
Abstract
Focal renal lesions in the background of chronic kidney disease (CKD) present a diagnostic challenge. Contrast administration is usually avoided in such a setting, undermining the usefulness of computed tomography and magnetic resonance imaging. Focal regenerating nodules may occur in the background of CKD and closely mimic renal neoplasms. The aim of the present article was to highlight the salient manifestations of such CKD pseudotumors on different imaging modalities and also to depict the differentiating features from malignancy. Radiologists must be aware of the imaging appearance of this uncommonly talked about entity so as to avoid inadvertent surgery or cause undue anxiety to the patient.
Keywords
Introduction
The incidence of benign pathological findings at surgery for suspected malignant renal mass remains high (1). Certain lesions may mimic tumors on imaging but are histologically composed of normal or benign renal tissue. Such pseudo-mass lesions are termed renal pseudotumors and may be developmental, infectious, granulomatous, or vascular in etiology. Some of these may represent nodular hypertrophy in a background of end-stage renal disease (ESRD) (2). Especially noteworthy are normal variants like the hypertrophied column of Bertin, dromedary hump, and persistent fetal lobulations. Some of these pseudotumors may be diagnosed confidently on imaging, but few are resected or subjected to repeated biopsies because of the concern about malignancy and lack of diagnostic certainty. The prevalence of chronic kidney disease (CKD) is rising globally, more so in high-income countries, attributed to increasing life expectancy and lifestyle diseases (3).
Contentious issues and possible solutions
Abdominal imaging in patients with renal dysfunction poses a diagnostic problem because administration of both iodinated computed tomography (CT) contrast as well as gadolinium-based magnetic resonance imaging (MRI) contrast is not desirable. The former may result in contrast-induced nephropathy while the latter may lead to nephrogenic systemic fibrosis (4, 5).
Sonography is an important preliminary investigation in the evaluation of focal renal lesions; however, further evaluation using contrast-enhanced CT (CECT) or MRI is frequently required. Contrast administration is thus vital and demonstration of enhancing solid components in the absence of macroscopic fat is the imaging criterion for diagnosing renal malignancy (6, 7). Thus, characterization of renal lesions in patients with renal dysfunction is a diagnostic challenge. Diffusion-weighted imaging (DWI) is a useful MRI technique for renal lesion evaluation based on measuring Brownian motion of free water molecules in different tissues, without employing contrast (8–11). Contrast-enhanced ultrasound is another useful paradigm that enables assessment of contrast dynamics without any risk of nephrotoxicity.
Pseudotumors and renal cell carcinoma: a diagnostic conundrum
Patients with ESRD are at an increased risk for the development of cysts and renal cell carcinomas (RCCs) (12, 13). However, these patients also have another unique problem. Because of non-uniform parenchymal atrophy and compensatory focal nodular hypertrophy, the latter may be misinterpreted as a neoplastic mass (14). Such pseudolesions are commonly misdiagnosed as malignancy because they appear as ball-type lesions producing contour abnormalities or mass effect on the pelvicalyceal system (PCS) (Fig. 1) (14, 15). These kidneys are usually irregular in contour, contracted in appearance, and have increased echogenicity on sonography with loss of corticomedullary (CM) differentiation (16). Thus, it becomes difficult to detect and recognize the benign nature of these pseudotumors in the background heterogeneity. Differentiation of these lesions from RCC is even more difficult since these are solid enhancing lesions and the normal CM differentiation is already lost in these kidneys.

Mass-like appearance of CKD pseudotumors. (a) Axial NCCT image reveals multiple ball-type isodense lesions in both kidneys (*). (b–d) The corresponding T2W FS MRI images (axial (b, c) and coronal (d)) of the same patient show hyperintense signal intensity of the masses. Both the kidneys appear small, contracted, and shrunken. (e) Sagittal NCCT image in a different patient shows large hypodense mass in upper pole of right kidney. (f, g) The gray-scale and (h) color Doppler images of the right kidney (same patient as (e)) denote the solid echogenic morphology of the mass (*). No splaying or distortion of the traversing vessels is seen (*). Biopsy confirmed the diagnosis. CKD, chronic kidney disease; FS, fat-suppressed; MRI, magnetic resonance imaging; NCCT, non-contrast computed tomography; T2W, T2-weighted.
Clinically, the CKD pseudotumors are usually silent. However, they are usually detected while imaging these patients for non-specific complaints (such as pain in the abdomen, symptoms related to urinary tract infection) or as part of CKD evaluation.
Objectives
There is a severe paucity of literature regarding the imaging appearance of renal pseudotumors in the background of CKD. The aim of the present review was to illustrate the appearance of these lesions on ultrasonography (US), CEUS, CT, MRI, and DWI, and to highlight the differentiating features from RCC. Radiologists, nephrologists, and surgeons must be aware of the imaging appearance of these pseudotumors so as to avoid inadvertent surgery, which may deprive the patient of precious remaining functional parenchyma.
Pathogenesis and background
Parenchymal insults to the kidney can be varied in the form of surgical, traumatic, vascular, or infective (14, 17). After the resultant loss of the nephrons in the renal parenchyma, the spared tissue can undergo compensatory hyperplasia and hypertrophy. The renal parenchymal loss may be patchy depending on the underlying etiology of chronic renal parenchymal disease. This gives rise to mass-like areas of relatively preserved renal parenchyma giving the appearance of tumor, thus called pseudotumor (14).
These pseudotumors may occur in kidneys that are scarred and deformed by chronic pyelonephritis, glomerulonephritis, trauma, or infarction (14, 17–22). Chronic pyelonephritis involves the kidney in a patchy distribution, resulting in irregular indented cortical outline with focal scarring and skip areas (18, 20, 21). Chronic glomerulonephritis usually involves the kidneys in a uniform distribution, resulting in smooth cortical outlines and diffuse cortical atrophy (18, 20). However, it may develop in segmental distribution sparing the intervening segments, which may masquerade as neoplasms (18, 20). Diabetes and hypertension lead to patchy atrophy (resulting from glomerular and arteriolar lesions) leading to non-uniform attenuation of renal parenchyma (23, 24).
Initial case reports of this entity date back to 1968, which describe its intravenous urography (IVU) and angiographic appearance (18). IVU may show an exophytic soft-tissue mass causing distortion or splaying of the PCS (14). The corresponding area reveals enlarged vessels with parenchymal blush on angiography raising the suspicion of a tumor (18). CKD pseudotumors are uncommon and their description in literature is limited to case reports and series; thus, the exact prevalence is difficult to ascertain (14–22).
Imaging appearance
Gray-scale US and Doppler
The kidneys affected by chronic parenchymal disease are usually irregular in contour, small and contracted in appearance, and have increased echogenicity on sonography (16). The renal echotexture is heterogeneous with attenuation or loss of CM differentiation. In addition, because of non-uniform parenchymal atrophy, the kidneys appear lobulated. Both RCC and pseudotumors appear as ball-type solid lesions producing contour abnormalities or mass effect on the PCS (14, 15).
The pseudotumors are usually multiple and bilateral though they may be unifocal as well. They are usually isoechoic/mildly hyperechoic compared to the surrounding parenchyma. They can have variable echogenicity and especially mimic neoplasms when their echogenicity is different from the surrounding parenchyma. CM differentiation is usually not apparent either within the lesion or in the surrounding parenchyma. The lesions are usually homogeneous with absence of necrosis or calcification. The most common renal neoplasm is RCC and commonly shows hypoechogenicity/heterogeneous echotexture (25). Internal vascularity may be appreciated in pseudotumors but they do not cause any splaying or distortion of the normal vessels (Fig. 2).

Ultrasound and Doppler appearance of pseudotumors in background renal parenchymal disease. (a–e) These lesions are solid isoechoic/hyperechoic (a, c, d, e) (*) and show internal vascularity (b and d). No splaying of vessels is seen (b, d). The lesions are homogeneous without any cystic component.
CEUS
There are various studies describing the role of CEUS in anatomic variants seen as renal pseudotumors where the contrast enhancement pattern is similar to that on multiphase CT/MRI (26, 27). However, there is a paucity of literature specifically on the CEUS appearance of CKD pseudotumors. In our experience, these lesions show enhancement similar to the surrounding parenchyma in all the phases and do not show any washout. A close scrutiny of the cine-loop may show mildly earlier enhancement compared to surrounding diseased parenchyma and suggestion of CM differentiation in the early phase (Figs. 3 and 4).
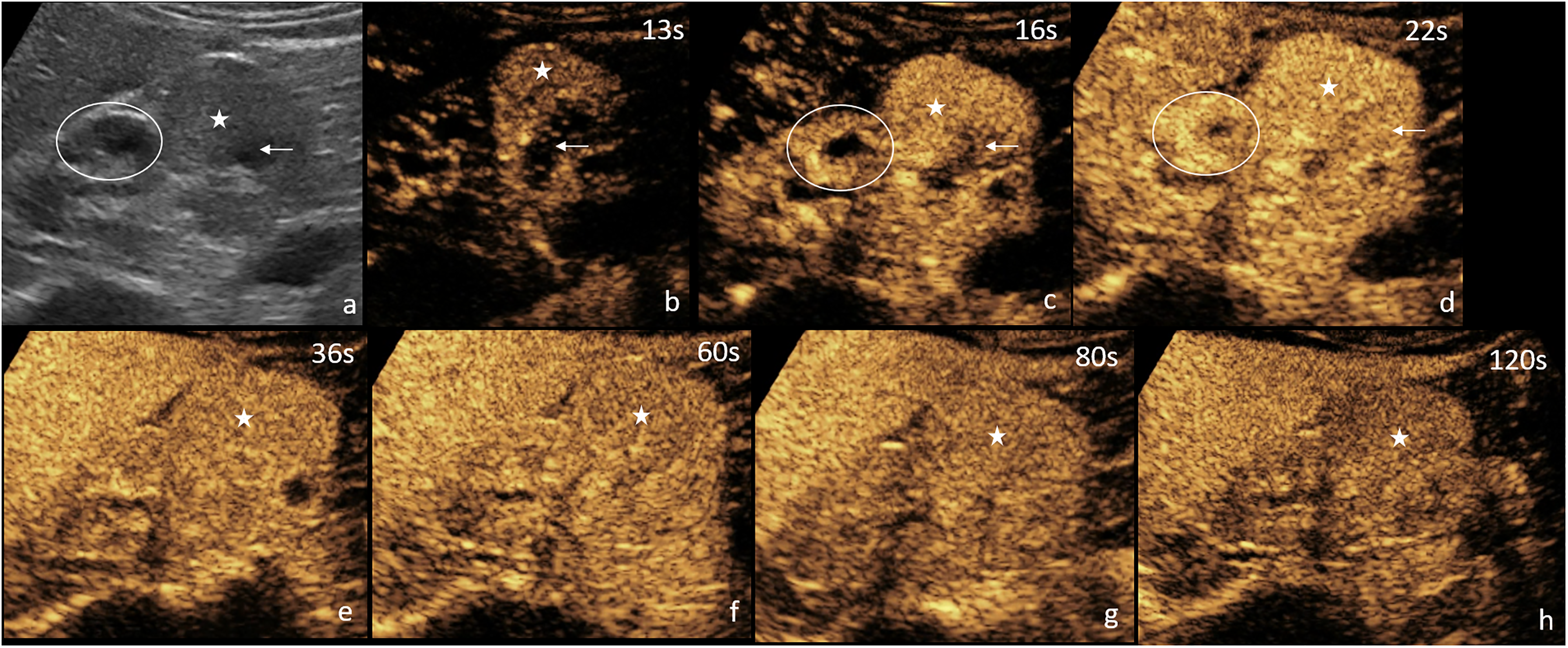
CEUS showing CKD pseudotumor enhancing earlier than surrounding parenchyma. (a) Reference gray-scale ultrasound image. (b–h) Static images saved from the cine-loop after injection of sulfur hexafluoride ultrasound contrast agent show early enhancement of the lesion (b, c) and then similar enhancement compared to surrounding renal parenchyma (with corticomedullary differentiation). No washout of the contrast is seen. The asterisk denotes the hypertrophied part enhancing similar to cortex, while the arrow depicts the hypertrophied part after the medullary enhancement. Oval denotes the adjacent renal parenchyma with apparent corticomedullary differentiation after contrast administration. US-guided biopsy was confirmatory. CEUS, contrast-enhanced ultrasound; CKD, chronic kidney disease.
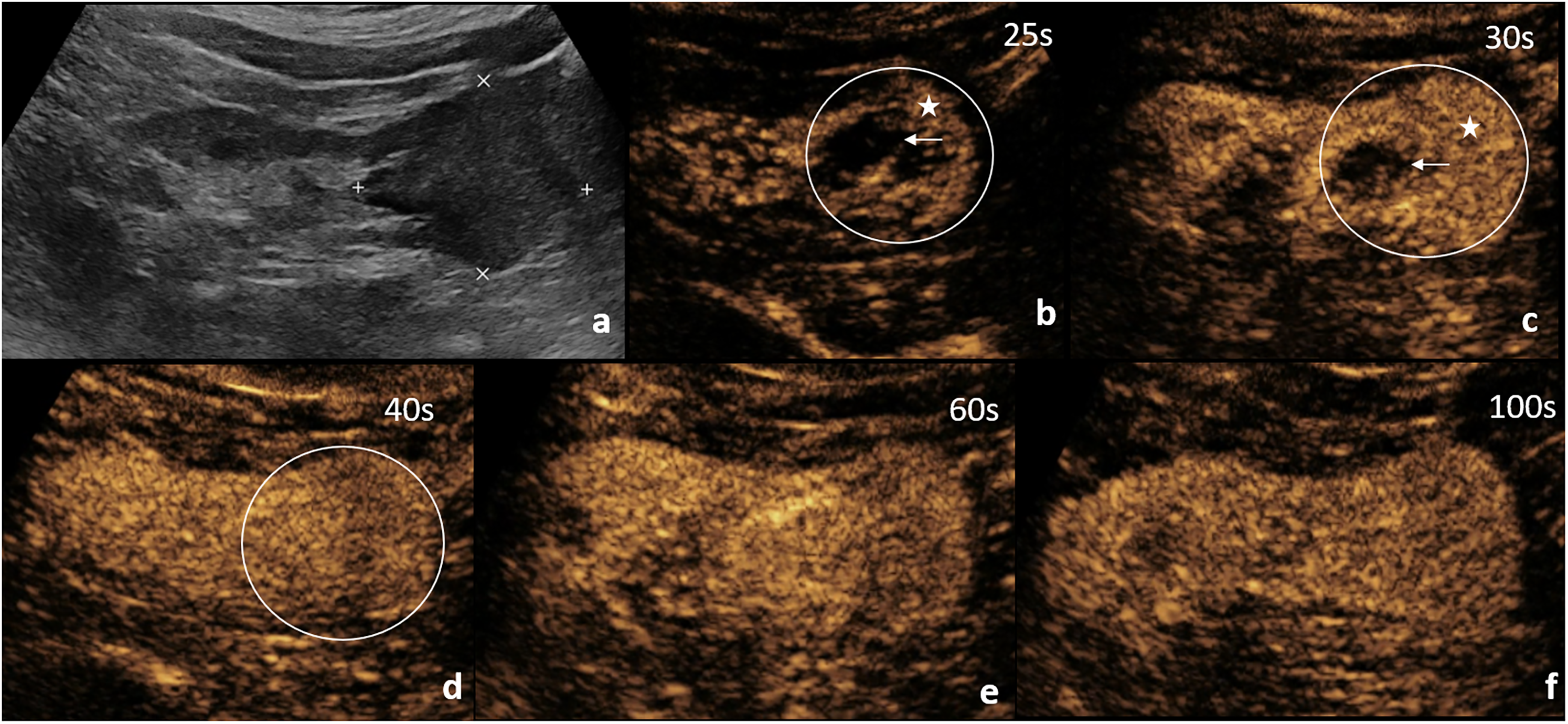
CEUS showing CKD pseudotumor enhancing similar to surrounding renal parenchyma. (a) Reference gray-scale ultrasound image showing hypoechoic solid mass in the lower pole. (b–f) Static images saved from the cine-loop after injection of sulfur hexafluoride US contrast agent show similar enhancement compared to surrounding renal parenchyma (with corticomedullary differentiation). No washout of the contrast is seen. The asterisk denotes the hypertrophied part enhancing similar to cortex, while the arrow depicts the hypertrophied part after the medullary enhancement. Oval denotes the mass on CEUS images. The diagnosis was validated on sampling. CEUS, contrast-enhanced ultrasound; CKD, chronic kidney disease.
RCCs on the other hand show heterogeneous enhancement on the CM phase due to their hypervascular nature (28). Few histological subtypes may appear hypoenhancing compared to surrounding parenchyma. Either way, RCCs show enhancement different from the surrounding parenchyma on at least one phase and show subsequent washout of contrast on delayed phases (29). Some studies also describe an enhancing pseudocapsule in RCCs (30). A chaotic pattern of vessels can also point towards the diagnosis of a malignant neoplastic etiology (31).
CT
The usual hurdle faced when evaluating a renal mass in the presence of renal dysfunction is the safety of iodinated contrast agent. The usual multiphase CT protocol for evaluation of renal lesions includes non-contrast scan, late arterial or CM phase at 30–50 s, venous or nephrographic phase at 80–100 s, and a delayed phase at 180 s after contrast administration. These lesions are usually hypodense on non-contrast scans without any fat/calcification or hemorrhage. Renal pseudotumors may show normal CM differentiation on CM phase unlike true masses which are hyper or hypoenhancing (2, 6, 32). These appear similar to the surrounding parenchyma in the nephrographic phase, in contrast to RCCs which usually appear hypoenhancing to the adjacent parenchyma (6). In the delayed phase, these lesions appear hyperdense because these are the areas with preserved renal function and thus the contrast uptake and excretion make them appear denser compared to the rest of the parenchyma (Fig. 5). RCCs may appear as washout in the delayed phase (33). However, in patients with renal dysfunction, especially having an estimated glomerular filtration rate <30 mL/kg/min, administration of i.v. iodinated contrast agents increase the risk of contrast-induced nephropathy. Hence CT has a limited role in these patients. If CE-CT is still undertaken, then iso-osmolar non-ionic contrast agents should be preferred.
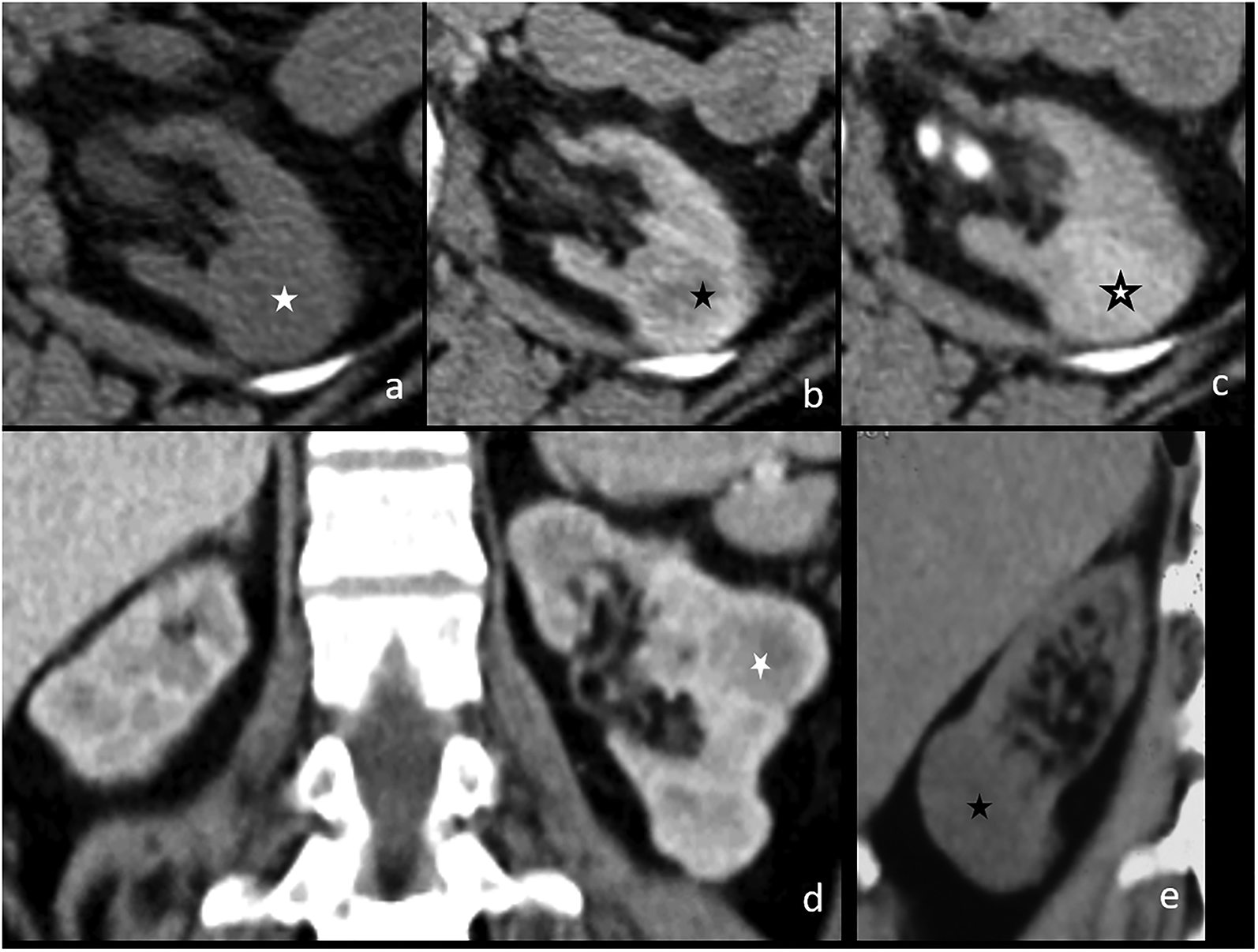
CT appearance of pseudotumors in background renal parenchymal disease. (a) There is an isodense left renal lesion on non-contrast scan, showing corticomedullary differentiation in early (35 s) post-contrast phase (b) and appearing hyperdense on delayed phase (3 min) (c) due to contrast retention, since these lesions represent hypertrophied renal parenchyma. (d) Coronal image shows a ball-type appearance of such lesions, mimicking neoplasms. Another patient with hypodense appearance of pseudotumor on non-contrast CT (e). The diagnosis was confirmed on biopsy in both the cases. CT, computed tomography.
MRI with DWI
MR has superior soft-tissue contrast resolution, because of which non-contrast MRI provides an edge over non-contrast CT. Contrast-enhanced MRI in CKD is associated with the ominous complication of nephrogenic systemic sclerosis and is thus best avoided. Conventional MR sequences show similar findings in RCCs and pseudotumors described as T1 hypo to isointense and T2 hyperintense lesions and hence are not very helpful in characterization. However, the interface between the lesion and the surrounding parenchyma is usually sharply demarcated in RCC and ill-defined in CKD pseudotumors. No capsule is present in the latter. If contrast is administered, then similar to CT, the pseudotumors may show CM differentiation in early phase, isointensity on nephrographic phase, and mild hyperintensity on delayed phase. However, absence of this typical enhancement pattern does not rule out pseudotumor since CM differentiation is already lost in such kidneys. There is no intracellular or intercellular fat/hemorrhage/necrosis in these lesions.
DWI provides quantification of the random Brownian motion of water molecules, which gives insights into the biological properties of the tissues. DWI has been found to be a useful adjunct in the characterization of focal renal lesions (9, 10, 34–37) and evaluation of renal parenchymal diseases (38–40). Studies describing the role of DWI have shown promising results with nearly all solid neoplastic masses showing restricted diffusion in contrast to CKD pseudotumors that did not show presence of restricted diffusion (Figs. 6–8). ADC values of pseudotumors were significantly higher than that of surrounding affected renal parenchyma and that of RCCs. A cutoff ADC value of 2.04 × 10−3 mm2/s is described in the published literature, to differentiate solid RCCs from pseudotumors with a specificity of 100% (15). Thus, absence of restricted diffusion in a solid mass favors pseudotumor, rather than malignancy. These increased ADC values are attributed to glomerular hypertrophy due to glomerular hyperperfusion with increased extracellular matrix in these relatively spared areas of the CKD kidney. Both increased capillary perfusion and decreased cell density leads to higher ADC values in pseudotumors (23). The surrounding parenchyma in these cases shows multiple peripheral-based wedge-shaped foci of restricted diffusion, becoming confluent at places.

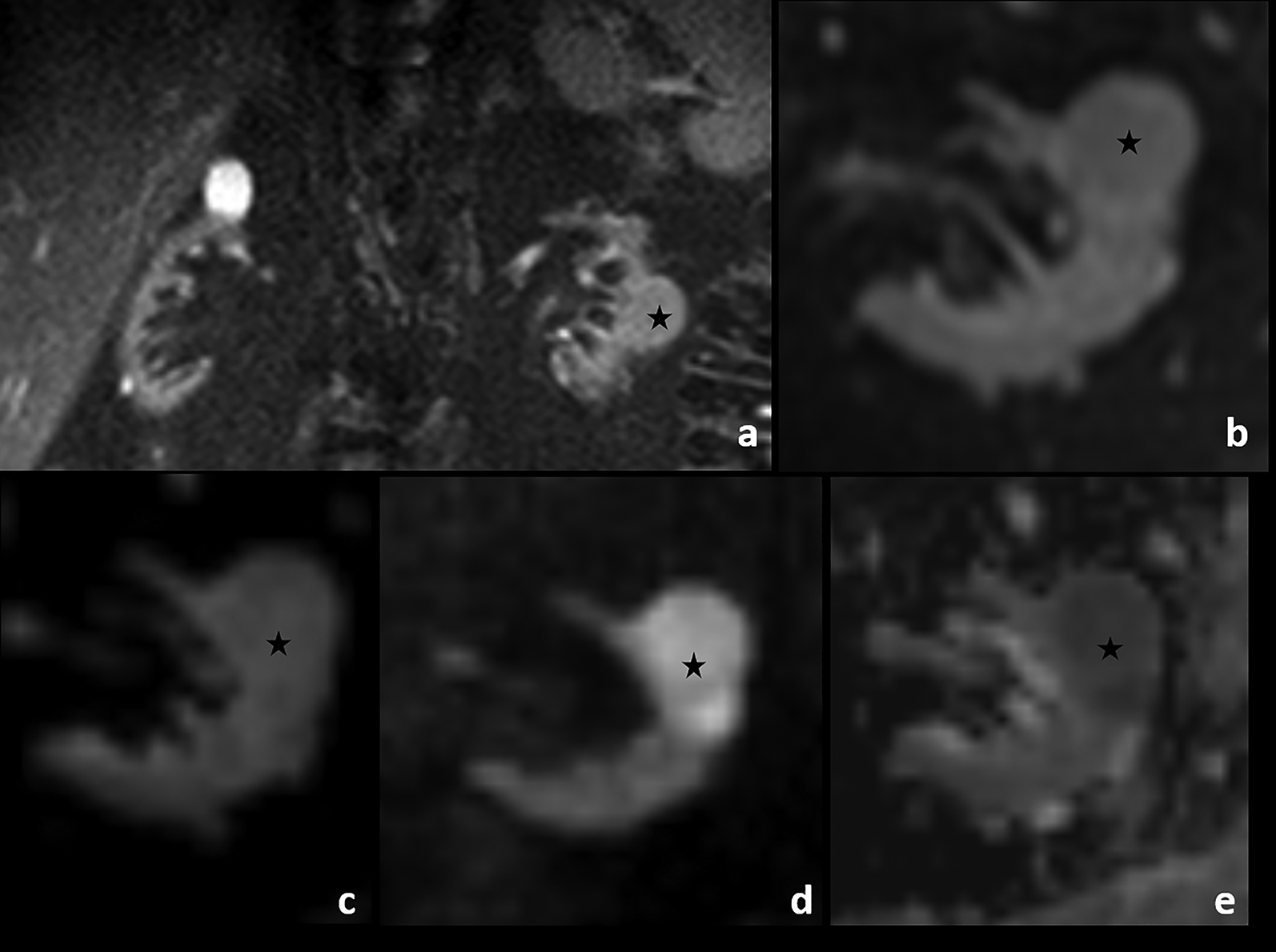
MRI appearance of pseudotumors in background renal parenchymal disease. (a–c) These lesions are hyperintense on T2W FS image (a) and isointense on T1W images (b, c). (d–f) Solid appearance and hyperintense signal on T2W images suggest malignancy; however, these lesions do not show diffusion restriction. Interestingly, background renal parenchyma shows restricted diffusion because of chronic parenchymal disease. ADC of lesion: 2 × 10−3 mm2/s and of diseased parenchyma was 1.6 × 10−3 mm2/s. ADC, apparent diffusion coefficient; FS, fat-suppressed; MRI, magnetic resonance imaging; T2W, T2-weighted.
Utility of DWI. (a–d) The CKD pseudotumors are ball-type lesions appearing as hyperintense on coronal T2W FS image (*) (a), simulating neoplasms but they show absence of diffusion restriction (*) (b–d). The background diseased renal parenchyma shows restricted diffusion because of chronic parenchymal disease. The ADC of the lesion was 2.1 × 10−3 mm2/s and of diseased parenchyma was 1.7 × 10−3 mm2/s. ADC, apparent diffusion coefficient; CKD, chronic kidney disease; DWI, diffusion-weighted imaging; FS, fat-suppressed; T2W, T2-weighted.
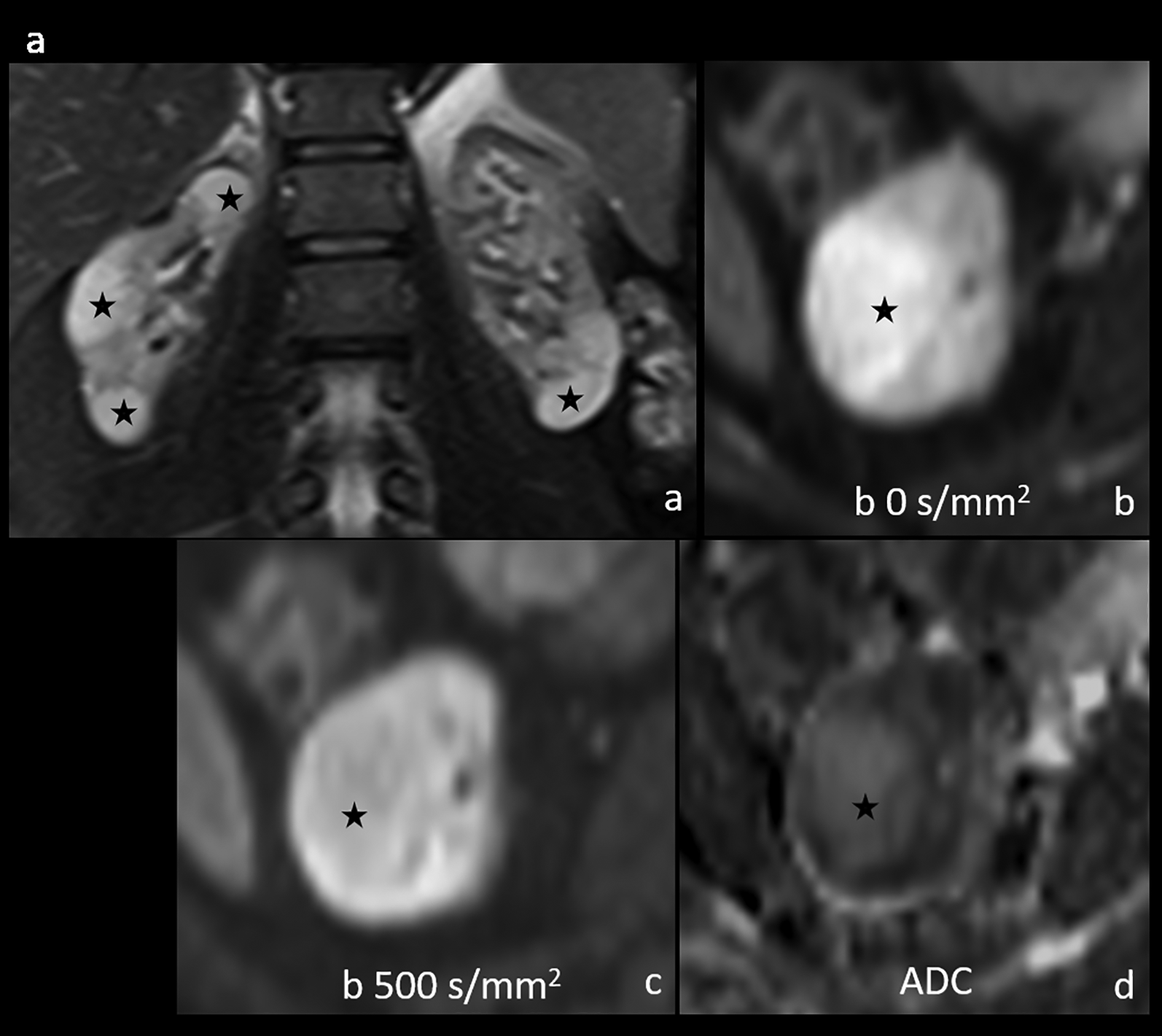
DWI in RCC in background CKD (biopsy proven). (a) Coronal T2W FS image shows bilateral small kidneys with attenuated parenchyma. There is a simple cyst in the upper pole of right kidney, another tiny cyst in the lower pole. A ball-type solid isointense lesion is seen in the interpolar region of the left kidney (*). (c) Axial T2W FS image, (c) DWI at b 0 s/mm2, (d) b 500 s/mm2, and (e) ADC map depict diffusion restriction within the lesion (ADC 1.1 × 10−3 mm2/s). The background diseased renal parenchyma also showed restricted diffusion because of chronic parenchymal disease lesion (ADC 1.5 × 10−3 mm2/s). ADC, apparent diffusion coefficient; CKD, chronic kidney disease; DWI, diffusion-weighted imaging; FS, fat-suppressed; RCC, renal cell carcinoma; T2W, T2-weighted.
How to differentiate pseudotumors from RCCs?
CKD pseudotumors are usually multiple and bilateral, homogeneous solid in appearance without any restricted diffusion. Table 1 summarizes the differentiating features of these mass-like regions of preserved renal parenchyma in CKD from RCC.
Summary of common imaging features of CKD pseudotumors and distinguishing parameters from malignancy.
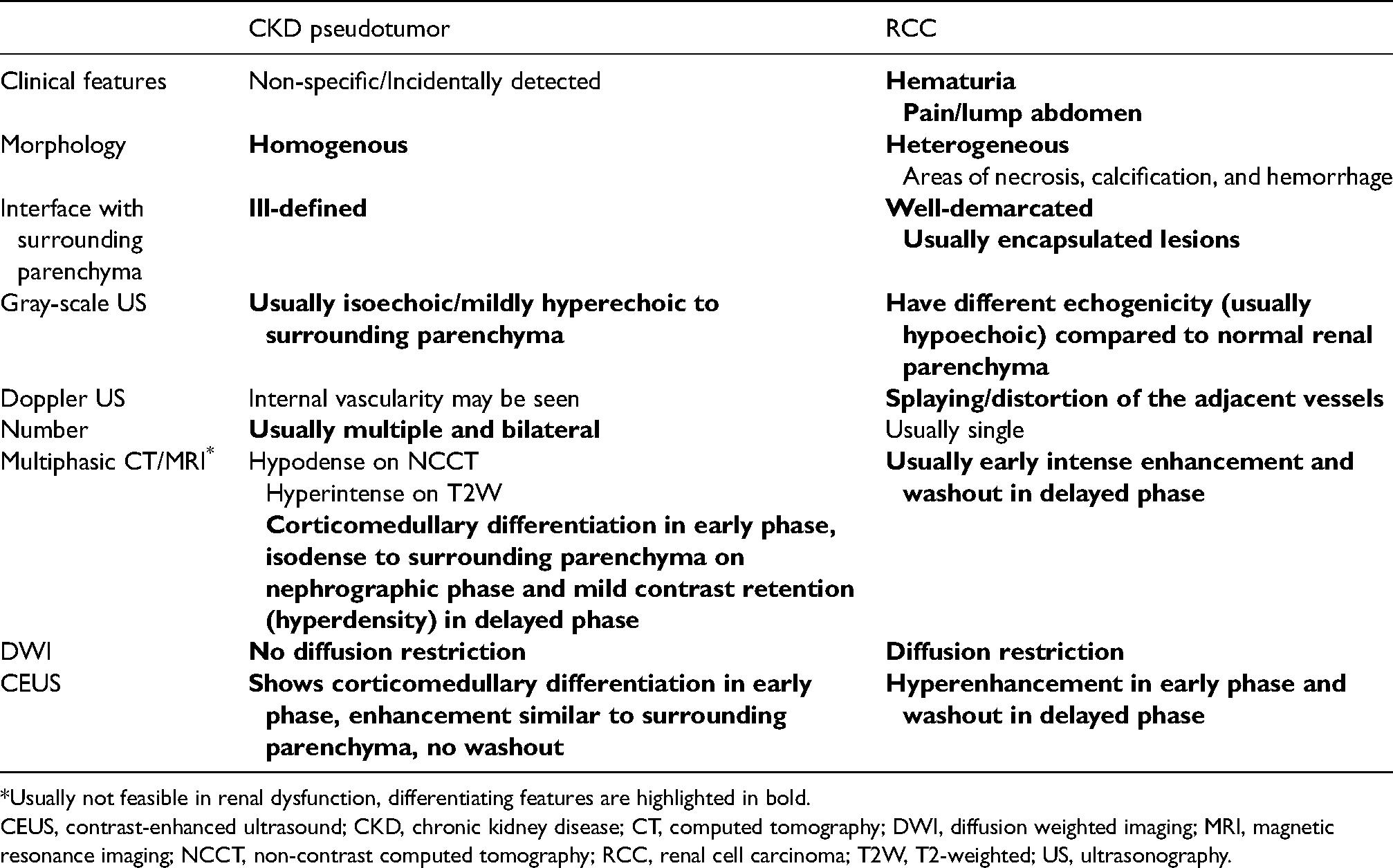
Usually not feasible in renal dysfunction, differentiating features are highlighted in bold.
CEUS, contrast-enhanced ultrasound; CKD, chronic kidney disease; CT, computed tomography; DWI, diffusion weighted imaging; MRI, magnetic resonance imaging; NCCT, non-contrast computed tomography; RCC, renal cell carcinoma; T2W, T2-weighted; US, ultrasonography.
Role of sampling
If typical imaging features are present with a low index of clinical suspicion, then these patients may be followed up on US to document lesion stability for one year. In equivocal cases, tissue sampling may be done under US guidance. The definitive diagnosis can be achieved by the absence of malignancy on biopsy. Rather, the pathological analysis shows features of background renal parenchymal disease. However, one should keep in mind that chronic renal dysfunction makes the patient prone to bleeding complications due to altered platelet function even in the presence of a normal platelet count and the usual co-existence of renal or renovascular hypertension (41, 42).
Conclusion
With the surge in chronic kidney disease globally coupled with wider availability of imaging, detection of focal renal masses in such a setting has increased. It is imperative for the radiologist, urologist, and nephrologist to be aware of this underrecognized entity of pseudotumor in renal dysfunction to avoid inadvertent surgery and biopsies. Multiple bilateral incidentally detected lesions favor the diagnosis; DW-MRI and CEUS increase the diagnostic confidence to differentiate these pseudotumors from RCC.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.