
Abstract
Background
Contrast-enhanced spectral mammography (CESM) may help to determine the malignancy potential of lesions according to the degree of enhancement.
Purpose
To investigate the correlation between the degree of contrast enhancement of the lesions in contrast-enhanced spectral mammography (CESM) and the final histopathological diagnosis in patients with BI-RADS 4 and 5 lesions.
Material and Methods
CESM was performed in 128 patients who had BI-RADS 4 and 5 lesions on mammography and underwent histopathological examination. A total of 128 index lesions were scored using a 4-point scale regarding the degree of contrast enhancement (0 = no contrast enhancement, 1 = minimal, 2 = moderate, 3 = marked), a score of 2 and 3 was accepted as suggestive of malignancy. The study was approved in our institutional scientific committee.
Results
In total, 76 (59.4%) of the lesions had benign histopathological results, whereas 52 of them had malignant results. Contrast enhancement was not observed in 22.7% of the lesions while 24.2% had minimal enhancement, 18.8% had moderate enhancement, and 34.4% had marked enhancement in CESM. The sensitivity of the degree of contrast enhancement in CESM was 98.1%, when the specificity was 77.6%, positive predictive value was 75%, negative predictive value was 98.3%, and accuracy was 85.9%.
Conclusion
This study demonstrated that the degree of contrast enhancement of the lesions in CESM may be used in daily practice with easily performing a visual scale in predicting the malignancy potential of the lesions.
Introduction
Mammography as the standard imaging technique of the breast often needs advanced imaging modalities to increase diagnostic sensitivity especially in patients with dense breast. Subsequent breast ultrasound and dynamic contrast-enhanced (DCE) magnetic resonance imaging (MRI) is the classic pathway in routine practice providing more detailed detection and characterization of the lesions. However, those modalities have their own limitations (1,2). Contrast-enhanced spectral mammography (CESM) is a recently emerged technique for this purpose. The use of CESM has increased since it is an easy modality to access, perform, and interpret, and is also cost-effective when compared to MRI. CESM has an advantage over mammography when demonstrating the structural pattern of the breast parenchyma as well as mass and non-mass lesions and microcalcifications in low-dose images. Although the present dual-energy CESM technique does not provide dynamic imaging, it exhibits the contrast uptake of breast lesions in high-dose subtracted images. Therefore, the diagnostic performance of CESM is nearly equal when compared with MRI including dynamic sequences regarding sensitivity and it has even a higher specificity (3–5). Furthermore, previous studies performing the temporal-dynamic technique have shown that the high accuracy of CESM resulting from its nature of demonstrating contrast uptake and kinetic curves did not correlate with MRI curves (6). However, there are limited studies in the literature investigating the degree of contrast enhancement of the breast lesions in CESM examination (7). The aim of the present study was to evaluate the association between the degree of contrast enhancement and the final diagnosis of the lesions with CESM in patients with ACR BI-RADS 4 and 5 lesions (8).
Material and Methods
Study patients
A total of 128 patients who had ACR BI-RADS 4 and 5 lesions in mammography and underwent CESM, between November 2014 and May 2019 were selected. Index lesions were evaluated, and all 128 lesions had subsequent histopathological examination with core biopsy. Patients with breast implants, previous breast surgery, receipt of radiation, or neoadjuvant chemotherapy for breast malignancy were not included in the study. The approval was given by the institutional scientific committee for this retrospective study with a waiver of patient informed consent.
Mammography
Full-field digital mammography was performed with Senographe DS (GE Healthcare ), with at least two standard views in the craniocaudal (CC) and mediolateral oblique (MLO) views as part of the routine clinical workup.
CESM
CESM was performed using a prototype of a full-field digital mammography unit derived from a Senographe DS (GE Healthcare) that was modified to allow dual-energy exposures.
When patients were in a comfortable position, the contrast material (300 mg iodine/mL, 1.5 mL/kg, Xenetix® 300, Guerbet, France) was injected intravenously via an automated injector with a flow rate of 2 mL/s. After 2 min from the start of injection, the images were obtained by a dedicated software program that generates the low- and high-energy images. Low-energy images were acquired at peak kilovoltage (kVp) values in the range of 26–31 kVp while high-energy images were acquired with peak kVp values in the range of 45–49 kVP. Filter, kVp, and mAs were automatically selected by the device based on breast thickness. We first performed the CC projection of the lesion side unless the lesion was better demonstrated in the MLO projection. The CC projection of the other side and MLO projections of the lesion and contralateral breast were subsequently acquired. Examination of both breasts was completed within approximately 5 min. Late images were obtained at the 7 min for suspicious lesions. The subtracted images were produced by the software program that deletes the background parenchymal structures and non-enhancing lesions.
Image interpretation
Anonymized images were sent to a dedicated mammography workstation (Seno Iris; GE Healthcare) for CESM cases. All images were reviewed by two experienced breast radiologists in consensus (Radiologist A, with 16 years of breast imaging experience, and Radiologist B, with 14 years of breast imaging experience). The radiologists were blinded to the clinical findings and previous reports of the patients, but they were aware that the study included only patients with a suspicion of breast cancer. They were asked to give a score to the index lesion according only to the degree of contrast enhancement using a visual scale of 0–3 (0 = no contrast enhancement, 1 = minimal, 2 = moderate, 3 = marked). The scores of 0 and 1 were accepted as suggestive of benignity and the scores of 2 and 3 were accepted as suggestive of malignancy (Figs. 1–4). Morphologic criteria of the lesions were not included in scoring system. Images were evaluated in four independent viewing sessions. Images and histopathology were cross-referenced by the corresponding author after all sessions were completed. Invasive ductal carcinoma (IDC), invasive lobular carcinoma (ILC), and ductal carcinoma in situ (DCIS) were considered malignant lesions. Benign and premalignant lesions (e.g. atypical ductal hyperplasia) were defined as non-malignant lesions.
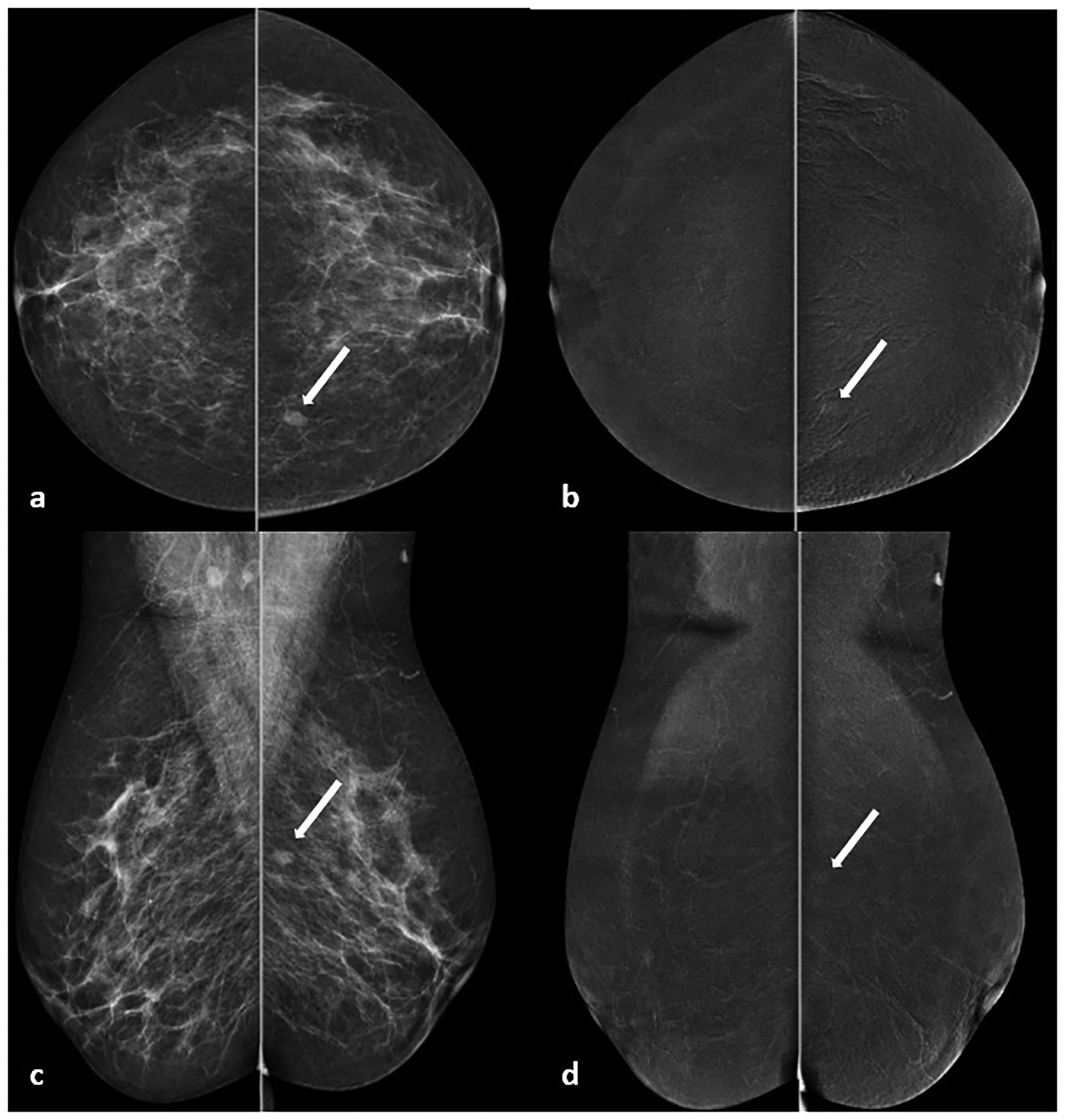
Example of a 42-year-old high-risk patient. On CESM imaging, (a, b) low dose images show an oval mass with a diameter of 8 mm in the upper inner quadrant of the left breast, (c, d) subtracted images show minimal contrast enhancement in the lesion. The lesion was scored as “1” and confirmed by histopathology as adenosis-fibrosis. CESM, contrast-enhanced spectral mammography.
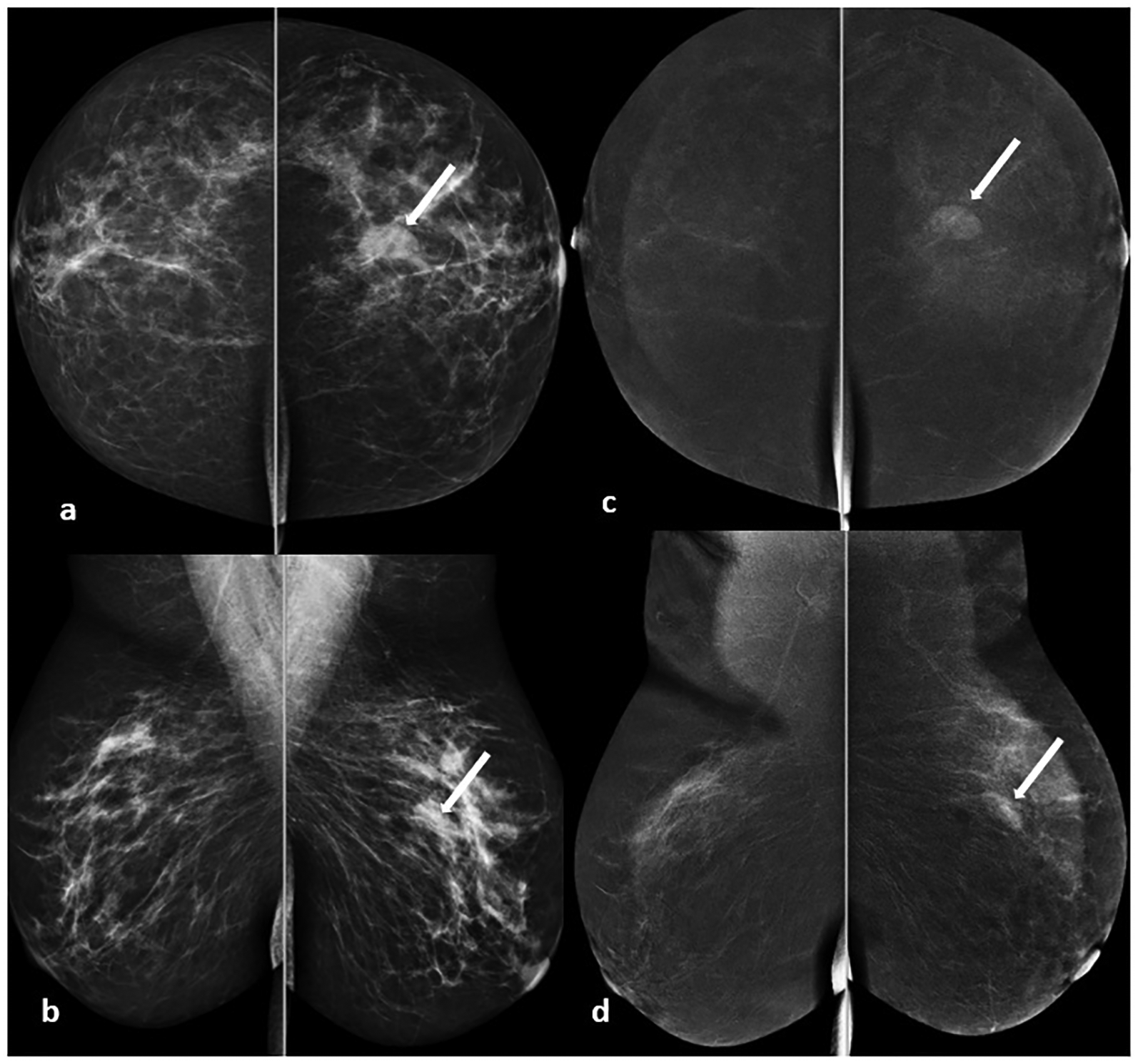
Example of a 55-year-old woman with pain in her left breast. On CESM imaging, (a, b) low dose images show an oval mass with indistinct margins and a diameter of 15 mm in the upper outer quadrant of the left breast, (c, d) subtracted images show moderate contrast enhancement in the lesion. The lesion was scored as ‘2’, but the histopathological diagnosis was fibroadenoma. CESM, contrast-enhanced spectral mammography.
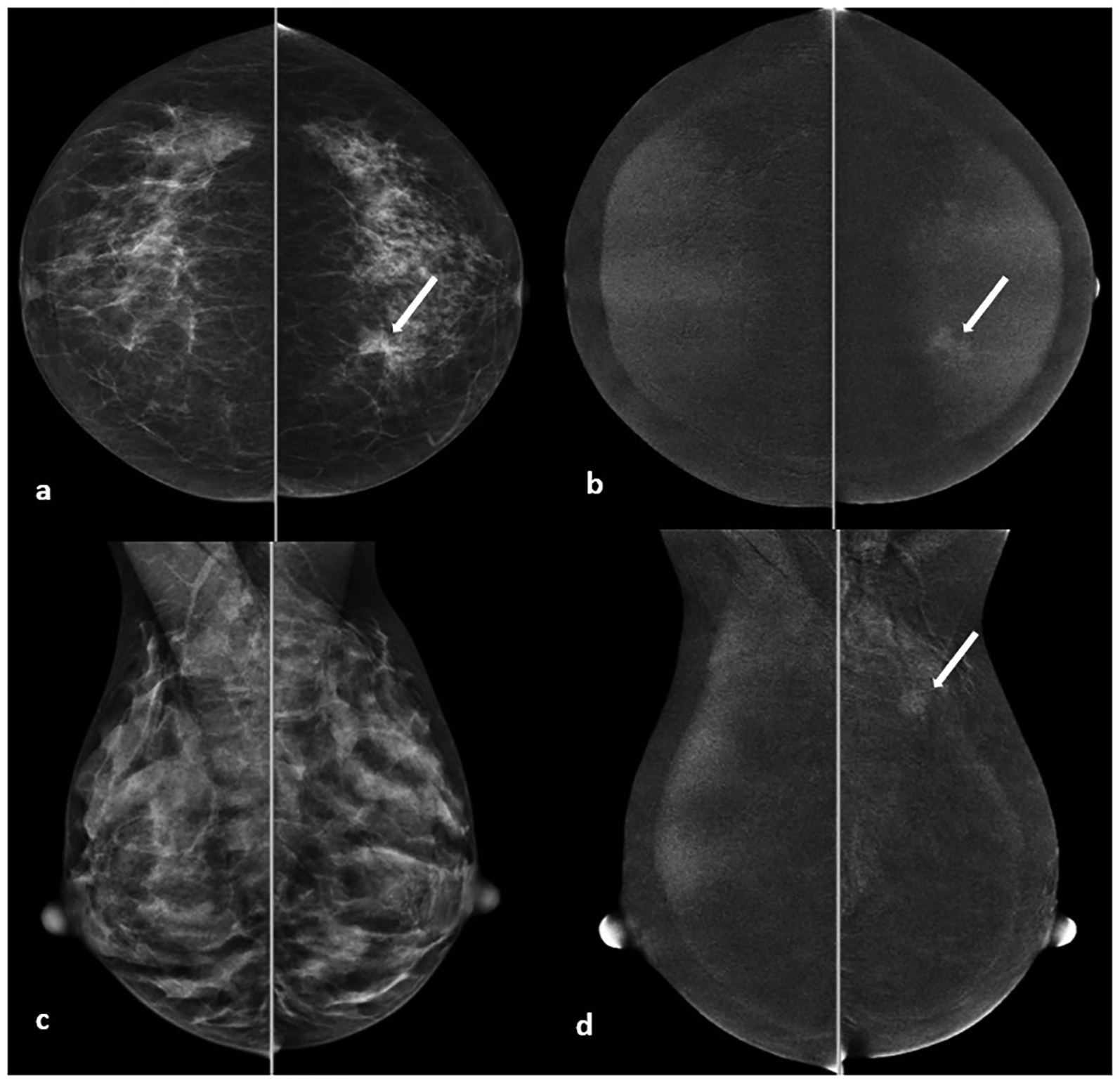
Example of a 52-year-old woman with dense breast parenchyma. In CESM imaging, (a) low dose craniocaudal image shows architectural distortion (arrow) in the left breast, with no apparent finding in (b) mediolateral oblique projection; (c, d) subtracted images demonstrate an associating irregular mass lesion with moderate contrast enhancement. The lesion was scored as “2” and confirmed by histopathology as ductal carcinoma in situ. CESM, contrast-enhanced spectral mammography.
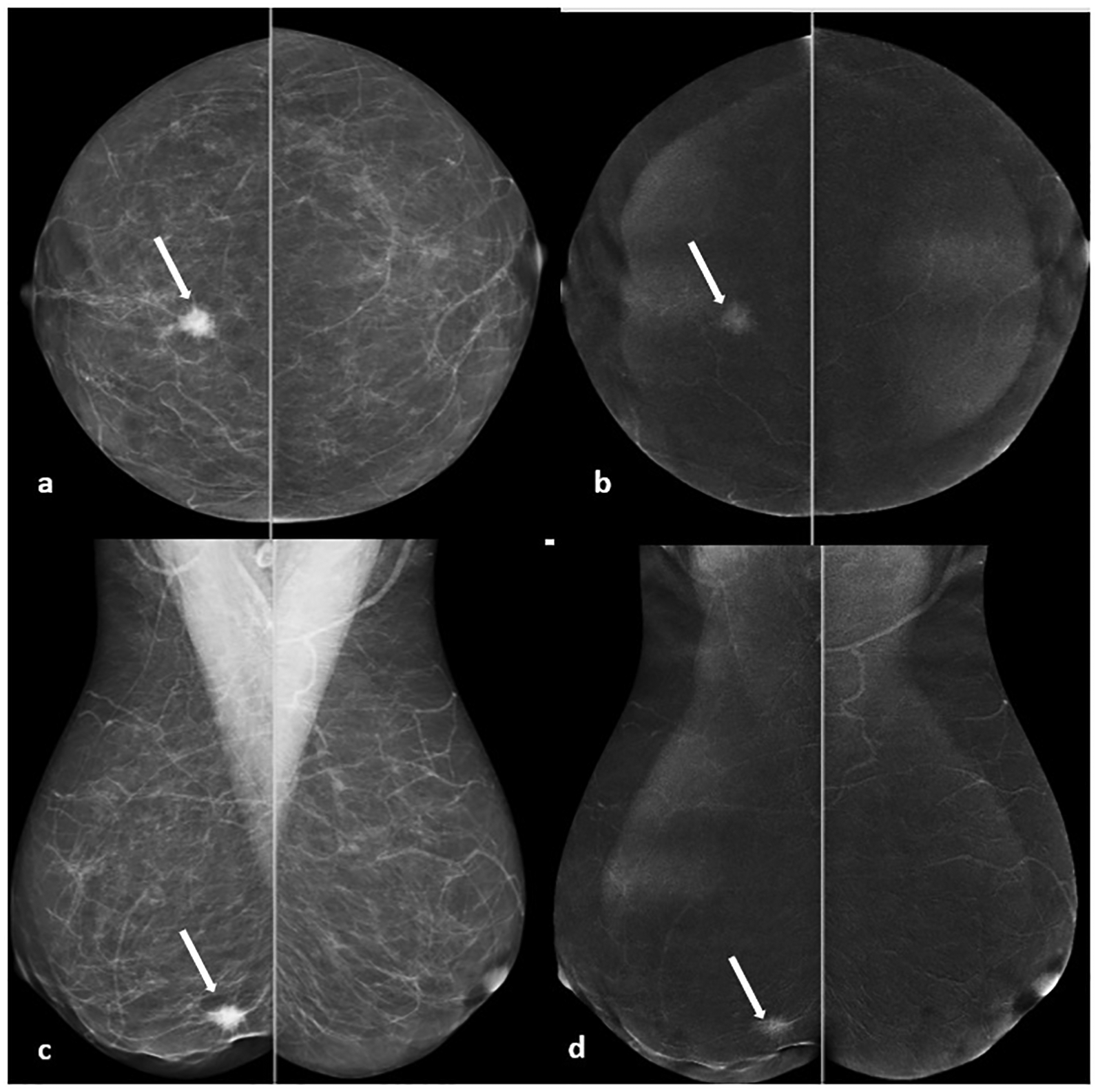
Example of a 60-year-old woman with a right breast lump. On CESM imaging, (a, b) low dose images show a spiculated mass lesion with a diameter of 12 mm in the right breast; (c, d) marked enhancement was observed in the subtracted images. The lesion was scored as “3” and confirmed by histopathology as invasive ductal carcinoma. CESM, contrast-enhanced spectral mammography.
Statistical analysis
All statistical analyses were performed using the IBM SPSS Statistics 22.
Shapiro–Wilk test was used for the convenience of normal distribution of the parameters. Sensitivity, specificity, positive predictive value (PPV, and negative predictive value (NPV) in the diagnosis of index cancer were calculated. A true-positive diagnosis was defined as a histopathologically confirmed breast cancer that was scored by the radiologists as 2 or 3 and a true-negative diagnosis was defined as histopathologically confirmed lack of breast cancer that was rated by a radiologist as 0 or 1. McNemar’s test was used to estimate the accordance between histopathological results and CESM score. All P values were two-sided, and P < 0.05 was considered to indicate a statistically significant difference.
Results
Lesion analysis
According to mammography images, morphologic characteristics of the lesions were as follows: 80 masses (34/80 were with spiculated and 46/80 were with indistinct or obscured margins), 18 asymmetries, four parenchymal distortions, and 26 microcalcifications with suspicious morphology. Associated features defined by ACR BI-RADS were seen in 24 of the patients.
Histopathological outcome
Histopathological analysis showed that 76 of the lesions were benign (76/128, 59.4%) and 52 of the lesions were malignant (52/128, 40.6%). Subtypes of the benign lesions were as follows: adenosis, fibroadenoma, fibrocystic changes, intraductal papilloma, granulomatous mastitis, chronic inflammatory changes, fat necrosis, inflammatory fibrosis, and apocrine metaplasia. Malignant lesions were detected as DCIS, IDC, ILC, IDC and ILC, medullary carcinoma accompanied with IDC, and mucinous carcinoma. Histopathological subtypes of the lesions are shown in Table 1.
Results for CESM and histopathological analysis.
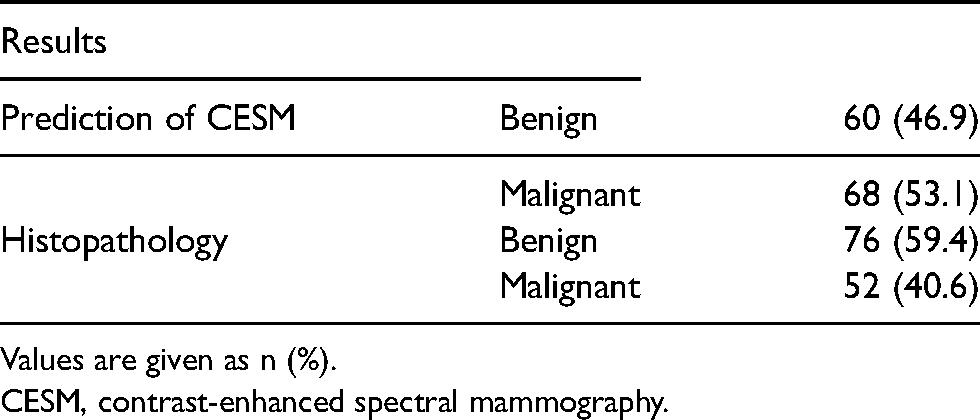
Values are given as n (%).
CESM, contrast-enhanced spectral mammography.
H
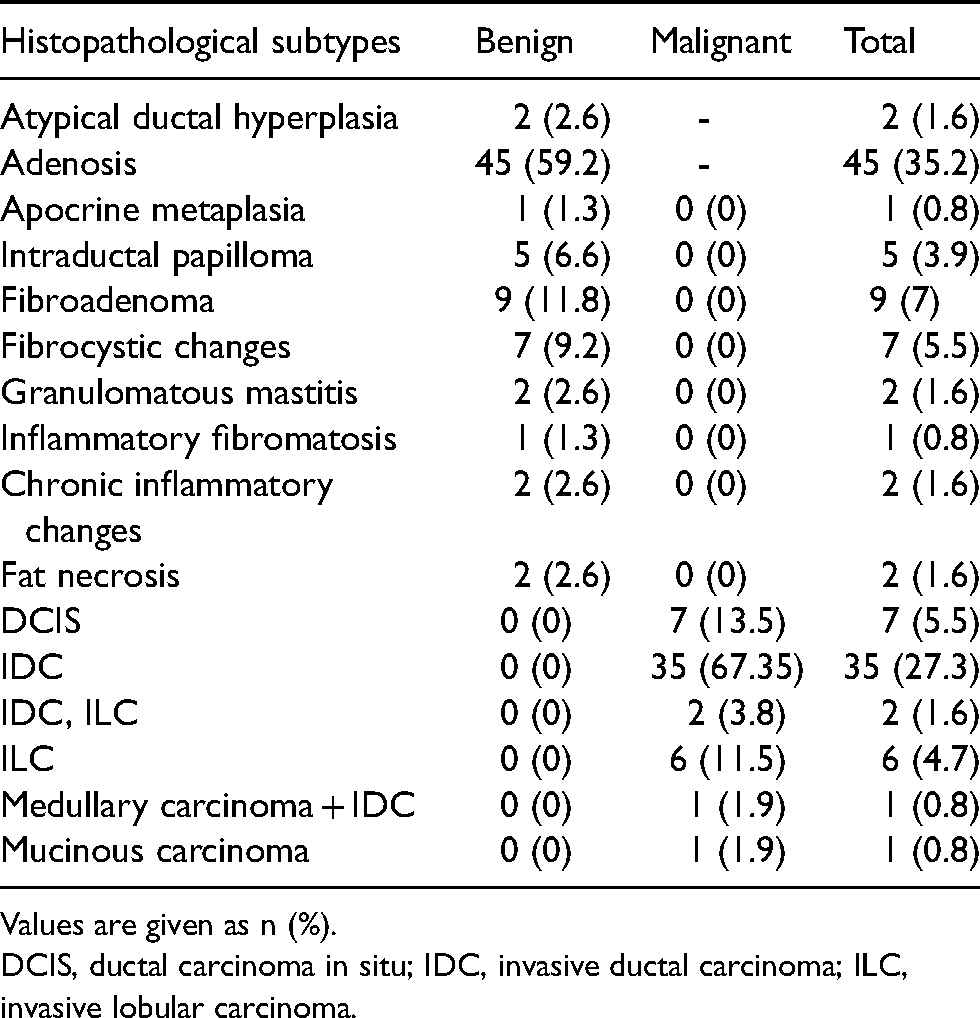
Values are given as n (%).
DCIS, ductal carcinoma in situ; IDC, invasive ductal carcinoma; ILC, invasive lobular carcinoma.
The age range of the patients was 32–80 years (mean age = 52 ± 11 years). The mean age of the patients was significantly lower in benign lesions (49.5 ± 10 years) than in malignant lesions (55.4 ± 12 years; P = 0004; P < 0.05).
CESM results
No contrast enhancement was seen in 22.7% of the lesions; 24.2% of the lesions had minimal enhancement, 18.8% had moderate enhancement, and 34.4% had marked enhancement in CESM (Table 1). Therefore, CESM scored 46.9% of the lesions as suggestive of benign and 53.1% of the lesions as suggestive of malignant. The sensitivity of the degree of contrast enhancement in CESM was 98.1% (51/52), when the specificity was 77.6% (59/76), PPV was 75% (51/68), NPV was 98.3% (59/60), and accuracy was 85.9% (110/128). Seventeen lesions scored as malignant in CESM finally had benign histopathological results. These lesions were fibroadenoma (5), adenosis (4), granulomatous mastitis (2), fat necrosis (2), atypical ductal hyperplasia (1), chronic inflammatory changes (1), inflammatory fibromatosis (1), intraductal papilloma with atypia (1). Morphologic characteristics of these lesions were masses in 10 cases (three cases with indistinct margins, three cases with obscured margins, and four cases with microlobulated margins), asymmetries in three cases, microcalcification in two cases, and architectural distortion in two cases. One of the seven DCIS lesions was scored as benign in CESM (the score was 1 for that lesion), which was exhibiting as asymmetry in mammography.
No major contrast reactions were observed after CESM examination. Four patients had minor reactions: two with flushing and dizziness, one with nausea, and one with mild hypertension. However, these reactions were self-limited and needed no more medical treatment.
Discussion
Our results demonstrated that scoring of the lesions according to degree of contrast enhancement in CESM can show the malignancy potential of the lesions with a high sensitivity (98.1%, 51/52). Morphologic criteria were not included in scoring system since we basically aimed to show the relationship between the degree of contrast enhancement of lesions and histopathological results. A relatively high number of DCIS cases could be a disadvantage for the study results since DCIS may be missed in contrast-enhanced studies (3,4). In this regard, one case leading to a decrease in sensitivity was a DCIS lesion that showed minimal enhancement and was scored as 1 in the subtracted images. This lesion was expressing as focal asymmetry, whereas other DCIS lesions expressing with mass lesion, asymmetry, or microcalcification were scored as malignant in CESM according to their contrast enhancement degrees. In addition, high NPVs (98.3%) in this study may be interpreted as breast lesions that had no or minimal contrast enhancement in CESM are highly associated with benign processes, since the degree of contrast enhancement was weak in benign lesions, whereas it was considerably more intense in malignant lesions. This also supports that evaluation of degree of contrast enhancement may be useful in CESM, independently from the morphology of the lesions.
Increased vascularization is a characteristic feature of malignant breast lesions. It is also an independent prognostic factor regarding patient survey (9). Studies with contrast-enhanced examinations showed that malignant tumors usually have rapid and strong contrast uptake and accelerated extravasation whereas benign lesions tend to have minimal or no contrast uptake (10–12). In recent decades, MRI has been the only established contrast-enhanced method in this regard with a highest sensitivity among other breast imaging modalities (13). However, it has well-known limitations such as low specificity, high cost and, limited accessibility. CESM is a recently emerged contrast-enhanced technique, used to increase the diagnostic sensitivity for detecting breast cancer, especially in patients with dense parenchyma. CESM has the advantage of matching the morphological information provided by mammography with the knowledge of contrast enhancement as it increases the contrast between the vascular tumors and background parenchyma. In this respect, our study is also consistent with the literature that CESM can show malignancy with a high sensitivity (3,4,14,15).
Seventeen lesions were commented as suggestive of malignancy in our study, which were scored as 2 (moderate) or 3 (marked) and had benign histopathological findings. The morphologic characteristics of these lesions were mass lesions in 10 cases with indistinct, obscured, or microlobulated margins: asymmetries in three cases; microcalcifications in two cases (pleomorphic type in one case diagnosed as atypical ductal hyperplasia and coarse heterogeneous type in one case diagnosed with adenosis histopathologically); and architectural distortion in two cases. Therefore, our specificity and PPVs (77.6% and 75%, respectively) were lower than some studies in the literature (4,16). However, the specificity level in our study was higher than the pooled level of this parameter, which was reported as 66% in a recent meta-analysis (17). This result shows that CESM may not surpass the disadvantages of MRI in some inflammatory or fibroproliferative processes that show an increased uptake of contrast agents and mimic the malignancy.
Previous CESM studies, performing the temporal subtraction method, showed that the superiority of CESM compared to mammography resulted only from contrast enhancement of the lesions but there was no effect of contrast uptake-time relation (6). Deng et al. reported that the malignant lesions significantly have stronger enhancement than benign lesions on CESM (7). They used a semi-automated segmentation program to measure the degree of enhancement of the lesions (area under the curve [AUC] = 0.877; 95% confidence interval [CI] = 0.813–0.941); however, they only evaluated the relative enhancement of the lesions between early (2–3 min) and late (4–6 min) phases. However, we believe that further studies with new software technologies measuring the contrast density of the lesions should be conducted. We did not perform a quantitative measurement, since the aim of this study was to show the simplicity of the interpretation of CESM images, which apparently shows the difference in contrast uptake mechanism between benign and malignant lesions. CESM is an easier modality to perform and interpret and has a low cost when compared to MRI. Despite all the advantages, there are still doubts about CESM regarding its routine clinical use and interpretation in some centers. This study demonstrates that a simple visual scale used in the interpretation of CESM can reliably distinguish malignant tumors from the benign lesions.
The present study has some limitations. First, we scored lesions only with their contrast enhancement, since the aim of the study was to show the relation of malignancy potential of the lesions with the degree of enhancement, independently from morphologic criteria. However, high sensitivity and NPV show that CESM is a valuable method to demonstrate breast cancer even without the evaluation of morphologic criteria. Further, the addition of morphologic characteristics may not increase our PPV, since we included only suspicious lesions in this study. Second, we did not consider the background parenchymal enhancement separately. However, the degree of contrast enhancement we used in the visual scale was relative to background enhancement in every case. Third, we could not perform a quantitative measurement to categorize the lesions.
In conclusion, a visual scale may be used as a practical method to predict the malignancy potential of the suspicious lesions in routine clinical practice of CESM.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.