
Abstract
Rhinocerebral mucormycosis (RCM) may result in severe intracranial ischemic and hemorrhagic lesions. Both computed tomography (CT) and magnetic resonance imaging (MRI) play an essential role in the diagnosis of RCM, but whereas CT is better for assessing bone erosion, MRI is superior in evaluating soft tissue, intraorbital extension, and in assessing intracranial and vascular invasion. Specific CT and MRI techniques, such as CT angiography or enhanced MR angiography, and more advanced MRI sequences such as gadolinium-3D Black Blood imaging, contribute to the assessment of the extension of vascular invasion.
In this pictorial review, we describe specific CT and MRI signs of RCM, mainly focusing on its life-threatening complications due to vascular involvement.
Keywords
Introduction
Rhinocerebral mucormycosis (RCM) is an acute, fulminant, and often lethal, opportunistic infection typically affecting uncontrolled diabetic and immunocompromised patients (1–3). The last group consists of patients with acquired immunodeficiency syndrome, liver cirrhosis, severe burn wounds, and hematologic malignancy; namely patients undergoing systemic chemotherapy, systemic steroid therapy, bone marrow transplantation, or immunosuppressive therapy for organ transplantation (4–8).
RCM is caused by fungi of the Mucorales order, such as Absidia, Mucor, and Rhizopus. The clinical symptoms are non-specific, such as headache, low-grade fever, facial swelling, and orbital or paranasal sinusitis (2).
The disease is generally characterized by three stages (9,10). In the first one, inhaled spores infect the paranasal sinuses and necrotic lesions develop in the nasal mucosa and hard palate (9).
In the second stage, infection spreads into the orbital space by directly eroding maxillary, orbit, and ethmoid bone structures, or following the path of orbit’s vessels, such as the orbit vein and ethmoidal arteries (11).
In the third stage, Mucor fungus invades the intracranial space either: (i) directly eroding bone structures such as the cribriform palate, frontal and sphenoid sinus bone wall or orbital apex; or (ii) through the pathways of cranial nerves; or (iii) following the blood circulation of the ophthalmic vessels, internal carotid artery (ICA), and basilar artery, causing necrosis of the vessels’ wall, which predisposes to intraluminal thrombus formation and brain infarcts (10–12).
If the infection is limited to the paranasal sinuses, the survival rate is in the range of 50%–80%; however, when brain invasion occurs, mortality is >80% (13). Survival rates are reported to be approximately 70% when amphotericin B and a rapid, aggressive surgical approach are combined. Given the delay in diagnosis and treatment, most cases of mucormycosis have a poor prognosis (14).
The main reason for Mucor fungus lethality is its high affinity for blood vessels, and in particular for the elastic membrane of arteries (15). The spores invade the vascular structures and are multiplied in the elastic lamina of the arteries. Hifae erodes the endothelium of the vessel walls and then causes necrosis, thrombi, and infarcts (11). The angioinvasive nature of the fungus may result in extensive thrombosis of the main cerebral vessels, like the ICA and basilar artery, with consequent extensive cerebral infarctions. Moreover, cerebral vascular invasion may lead to other severe complications, such as cerebral hemorrhage and subarachnoid hemorrhage (16).
Since the early diagnosis and treatment improve the outcome of RCM (17), neuroimaging plays a main role in patients with acute invasive sinusitis. Thus, the aim of the present study was to make the radiologists familiar with the life-threatening cerebrovascular complications of RCM, suggesting specific protocols and highlighting the peculiar diagnostic key findings of this uncommon disease at each stage.
Imaging techniques
Both computed tomography (CT) and magnetic resonance imaging (MRI) play an essential role in the diagnostic process of RCM.
Paranasal sinuses invasion is detected by standard CT protocols. Unenhanced CT is useful to depict hyperdense foci of fungal elements in paranasal sinuses. To optimally assess bony erosion and orbital invasion, both bone and soft tissue algorithms are needed (8). MRI of the paranasal sinuses is superior to CT in evaluating the infraorbital extension of the disease; in particular, fat-saturated T2-weighted (T2W) and T1-weighted (T1W) contrast-enhanced sequences are useful to assess the orbital involvement and eventually dry gangrene (18).
For the evaluation of brain invasion, unenhanced CT is useful to depict hemorrhagic complications, and CT angiography provides additional information if arterial occlusions and/or mycotic aneurysms are suspected (19,20).
Standard brain MRI protocols with turbo spin echo (TSE) T1W and T2W imaging, fluid attenuation inversion recovery (FLAIR), diffusion-weighted imaging (DWI), and contrast medium administration are necessary to study intracranial complications such as acute cerebral ischemia, cerebral infarcts, and intracranial abscesses (9,13,21).
MR angiography is useful in invasive cases to diagnose the intra-cranial vascular invasion whereas enhanced MR angiography may contribute to the assessment of the extracranial angioinvasion (20).
Beyond standard MRI brain protocols, advanced MRI sequences such as susceptibility-weighted imaging (SWI) and gadolinium-3D Black Blood (Gd-3DBB) imaging should be considered to detect intraluminal and vessels’ walls invasion.
SWI is a fully velocity-compensated high-resolution 3D gradient-echo sequence which is highly sensitive to compounds that distort the local magnetic field such as deoxygenated blood, hemosiderin, ferritin, and calcium (22). SWI has been widely incorporated into the routine diagnostic imaging evaluation in the last decade and offers the possibility of directly visualizing thrombotic material independently of the presence of blood flow or contrast media (23), as intravascular hypointensity.
To avoid spatial resolution limitations in detecting fungal arteritis at the very beginning, Gd-3DBB imaging could be a useful tool that allows the direct view of the vessel wall by suppressing the blood signal. At 3-T MRI with isotropic voxel dimensions in the range of 0.4–0.7 mm for 3D acquisitions, it is possible to scan the circle of Willis arteries and main branches in 7–10 min. Rapid thickening and enhancement of the carotid artery wall on serial MRI establish the nature of the arterial involvement by mucormycosis rather than atherosclerosis, and it is better recognizable in Gd-3DBB sequence (24).
Imaging findings Stage 1 and 2: sinusitis and orbital infection Paranasal sinuses infection
Most common findings on standard imaging protocols
The most common finding in RCM is unilateral involvement of the ethmoid and sphenoid sinuses (8). RCM is detected by unenhanced CT as homogeneous opacification of the sinus cavity, with well defined, markedly hyperdense foci within the inflammatory reaction, probably due to calcium phosphate and calcium sulfate deposits in necrotic areas of the mycetoma (25).
Bone algorithm unenhanced CT reconstruction may demonstrate bony erosion; however, erosion of bone walls could be very subtle (Fig. 1), because progression of the disease beyond the sinuses may occur with intact bony wall through the vascular and perineural spread (8).
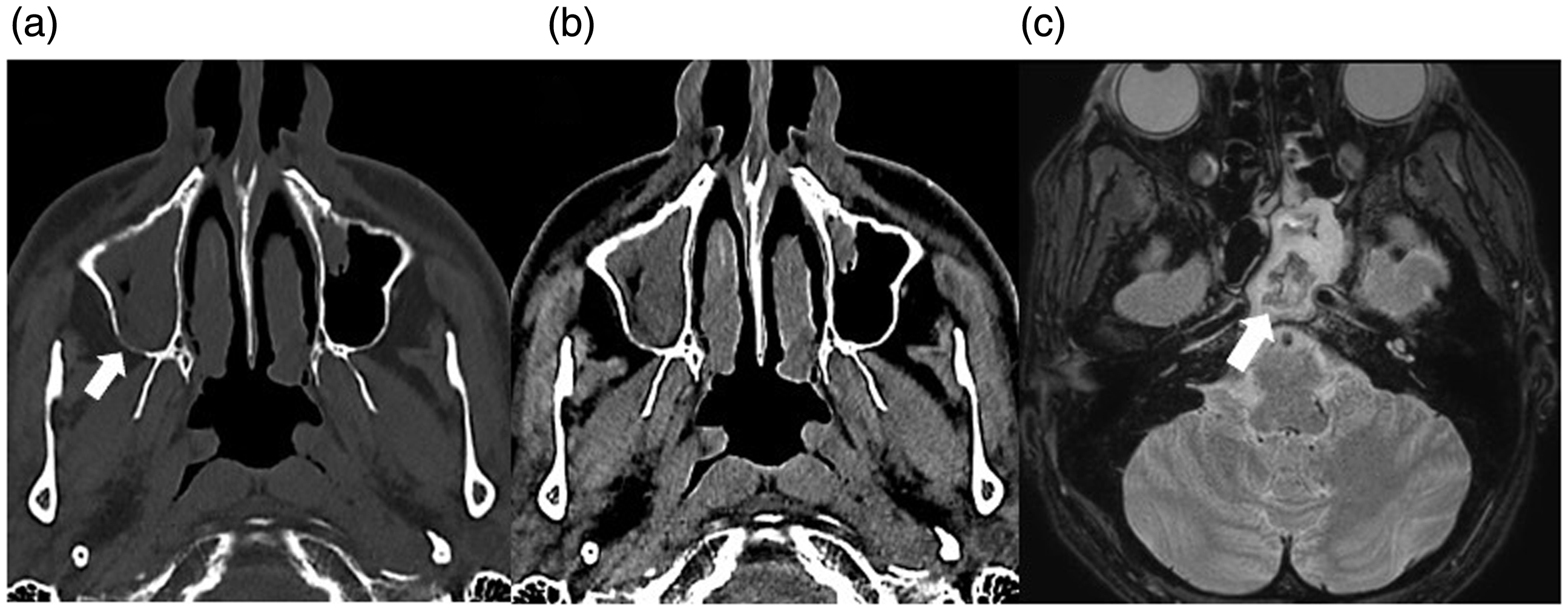
(a, b) Unenhanced CT of a 64-year-old male patient affected by acute myeloid leukemia and RCM (same patient as in Figs. 2, 3, and 8). (a) Bone window demonstrates subtle bony erosion of the posterior wall of the right maxillary sinus (arrow) and (b) soft-tissue window shows right maxillary sinusitis. (c) TSE T2W fat-saturated axial MRI of a 46-year-old female patient (same patient as in Figs. 4 and 6) with acute myeloid leukemia and RCM showing ferromagnetic hypointense fungal materials in the sphenoid sinus (arrow). CT, computed tomography; MRI, magnetic resonance imaging; RCM, rhinocerebral mucormycosis; T2W, T2-weighted; TSE, turbo spin echo.
Another early sign is soft-tissue infiltration of the deep face characterized by obliteration of the normal fat planes in the infratemporal fossa, pterygopalatine fossa, and pterygomaxillary fissure (26).
Peculiar findings valuable to differential diagnosis
With MRI, the affected sinuses appear hypointense on T2W and iso- to hypointense on T1W images because of calcium deposits, air, and ferromagnetic elements (e.g. manganese, iron, and magnesium) (18) (Fig. 1). The affected tissue is prone to necrosis and devitalization, which subsequently leads to a lack of enhancement on postcontrast MRI, also known as the “black turbinate sign,” a peculiar feature usually aiding an earlier diagnosis (18,27) (Fig. 2). It has to also be highlighted that the affected non-enhancing tissue may also show restricted diffusion on DWI. Instead, non-infarcted sinusitis shows T1 postcontrast enhancement of the mucosa (18).
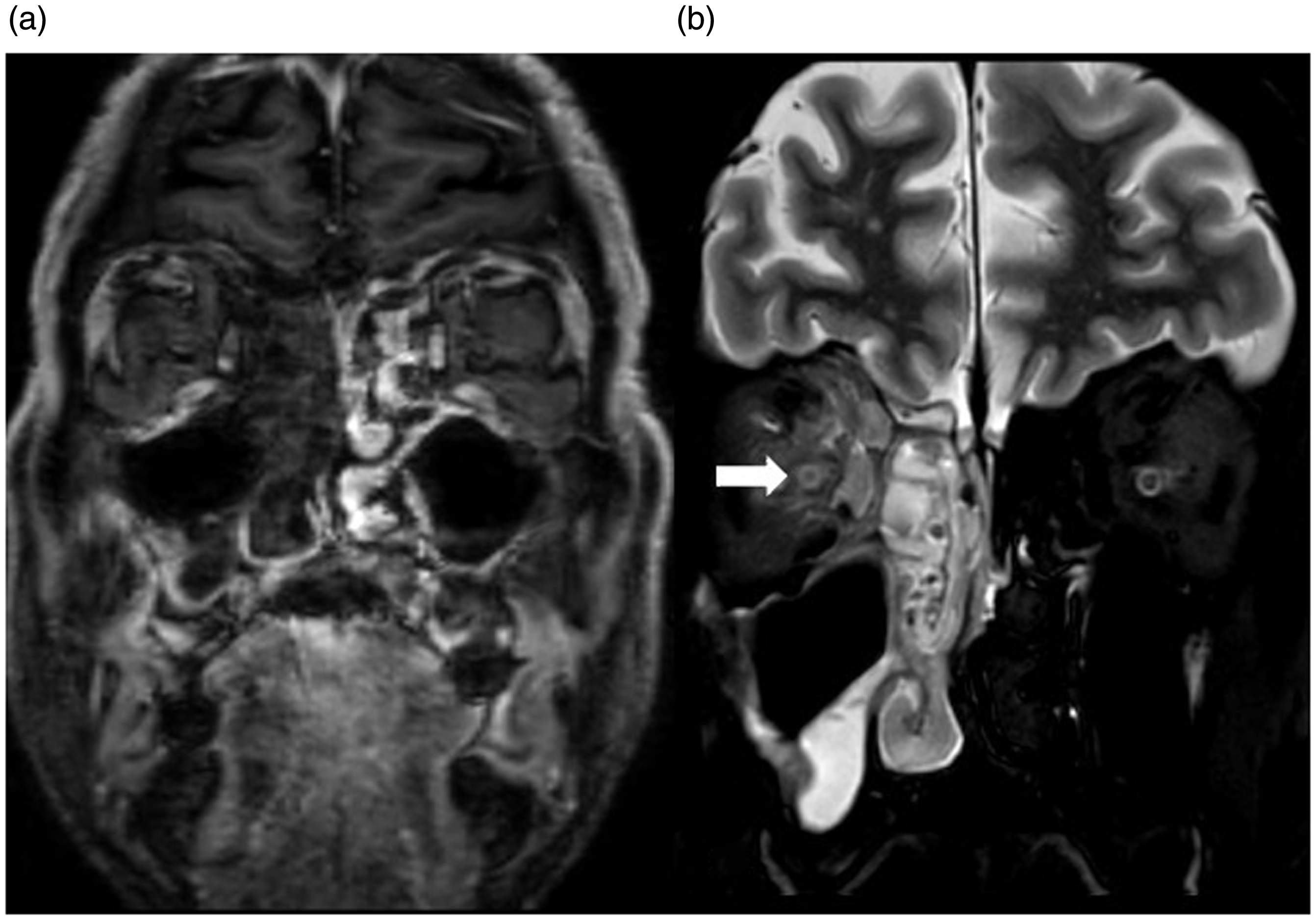
MRI of a 64-year-old male patient with acute myeloid leukemia and RCM (same patient as in Figs. 1a, 1b, 3, and 8). (a) Enhanced 3D-T1W MRI with coronal reconstruction showing the black turbinate sign: lack of enhancement (arrows) of the right turbinates due to devitalized mucosa gangrene. (b) TSE T2W fat-saturated coronal shows orbital invasion: hyperintensity of the right retro-orbital fat with lateral displacement and thickening of the medial rectus and superior oblique muscles. Optic nerve (arrow) is also involved. MRI, magnetic resonance imaging; RCM, rhinocerebral mucormycosis; T1W, T1-weighted; TSE, turbo spin echo.
Orbital infection
Most common findings on standard imaging protocols
MRI is superior to unenhanced CT to define the extension and severity of orbital infection (9). Orbital invasion is characterized by proptosis and T2W hyperintensity of the orbital fat and extraocular muscles. Another typical finding is lateral displacement and thickening of medial rectus muscle and retro-orbital fat hyperintensity on fat-saturated T2W images (9) (Fig. 2).
Complications such as optic nerve ischemia (i.e. T2 hyperintensity of the optic nerve at MRI) (9) may occur. Other complications such as cellulitis, subperiosteal abscess, or orbital abscess can be assessed by standard MRI protocols with T1W, fat-saturated T2W, DWI, and postcontrast imaging (25).
Stage 3: intracranial and vascular invasion
RCM usually has a sudden clinical course; therefore it is important for the radiologist to be aware of the risk of intracranial and vascular invasion of this disease and seek for early radiological signs also in patients who do not manifests neurological impairment yet.
Intracranial invasion
Most common findings on standard imaging protocols
The most common finding of intracranial invasion of RCM on standard brain MRI is leptomeningeal enhancement, which could be subtle and must be diligently sought (25).
The perineural spread through the cribriform plate into the anterior cranial fossa can also cause epidural and subdural empyemas, respectively, with a biconvex and crescentic shape with surrounding membrane that enhances uniformly following contrast administration (8).
Peculiar findings valuable to differential diagnosis
The anterior cranial fossa is a typical localization of RCM intracranial complications. Invasion of the anterior cranial fossa by bony erosion or perineural spread through the cribriform plate can cause adjacent cerebritis, which represents brain inflammation caused by non-viral infection, before the development of a cerebral abscess (8). Early cerebritis manifests as poorly marginated cortical or subcortical T2-FLAIR hyperintensity with surrounding vasogenic edema, with no or minimal heterogeneous enhancement and patchy restricted diffusion; late cerebritis shows progressive peripheral enhancement and progressively restricted diffusion (28). Late cerebritis may develop and organize to form a cerebral abscess, where a capsule of granulation tissue lines a cavity containing purulent material, with true restricted diffusion and a thick ring-enhancement capsule (28,29), or granulomas, which appear hypointense on T1W and T2W images with minimal enhancement after administration of contrast medium (8).
Vascular invasion
Vascular invasion may cause several complications such as arterial thrombosis, cavernous sinus thrombosis, mycotic aneurysm, and intracerebral hemorrhage (8,10,17).
We searched the literature for case reports of patients with RCM and vascular complications.
Thirty articles with 42 cases were selected; all were published in English within the period 1975–2019. Age and gender, type of vascular complications, infection involvement, outcome, and immunological and diabetes status were collected (Table 1).
Clinical findings, imaging features, risk factors, and outcomes in patients with RCM and vascular complications.
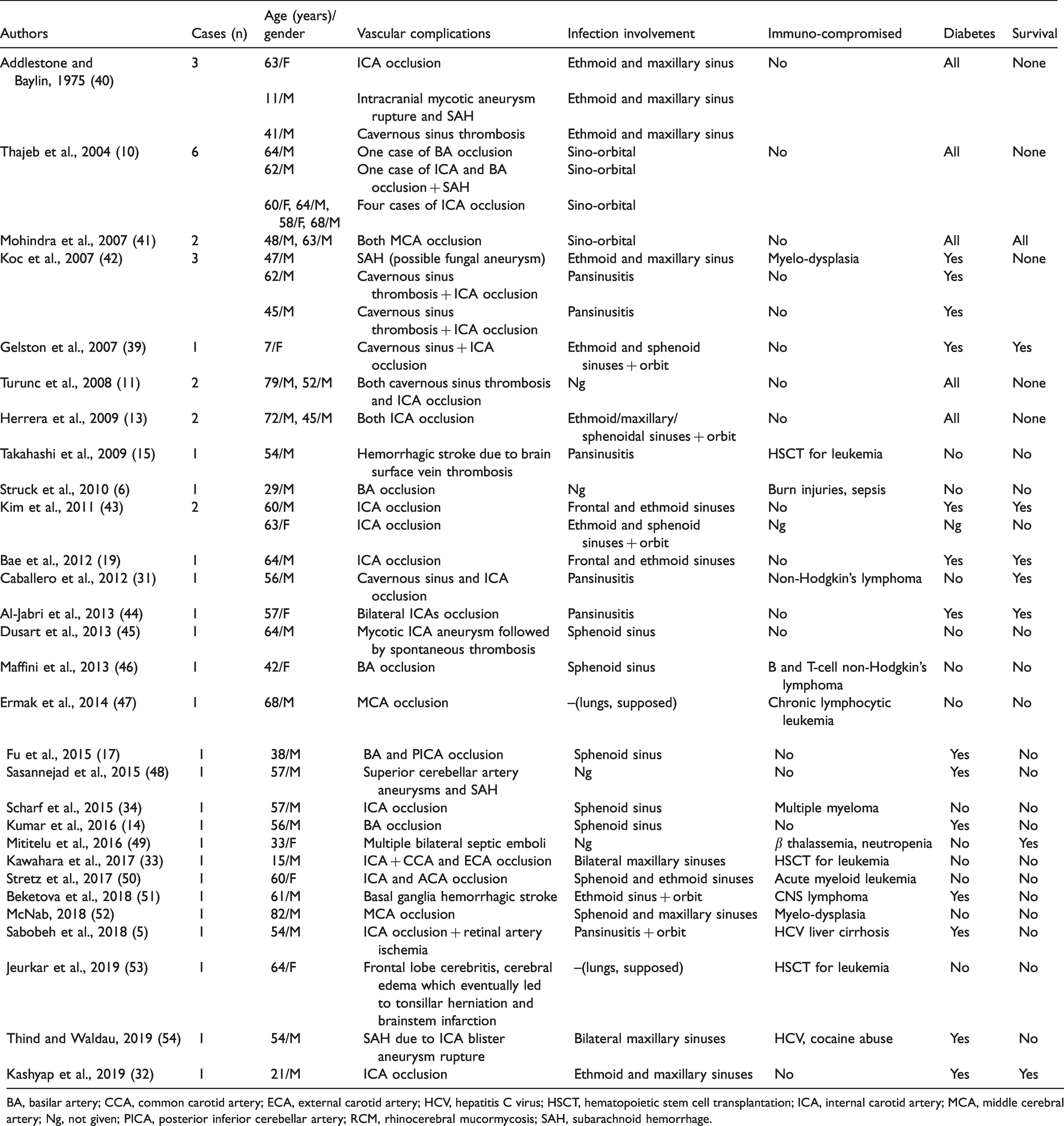
BA, basilar artery; CCA, common carotid artery; ECA, external carotid artery; HCV, hepatitis C virus; HSCT, hematopoietic stem cell transplantation; ICA, internal carotid artery; MCA, middle cerebral artery; Ng, not given; PICA, posterior inferior cerebellar artery; RCM, rhinocerebral mucormycosis; SAH, subarachnoid hemorrhage.
Of the 42 described cases, 32 (76%) were male. Twenty-six participants were diabetic patients, 11 were immunocompromised, and four patients had both diabetes and immunodeficiency (62%, 26%, and 10%, respectively); for one participants, diabetic and immunological status was not given. Vascular complications were described as follows: 35 cases of arterial and/or cavernous sinus thrombosis with subsequent cerebral ischemia; six cases of subarachnoid hemorrhage; five arterial aneurysms; and one case of multiple cerebral septic emboli. Only nine individuals survived, and there were 33 deaths (79%). Of the 33 cases who died, the majority (n = 31, 93%) was diabetic, immunocompromised, or both (18, 9, and 4 cases, respectively), and one case was neither diabetic nor immunocompromised; for one individual, this information was not available.
The prognosis is often very poor once the ICA is involved; however, despite all the participants who survived with ICA occlusion, the patients did not die, probably due to good collateral circulation from the contralateral ICA, although surgery and postoperative medication management are also important (19). A few successful cases have been reported after extensive sinus debridement and intravenous amphotericin B therapy (30–32).
Arterial thrombosis
Most common findings on standard imaging protocols
Arterial thrombosis is the main cause of cerebral infarction and a prompt diagnosis is crucial for a good prognosis, with neuroimaging assuming a substantial role in the diagnostic process (20).
Even if unenhanced brain CT is the mainstay of imaging in the emergency setting, DWI has been demonstrated to provide significantly higher sensitivity and specificity in the diagnosis of acute ischemic infarction in the first few hours after onset (21) (Fig. 3). Clinicians should be aware of invasive sinusitis as an uncommon cause of stroke in immunocompromised and diabetic patients, and an MRI examination, including DWI, should be required when acute invasive fungal sinusitis with a probable intracranial extension is suspected (33).

DWI and ADC map of a 64-year-old male patient with acute myeloid leukemia and RCM (same patient as in Figs. 1a, 1b, 2, and 8): cerebral infarction of left rectus gyrus, due to septic emboli or contiguous spread of Mucor fungus through the cribriform plate. ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; RCM, rhinocerebral mucormycosis.
T2W or FLAIR, as well as T1W contrast-enhanced sequence, well demonstrate slow vascular flow (20). The early detection of thromboembolism is essential to establish a prompt treatment with endovascular retrieval of mycotic thrombus and stenting of the involved vessel (34).
Even if digital subtraction angiography (DSA) is the gold standard for investigating the vascular system, arterial occlusion by fungal thrombosis can be easily detected by CT angiography or MR angiography, which does not require the injection of contrast medium and does not expose the patient to ionizing radiations.
Peculiar findings valuable to differential diagnosis
Different cerebral arteries have been described to be affected by fungal thrombi.
Ophthalmic vessels: The ophthalmic vessels are frequently involved and contrast-enhanced MRI usually shows a lack of enhancement of the superior ophthalmic vein and ophthalmic artery, because of vasculitis and thrombosis.
Internal carotid artery: ICA thrombosis is the consequence of the extension of the inflammation from the frontal, ethmoidal, and maxillary sinuses through the frontal bone, ethmoid sinus wall, and cribriform plate into the cavernous sinuses and anterior intracranial fossa (10,27). Loss of signal void in the petrous and cavernous portion of the ICA and high signal intensity on both T1W and T2W are diagnostic findings. Contrast-enhanced MR angiography, CT angiography, or DSA should be performed to explore the extracranial tract of the ICA (Fig. 4) (19,33).

A 61-year-old male diabetic patient with RCM and right ICA thrombosis. (a) Enhanced SE T1W axial MRI: right vascular space, retropharyngeal space, and prevertebral space enhancement with right ICA occlusion (arrow). (b) CT angiography (3D reconstruction), (c) MR angiography (3D reconstruction), and (d) digital subtraction angiography: three different techniques showing the right ICA thrombosis (arrows). CT, computed tomography; ICA, internal carotid artery; MRI, magnetic resonance imaging; RCM, rhinocerebral mucormycosis; SE, spin echo; T1W, T1-weighted.
Basilar artery: Mucor fungus can cause basilar artery thrombosis by the invasion of the sphenoid sinus with the destruction of the posterior wall and clivus (Fig. 5) (17). Brain MRI may show enhancing soft tissue extending into the prepontine cistern, encasing, and causing thrombosis of the basilar artery, which could result in acute pontine infarction. Occlusion of the posterior cerebral arteries leads to an acute infarction of the midbrain, thalami, medial part of the temporal lobe, occipital pole, and visual cortex (Fig. 6) (14). The extension into the basal cisterns may also cause involvement of the II, III, IV, and VI cranial nerves resulting in proptosis, ptosis, pupillary dilatation, and visual loss as well as periorbital cellulitis (35).

Basilar artery thrombosis in a 46-year-old female patient (same patient as in Figs. 1c and 7) with acute myeloid leukemia and RCM: (a, b) Axial plane DWI with pontine and right cerebellar infarction in vascular territories of basilar artery and right posterior inferior cerebellar artery. (c, d) Digital subtraction angiography showing basilar artery stricture (arrows). DWI, diffusion-weighted imaging; RCM, rhinocerebral mucormycosis.
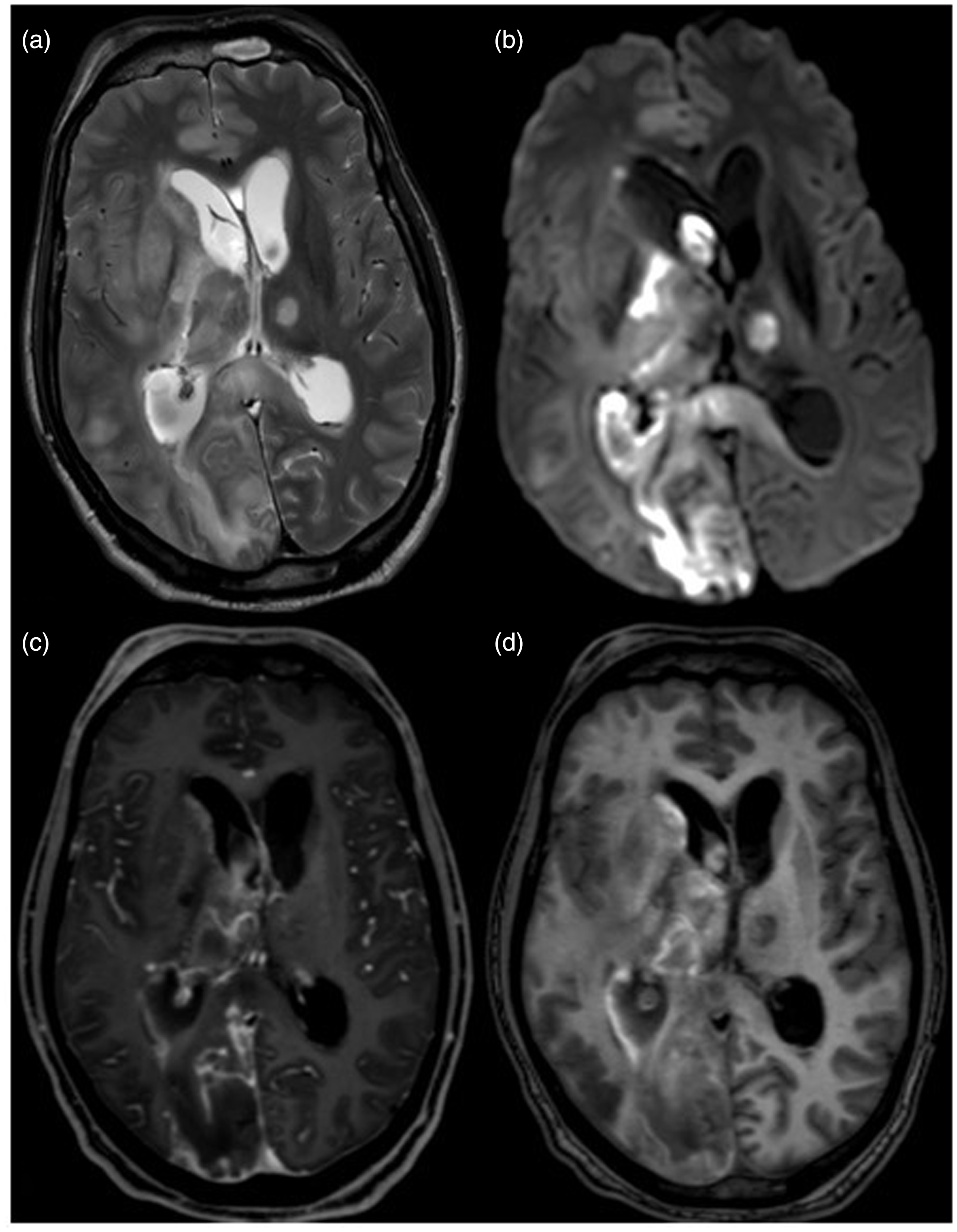
A 63-year-old male diabetic patient with RCM and bilateral posterior cerebral artery thrombosis. (a) TSE T2W, (b) DWI, and (c) 3D-T1 post-gadolinium showing extensive cerebral ischemia in right occipital-temporal lobe and visual cortex with thalamic involvement and extension to corpus callosum and left thalamus as T2W hyperintensities, restricted diffusion (ADC not shown) and faint enhancement of cortical gyri. (d) TE T1 shows hemorrhagic components recognizable as spontaneous T1W hyperintensities. ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; RCM, rhinocerebral mucormycosis; T1W, T1-weighted; T2W, T2-weighted.
Imaging findings on advanced sequences
Thromboembolism may be detected on SWI as intravascular hypointensity.
Recognizing arterials wall invasion due to RCM could be very challenging, especially in the initial stages (36,37). In our experience, a suspected case of basilar artery thrombosis showed enhancement of the basilar artery’s walls and endoluminal thrombus with Gd-3DBB and was finally diagnosed as Mucor infection (Fig. 7). Fig. 7 is an example of mucormycosis arteritis and mucosal necrosis of the sphenoid sinus depicted by Gd-3DBB.
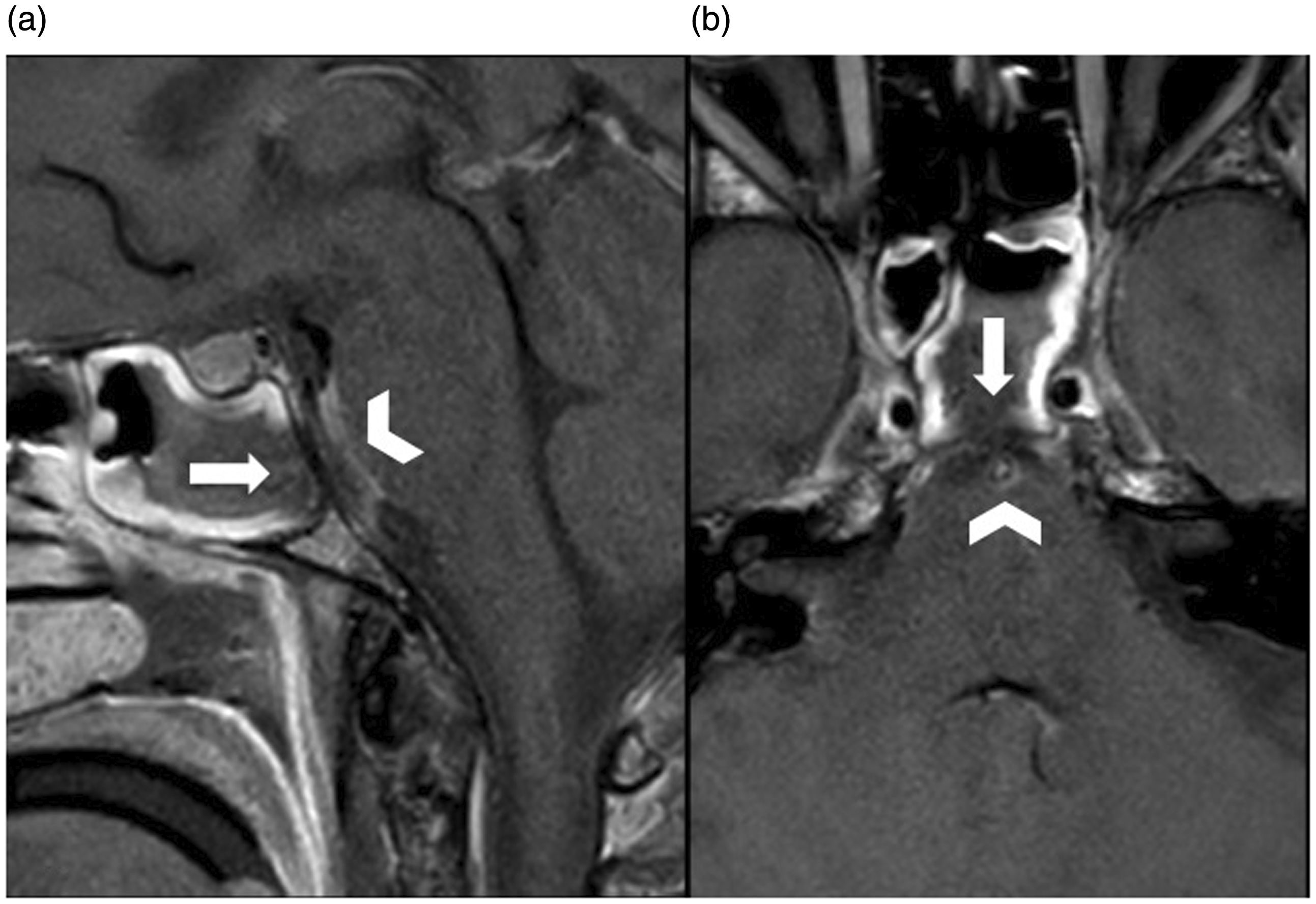
Gd-3DBB (a) sagittal and (b) axial MRI of a 46-year-old female patient with acute myeloid leukemia and RCM (same patient as in Figs. 1c and 5): the basilar artery’s walls show contrast enhancement and endoluminal thrombus (arrowheads) best seen in the axial plane. Note the lack of enhancement of the posterior wall of the left side of the sphenoidal sinus (arrows) due to necrotic mucosa and dry gangrene, which involves the clivus and causes basilar artery’s arteritis. Gd-3DBB, gadolinium-3D Black Blood; MRI, magnetic resonance imaging; RCM, rhinocerebral mucormycosis.
Cavernous sinus thrombosis
Most common findings on standard imaging protocols
T1W and T2W sequences show absent flow voids, but signal characteristics vary depending on the age of the thrombus, and contrast-enhancement or lack of is not a reliable indicator as organizing thrombus can enhance (38).
Image findings on advanced sequences
Currently, MRI is the modality of choice to confirm the diagnosis of cavernous sinus thrombosis. MRI with MR venogram shows the absence of venous flow in the affected cavernous sinus, and carotid CT angiography or MR angiography can demonstrate narrowing or obstruction of the inter-cavernous segment of the ICA (38,39).
Cerebral hemorrhage and mycotic aneurysms
Hemorrhagic transformation of a brain ischemic infarct (Fig. 8), rupture of mycotic aneurysms, and hemorrhagic venous ischemia are three main causes of intracranial hemorrhagic complications in RCM (15,27).
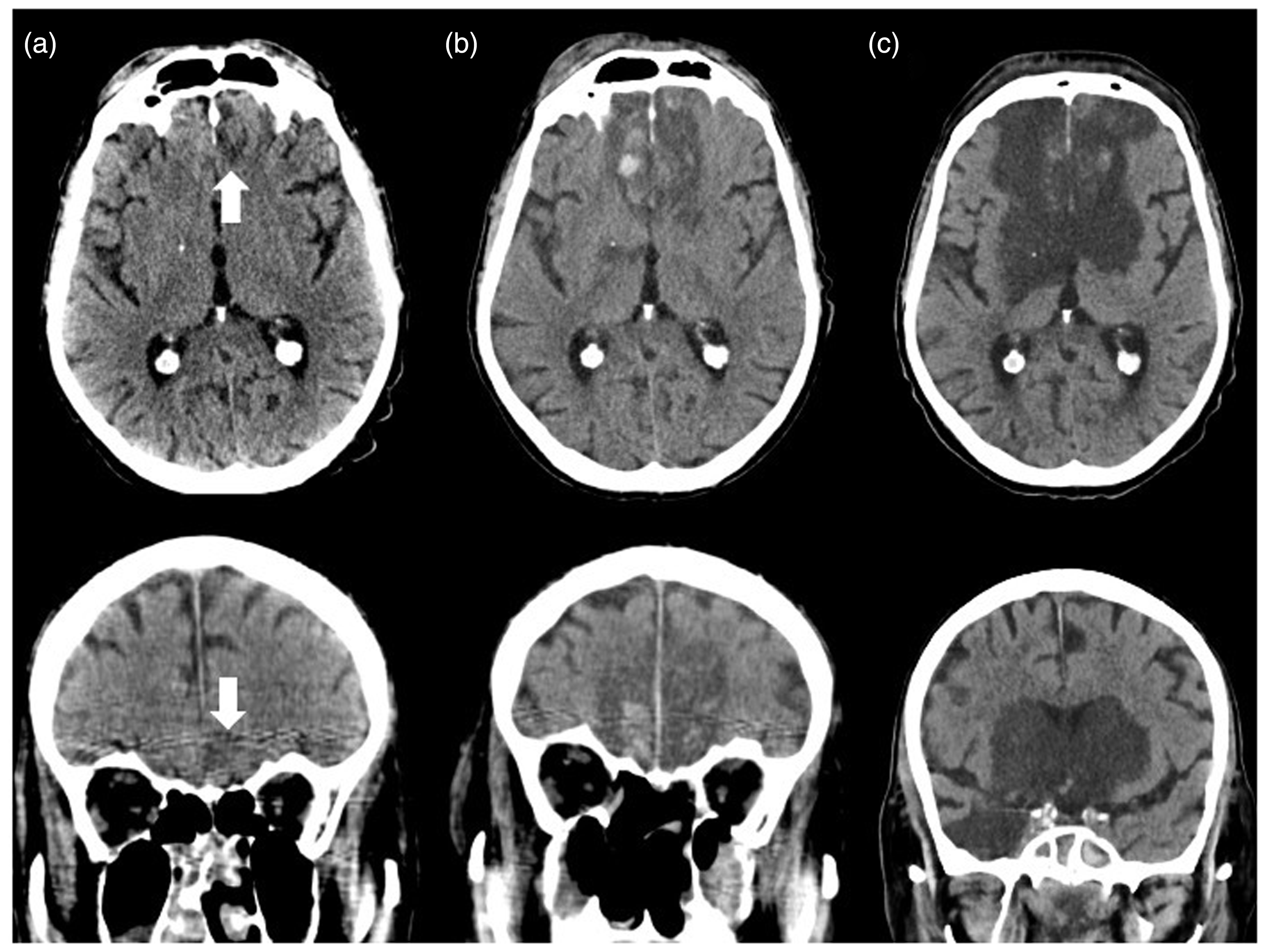
Unenhanced CT in the axial and coronal planes of a 64-year-old male patient with acute myeloid leukemia and RCM (same patient as in Figs. 1a, 1b, 2, and 3) shows hemorrhagic transformation of a brain infarct: (a) cerebral infarction of gyrus rectus (arrows) by RCM complicated by (b) frontal cerebral hemorrhage (one day later) and (c) right temporal and bilateral basal ganglia infarction (two days later). CT, computed tomography; RCM, rhinocerebral mucormycosis.
Mycotic aneurysms carry a high mortality rate and are listed among the main causes of subarachnoid hemorrhage in fungal cerebral infections. Further complications associated with mycotic aneurysms include embolic infarction and an ongoing source of infected microemboli (35).
Unenhanced brain CT is a fast and readily available tool to detect intracranial blood and its extension. CT angiography, or MR angiography, are necessary to define the location and size of the aneurismatic dilatation.
Spread into the intracranial space may also result in sagittal sinus thrombosis or brain surface vein thrombosis, with consequent venous congestion, and subsequent cerebral hemorrhagic ischemia. CT venography or MR angiography with MR venogram demonstrates the absence of venous flow in the affected venous dural sinus (38).
Generally, unenhanced CT with soft and bone algorithm reconstruction should be done in every patient with suspected RCM infection to assess the real extension of paranasal sinuses inflammation.
An MRI scan should be executed in every patient with confirmed RCM infection, to better define orbital invasion and intracranial complications, considering MR angiography as a first choice for studying intracranial arteries, since it does not expose the patient to ionizing radiations and does not require administration of contrast medium.
For early detection of arterial wall invasion and to prevent arterial occlusion and cerebral infarct, advanced MRI sequences should be performed in every patient with intracranial complications at risk of vascular involvement (e.g. proximity of the infection to main intracranial arteries, such as the pharyngeal space or posterior wall of the sphenoid sinus).
Conclusions
Neuroimaging plays a critical role in the early diagnostic process of RCM. Specific imaging findings and advanced MRI sequences contribute to the assessment of RCM vascular complications, which are the main cause of this disease’s lethality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.