
Abstract
Background
Little is known about the associations between cardiovascular risk factors (CRF) and disc degeneration (DD).
Purpose
To evaluate the potential association between CRFs and intervertebral DD in a population-based sample.
Methods
A total of 400 participants from the community-based KORA-study were assessed in terms of CRFs, specifically obesity, hypertension, diabetes, elevated LDL-c, low HDL-c, elevated triglycerides, smoking status, and alcohol consumption. The patients additionally underwent whole-body magnetic resonance imaging (MRI) using T2-weighted single-shot fast-spin-echo and T1 dual-echo gradient-echo Dixon pulse sequences. Thoracic and lumbar DD were assessed using the Pfirrmann score and for the presence of disc bulging/protrusion. Cross-sectional associations between CRFs and MR-based Pfirrmann score were then analyzed.
Results
A total of 385 individuals (58.2% men; mean age 56.3 ± 9.2 years) were included. Prevalence of DD was 76.4%. Older age (β = 0.18; 95% CI 0.12–0.25; P < 0.001) and higher body mass index (BMI) (β = 0.19; 95% CI 0.06–0.30; P = 0.003) were significantly associated with DD of the thoracolumbar spine. Diabetes was significantly associated with DD at T7/8 (P = 0.029) and L3/4 (P = 0.017). Hypertension correlated significantly with DD in univariate analysis, but the association did not persist using multivariate analysis (β = 0.53; 95% CI –0.74 to 1.81; P = 0.41). None of the other CRFs (P ≥ 0.11) were associated with advanced DD. Disc bulging was independently associated with hypertension (β = 0.47; 95% CI 0.27–0.81; P = 0.01).
Conclusion
A significant independent association exists between age, BMI, and intervertebral DD. In contrast, there is no significant association between cardiovascular risk factors and DD. Providing strong evidence that the pathologic process undergirding DD is mechanical, rather than microvascular, in nature.
Keywords
Introduction
Chronic back pain is extremely common in western nations, potentially leading to physical and psychological restrictions of patients, and carrying considerable societal cost as a consequence (1–3). Commonly associated factors predisposing individuals to chronic back-pain include disc degeneration (DD) with reduced intervertebral disc space, obesity, congenital spine disorders, and vertebral injuries; however, the majority of cases involve no clear inciting factor and are likely multifactorial (4–6).
DD is considered the initial step in the spinal alteration process (4). The prevalence of DD is in the range of 37%–96%, depending on spinal section and patient age (7–9). Degenerative disc changes result fundamentally from the loss of proteoglycans from within the nucleus pulposus of the intervertebral discs, which results in disk height loss and disc herniation, which may subsequently cause stenosis of the spinal canal or neuroforamina (4).
Data regarding specific risk factors for DD are chiefly derived from clinical studies evaluating patients with back pain; comparatively little is known about the associations between cardiovascular risk factors (CRFs) and DD in a general population. Recently, there has been growing evidence that DD may be caused by compromised microcirculation of the intervertebral discs due to atherosclerosis and resulting vascular occlusion. A patient’s risk for these vascular occlusions is markedly affected by CRF, which include high body mass index (BMI), hypertension, diabetes, low HDL-c, elevated LDL-c, and elevated triglycerides (10–13). Thus, recent studies suggest that high LDL and triglyceride levels may directly contribute to DD (14,15). Smoking has been theorized to potentially impact DD; similarly, there is evidence that alcohol consumption may be associated with lower back pain but has not been shown to have a direct effect on degenerative disc changes (6,11,16). Despite this mounting evidence, the precise relationship of CRFs and DD remains controversial.
While age substantially influences degenerative changes of the disc (7,17,18), little is known about diabetes-related effects on DD (19,20). Recent research has demonstrated that high BMI represents a major risk factor for DD along the entire spine (10,19); both waist circumference and abdominal diameter as measured by magnetic resonance imaging (MRI) in male patients were significantly associated with DD, which may be due to chronic inflammation caused by proinflammatory cytokines released from excess adipose tissue (1,20). In contrast, evidence for an association between DD and hypertension is limited and remains controversial (21).
The aim of the present study was to evaluate the potential association between CRFs and intervertebral DD in a population-based sample.
Material and Methods
Study design
The KORA Study (Cooperative Health Research in the Augsburg Region) was established in 1996 as a prospective study with a focus on cardiovascular and cerebrovascular complications and impaired glucose metabolism (22). The participants in this study were drawn from the second follow-up KORA-FF4 cohort between 2013 and 2014, which comprises a sub-group of 400 individuals who underwent whole-body MR scans. The detailed study design with inclusion and exclusion criteria has been described previously (23).
Written consent was obtained from each participant. Ethical approval was granted by the institutional review board of the Ludwig Maximilian’s University Munich (Germany) (Project No. 498-12).
Cardiovascular risk factors
CRFs were assessed as a part of the primary KORA Study. Participants were classified depending on their oral glucose tolerance test (OGTT) and fasting glucose levels into healthy, prediabetic, and diabetic strata. Healthy participants were defined as having no known diabetes, serum glucose levels < 140 mg/dL 2 h after the OGTT, and fasting glucose levels < 110 mg/dL. Prediabetic participants were defined as having elevated serum glucose levels in the range of 140–199 mg/dL 2 h after OGTT and/or impaired fasting glucose of 110–125 mg/dL. Participants with diabetes were characterized as having serum glucose levels ≥200 mg/dL after 2 h after OGTT and/or fasting glucose levels of ≥126 mg/dL.
Age and obesity measures of this population have been described in detail elsewhere (22). BMI was assessed as the participants’ weight in kilograms (kg) divided by square of height in meters (m2).
Hypertension was defined as systolic and diastolic blood pressure ≥140 mmHg and 90 mmHg, respectively. Participants with a prior diagnosis of hypertension actively treated with antihypertensive medication were included in the hypertensive group. The measurements of serum triglycerides, LDL-c, and HDL-c were conducted, and are described in detail in prior work (22).
Lifestyle and back pain
Lifestyle conditions were assessed using a standardized interview. Smoking was classified in three subgroups: current smoker; former smoker; or never smoker. Alcohol was assessed as grams per day.
Back pain was graded on a single-choice question with five levels: A = none; B = little; C = moderate; D = strong; and E = very strong.
Imaging protocol
MRI whole-body datasets were acquired on a clinical 3-T scanner (Magnetom Skyra, Siemens Healthcare, Erlangen, Germany). A detailed description of the imaging protocol and technical details are described by Bamberg et al. (23). To assess musculoskeletal structures, a T1-weighted (T1W) dual-echo Dixon gradient-echo (GRE) sequence was employed (imaging parameters: matrix = 256 × 256; field of view [FOV] = 488 × 716 mm; TE = 1.26 ms and 2.49 ms; TR = 4.06 ms; partition segments = 1.7mm; flip angle = 9°). A T2-weighted (T2W) single-shot fast spin-echo (FSE) sequence was additionally performed (image parameters: matrix = 320 × 200; FOV = 296 × 380 mm; TE = 91 ms; TR = 1000 ms; partition segments = 5 mm; flip angle = 131°).
Image analysis
Image evaluation was performed independently in a randomized and blinded fashion by two radiologists with 4 and 11 years of experience in musculoskeletal imaging, respectively. To determine intra-reader agreement, 40 cases were randomized and blinded in order to be re-evaluated by the primary reader.
DD was assessed using the Pfirrmann score for each segment from thoracic vertebrae 1 (T1) to lumbar vertebrae 5 (L5) (9,24). Using this technique, grade 1 was defined as homogenous white structure of the disc, grade 2 as inhomogeneous with/without horizontal bands, grade 3 as annulus and nucleus with clear distinction, grade 4 as an almost collapsed disc, and grade 5 as a collapsed disc. An aggregation of grades 1 and 2 as a subgroup was performed, as both are classified as low-grade DD (9). Classification in accordance with the Pfirrmann score was implemented on coronal and reconstructed sagittal image datasets (Fig. 1).
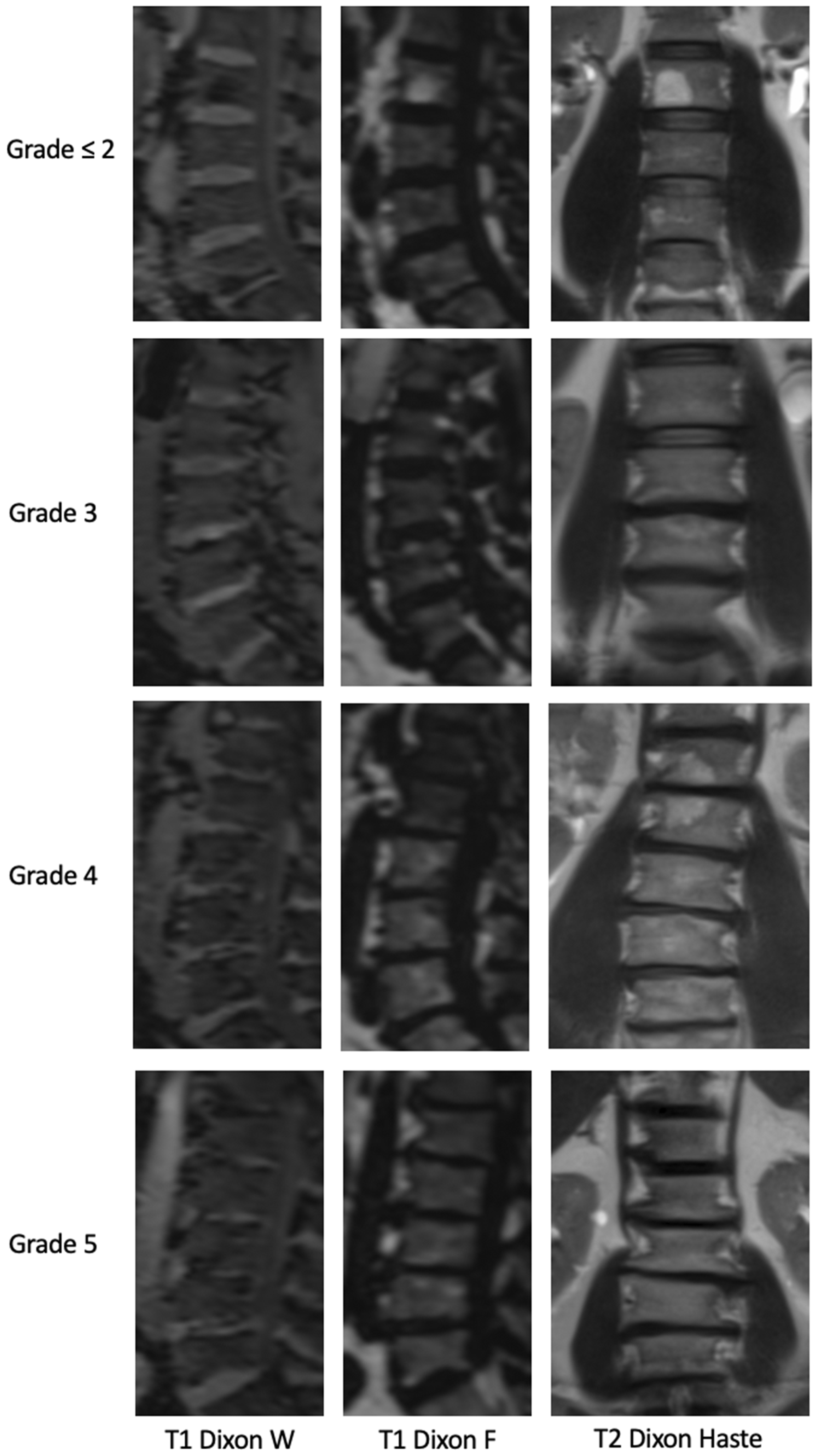
Example images of Pfirrmann grading of the lumbar spine (from the bottom plate of thoracic vertebra 12 to the cover plate of sacral vertebra 1) using reconstructed sagittal T1 Dixon iso F and W, and coronal T2 Haste. Increasing Pfirrmann score is demonstrated at intervertebral disc level L3/4. The complete grades for each of the lumbar vertebral discs depicted are as follows:
Visible disc herniation into the spinal canal was subclassified as disc bulging (a bulge not exceeding the adjoining vertebrae) or disc protrusion (a perimeter of the intervertebral discs exceeding the adjoining vertebrae).
Statistical analysis
CRF and MR-based Pfirrmann scores are presented as mean and standard deviation (SD) for continuous variables and counts and percentages for categorical variables.
Cross-sectional associations of CRF with the dependent outcome variables of MR-based summed continuous Pfirrmann scores (thoracic, lumbar, and thoracolumbar spine) were assessed via multivariate linear regression providing β-coefficients with 95% confidence intervals (CI). The models included age, sex, BMI, hypertension, HDL-c, LDL-c, triglyceride, hemoglobin A1c percentage, diabetes status, smoking status, and consumption of alcohol, and were adjusted by disc bulging and disc protrusion. Associations of the same risk factors with disc bulging and protrusion were assessed by multivariable logistic regression models providing odds ratios (OR) with 95% CIs. Inter- and intra-reader agreement were performed using Cohen’s Kappa (K).
A P value < 0.05 was considered statistically significant. All analyses were conducted using Stata 14.1 (Stata Corporation, College Station, TX, USA).
Results
Among the 400 participants in the study, 15 (3.8%) were excluded due to poor image quality. In total, 385 participants (96.2%) were included (Fig. 2).

Inclusion and exclusion flow chart.
The mean age of the study participants was 56.3 ± 9.2 years with 58.2% men. Participants were generally overweight with an average BMI of 28.1 ± 4.97 kg/m2. Of the participants, 34.8% had hypertension, 13.5% had diabetes mellitus, and 24.9% had prediabetes. Some degree of back pain was reported by 55.1% of the participants. Rates of CRF across the study participants are shown in Table 1.
Rates of cardiovascular risk factors and disc degeneration within the study sample (n = 385).

Values are given as n (%) or mean ± SD.
BMI, body mass index.
Disc degeneration
Prevalence of DD in the thoracolumbar spine was 76.4% (mean summed overall Pfirrmann score = 4.2 ± 5.6), with the majority located in the lumbar (68.1%) and the minority in the thoracic region (40.8%). Univariate correlation showed that increasing age (P < 0.001), elevated BMI (P = 0.01), and hypertension (P = 0.003) were significantly associated with DD of the thoracolumbar spine.
Using multivariable analysis, both age (P < 0.001) and BMI (P = 0.003) were significantly correlated with DD of the thoracolumbar spine. Although gender correlated with degenerative disc changes of the thoracolumbar spine in its entirety (P = 0.05), a sub-analysis of the sections (thoracic or lumbar spine) showed no significance. Neither hypertension, diabetes, HDL-c level, LDL-c level, triglyceride level, smoking status, nor amount of alcohol consumption correlated with DD of the thoracolumbar spine using multivariate analysis.
Disc bulging significantly correlated with lumbar, but not with thoracic DD, whereas disc protrusion was found to be significantly correlated with thoracic and lumbar DD using multivariate analysis (Table 2). No correlation was observed between back pain and the degree of DD (test of trend; P = 0.990), disc bulging (test of trend; P = 0.339), or disc protrusion (test of trend; P = 0.229).
Multivariate associations of cardiovascular risk factors with Pfirrmann score.

β-coefficients are from multivariable linear regression.Significant values/results are printed in bold.
BMI, body mass index; Ref., reference category.
Comparing each segment of the thoracic and lumbar spine regarding the influence of diabetes on DD, participants with diabetes showed significantly increased DD of T7/8 and L3/4 (P ≤ 0.029) compared to healthy patients (Fig. 3).

Level of DD for each segment of the thoracic and lumbar spine in healthy controls (left) and patients with diabetes (right). Severe degenerative changes with higher Pfirrmann scores (grade >2; pathological) are presented as light gray bars, while none to mild degenerative changes (grade ≤2; not pathological) are presented by a dark gray bar. Significantly increased DD of Th 7/8 and L3/4 was found in patients with diabetes compared to healthy controls. DD, disc degeneration.
Disc bulging and disc protrusion
The prevalence of disc bulging and disc protrusion were 37.4% and 27.8%, respectively. Using multivariable analysis, the frequency of disc bulging (P < 0.001) and disc protrusion (P = 0.019) increased with age. Hypertension was significantly associated with disc bulging (P = 0.01), but not with disc protrusion. There was no correlation between gender, BMI, HDL-c, LDL-c, triglyceride level, diabetes status, smoking status, or consumption of alcohol with disc bulging or disc protrusion of the thoracolumbar spine. Detailed data are summarized in Table 3.
Multivariable associations of cardiovascular risk factors with disc protrusion and disc bulging.

Values are given as OR (95% CI). ORs are from multivariable logistic regression.Significant values/results are printed in bold.
BMI, body mass index; CI, confidence interval; OR, odds ratio; Ref., reference category
Correlation of back pain with hypertension
Of the participants, 134 (34.8%) had hypertension. Of these, 81 (60.4%) experienced some level of back pain. However, there was no significant correlation between back pain and hypertension (P = 0.079), even when combining the back pain subcategories “strong” and “very strong” into one variable (P = 0.100) (Table 4).
Correlation between back pain and hypertension.

Values are given as n (%).
Inter- and intra-reader agreement
The intra-reader agreement on assessing thoracolumbar DD was almost perfect (85%; Kendall W = 0.93), as was the inter-reader agreement (87.5%; Kendall W = 0.92). Disc bulging showed perfect intra- and inter-reader reliability with 100% concordance (K = 1.0). Disc protrusion also showed a perfect intra-reader concordance (100%; K = 1.0) and near-perfect inter-reader agreement (95%, K = 0.84).
Discussion
The present study examined the association between CRFs and DD of the thoracolumbar spine using whole-body MRI scans in a population-based sample without clinical cardiovascular disease. It was found that age and BMI are independently associated with DD of the thoracolumbar spine.
In contrast, HDL-c, LDL-c, triglyceride level, smoking habits, and consumption of alcohol were not significantly associated with DD. The association of DD and hypertension was limited to univariate analysis alone and did not persist on multivariate analysis. Participants with diabetes showed increased DD at T7/8 and L3/4 compared to participants without diabetes. Age was positively correlated with disc bulging and protrusion, while BMI was not. Hypertension was significantly associated with disc bulging but did not correlate with back pain.
Prevalence of DD in this study was in line with the literature, which is in the range of 37%–96%, depending on spinal section and patient age (4,7,8). Our results agree, with the lumbar spine being more frequently affected than the thoracic.
Age was strongly associated with DD of the thoracolumbar spine. This is consistent with findings from prior literature, though Teraguchi et al. (4,18) demonstrate that only the incidence correlates with age and not progression (7,8,17,25).
Teraguchi et al. (4,19) additionally investigated the correlation between body weight and DD throughout the spine using MRI. They found a positive correlation for the thoracolumbar and cervical spine, similar to the association of the thoracolumbar spine in our cohort. Both obese adolescents and adults were more likely to develop lumbar DD (17,26,27); the impact of being overweight at a young age was significantly greater than being overweight at the age of 40–45 years (28).
However, discrepancy exists within the literature, as other studies have shown no correlation between BMI and cervicothoracic DD (29,30). The effect of body weight on DD seems to be further influenced by gender, as abdominal obesity was associated with lumbar DD in men but not women (1).
Lener et al. (31) demonstrated a correlation between obesity and disc herniation in patients aged less than 25 years; interestingly, to the authors’ knowledge, no previous data regarding the association between weight and disc bulging exists for patients aged 25 years and older.
No association was observed between diabetes and DD of the thoracolumbar spine, except for the segments T7/8 and L3/4. While only these two-disc levels meet this threshold of significance, this is most likely due to statistical coincidence alone.
The results of the present study agree with those of Fabiane et al. (32), who showed that diabetes was not independently associated with DD when adjusted for age and BMI. In contrast, a four-year follow-up study with 617 participants by Teraguchi et al. (18) found diabetes to be a significant risk factor for DD of the upper lumbar spine, noting that a preceding study by their working group demonstrated an association between diabetes and thoracic, but not lumbar, DD. They hypothesize that the variance was the result of a brief follow-up period and a relatively small sample size in their initial study. Liu et al. (33) emphasized that the duration of diabetes, and the management of the disease, have a decisive influence on lumbar DD as well, although a precise mechanism for the resulting DD was not elucidated.
A pathologic process linking diabetes and DD has not been established; it is hypothesized that (i) DD may be caused by microangiopathy and worsened by diabetes (34) or (ii) that the formation of advanced glycation end products effect catabolic on the nucleus pulposus and induce inflammatory reactions by enhancing proinflammatory cytokines (35,36).
One of the first studies evaluating the impact of CRFs on DD was the Wakayama spine study in Japan. A significant association between hypertension and thoracic DD was shown; however, this was observed in the thoracic, but not the cervical or lumbar regions (19). The proposed pathophysiology was based upon hypertension-induced vasosclerosis, which may result in derangements of disc perfusion (19). Contrasting data were subsequently published by Samartzis et al. (21) showing that patients with lumbar DD had a significantly higher blood pressure than those with healthy discs. Bruehl et al. (37) identify an interaction between the cardiovascular and the pain regulation systems, showing that an increased resting blood pressure is associated with an increased pain sensitivity and pain intensity in patients with chronic pain. In contrast to this prior work, the present study did not find a significant relationship between hypertension and DD at any level.
This results of this study demonstrate no association between HDL level, LDL level, or triglyceride level and DD or disc bulging, which is in line with the findings by Teraguchi et al. (19). In contrast, Hangai et al. (17) associated LDL level with DD and Longo et al. (15) demonstrated that patients with symptomatic lumbar disc herniation had significantly higher triglyceride and total cholesterol levels, concluding that increased serum lipid levels increase the risk for DD. These findings are supported by a recent study by Zhang et al. (14), which demonstrated that lumbar disc herniation is associated with dyslipidemia.
Nicotine is known to cause vasoconstriction, and is postulated to consequently reduce blood flow to the intervertebral discs (38). However, findings on the impact of alcohol and tobacco on DD remain controversial (39). Some studies verified that smoking was associated with lumbar disc protrusion or DD (30,40). Contrary, but in line with the results of the present study, Gore et al. (41) did not find that smoking was a risk factor for DD of the cervical spine (39). Similar to the results of the present study, recent studies have shown no association between alcohol and DD (32,42).
The study cohort included in this study was drawn from a healthy sample of the southern German population, which may limit comparisons to other populations. The study consisted of a small sample size of participants with well-controlled diabetes mellitus. Thus, larger clinical studies in specific cohorts may be necessary to increase statistical power in order to observe statically significant associations of small magnitude; however, these associations are less likely to be clinically significant. The study protocol did not include specific MR sequences of the spine which might have an impact on the visually assessed Pfirrmann score. Since this score has no quantitative measurements, it may have been influenced negatively by the sagittally reconstructed nature of the coronally acquired images. Additionally, bony degenerative changes, such as osteochondrosis, were not considered in the criteria of degenerative spine changes.
Lastly, although the pathophysiology and effect magnitude are not yet fully understood (43), there is a known genetic component affecting DD. While the standardized questionnaire for participants of the KORA study included questions regarding heredity diseases (e.g. stroke and malignancies), familial DD was not assessed, and thus could not be included in statistical analysis.
In conclusion, a significant independent association exists between age, BMI, and intervertebral DD. In contrast, there is no significant association between CRFs and DD. Providing strong evidence that the pathologic process undergirding DD is mechanical, rather than microvascular, in nature.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.