
Abstract
This review looks at highlights of the development in ultrasound, ranging from interventional ultrasound and Doppler to the newest techniques like contrast-enhanced ultrasound and elastography, and gives reference to some of the valuable articles in Acta Radiologica. Ultrasound equipment is now available in any size and for any purpose, ranging from handheld devices to high-end devices, and the scientific societies include ultrasound professionals of all disciplines publishing guidelines and recommendations. Interventional ultrasound is expanding the field of use of ultrasound-guided interventions into nearly all specialties of medicine, from ultrasound guidance in minimally invasive robotic procedures to simple ultrasound-guided punctures performed by general practitioners. Each medical specialty is urged to define minimum requirements for equipment, education, training, and maintenance of skills, also for medical students. The clinical application of contrast-enhanced ultrasound and elastography is a topic often seen in current research settings.
Keywords
Introduction
Diagnostic use of ultrasound (US) was described almost 70 years ago (1–3). The development from bistable to grayscale images to real-time imaging, combined with an increasing number of commercially available systems, has led to a growing number of applications for US scanning (4).
We will look at some of the highlights in the development of US from interventional US, Doppler, and endoluminal US to the newest techniques like contrast-enhanced US and elastography and give references to some of the valuable articles published in Acta Radiologica.
Interventional Ultrasound
Interventional US is defined as a diagnostic or therapeutic procedure performed under US guidance. Along with the development of modern real-time ultrasound, US-guided interventional procedures for minimally invasive diagnostic and therapeutic purposes have evolved (5–7) either as freehand techniques, or assisted by a puncture attachment or puncture channel mounted on or built into the transducers.
US-assisted interventions were first reported by Berlyn and Joyner, both using a single element (A-mode) US transducer (8,9). The first US-guided procedure based on echoes representing a needle and a cystic target was presented at the first World Congress on Ultrasound by Kratochwill in 1969 using an A-mode US puncture transducer with a central slot for the puncture needle (10). Goldberg and Pollack developed a similar transducer in the USA and issued the first publication on US-guided puncture in 1972 (11).
The first punctures guided by static B-mode US images were carried out by Hans Henrik Holm (Figure 1) and his group in Denmark and presented at the annual meeting of the AIUM in 1970 (12). Holm's group performed US-guided biopsies from liver metastases (13,14) and US-guided aspiration of amniotic fluid (15) as well as pancreatic biopsies (16). US-guided percutaneous procedures from various sites were simultaneously reported 1972–1973 by Goldberg (11,17–20).
Prof. Hans Henrik Holm with a prototype dynamic ultrasound transducer—with the nick name “Rolling Mary”. Approx. 1974 (Photo by permission from Kirsten Holm).
The static US scanners were replaced by dynamic B-mode US scanners providing real-time imaging, which enabled continuous monitoring of a needle tip along a predicted route in the image plane, toward and into a predetermined target (Figure 2) as described by Saitoh & Watanabe (21) in 1979. The real-time US catalyzed the development of numerous clinical applications and remains an unsurpassed guide for interventional procedures, without radiation hazards or the need for electro-magnetic precautions, and cost-effective too.
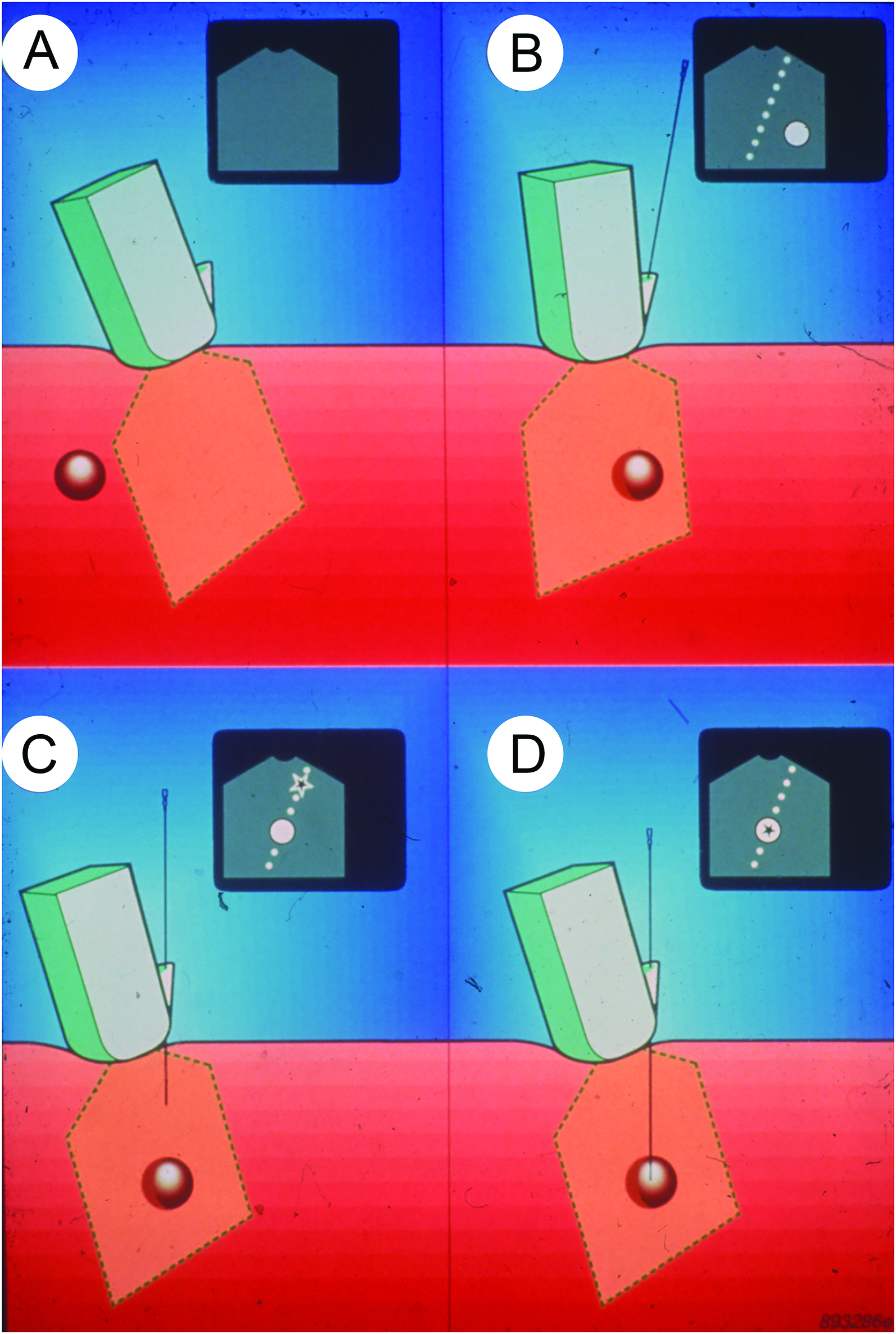
The principle of ultrasound-guided puncture.
US-guided percutaneous biopsy
Percutaneous US-guided fine and coarse needle biopsies of any US-detectable targets were developed and reported, e.g., from the pancreas (22,23), neuroendocrine metastasis (24), the spleen (25), and intrathoracic lesions (26). The type and diameter of the biopsy needle depend on the purpose and demand for diagnostic material (27). Dedicated automatic biopsy systems were developed for core biopsies to improve the yield (28,29) and these are widely used with US guidance today. High-resolution small-part transducers facilitated US-guided percutaneous biopsy from various sites, i.e., head and neck (30), parathyroid (31), thyroid (32), lymph nodes (33), brain (34), and breast (35).
US-guided needle and catheter drainage
Multiple US-guided drainages and catheterization procedures such as nephrostomy, paracentesis, cholecystostomy, abscess drainage, and vascular catheterization were established as rapid and safe alternatives to conventional drainage methods and open surgery. Either the US-guided needle puncture or one of two basic catheterization methods, the Seldinger technique or the trocar (one-step) technique, are used for US-guided drainage procedures (Figure 2). Percutaneous drainage of intra-abdominal abscesses and fluid collections was reported in 1982 (36) by the group of Van Sonnenberg, who never missed to include the words “Never let the sun set on an undrained abscess” in his numerous international lectures.
Dedicated catheters for drainage in combination with US-guidance provided a minimally invasive bedside alternative to surgery, i.e., in intensive care units (37), for percutaneous drainage of liver abscesses (38), breast abscesses (39), nephrostomy with an 8Fr. one step-balloon catheter (40), US-guided pericardiocentesis (41), as well as insertion of a peritoneo-gastric shunt for drainage of ascites (42). Transducers for transvaginal, transrectal, transoesophageal, and intraoperative use may circumvent the physical obstructions of percutaneous ultrasound from gas and bone and provide optimal transducer positions for visualization and guided access to internal organs subject for minimally invasive procedures. Endoluminal US-guided punctures evolved from transrectal US-guided prostatic punctures (43), and dedicated transducers with needle steering devices for transperineal, transrectal, and transvaginal interventional applications were subsequently developed (Figure 3) (43–46). Endoscopic US transducers with built-in puncture canals, used with dedicated biopsy systems, enabled US-guided biopsy of suspected malignant lesions in the upper gastrointestinal tract, mediastinum, pancreas, and retroperitoneal lymph nodes (47,48). US-guided biopsies during laparoscopy found use in the assessment of operability of patients with abdominal malignancies prior to major abdominal surgery (49).

Examples of guiding facilities for various ultrasound transducers for (A) transvaginal, (B) transperineal, and (C) multiplane transrectal interventions.
Other interventional procedures
US-guided fine-needle pyelography, combined endoscopic and abdominal US-guided cysto-gastrostomy, and combined fluoroscopic and US-guided gastrostomy (50,51) are examples of how combined imaging modalities facilitated by real-time ultrasound paved the way for minimally invasive procedures to substitute more invasive alternatives.
Nolsøe et al. reported as early as 1989 that US-guided subclavian vein catheterization was superior to the standard “blind” approach, with a substantial reduction of the procedure-related complications such as pneumothorax and bleedings (52). Today, US-guided vascular access is a common and widely used procedure, either using a transverse or a longitudinal image plane for US-guided vascular access.
Complications to interventional ultrasound
US-guided procedures have earned credit as minimally invasive procedures due to the low complication rates (53,54), although needle track seedings with a malignant deposit during biopsies have to be considered (55).
US-guided ablation
US-guided ablation techniques are based on the precise placement of a needle-shaped device or applicator in lesions subject to ablation by one of the ablation methods introduced along with the development of interventional US (6). US-guided interstitial brachytherapy has been used for years in the treatment of prostatic cancer, by some also for anal carcinomas. Transperineal I-125 seed implantation in prostatic cancer guided by transrectal US using a matrix steering device was used by Holm et al. in 1983 (56) followed by Blasko et al. (57). A variety of US-guided hyper-thermal injections of purified alcohol for ablation of parathyroid adenomas and hepatocellular carcinomas are low-cost, worldwide available ablation alternatives (58,59).
Thermal ablation procedures became treatment options for patients with non-resectable malignant tumors. These procedures included US-guided NdYAG Laser ablation (60), radiofrequency (RF) electrodes, and microwave-antennas, some with water-cooled shafts that extended the ablation volume and shaped it more spherical, and reduced unintended thermal injury during percutaneous US-guided procedures (61–64). Cryo-ablation and high intensity focused ultrasound (HIFU) are ablation alternatives, both with considerable logistic demands to be operative and therefore not widely used. Irreversible electroporation has been introduced as a non-thermal ablation modality available for US-guided procedures, including ablation of malignant pancreatic tumors (65).
Recent developments in interventional ultrasound
Contrast-enhanced ultrasound has improved the detection and differentiation of focal liver lesions and contributed to the reduction of the need for diagnostic biopsies, but may also be used to improve enhancement of biopsy targets, as well as for immediate detection of ablation insufficiency during radiofrequency and microwave ablations (66). 4-D real-time ultrasound transducers can display a needle tip in three orthogonal planes simultaneously, but comparative studies have not yet presented an advantage over 2D US in guiding percutaneous interventional procedures (67). Fusion US imaging, where a data set of a recent pre-recorded CT or MR volume is aligned with a real-time US image presented as side-by-side simultaneous images, has the potential to assist US-guided procedures otherwise blurred of US artifacts, i.e., US-guided ablation procedures (Figure 4) or US-guided marker implantation for stereotactic radiation therapy (68–70).
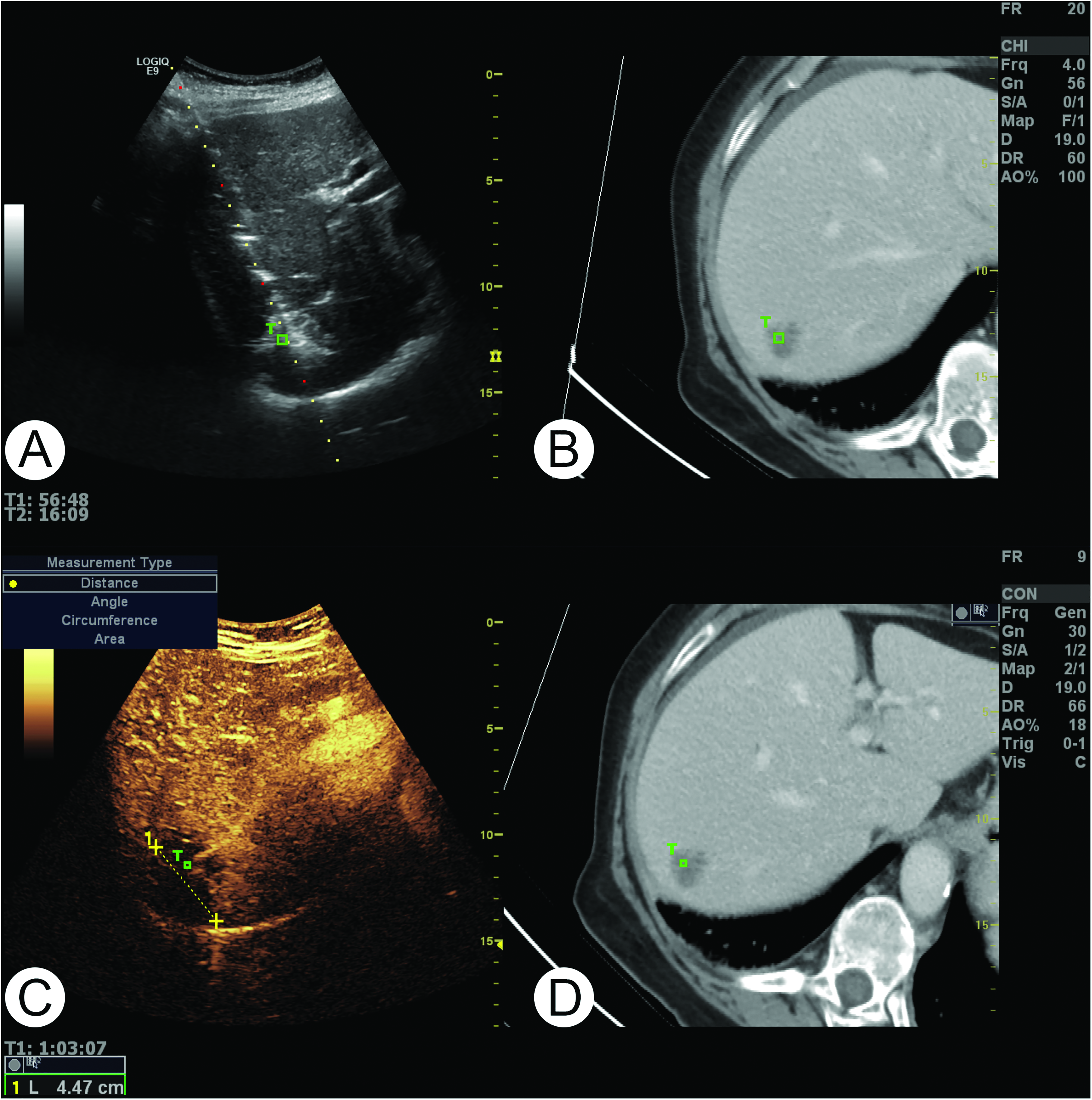
Fusion ultrasound imaging is applied for ultrasound-guided ablation of a colo-rectal metastasis in the liver.
Doppler
According to Christian Doppler's principle, a moving object exposed to one frequency will echo with another frequency depending on the direction and velocity of motion (71). The evaluation of blood flow has continuously been developed for more than 60 years (72). The method devised by Satomura was built upon the Doppler effect using transcutaneous continuous wave ultrasound with two piezoelectric quartz crystals, one emitting and one receiving (73). The first papers dealt with heart wall motion and flow patterns in the peripheral arteries but were soon followed by studies of e.g., aortic flow and venous return to the heart (74,75).
The early Doppler systems only generated an audible output for blood flow, and later in the early days presented as a frequency shift. Despite the non-invasive nature of the Doppler estimation being commercially available in 1965 by Smith Kline Instrument Co., the method was not a commercial success nor used for clinical decision making, which instead was guided by conventional invasive measurements. However, when pioneers began to convert the obtained signals to velocity, volume flow, and pressure gradients, the ultrasound method for flow evaluation became clinically interesting (76–78).
Doppler ultrasound was based on continuous-wave ultrasound, which has the limitation that the velocity is found along the interrogation line, and no information of depth is provided. A solution was proposed by Baker and Wells with the pulsed wave ultrasound system, known as the “intracardiac stethoscope” (79,80). With this development, a certain depth could be evaluated, and by applying angle correction to the velocity estimate of the range gate, the actual velocity content displayed when assuming flow parallel to the vessel borders.
Quantitative spectral Doppler has been developed in two directions: For flow evaluation of the heart and major vessels in the thorax as a cornerstone in cardiology, and flow in peripheral vessels of the systemic circulation used in radiology and other clinical specialties. Continuous- and pulsed-wave ultrasound systems form the basis of modern conventional spectral Doppler systems, where each Doppler approach has its limitations and advantages. Continuous-wave ultrasound is today mainly is used in cardiology (81).
The first B-mode ultrasound system for visualization of anatomy was designed to examine arteries just below the skin for the assessment of atherosclerosis (82). In 1974, a single probe for duplex scanning was invented for carotid flow, where B-mode and Doppler ultrasound were combined, which turned out to be a major advantage for flow mapping and grading of vessel lesions (83,84). Duplex and later triplex scans were rapidly used in the clinic e.g., for evaluation of arteriovenous fistulas and assessment of renal stenosis (85,86). From pulsed spectral Doppler, one of the most used Doppler indices—the resistive index—was introduced for kidney disorders but has later also been applied for other disorders such as rheumatoid arthritis (87–89).
The spectral Doppler ultrasound only evaluates flow in one dimension, i.e., along one line with continuous-wave Doppler and at one single spatial location with pulsed-wave Doppler. This limit was lifted by color Doppler, introduced by Kasai and Namekawa, where blood flow was visualized in 2-D within a color box displaying the axial motion of the blood flow (90,91). While spectral Doppler is a quantitative method, the color Doppler displays flow direction without quantitative measures.
Along with color Doppler, a variation called power Doppler was proposed, which is more sensitive to flow, though without the information of flow direction (92). The qualitative Doppler modes (power and color Doppler) and spectral Doppler are the Doppler modes available on all commercial scanners. They have been used for a variety of studies, ranging from tumor characterization to arthritis (93–98).
Doppler ultrasound is today an integrated part of the ultrasound examination and performed on the pediatric to the geriatric patient for both chronic and acute disorders. As in the early days, atherosclerosis is a major concern in Doppler diagnostics and can be assessed with spectral Doppler with analysis of the arterial acceleration curves (99). Another important task is the monitoring of transplants using ultrasound and Doppler assessment, as consecutive computed tomography seldom is possible due to the radiation exposure. This was early investigated, and several papers concerning Doppler ultrasound evaluation of renal and liver transplants have been published (100–102).
Recent developments in Doppler ultrasound
Conventional Doppler ultrasound is limited by angle dependency. New ultrasound methods for flow estimation, named vector flow imaging (VFI), have been proposed, where angle-independent velocity estimation can be achieved (103). Several studies have indicated that vector flow imaging is superior to conventional Doppler methods with higher precision and less operator dependency for velocity and volume flow estimation (104,105). Additionally, with the angle-independent estimation, complex flow patterns can be visualized and flow complexity assessed (106,107).
Conventional Doppler is also limited by framerate, as Doppler estimation and B-mode imaging are calculated line by line, which is a time-consuming process. This limitation is addressed by methods where the image plane is insonified by unfocused plane waves instead of focused ultrasound emissions. Combined with VFI, these methods have provided new insight to flow in complex geometries like the carotid bifurcation and around venous valves (108,109).
The newest branch in ultrasound flow estimation is done with contrast-enhanced ultrasound imaging and is called super-resolution imaging. With this technique, the microvasculature can be visualized, and functional imaging of the rodent brain has been achieved, along with an evaluation of the microvasculature of rodent kidneys (110,111).
Rectal Endosonography
“It has been said that the radiologist need not concern himself with detailed or special examination of the rectum and pelvic sigmoid colon, since this area is within easy reach of the gloved finger or sigmoidoscope and should naturally be relegated to the attention of the experienced proctologist or surgeon” (112). The above quote from 1960 is a great example of the view on colorectal examination in the medical world up until then. There was no need for further exploration than what could be achieved with a gloved finger. However, John J. Wild and John Reid had developed the first endorectal ultrasound scanner and examined the first patients already years before. Using a rotating high-frequency crystal, they managed to image rectal tumors and sonographically visualize the tumor through the intestinal wall (3). Their method, however, did not gain ground in clinical use at the time.
In the first half of the 1980s came the next publications on rectal endosonography (or transrectal ultrasound) of primary rectal tumors (113,114). The technique improved and paved the way for studies with a larger number of patients in the late 1980s and 1990s. A 1994 study using a 7.5 MHz linear array transrectal transducer showed a sensitivity of 96% and a specificity of 77% in staging tumor invasion into the mesorectal fat (115). The authors also found that the accuracy of rectal endosonography was superior to digital rectal examination using histopathology as an endpoint (115). Another study using a rotating transducer found a sensitivity of 96% and a specificity of 87% in diagnosing the tumor invasion (116). In addition, the normal sonographic anatomy of the anal sphincter was described (117–119).
In the new millennium, Blomqvist et al. showed that MRI was superior to endosonography in staging rectal cancer and that the mesorectal fascia was easier to visualize using MRI in contrast to using ultrasound (120). MRI has since then been recommended as the main staging method in rectal cancer. However, since MRI tends to over-stage small tumors, rectal endosonography is recommended in the staging of these (121). Rectal endosonography further allows distinguishing between adenomas and carcinomas to a certain degree (122). Recent technological advances with strain elastography have improved these results (123), but further studies using shear-wave elastography are required to confirm this initial promising outcome finally. The differential diagnosis between adenomas from adenocarcinomas before polyp removal is crucial to avoid removing a suspected benign polyp with piecemeal technique, only to discover later that it was “ups” cancer, in a situation where the pathologist is not able to tell whether the cancer was radically removed. The dilemma is then whether to pre-emptively resect the rectum or wait and risk a possible local recurrence. Rectal endosonography has also been used in the staging of anal cancer, as well as in the guiding of treatment (124). In addition, the scanning technique can be used for several benign disorders, including evaluation of anal fistulae and abscesses (121,125,126).
The new European guidelines now recommend using rectal endosonography in the staging of small rectal tumors (121). The technique requires 5−15 MHz transducers, and training is recommended as well as at least 50 examinations of experience. At the moment, endosonography cannot be recommended for assessing lymph node involvement in rectal cancer patients alone due to its moderate accuracy for differential diagnosis between benign and malignant lymph nodes. The method allows for biopsy and drainage, where percutaneous placement is not possible (45,46). In addition, it can be used in several benign conditions as well. Endosonography combined with elastography has shown promising results, but further studies of this method are still required (121).
Ultrasound of the Prostate
Ultrasound images of the prostate can be achieved in three different ways: transperineally, transabdominally, and transrectally (Figure 3). Transperineal and transabdominal ultrasound give only coarse images and cannot be used for detailed information. As for all ultrasound, high-frequency transducers and a short distance give the best images. Since digital rectal examination was the way to get information about the prostate before ultrasound was introduced, it was obvious to do ultrasound through the rectum (TRUS). In 1971, Professor Watanabe from Kyoto University was the first to do so (127). The equipment was far from what we know today, using a 360° rotating single crystal transducer in the rectum providing images with poor resolution and extreme contrast. However, symmetry/asymmetry could indicate benign or malignant conditions. After further research, Watanabe in 1975 stated: “The procedure is likely to become one of the most important diagnostic tools in the field of urology” (128). He was so right.
A fourth way—transurethral—of scanning the prostate, also using a 360° rotating single crystal mounted on a regular cystoscope, was described by Holm et al. in 1974 (129). However, the purpose of this technique was to determine the depth of invasion of tumors in the urinary bladder wall, and the technique is no longer used. In 1982, Holm et al. were the first to perform biopsies from the prostate guided by TRUS. The biopsies were done transperineally, and the transrectal transducer was still the 4 MHz 360° rotating single crystal type (130).
Now, being able to obtain precise samples from the prostate, it seemed obvious to place material in the prostate with the same precision, and in 1983, Holm et al. revolutionized brachytherapy treatment of prostatic cancer with the precise transperineal placement of radioactive I125 seeds in the prostate guided by TRUS, in contrast to the previous technique through an open laparotomy (56,131). The transperineal approach and transrectal ultrasound are still, almost 40 years later, the gold standard of prostatic brachytherapy. The ultrasound and the dose planning systems have, of course, evolved.
As the quality of the ultrasound equipment got better, more details in the prostate could be recognized. In 1989, Lee et al. described the zonal anatomy of the prostate using a high-frequency mechanical bi-plane transducer to give detailed transverse and sagittal images of the prostate and described the use of TRUS and biopsies in diagnosis and staging of prostate cancer (132,133). Numerous other studies have since been published regarding TRUS and biopsies, local staging, correlation with Gleason grading, and correspondence to histopathology after surgery (134–136). Extra “add-ons” to TRUS, like the elasticity of prostatic tissue, HistoscanningTM, or contrast-enhanced Doppler scanning, have been tested to identify prostate cancer but have never gained worldwide acceptance (137,138).
The use of TRUS and biopsies based on Prostatic Specific Antigen, PSA, and/or abnormal digital rectal examination (DRE) has diagnosed many with prostatic cancer, maybe too many, leading to over-diagnosis and over-treatment. However, over the last approximately eight years, a new technique, multiparametric or biparametric MRI of the prostate and image fusion with TRUS for biopsies for detecting and ruling out significant cancer has been used. The aim is to diagnose the significant cancers that need treatment or can be followed by active surveillance and not find all the insignificant cancers that might lead to over-treatment (139,140). The use of MRI to determine which men to biopsy should reduce the number of patients for immediate biopsies and thereby reduce the morbidity after biopsy and the costs for the community.
Contrast-Enhanced Ultrasound
Contrast-enhanced ultrasound (CEUS) has evolved tremendously over the last decades. In the 1960s, Gramiak and Shah first reported minute air bubbles as contrast enhancers of vascular anatomy (141). The discovery of the echo-enhancing and nonlinear properties of intravascular microbubbles initiated the development of more stable and safe ultrasound contrast agents along with dedicated contrast-enhancing scanner modes.
Initially, the contrast agents were produced as hand-agitated or sonication-generated microbubbles (142). However, the contrast agents were soon designed to meet several criteria such as surviving transpulmonary passage, being biologically inert and sustained over an adequately long period for diagnostic examinations, and having a small size distribution to avoid adverse effects on the microcirculation (143). The first commercially available ultrasound contrast agents, e.g., Levovist (Schering AG, Berlin, Germany) and Albunex (Molecular Biosystems Inc., San Diego, USA), consisted of air with a stabilizing shell. Due to high water solubility, they suffered from instability and circulated only shortly. The second-generation ultrasound contrast agents had the air replaced with inert gasses, such as the sulfur hexafluoride in SonoVue (Bracco Imaging, Milan, Italy) or the perflutren in Luminity (Lantheus Medical Imaging Inc, North Billerica, USA), which resulted in longer circulation time.
Another feature that improved with the introduction of more flexible lipid shells was the harmonic resonance capability. For contrast imaging, some researchers used the strong echo-scattering properties of the microbubbles to enhance Doppler signals (144–146). However, it was discovered that using the nonlinear properties of the microbubbles to create harmonic contrast-enhanced Doppler eliminated unwanted artifacts such as the flash or blooming artifacts (147). A general disadvantage of harmonic contrast-enhanced imaging is the harmonic signals produced by the tissue. Therefore, contrast-specific pulse transmission sequences, such as pulse inversion and amplitude modulation, were developed to exploit the nonlinear behavior of the microbubbles for contrast detection while at the same time removing the tissue signals (148,149). In addition, the new imaging sequences were designed with a low mechanical index to further promote microbubble survival as well as lower the risk of adverse biological effects from microbubble cavitation (150).
Clinically, CEUS has been used mainly in abdominal ultrasound and echocardiography. The dedicated contrast-enhancing imaging sequences with a lower mechanical index for contrast agent stabilization allowed real-time qualitative analysis of liver lesions (151–153). The enhancement patterns of liver lesions in the arterial, portal venous, and late phase can separate benign from malignant liver tumors, and today, this technique is a recommended examination for liver lesion assessment, also in children (Figures 5 and 6) (154–157).
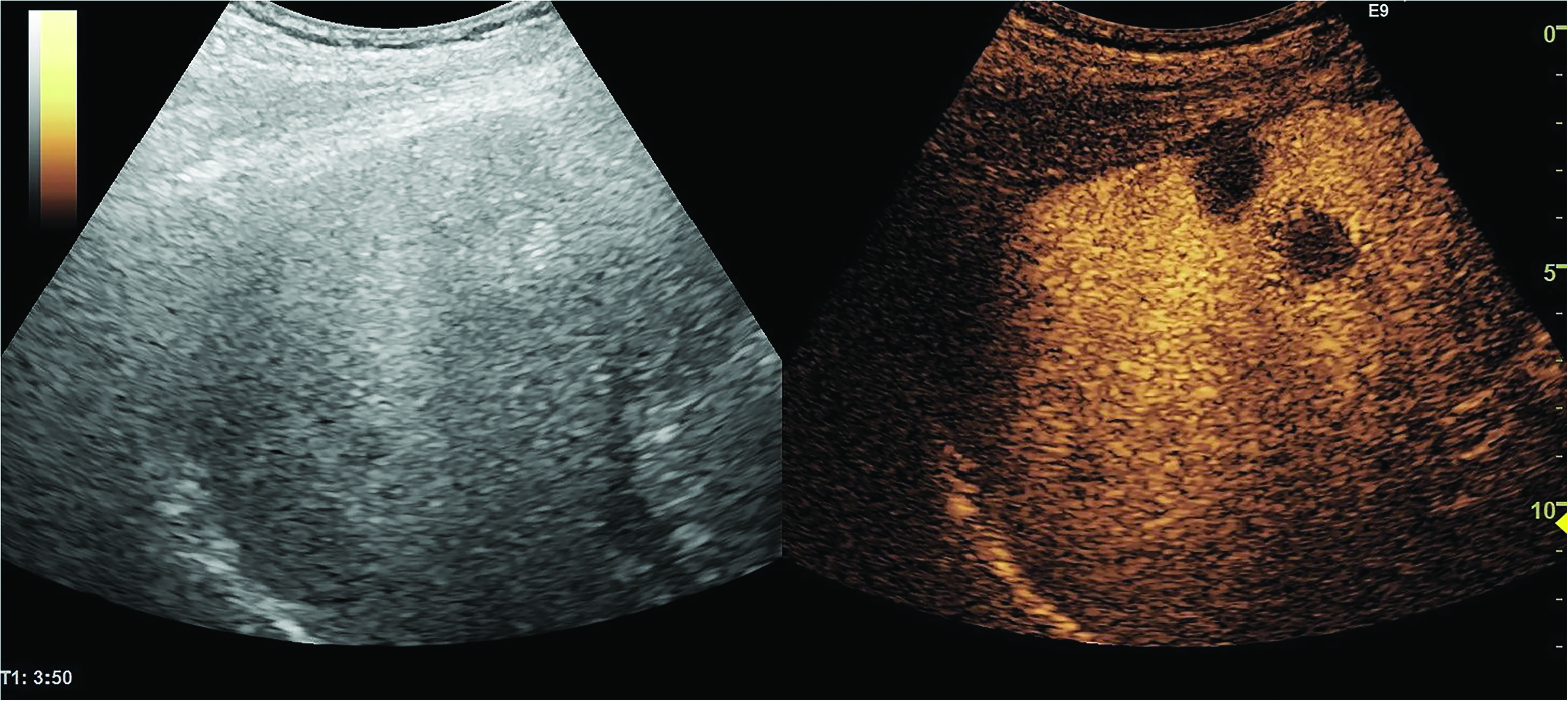
Liver metastases with contrast-enhanced ultrasound (right image).

A typical hemangioma with contrast-enhanced ultrasound (right image).
CEUS can complement conventional ultrasound in other ultrasound-guided percutaneous procedures such as abscess drainage with contrast injected intracavitary to guide the operator or in tumor biopsy procedures where contrast injected intravenously can prevent samples with necrotic material (158,159). Prior to ultrasound-guided liver tumor ablation, CEUS can complement CT and MR in the planning of the procedure but also in the evaluation of the treatment effect (160).
CEUS is also important for the detection of renal infarction, renal abscesses, graft dysfunction (161,162), and for follow-up after blunt trauma to solid organs in patients where CT is contraindicated, e.g., in children and pregnant women (163). The list of the potential clinical applications of CEUS is much longer than presented here, and it is still an attractive topic for research.
Quantification of tumor perfusion with CEUS has been widely investigated to improve lesion characterization and early assessment of cancer therapy response. Initially, semi-quantitative techniques were applied for evaluation of e.g., tumor response to anti-angiogenic treatment for renal cell carcinoma, where the percentage of perfused tumor tissue indicated treatment response, and focal liver lesions, where sonography videotape intensities characterized the tumors (164,165). More advanced quantification strategies with parameters extracted from the time-intensity curves of contrast wash-in and wash-out were subsequently introduced (166,167). However, the quantitative parameters are subject to considerable variations caused by factors such as scanner settings, microbubble type, handling, and administration, or physiological variations as reviewed by Tang et al. and summed in the European guidelines for quantitative CEUS (168,169). Therefore, evaluation of the reproducibility of the quantitative outcomes is crucial to consider in the planning of future clinical studies (170,171).
Recent developments in CEUS
Microbubbles loaded with therapeutic compounds can be used for targeted gene and drug delivery, where high-power ultrasound waves are used to disrupt the loaded microbubbles in specific regions of interest (172,173). Functionalized microbubbles with ligands targeted for specific disease biomarkers can be used for molecular imaging beyond the vasculature (174,175). For both of the techniques above, nano-sized bubbles are also being developed, allowing permeability and retention of the bubbles in the targeted tissues (176). Lastly, inspired by super-resolution fluorescence microscopy, ultrasound super-resolution imaging utilizes diluted microbubbles as single and separable ultrasound scatterers (177,178). Mapping structures smaller than the diffraction limit is possible by localizing and tracking the single microbubbles over thousands of image frames. Combining all the microbubble tracks into one image results in a map of the microvascular network. In addition, the estimation of the microbubble velocity has the potential to give new insights into microvascular flow dynamics. Super-resolved images of animal organs such as the brain and the kidney underline the big potential of ultrasound super-resolution imaging (110,177,179).
Elastography
Ultrasound elastography is one of the latest additions to the spectrum of ultrasound imaging techniques (180). Two main types of ultrasound elastography are currently used: strain elastography and shear-wave elastography. Common to all elastography methods is that they assess the stiffness of tissue. To some degree, tissue stiffness correlates with pathology and this feature can be used for discerning malignant focal lesions from benign ones, as in tumor classification, and for grading the severity of certain non-focal diseases, such as liver fibrosis (181).
The first elastography method to become clinically available was strain elastography, published in 1991 by Ophir et al. (182). Using slight repetitive compression with the transducer on the skin of the patient, cross-correlation functions could now be used to find matching segments of radiofrequency (RF) waveforms on pre- and post-compression data (183). The relative displacements of matching waveforms between pre- and post-compression data could be used to make images of tissue strain, which is a tissue characteristic, inversely proportional to tissue stiffness, i.e., soft tissue has large strain, and hard tissue has little strain (184). Two-dimensional strain images could now be displayed and are known as strain elastograms.
Among the first publications on strain elastography, greyscale strain elastograms were displayed alongside the B-mode image (185). Soon, color elastograms became widely available, allowing for elastograms to be superimposed on the B-mode images for easy qualitative correlation. The earliest studies of strain elastography focused on focal lesions in breast and thyroid glands, which are still some of the most used applications of strain elastography. In 2006, Itoh et al. proposed a visual scoring system for stratifying breast tumors according to their appearance on color strain elastograms, which was and is widely used for breast cancer diagnosis (186). Semi-quantifications of tumor strain using either tumor-to-normal-tissue strain-ratios or strain-to-B-mode tumor diameter ratios have also been widely applied (187–189).
The second elastography method which has gained widespread clinical use is shear-wave elastography (190). In contrast to strain elastography, shear-wave elastography yields direct measurements of shear-wave speed. The method uses an acoustic push-pulse to excite the tissue yielding shear-waves that propagate perpendicular to the direction of the pulse itself. Assuming a tissue density of 1 g/cm3 for soft tissues, shear-wave speed is proportional to the square root of tissue elasticity (Young's modulus). Building on early works examining acoustic radiation force impulse (ARFI) methods for strain image acquisition, Bercoff et al. published the first study on clinical SWE in 2004 (190–192). Early shear-wave elastography methods measured shear-wave speed inside an elastography box placed by the operator, while newer methods can depict a color-coded elasticity map of either the entire region observed with B-mode ultrasound or a larger elastogram box within it. Shear-wave elastography measurements can either be reported as an average tumor stiffness or as a maximal tumor stiffness in (m/s) or tissue elasticity (kPa) and color shear-wave elastograms can be displayed on a color scale similar to strain elastograms (193).
Owing to the widespread availability and ease of use of ultrasound elastography it has been extensively investigated as an adjunct to B-mode ultrasound in many diagnostic subspecialties. Clinical guidelines are available from international ultrasound societies, which have focused on the use of elastography for breast and thyroid nodule evaluation, liver stiffness measurements, and prostate biopsy targeting (180,181,194,195).
In breast cancer diagnosis, elastography guidelines suggest that both strain- and shear-wave elastography have high accuracy and may increase diagnostic confidence and elastography has been added to the latest edition of the ultrasound BI-RADS atlas (194,196). Many studies have suggested the use of elastography to either downgrade BI-RADS 4a tumors, to follow-up examinations instead of an immediate biopsy, or to upgrade BI-RADS 3 tumors for immediate biopsy (197). There is no clear evidence on which elastography method should be preferred, but some data suggest that while strain elastography is prone to a higher degree of observer variability than shear-wave elastography, shear-wave elastography may on the other hand yield false-negative results in very stiff tumors, which have shear-wave speed beyond the measurable range (198). Several studies have also shown the feasibility of elastography to assess reliably cystic breast lesions (187).
In thyroid nodule evaluation, elastography has been used to increase diagnostic performance and for biopsy targeting (199). There are no certain differences in the diagnostic gains between the two methods, but it has been reported for both strain and shear-wave elastography that non-papillary thyroid carcinomas may appear soft, leading to false-negative results (200). Additionally, elastography can be challenging in large focal lesions with little reference tissue available, in nodules located in the isthmus, and in irregular or very calcified nodules.
In liver elastography, mainly shear-wave elastography has been applied and has been shown to reduce the number of liver biopsies when elastography findings are in accordance with other clinical findings (201). The most studied field of liver elastography is in chronic viral hepatitis, while the evidence is heavily dependent on the elastography method used for other etiologies (202). In addition, obesity and ascites are a major limitation to all shear-wave methods applied (203).
In recent years, many clinical studies of ultrasound elastography have focused on the prognostication and treatment response evaluation in different soft tissue tumors (204). In some studies, a correlation between breast tumor stiffness and receptor status, histological grade, and Ki-67 expression has been reported, suggesting that tumor evaluation using elastography could in future venture beyond determining whether tumors are malignant or benign (205). To this end, 3D elastography has recently become clinically available, facilitating whole tumor evaluation, which could also pave the way for more accurate tumor classifications (206).
Conclusion
Ultrasound equipment is now available in any size and for any purpose, ranging from handheld devices to high-end devices (207). The scientific societies include ultrasound professionals from all disciplines publishing guidelines and recommendations (200,208). Interventional ultrasound is expanding the field of use of US-guided interventions into nearly all specialties of medicine, from US guidance in minimally invasive robotic procedures (209) to simple US-guided punctures performed by general practitioners (210). Each medical specialty is urged to define minimum requirements for equipment, education, training, and maintenance of skills, also for medical students (158,211,212). The clinical application of CEUS and elastography is a topic often seen in current research settings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.