
Abstract
Background
Literature on radiologist-patient communication of musculoskeletal ultrasonography (US) results is currently lacking.
Purpose
To investigate the patient's view on receiving the results from a radiologist after a musculoskeletal US examination, and the additional time required to provide such a service.
Material and Methods
This prospective study included 106 outpatients who underwent musculoskeletal US, and who were equally randomized to either receive or not receive the results from the radiologist directly after the examination.
Results
In both randomization groups, all quality performance metrics (radiologist's friendliness, explanation, skill, concern for comfort, concern for patient questions/worries, overall rating of the examination, and likelihood of recommending the examination) received median scores of good/high to very good/very high. Patients who had received their US results from the radiologist rated the radiologist's explanation and concern for patient questions/worries as significantly higher (P = 0.009 and P = 0.002) than patients who had not. In both randomization groups, there were no significant differences between anxiety levels before and after the US examination (P = 0.222 and P = 1.000). Of the 48 responding patients, 46 (95.8%) rated a radiologist-patient discussion of US findings as important. US examinations with a radiologist-patient communication regarding US findings (median = 11.29 min) were significantly longer (P < 0.0001) than those without (median = 8.08 min).
Conclusion
Even without communicating musculoskeletal US results directly to patients, radiologists can still achieve high ratings from patients for their communication and empathy. Nevertheless, patient experience can be further enhanced if a radiologist adds this communication to the examination. However, this increases total examination time and therefore costs.
Introduction
Communication between radiologists and patients is regarded as a contribution to healthcare, as part of the value-based healthcare concept (1–3). However, it remains unclear which patient communication tasks belong to radiologists. Some argue that radiologists should not discuss results of imaging examinations with patients, because without the full clinical picture and established patient-physician relationships, this would cause confusion and may increase anxiety in patients (1). In addition, it has been postulated that it is unknown how many patients may wish to receive results directly from a radiologist, and that this places a false demand on radiology, which is already under siege from increasing workloads (4,5).
So far, there has been a lack of studies on this topic in the field of musculoskeletal ultrasonography (US). Meanwhile, the volume of musculoskeletal US has risen considerably over the past decades (6). US is increasingly performed by radiologists, but also by other specialists such as primary care physicians, emergency care physicians, rheumatologists, and podiatrists (6). In their role as treating physician, non-radiology specialists are in the natural position to directly communicate US findings to their patients. However, this does not apply to radiologists.
At our institution, musculoskeletal US is performed and interpreted by dedicated musculoskeletal radiologists. There is currently no consensus on whether the US findings should be communicated by the radiologist to the patient directly after the examination. Given the era of patient-centered medicine and recent studies that indicated a potential benefit of direct communication of imaging results from radiologists to patients (7–9), it is hypothesized that such a practice is valued by patients who undergo musculoskeletal US in a radiology department. Meanwhile, it is also important to gain knowledge on the additional time required to communicate results to patients in musculoskeletal US practice, given the fact that time equals costs from a management perspective. This information is necessary for healthcare professionals, patients, and society to weigh the potential benefits of radiologist-patient communication of imaging results against the costs.
Therefore, the aim of the present study was to investigate the patient's view on receiving the results from a radiologist after a musculoskeletal US examination, and the additional time required to provide such a service.
Material and Methods
Study design
The prospective study was approved by the institutional review board of the University Medical Center Groningen and informed consent was obtained from all participating patients. All diagnostic musculoskeletal US examinations that were performed by a single musculoskeletal radiologist (T.C.K., with 2.5 years of post-residency experience) in outpatients aged ≥18 years at a tertiary care center between February 2019 and May 2020 were potentially eligible for inclusion. Patients were equally randomized into two groups: one group in which patients were informed by the radiologist about their US findings directly after the examination; and a second group in which patients did not receive any information from the radiologist regarding their US findings directly after the examination. The following individuals were excluded from the study: patients who were already participating in another study; patients who were unable to read or write Dutch; patients who underwent an image-guided intervention immediately after the diagnostic US examination; and patients who refused to participate.
US procedure
A doctor's assistant prepared each patient for the examination by performing an identity check, instructing and/or helping the patient to uncover the body part of interest and to lie on the examination table or to sit on a mobile stool (the latter for all upper extremity examinations), and setting up the US system for direct use by the radiologist. All US examinations were performed with either one of two systems (Toshiba, Xario XG or Siemens Acuson S2000) using 8–18 MHz transducers.
Communication to patients
The radiologist introduced himself to each patient, performed history taking in addition to the information written on the clinical request form when deemed necessary, and told the patient that he would either inform or not inform the patient of the US findings after completion of the examination (depending on the randomization group). If a patient was randomized to receive the results from the radiologist after the examination, the radiologist also demonstrated and explained the stored US images on the monitor of the machine and answered any questions to his best ability. However, patients were told to discuss any questions related to treatment planning with their referring physician, to avoid interference and any potential discrepancies with the referring physician's patient management plan. All communication between the radiologist and the patient took place in the US examination room. Note that all patients also had a scheduled follow-up consultation with their referring physician in which the US findings were discussed between the referring physician and the patient, as part of standard clinical care.
Questionnaire
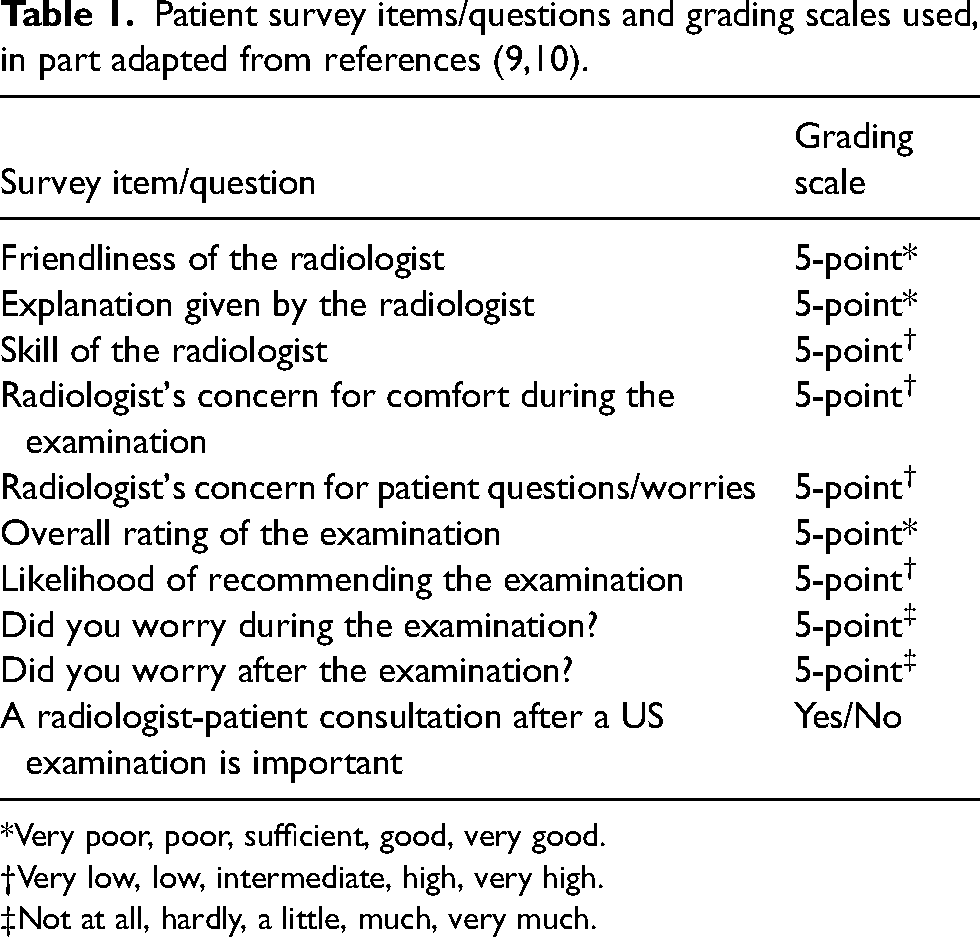
After completing the examination and instructing each patient to further discuss the US findings and the management plan with his or her referring physician, all patients were asked by the radiologist to participate in a study regarding patient satisfaction and services provided. Patients who were willing to participate, were given a paper-based questionnaire with a postage-paid self-addressed envelope. The questionnaire was anonymous, and all patients were asked to fill in the questionnaire anywhere outside the radiology department to avoid any potential influence of radiology staff on the patient's evaluation. The questionnaire was based on items from the Press Ganey patient satisfaction survey for radiography and US performed in the outpatient setting (10), and a previous study on radiologist-patient communication of magnetic resonance imaging (MRI) results (9). Patient survey items/questions and grading scales used are displayed in Table 1. In addition, patients were given the opportunity to write down any other remarks.
*Very poor, poor, sufficient, good, very good.
Very low, low, intermediate, high, very high.
Not at all, hardly, a little, much, very much.
Time measurement
The time between the moment the radiologist entered the examination room and the moment the radiologist left the examination room after completing the US (including communication of US findings to those patients who were randomized in this group) was measured with a digital timer.
Statistical analysis
Characteristics of included patients were descriptively analyzed. Age, gender, body part (upper extremity, lower extremity, or trunk), referring physician (general practitioner, orthopedic surgeon, rehabilitation medicine physician, plastic surgeon, sports medicine physician, or other), US findings (completely normal findings vs. any abnormality), and duration of the examination, were compared between patients who directly received information from the radiologist regarding their US findings and those who did not. Patients’ answers to the survey items/questions were compared between the two groups. Two-tailed unpaired t tests were used for Gaussian data (after a check for normal distribution using a Shapiro–Wilk test), Mann–Whitney tests for non-Gaussian and ordinal data, and chi-square tests for nominal data. A Wilcoxon test was used to compare differences in anxiety levels during and after the US examination. P values < 0.05 were considered statistically significant. Statistical analyses were executed using MedCalc version 17.2 Software (MedCalc, Ostend, Belgium).
Results
Patient population
A total of 119 patients were potentially eligible for inclusion. Eventually, 106 patients (43 men, 63 women; mean age = 51.3 ± 15.0 years; age range = 18–86 years) were included (Fig. 1). After randomization, 53 were assigned to the group of patients who received information from the radiologist regarding their US findings and 53 to the group of patients who did not. There were no significant differences in characteristics between the two groups (Table 2). One patient had a suspicion of residual malignant lymphoma, while there was no suspicion of malignancy in any of the other patients based on US findings.
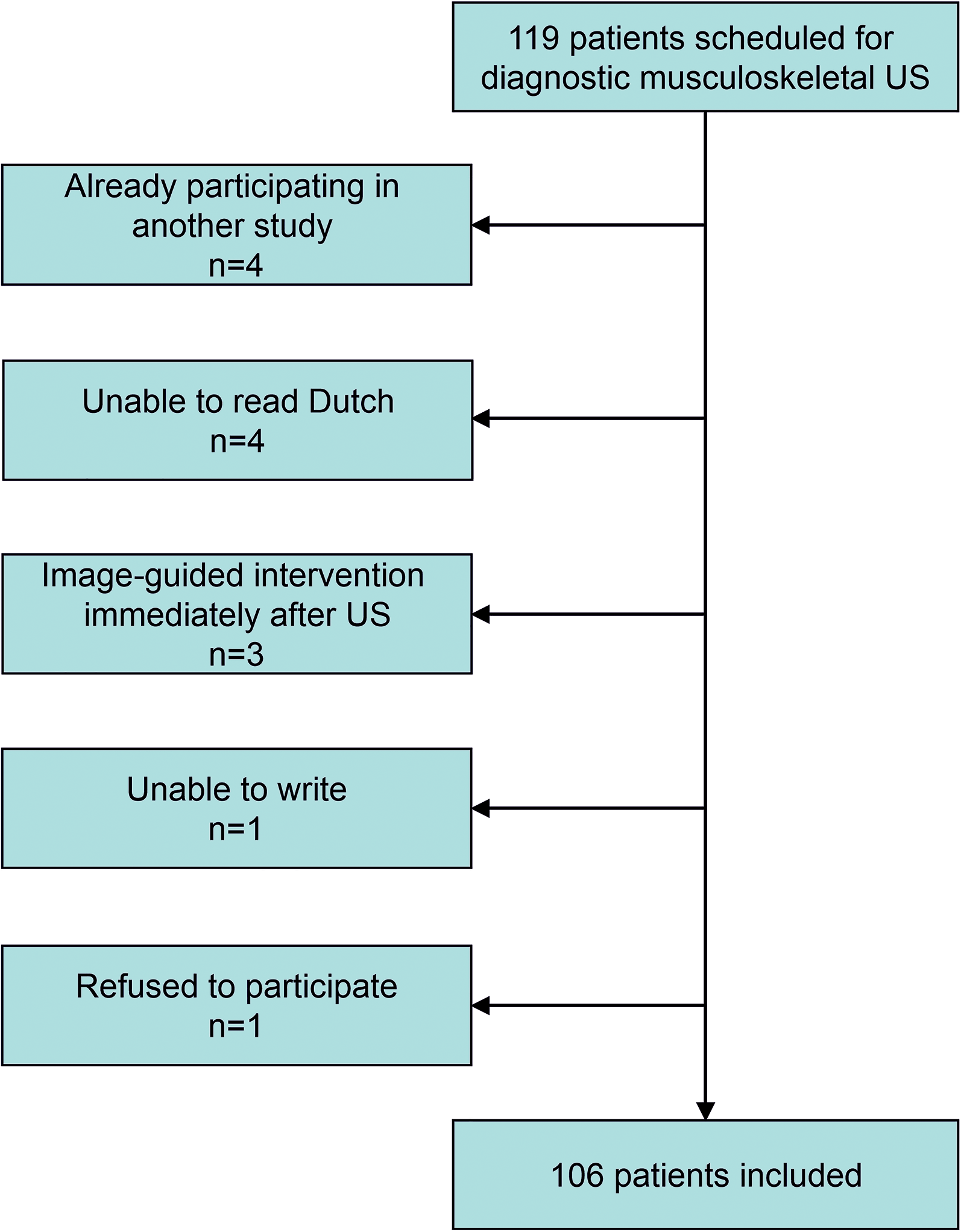
Flow chart of patient inclusion.
Comparison of characteristics between patients who received their US results from the radiologist directly after the examination to those who did not.
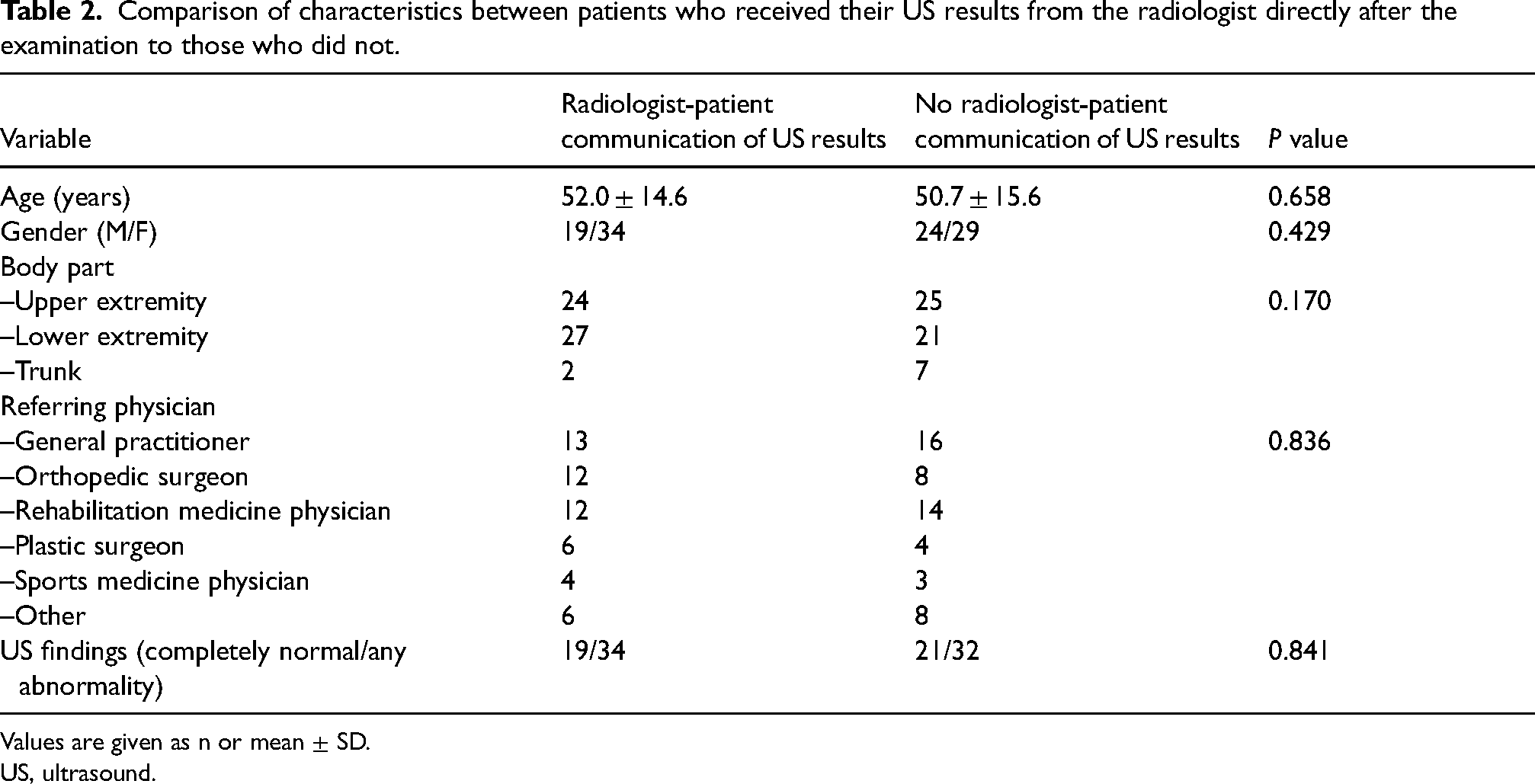
Values are given as n or mean ± SD.
US, ultrasound.
Patients’ experiences and preferences
Of 106 patients, 49 (46.2%) returned the questionnaire, of whom 27 had discussed their US findings with the radiologist and 22 had not. All quality performance metrics (radiologist's friendliness, explanation, skill, concern for comfort, and concern for patient questions/worries, overall rating of the examination, and likelihood of recommending the examination) received median scores of good/high to very good/very high in both groups (Table 3). The patients who had received their US results from the radiologist rated the radiologist's explanation and concern for patient questions/worries as significantly higher (P = 0.009 and P = 0.002) than the patients who had not. There were no significant differences in other quality performance metrics between the two groups (Table 3).
Comparison of responses to the survey items/questions between patients receiving a radiologist-patient consultation regarding their US findings and those not receiving such a consultation.

*Very poor (1) – poor (2) – sufficient (3) – good (4) – very good (5).
Very low (1) – low (2) – intermediate (3) – high (4) – very high (5).
Not at all (1) – hardly (2) – a little (3) – much (4) – very much (5).
Median with range between parentheses.
**One missing answer.
US, ultrasound.
Patients were generally not worried during and after the US examination, with median scores of “no to hardly any worries” in both groups (Table 3). There were only two patients who were “very much worried” during the US examination. The first patient was still “much worried” after being informed by the radiologist about the US findings and indicated the following on the survey form: “The radiologist was very involved and kind, and I highly appreciated this.” The second patient was not informed by the radiologist about the US findings, was still “very worried” after the US examination, and indicated the following on the survey form: “I could not watch the US images and nothing was told to me during the examination (whether the result was good or not good), I have no idea how it will go on from now and when I will receive the results.” Overall, there were no significant differences between anxiety levels before and after the US examination, in both the group of patients who had directly received information from the radiologist regarding their US findings and the group who had not (P = 0.222 and P = 1.000).
Of the 48 responding patients, 46 (95.8%) indicated a radiologist-patient discussion of US findings to be important, without any significant differences between patients who had actually received their US results from the radiologist and those who had not (Table 3).
Examination time
The median duration of all US examinations (i.e. time between the moment the radiologist entered the examination room and the moment the radiologist left the examination room after completing the US examination) was 9.55 min (range = 4.41–32.24 min). The duration of US examinations that involved a radiologist-patient communication regarding US findings (median = 11.29 min; range = 5.29–32.24 min) was significantly longer (P < 0.0001) than those that did not (median = 8.08 min; range = 4.41–18.20 min) (Fig. 2). The difference of the medians between both groups was 3.21 min.
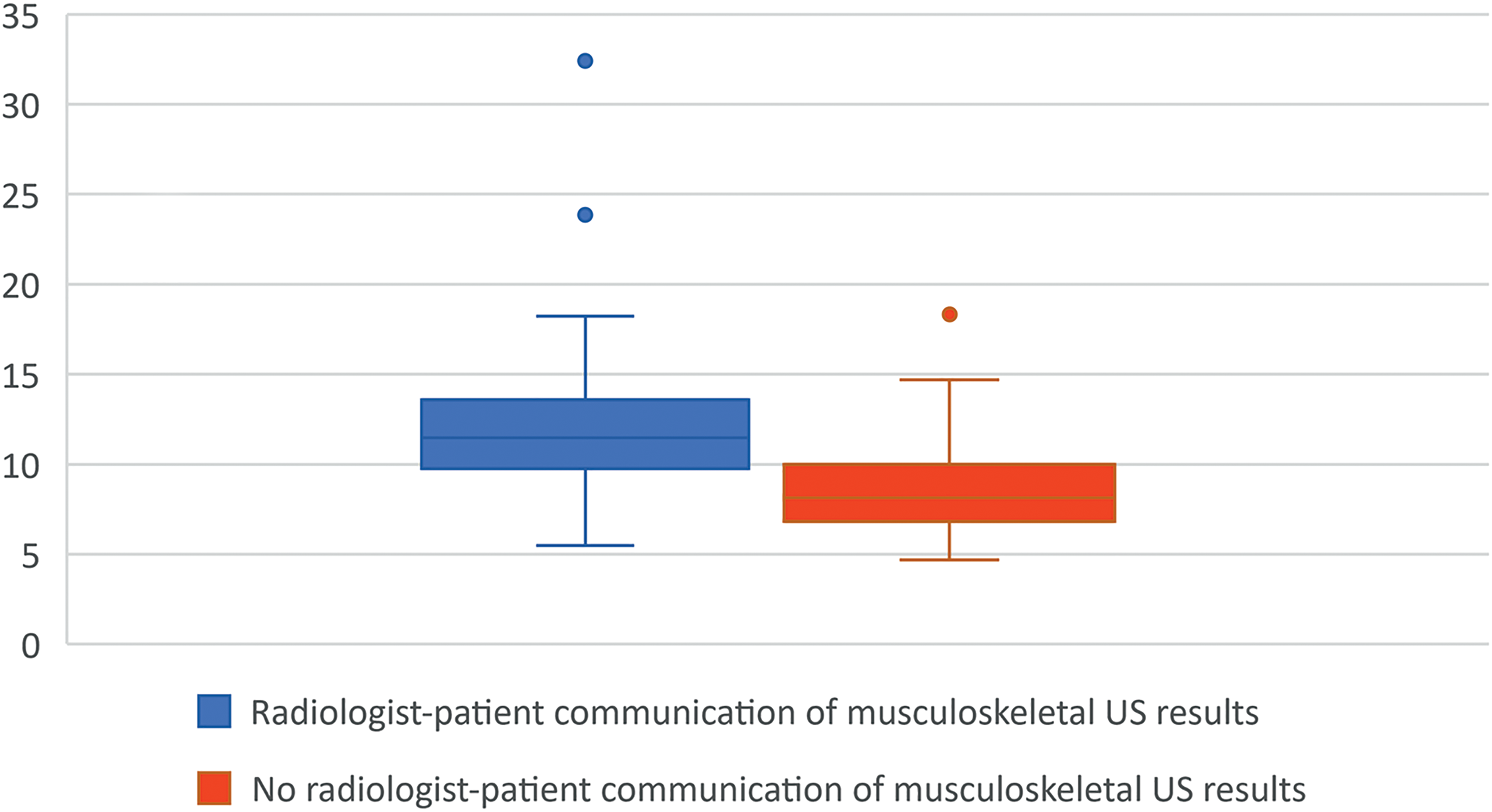
Box-and-whisker plots show median (middle line of box), quartiles (top and bottom lines of box), upper extreme value (upper whisker), lower extreme value (lower whisker), and outliers (circles) for US examination time (min) according to whether or not a radiologist-patient communication regarding US findings was included. The duration of US examinations that involved a radiologist-patient communication regarding US findings (median = 11.29 min) was significantly longer (P < 0.0001) than those US examinations that did not that involve a radiologist-patient communication regarding US findings (median = 8.08 min). The difference of the medians between both groups was 3.21 min. US, ultrasound.
Discussion
The results of the present study show that most patients wish to receive the results from the radiologist directly after a musculoskeletal US examination. When providing this service, radiologists can be regarded as more communicatively skilled and emphatic by their patients. Nevertheless, our findings also indicate that even without providing the US results directly to their patients, radiologists can still achieve a (sufficiently) high rating from their patients for their communication and empathy. Furthermore, all other quality performance metrics that were investigated in this study (radiologist's friendliness, skill, and concern for comfort, overall rating of the examination, and likelihood of recommending the examination) achieved high scores without any significant differences between patients who were and who were not informed of their US findings by their radiologist directly after the examination. In addition, patient anxiety levels were not significantly different during and after the examination in both groups. Therefore, although there is a potential benefit of incorporating a radiologist-patient communication regarding US findings in a musculoskeletal US examination, the added value does not appear to be huge. Finally, incorporating such a radiologist-patient communication requires an estimated additional 3.21 min per examination. For example, in a practice with 18 musculoskeletal US examinations on a daily basis, this would translate to 1 h of radiologist time. Whether or not the added value of a radiologist-patient communication of musculoskeletal US results weighs up against the costs should be decided by healthcare professionals, patients, and society.
There are two previous studies that have investigated the value of a direct radiologist-patient communication to discuss imaging results. In a study by Pahade et al. (8), 86 outpatients who underwent torso or abdominopelvic computed tomography (n = 37) or US performed by a sonographer (n = 49) were informed by a radiology fellow about their imaging results directly after the completion of their examination. After consultation, 91% preferred hearing results from both the ordering provider and the radiologist, 99% indicated they would be comfortable hearing normal or abnormal results from the person interpreting the examination, 99% agreed or strongly agreed that reviewing their examination findings with a radiologist was helpful, and 98% indicated they wanted the option of reviewing or always wanted to review future examination findings with a radiologist (8). In another study by Gutzeit et al. (9) in patients who underwent MRI of various body regions, 101 patients were given the opportunity to discuss the findings with the radiologist, and another 101 patients left the radiology department without any personal communication. Compared to the patients who did not discuss their imaging findings with the radiologist, the ones who did significantly more frequently perceived this opportunity as a characteristic of a good radiology consultation (81% vs. 14%) experienced significantly higher bonding and only wanted future examinations in the department with communication (93% vs. 75%) and regarded the radiology department they attended as significantly more competent (9). It is difficult to compare the present study with those of Pahade et al. (8) and Gutzeit et al. (9), because the latter two did not involve any musculoskeletal US. Nevertheless, all three studies showed that patients perceive a discussion with a radiologist of high value.
The present study had some limitations. First, the results are only applicable to musculoskeletal US. In addition, there was only one oncologic patient in the entire study population. The results may be different in other clinical settings. Second, only one radiologist performed all musculoskeletal US examinations. Future studies are required to confirm generalizability. Second, only 46.2% of patients returned the questionnaire, which may represent selection bias. Nevertheless, the distribution of respondents from each randomization group was fairly equal.
In conclusion, even without communicating musculoskeletal US results directly to patients, radiologists can still achieve high ratings from patients for their communication and empathy. Nevertheless, patient experience can be further enhanced if a radiologist adds this communication to the examination. However, this increases total examination time and therefore costs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.