs were performed under fluoroscopy guidance following previously described methods (16). The location of the pain can affect the choice of the type of ESI approach. If the patient complains of unilateral radiculopathy in the lower extremity, an ipsilateral transforaminal approach is preferred. On the other hand, if the patient complains of axial low back pain, an interlaminar approach is preferred. Details of the procedures are provided in Fig. 2 and Appendix E1 (supplemental material).
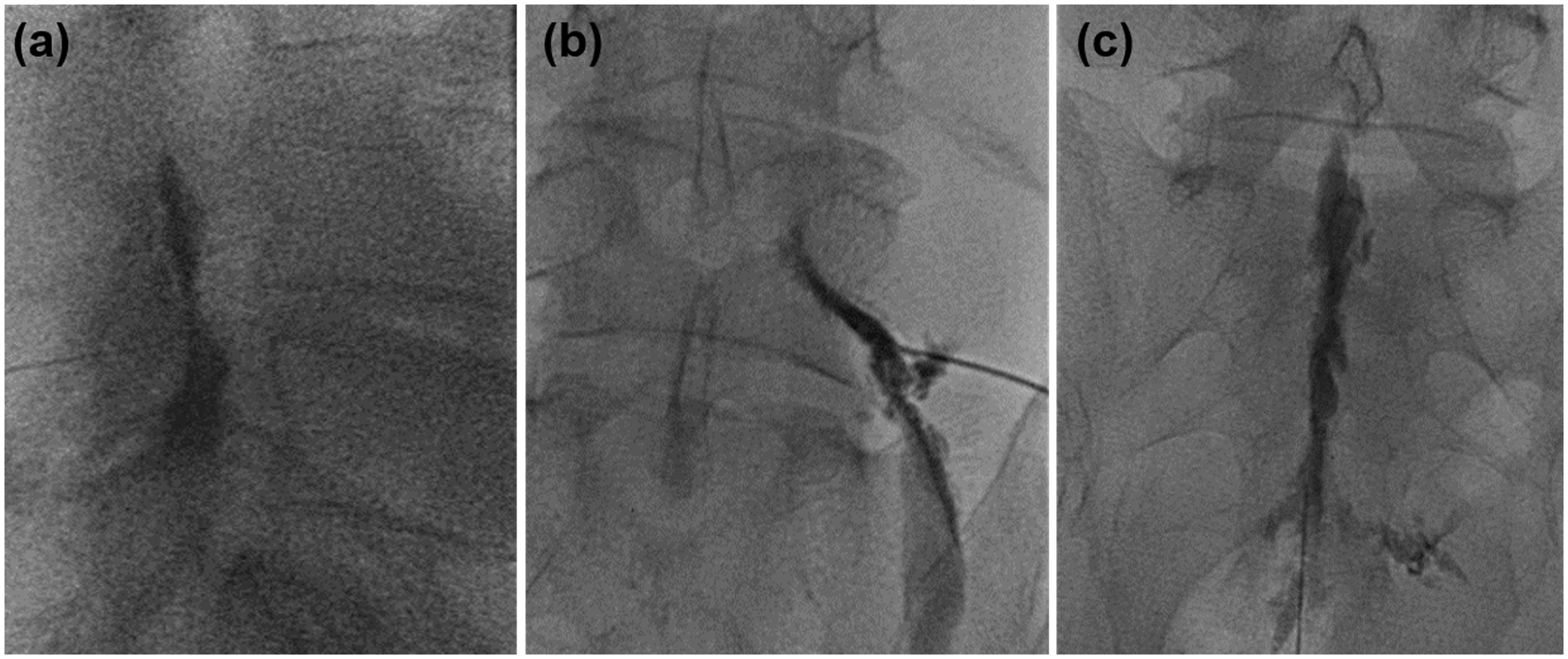
Typical pattern of lumbar epidurography with contrast agent under fluoroscopy guidance: (a) interlaminar approach, (b) transforaminal approach, (c) caudal approach
Statistical analysis
The chi-square test was used to compare categorical variables. The independent Student’s t-test was performed to compare quantitative data. A subgroup analysis of good responders and partial responders within the group was also performed. Additionally, to overcome referral bias in the early repeat-ESI group, we used propensity-score matching based on age, sex, previous operation history, type of ESI, duration of pain (divided in five categories: < 1 month; ≥ 1 to < 3 months; ≥ 3 to < 6 months; ≥ 6 to < 12 months; and ≥ 12 months), initial NRS score, and residual symptom percentage. We established 1:1 matching from the wait-and-see group and compared the outcome between the early repeat-ESI group and the matched wait-and-see group. SPSS version 25.0 (IBM) was used for all statistical analyses. P < 0.05 was considered significant.
Results
Demographics and ESI procedural characteristics of partial responders
Of the 141 patients with lumbar HIVD who partially responded to the initial injection, 124 (87.9%) were in the wait-and-see group (51 men, 73 women; mean age = 50.48 ± 17.64 years) and 17 (12.1%) were in the early repeat-ESI group (9 men, 8 women; mean age = 51.06 ± 15.16 years).
Table 1 shows the patient clinical demographics and ESI procedural characteristics. The mean pain duration of the wait-and-see group was 38.06 ± 89.23 weeks. The initial NRS score before ESI was 7.45 ± 1.75 and residual symptom after initial ESI was 46.77% ± 18.12%. Mean pain duration in the early repeat-ESI group was shorter than that in the wait-and-see group (24.06 ± 42.61 weeks vs. 39.98 ± 93.84 weeks) without a significant difference (P = 0.492). The initial NRS score before ESI was not significantly different (7.65 ± 1.76 for the wait-and-see group and 7.53 ± 1.70 for the early repeat-ESI group; P = 0.370). Although the early repeat-ESI group had a higher percentage of residual symptoms after initial injection than did the wait-and-see group, the difference was not significant (45.85% vs. 53.53%, P = 0.102). Within the wait-and-see group, the good responders showed shorter pain duration than did the partial responders (26.08 ± 59.19 vs. 49.06 ± 110.24 weeks). As for the early repeat-ESI group, pain duration was not different between the good and partial responders (25.50 ± 44.28 vs. 23.38 ± 43.94 weeks). Details of clinical characteristics including reasons for repeated ESI of the early repeat-ESI group are provided in Appendix E2 (supplemental material).
Patient demographics and ESI procedural characteristics of the study population.
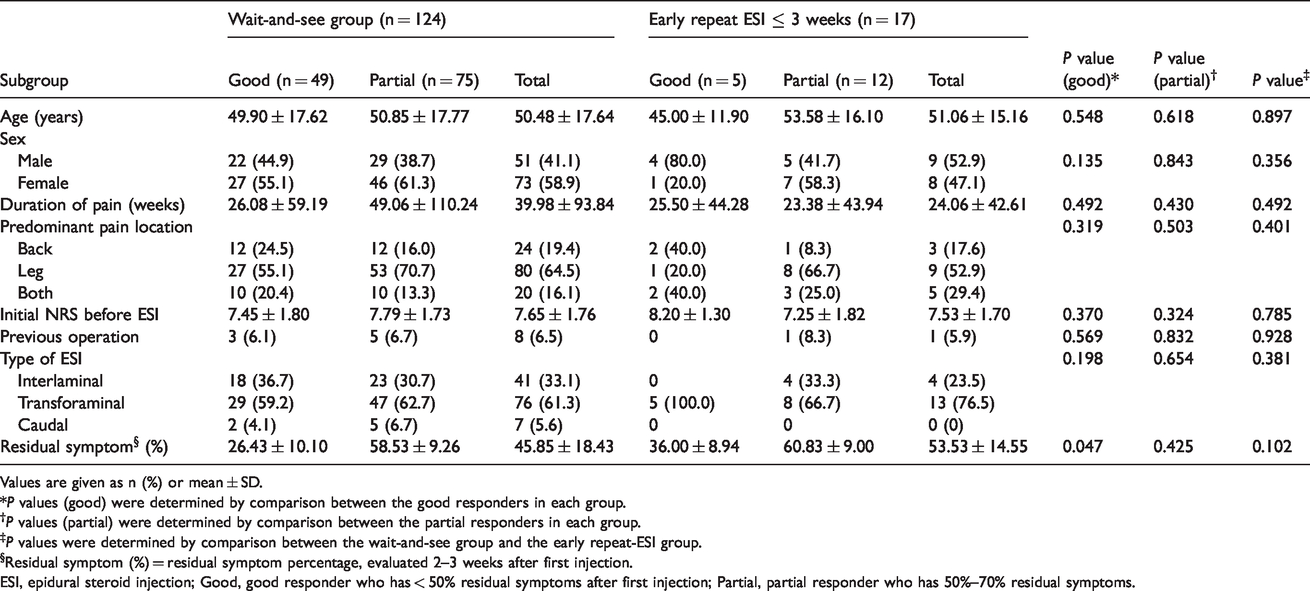
Values are given as n (%) or mean ± SD.
*P values (good) were determined by comparison between the good responders in each group.
†P values (partial) were determined by comparison between the partial responders in each group.
‡P values were determined by comparison between the wait-and-see group and the early repeat-ESI group.
§Residual symptom (%) = residual symptom percentage, evaluated 2–3 weeks after first injection.
ESI, epidural steroid injection; Good, good responder who has < 50% residual symptoms after first injection; Partial, partial responder who has 50%–70% residual symptoms.
Clinical outcome results at the 1-year follow up of the “wait-and-see” group and the early repeat-ESI group
Table 2 summarizes the clinical outcomes of the two groups. A mean of 1.52 ± 0.82 lumbar ESI sessions were performed in the wait-and-see group. The mean number of ESIs was 2.39 in the 46 of 124 patients (37.1%) who underwent repeat ESI in the wait-and-see group. In the early repeat-ESI group, the mean number of ESIs was 2.29.
Clinical outcome results of the patients with lumbar HIVD after initial lumbar ESI.
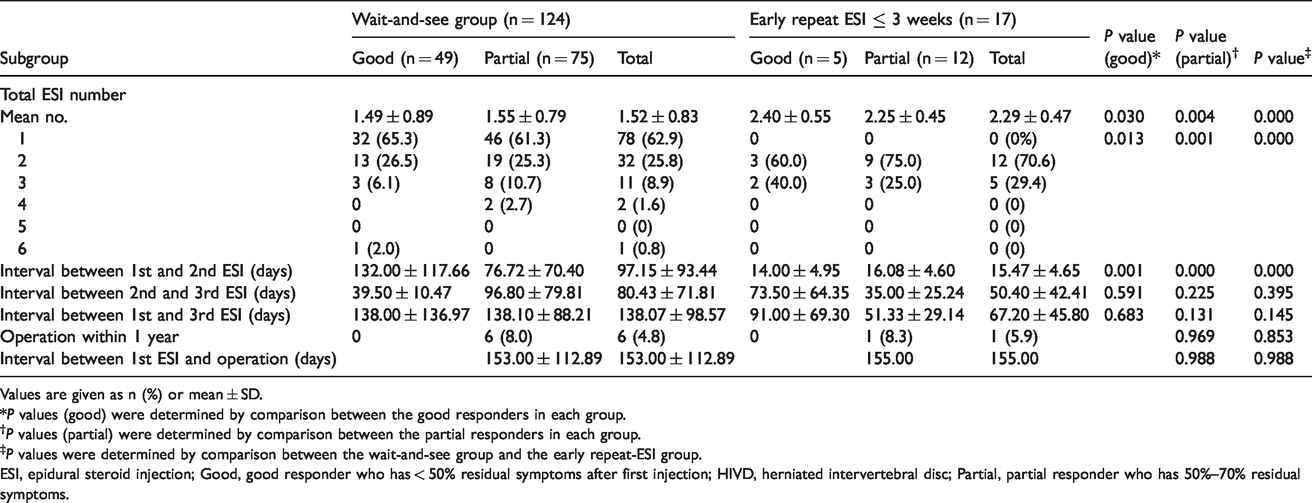
Values are given as n (%) or mean ± SD.
*P values (good) were determined by comparison between the good responders in each group.
†P values (partial) were determined by comparison between the partial responders in each group.
‡P values were determined by comparison between the wait-and-see group and the early repeat-ESI group.
ESI, epidural steroid injection; Good, good responder who has < 50% residual symptoms after first injection; HIVD, herniated intervertebral disc; Partial, partial responder who has 50%–70% residual symptoms.
The time interval between the first and second ESI sessions in the wait-and-see group was 97.15 ± 93.44 days, which was significantly longer than in the early repeat-ESI group (15.47 ± 4.65 days; P < 0.001). Considering the established interval between the first and second ESI in the early repeat-ESI group, it is valid to compare the interval between the first and second ESI in the wait-and-see group with that between the second and third ESI in the early repeat-ESI group. In this regard, the wait-and-see group also showed longer interval (first to second ESI) than did the early repeat ESI group (second to third ESI) both in good (132.00 ± 117.66 vs. 73.50 ± 64.35 days; P = 0.51) and in partial (76.72 ± 70.40 vs. 35.00 ± 25.24 days; P = 0.32) responders, although these differences were not significant.
Taken together, 7 of 141 patients (5%) underwent spinal surgery during the one-year follow-up period. All operations were performed in patients with partial response after the initial ESI. No patient underwent operation after good response to the first ESI. Of 124 patients, 6 (4.8%) were in the wait-and-see group (mean interval to operation = 153.00 ± 112.89 days). Two patients received three ESIs, three received two ESIs, and one received a single ESI preoperatively. Three patients underwent discectomy, one underwent unilateral laminectomy, and the other underwent posterior lumbar interbody fusion. We did not have access to the operational information of the patient who underwent surgery at another hospital. Of the 17 patients in the early repeat-ESI group, 1 (5.9%) underwent surgery at another hospital after two sessions of lumbar ESI (interval to operation = 155 days).
Comparison between the propensity-score matched wait-and-see group and early repeat-ESI group
Patient demographics and ESI procedural characteristics of the propensity-score matched wait-and-see group are summarized in Table 3. Even after propensity-score matching, there was no significant difference in the one-year operation rate for each group (1/17, 5.9% for both), albeit the matched wait-and-see group had a shorter interval between the initial ESI and the operation. Furthermore, fewer ESI sessions were needed for the matched wait-and-see group than for the early repeat-ESI group (1.65 ± 0.79 vs. 2.29 ± 0.47) during the one-year follow-up period (Table 4).
Patient demographics and ESI procedural characteristics of the propensity score matched wait-and-see group and the early repeat-ESI group.
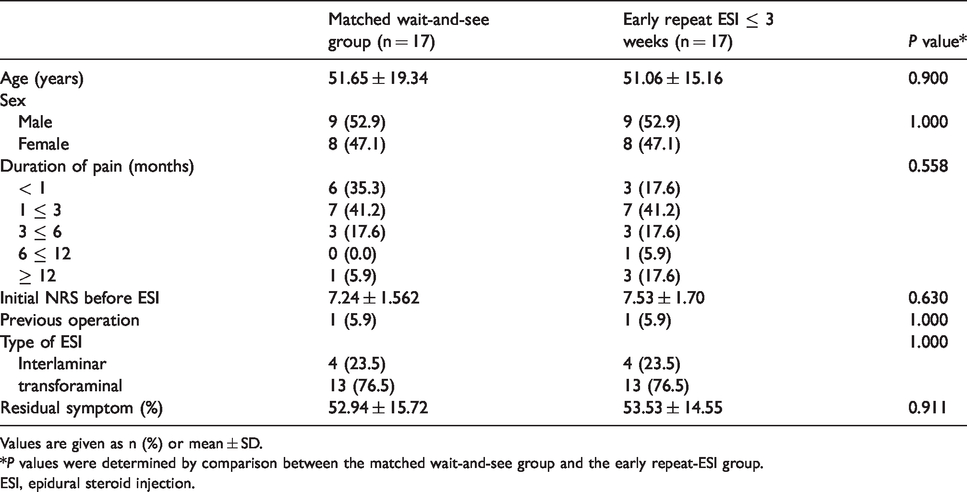
Values are given as n (%) or mean ± SD.
*P values were determined by comparison between the matched wait-and-see group and the early repeat-ESI group.
ESI, epidural steroid injection.
Clinical outcome comparison between the propensity score matched wait-and-see group and the early repeat-ESI group.

Values are given as n (%) or mean ± SD.
*P values were determined by comparison between the matched wait-and-see group and the early repeat-ESI group.
ESI, epidural steroid injection.
Discussion
In our study, 5% (7/141) of patients underwent spinal surgery during the one-year follow up, without a significant difference between the wait-and-see group and the early repeat-ESI group (4.8% vs. 5.9%; P = 0.85). For pain management, a mean of 1.52 ESI sessions were required in the wait-and-see group and a mean of 2.29 sessions were required in the early repeat-ESI group. Approximately two-thirds of patients in the wait-and-see group (78/124, 62.9%) could tolerate their pain with a single ESI during the one-year follow up.
To our knowledge, no recent study has examined the operation rate of ESI responders. However, previous studies (7,17,18) regarding ESI outcome for lumbar HIVD have reported operation rates in the range of 14.6%–18.9% during six-month or one-year follow-up periods. The results of the present study showed quite good clinical ESI outcomes for lumbar HIVD with a 5% operation rate, although it should be noted that our study only included good or partial responders, excluding non-responders and complete responders. Here, all spinal operations were performed to partial responders with an 8% operation rate for the wait-and-see group and an 8.3% operation rate for the early repeat-ESI group. No patient underwent surgery after good response to the first ESI; hence, we consider that early repeat ESI is unnecessary, especially in good responders after the initial ESI.
A mean of 1.4 ± 1.7 ESIs per patient during one-year follow-up periods were reported by previous studies (9,19) that employed similar “wait-and-see” protocols. According to our results, fewer ESIs are required for pain control under the “wait-and-see” policy than under the fixed regimen. Conversely, Lee et al. (10) reported more ESIs (2.67 ± 0.78) for a lumbar HIVD group who only received repeat injection for aggravated pain compared to the ESIs in our wait-and-see group (1.52 ± 0.82). Additionally, Lee at al. (10) suggested that a fixed regimen with prescribed interval repeat injection did not increase the number of total ESIs, without differences between a group that received repeat injection only for pain aggravation and a group that received repeat injection on a fixed regimen (2.67 ± 0.78 vs. 2.58 ± 0.68; P = 0.69). This discrepancy with our results can be attributed to differences in patient selection. Unlike our study, patients who partially responded to initial ESI and could control pain with only one injection over one year were not included in their study population, and all patients underwent repeat injection at least twice.
The underlying mechanism of steroid activity and the cumulative effect of steroids remain unclear. Understanding of the pathophysiology of lower-extremity radiating pain is also lacking (6,9). However, one possible explanation for the comparable and effective clinical outcome of the “wait-and-see” policy is that herniated disc has spontaneous regression potential (19–23). The spontaneous resorption rate of herniated disc reached 66.7% (20) and complete resorption could be achieved in 41% of migrated disc herniation cases (24). Autio et al. (19) reported that spontaneous resorption of herniated disc occurred within two months. Therefore, a favorable outcome can be expected before surgical intervention and even before the initial ESI. Thus, if patients with lumbar HIVD respond to initial ESI and have tolerable or medication-controllable residual pain, close observation of symptoms and patient needs without predetermined repeat ESI may be sufficient to reduce pain.
By applying a “wait-and-see” policy, we could reduce costs by simply reducing the number of injections as well as reduce ESI-related complications and systemic reactions to steroids. Boswell et al. (25) suggested limiting ESIs to up to 4–6 times/year in the evidence-based guideline for chronic spinal pain. Furthermore, previous studies (26–28) reported a one-year risk of recurrence of 23%–25% of lower-extremity radiating pain and a one-year risk of recurrence of 28%–43% of lower-back pain. Thus, applying a “wait-and-see” policy can provide the opportunity to use steroids appropriately, with relatively fewer restrictions on the number of injections if symptoms recur, by reducing the injection number and avoiding unnecessary injections.
The present study had some limitations. First, the study population was small and included heterogeneous ESI approaches under the retrospective study design. However, we selected patients with lumbar HIVD and excluded patients treated with facet joint injection and two different ESI approaches simultaneously to minimize selection bias caused by retrospective study design. Therefore, further prospective studies, designed with a homogeneous patient group and ESI approaches, are needed to be performed. Second, although we followed up the patients’ symptoms and operation status through telephone interviews, not all patients were followed up for one year through outpatient visits. Third, as our institution is academic, some patients had undergone surgery at other hospitals, regardless of repeat ESI or ESI outcome. However, we included the clinical characteristics and numbers of these patients in the results for use in clinical practice. Finally, we applied a “wait-and-see” policy to all patients. Nevertheless, several patients with early repeat ESI were included in our study cohort because of clinician or patient needs. Thus, we divided these groups from the patients who received ESI under the “wait and see” policy.
In conclusion, a “wait-and-see” policy could be an effective option for pain management for patients with lumbar HIVD who respond to initial ESI without predetermined interval ESI.
Supplemental Material
sj-pdf-1-acr-10.1177_0284185120985500 - Supplemental material for Effectiveness of epidural steroid injection in patients with lumbar herniated intervertebral disc under a “wait-and-see” policy
Supplemental material, sj-pdf-1-acr-10.1177_0284185120985500 for Effectiveness of epidural steroid injection in patients with lumbar herniated intervertebral disc under a “wait-and-see” policy by Bo Ram Kim, Joon Woo Lee, Eugene Lee, Yusuhn Kang, Joong Mo Ahn and Heung Sik Kang in Acta Radiologica
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.