
Abstract
Idiopathic inflammatory myopathies are a rare heterogeneous group of chronic, autoimmune conditions characterized by the slow, progressive weakness of the skeletal muscles and inflammatory infiltrates in the muscle tissue. The predominant role of magnetic resonance imaging (MRI) in myositis imaging is to assess disease activity and to identify the target site for biopsy. Its role in phenotyping the disease is less explored. The aim of the present review was to examine the role of MRI in differentiating between the common inflammatory myopathies, i.e. dermatomyositis, polymyositis, and sporadic inclusion body myositis, and to describe the specific spectrum of MRI findings in various inflammatory myopathies.
Keywords
Introduction
Idiopathic inflammatory myopathies (IIMs) are a rare heterogeneous group of chronic, autoimmune conditions characterized by slow, progressive weakness of the skeletal muscles. Inflammatory infiltrates in the muscle tissue on histopathology is considered the hallmark of the disease (1,2).
Dermatomyositis (DM), polymyositis (PM), and sporadic inclusion body myositis (IBM) are the most common types of IIMs. There are multiple other types and subtypes such as immune-mediated necrotizing myopathy and amyopathic dermatomyositis with specific classification criteria as per the 2017 European League Against Rheumatism/American College of Rheumatology (EULAR/ACR) (3).
The diagnosis is usually based on the clinical presentation, increased serum creatine kinase (CK), and myositis-specific autoantibodies/myositis-associated autoantibodies (MSAs/MAAs), EMG findings, and muscle biopsy, of which muscle biopsy is the gold standard.
Imaging for phenotyping the disease is less often relied upon; however, it helps narrow the differential diagnosis, and in cases with high clinical–radiological concordance, may obviate the need for biopsy (1,4).
Magnetic resonance imaging (MRI) has emerged as a useful technique in management of these IIMs and though it is more often used for assessing the disease activity and for identifying the target site for biopsy (5–9), multiple studies have reported specific MRI findings in the various IIMs.
Muscle edema and atrophy are the two key identifying features of IIMs. The aim of the present review was to analyze the role of MRI in myositis imaging, to describe the common findings that help in phenotyping the common IIMs, and to discuss the way in which MRI can often obviate the need for a biopsy.
MRI of the skeletal muscles
The important information sought from an MRI (10,11) include: (i) assessment of extent of disease activity; (ii) staging of the disease (i.e. differentiating active from inactive); (iii) identifying the target site for biopsy; (iv) assessing the chronicity (presence/absence of atrophy); and (v) evaluating any concomitant pathology (5–9,12). It is also useful in monitoring the temporal evolution of disease on follow-up scans.
Since then, MRI has been considered to have a low specificity in characterizing the various types of IIMs. However, multiple studies have reported specific MRI findings in the various IIMs.
Protocol
In order to be able to give precisely all the information expected and to be able to characterize the type of IIMs, the MRI scan needs to be done with a specific myositis protocol.
The protocol used at our institute on a 3-T scanner (Ingenia CX, Philips Ltd, Eindhoven, The Netherlands) simulates a restricted whole-body (WB)-MRI with the extent of coverage including both arms, both thighs, and both legs. The sequences used are coronal and axial short tau inversion recovery (STIR) and axial T1-weighted (T1W) sequences. A large field of view (FOV) covering both thighs together and both legs together is used. However, the arms are scanned separately since it is difficult to accommodate them together in the same FOV. The large FOV enabled a wholesome overview of the symmetry, extent, and pattern of disease.
There are other protocols described that use WB-MRI and some that omit trunk imaging with MRI of only the thigh muscles. They have shown more or less similar results (13–16). There has been no convincing evidence in the literature of any added clinical information from a WB-MRI.
Contrast is not routinely administered in our institution, unless there is a focal lesion that requires further characterization, or there is a suspicion of infection, Multiple studies have evaluated the role of contrast in myositis imaging (1,17), but there has been no convincing evidence that the use of gadolinium contrast improves the diagnostic performance of MRI in IIMs (18).
Diffusion-weighted images have been used for assessing and monitoring the disease activity (19). We have not used diffusion imaging in our protocol.
There is no universally accepted and validated protocol/scoring system for evaluation of muscle MRI findings (13). No definite advantage of 3-T over 1.5-T magnet has been proposed yet for myositis imaging.
Muscle biopsy
Muscle biopsy is the cornerstone for the diagnosis of various myopathies. However, false-negative results occur in 10%–20% of all biopsies due to sampling error (20–22).
Biopsies of either very early or end-stage muscle disease are often non-diagnostic. Correlation with muscle imaging and targeting the appropriate site based on presence of edema and adequate muscle tissue increases the diagnostic yield (20,23,24).
Van De Vlekkert et al. (23) performed open surgical biopsy after selecting the muscle for biopsy based on MRI findings. They did not use real-time imaging guidance but still found that there was a decrease in the false-negative sampling rate from 23% to 19%, when compared to blind biopsy. MRI-guided wire localization followed by open muscle biopsy has also seen described (25) for identifying the site of active disease involvement.
It was suggested that the usefulness of MRI could be further improved with real-time biopsy guidance. Both MRI-guided biopsy and ultrasound–MRI fusion imaging have been used for real-time targeted muscle biopsy in patients with suspected myopathies (26).
MRI is the most sensitive for muscle edema; however, real-time MRI-guided biopsy requires specialized equipment that add significantly to the cost of the procedure. Ultrasound–MRI fusion combines the strength of both modalities and is also used for guiding the biopsy, without the need of the special MR-compatible instruments. A detailed description of these techniques is beyond the scope of this review (26).
Evaluation of images
Normal appearance of skeletal muscles on MRI
Normal healthy skeletal muscles show an intermediate signal intensity on the T1W images, which is higher than water, but less than the bone marrow and fat. The signal of the healthy muscles on STIR/fat suppressed T2-weighted images, is much less than water but higher than fat (Fig. 1) (27).
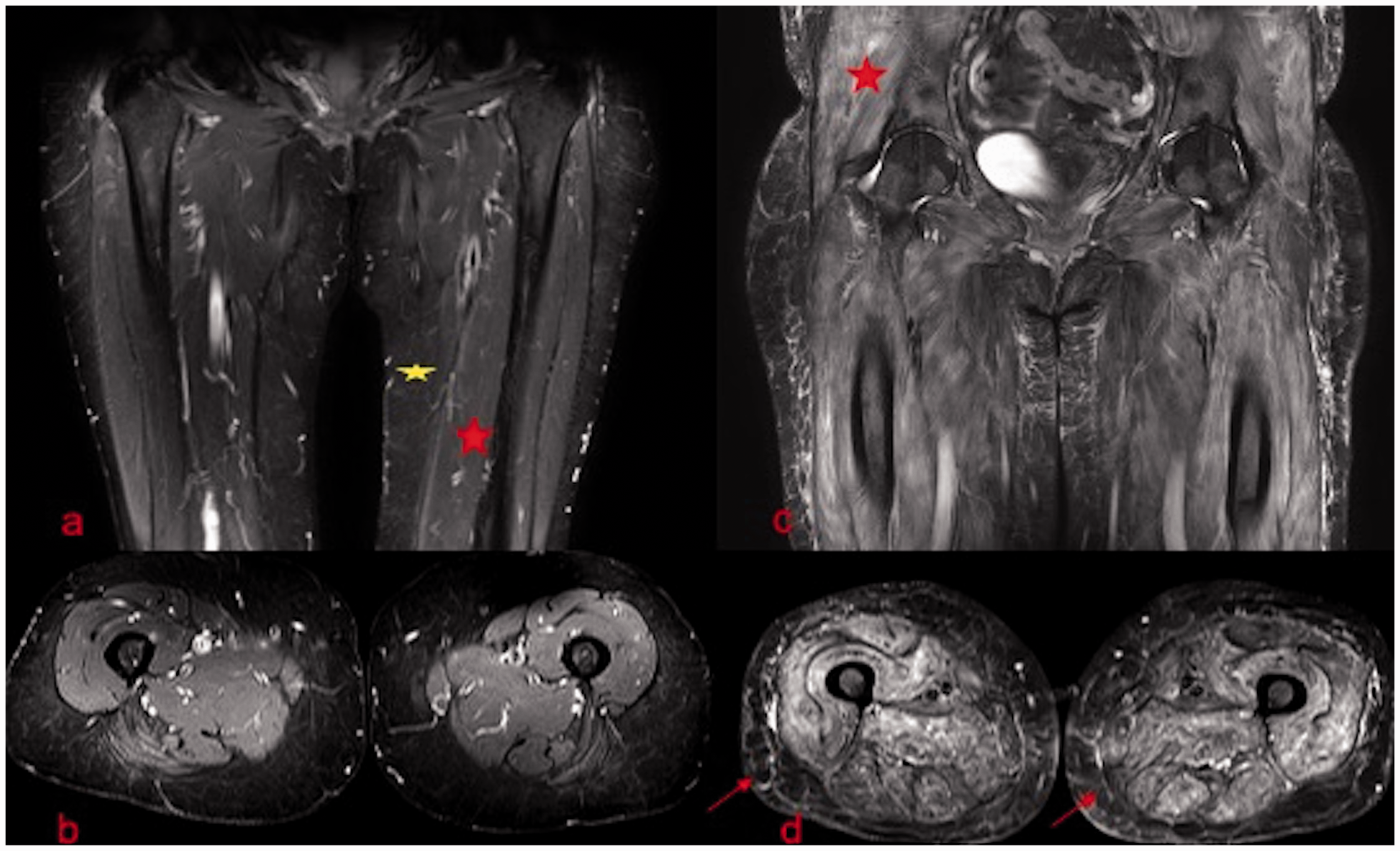
(a–d) Healthy vs. abnormal muscle. (a) Coronal STIR and (b) axial STIR images of both thighs in a healthy person show normal signal of the skeletal muscles (red asterisk), which is slightly hyperintense to fat (yellow asterisk). (c) Coronal STIR and (d) axial STIR images of the pelvis and proximal thigh region in a patient with inflammatory myopathy shows increased signal of the skeletal muscles consistent with edema (red asterisk). The subcutaneous edema is better appreciated on the STIR axial images (arrows in d).
Various pathological appearances seen with idiopathic inflammatory myopathies
Muscle edema and atrophy are the two key identifying features of IIMs.
Muscle edema
Edema/Inflammation is a marker of active disease and is evaluated on fluid-sensitive sequences like STIR/fat-saturated T2-weighted images, where it manifests as high signal (Fig. 1) (28).
Post-contrast fat-saturated T1W images may also be used to assess inflammation, where the enhancement is suggestive of active inflammation.
Distribution and types of muscle edema
The distribution and the pattern of edema helps in characterizing the IIM phenotype.
The edema can involve the muscles, the subcutaneous fat, or the fascial/perifascial planes. All of these structures or a variable combination of these structures can be involved. This can be easily evaluated/depicted on the MR images (Figs. 1 and 2).
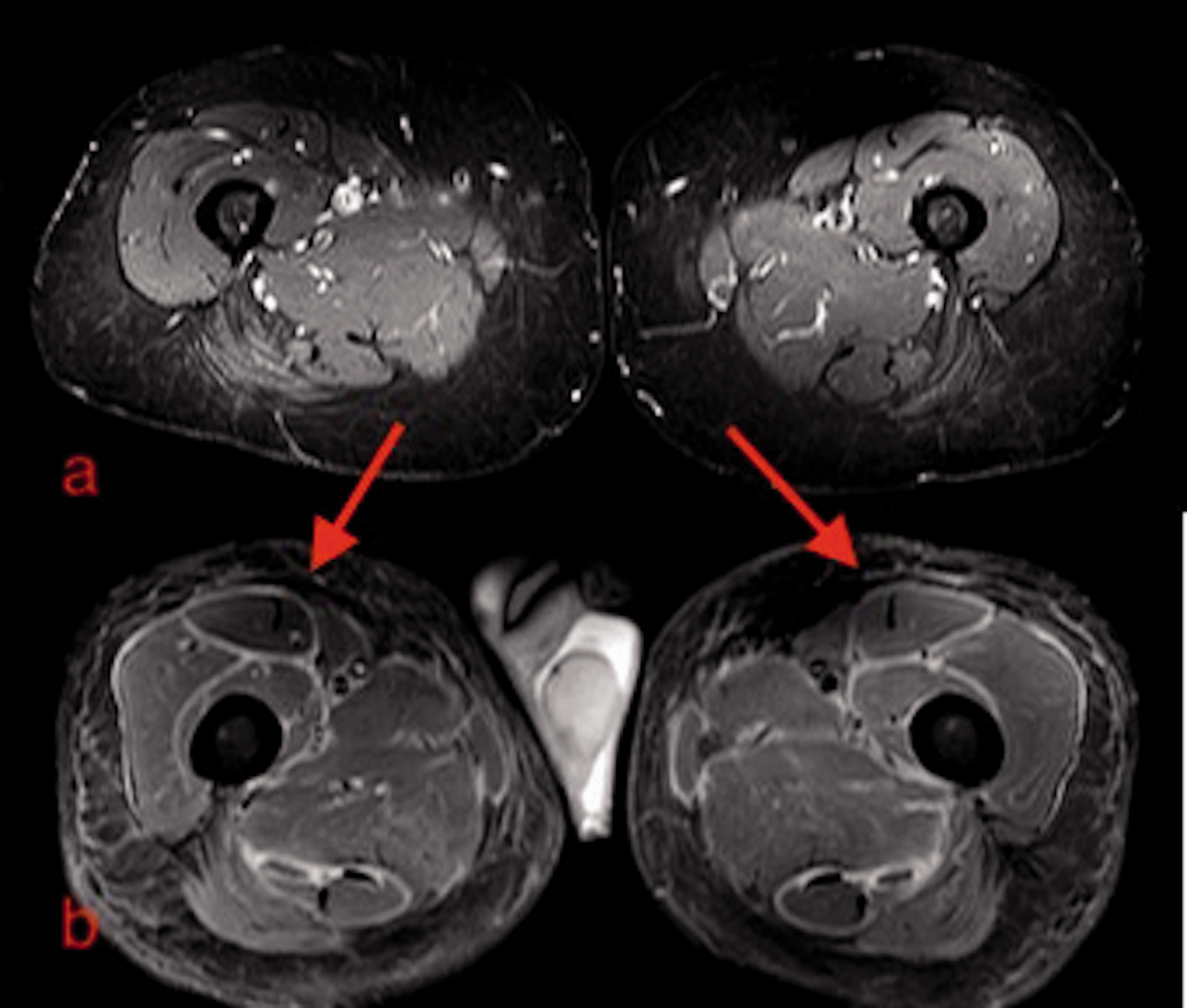
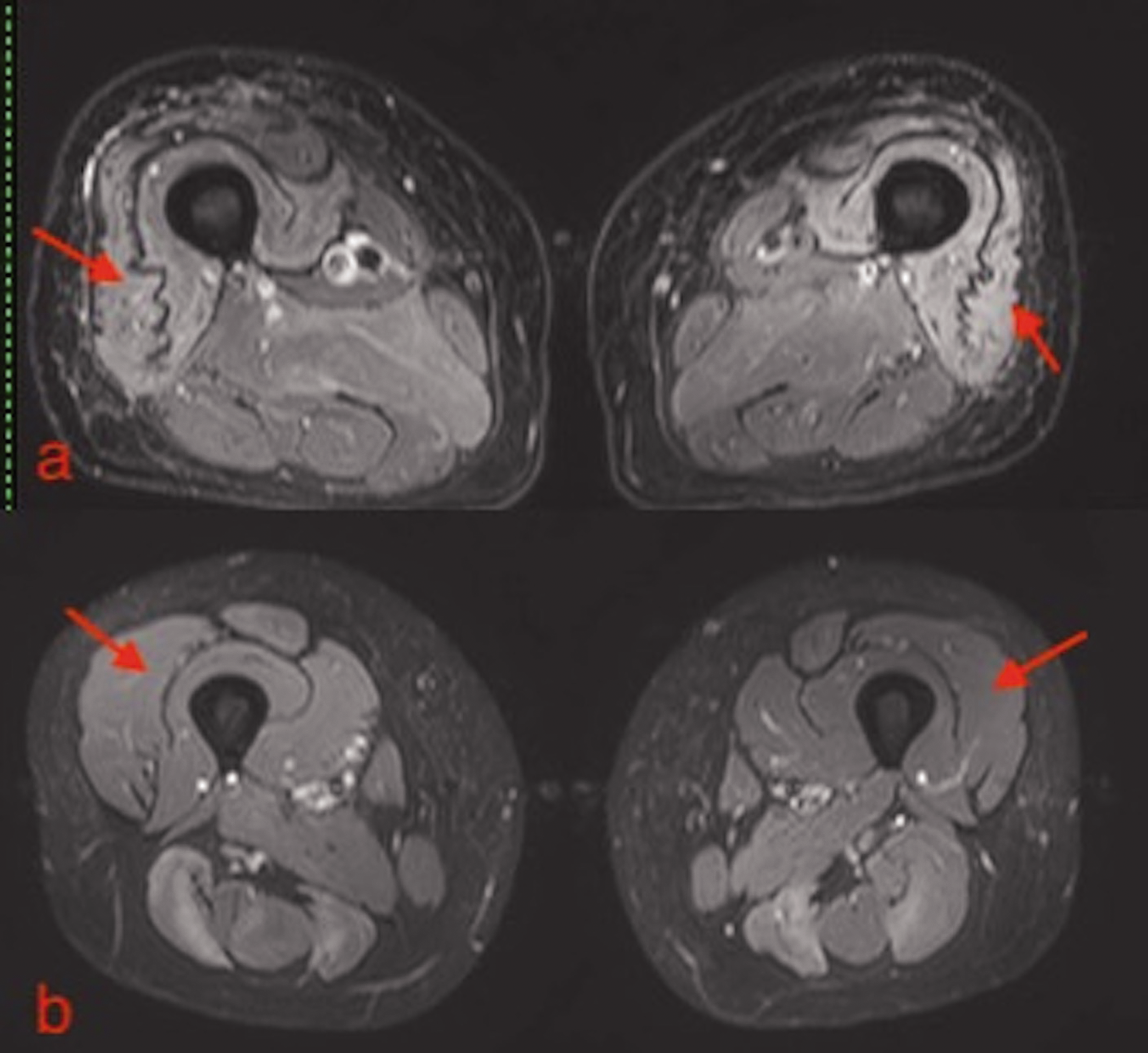
(a, b) Edema. (a) Axial STIR images of the thigh in a healthy person show normal signal of the skeletal muscles. (b) Axial STIR images of the thigh show symmetric fascial and perifascial edema (red arrows). There is also subcutaneous edema.
The muscle edema pattern can be subtyped into diffuse strong high signal edema, foggy edema, or a honeycomb pattern (Fig. 3) (1).

(a–c) Patterns of edema. (a) Axial STIR images of both shoulders show symmetrical diffuse strong high signal edema. (b) Axial STIR images of both thighs show foggy edema involving the posterior compartment muscles (arrows). The background vessel signal is well seen through the edema. (c) Axial STIR images of both thighs show a heterogeneous and reticular pattern of edema, representing honeycomb edema. The heterogeneous and reticular pattern is better appreciated in the posterior and medial compartment musculature.
The pattern is called “diffuse” when the entire muscle is involved homogenously with a high signal that masks the background vessels. It is called “foggy” when the signal is fainter, though still homogeneous and the background vessel signal can still be detected (1). A heterogeneous reticular pattern of edema within the muscle was labeled the “honeycomb” pattern (1).
The edema can also have a patchy distribution, which may be symmetric or asymmetric (Fig. 4). The edema is termed patchy when there are areas of muscle edema in a background of normal muscle signal intensity.
(a) Axial STIR image of both thigh in a lady with mixed connective tissue disease and overlap polymyositis shows patchy and symmetric edema predominantly involving the posterior compartment muscles of both thigh (arrows). There is no significant muscle atrophy. (b) Axial STIR image of both thighs in a 42-year-old man with myositis associated with systemic sclerosis, shows patchy, asymmetric edema involving the muscles of the bilateral thigh.
The spatial distribution of the edema (i.e. proximal/distal) can also be assessed with the MRI (Fig. 5).
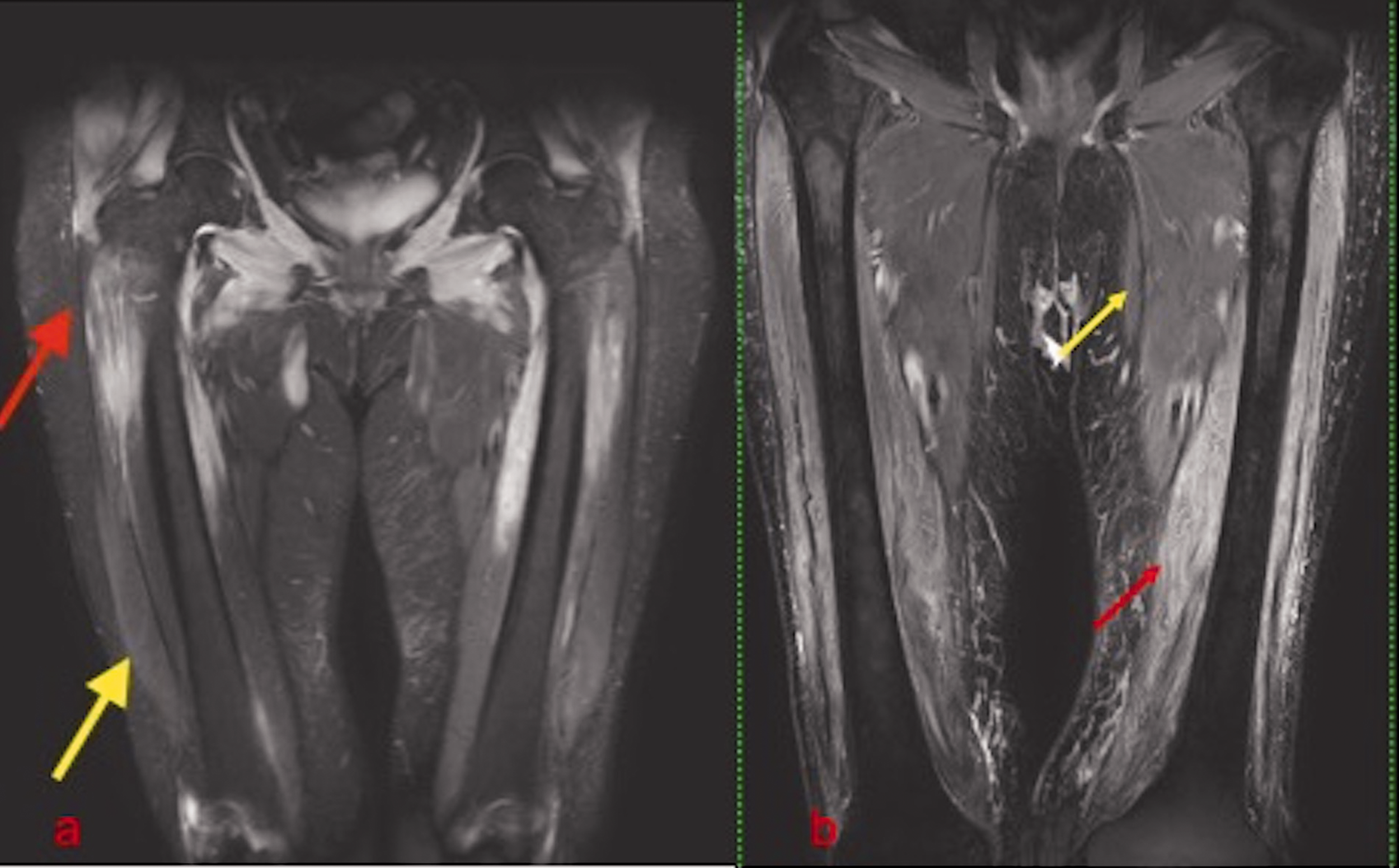
(a, b) Proximal–distal gradient. (a) Coronal STIR image of both thighs shows characteristic proximal distribution of edema (red arrow), with the relatively spared distal muscles in bilateral thigh (yellow arrow). (b) Coronal STIR image of both thighs shows more prominent involvement of the distal muscles of both thighs (red arrow), compared to the proximal muscles (yellow arrow).
Muscle atrophy
The chronicity of the disease is assessed by the presence of muscle atrophy and fat infiltration. This is best assessed on the T1W images.
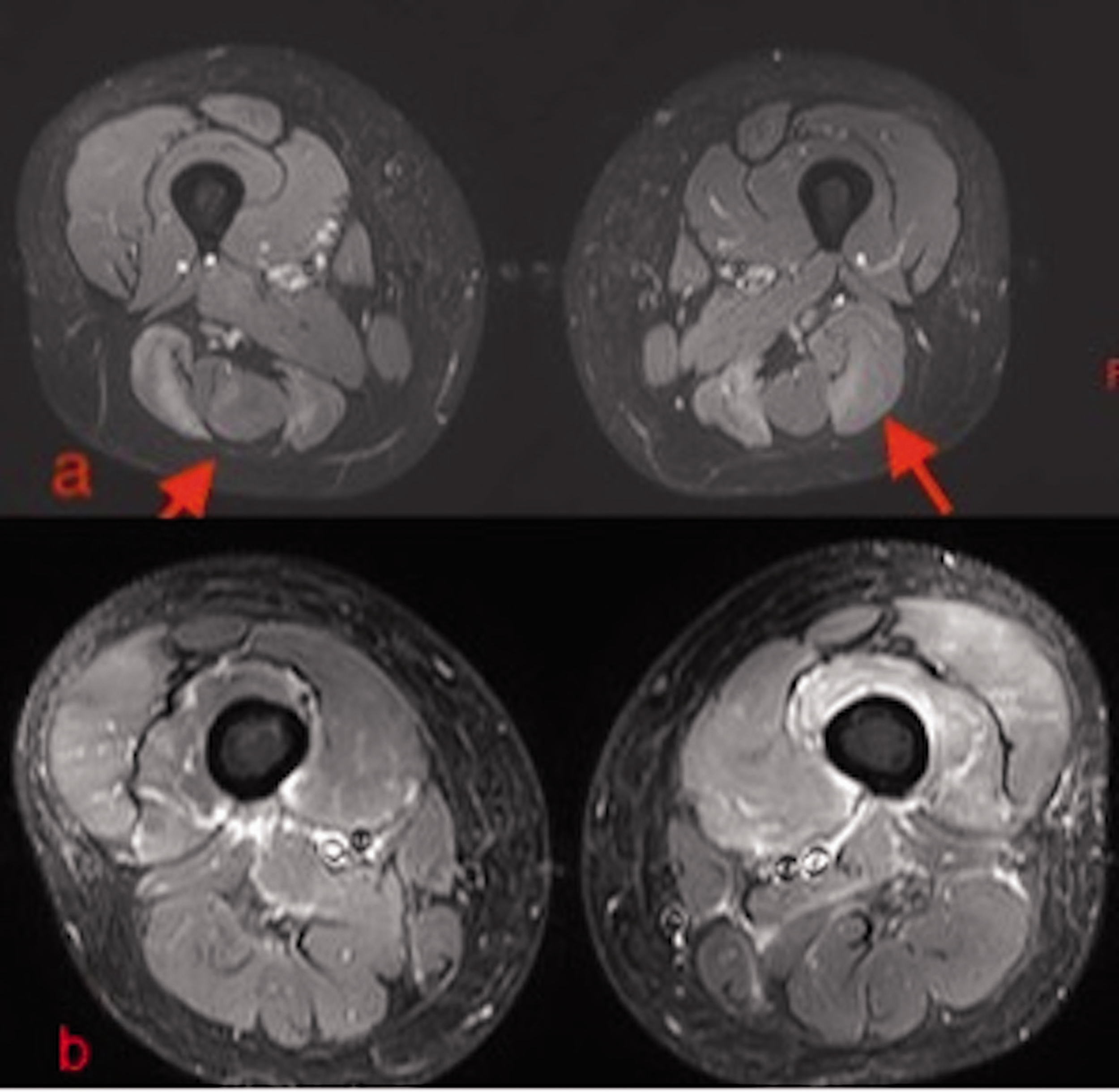
Muscle atrophy in cases of IIM is usually associated with fatty infiltration. Atrophy without fatty infiltration is not usually seen with IIMs (Fig. 6). The atrophy can be symmetric or asymmetric. It may also involve specific muscle subgroups, selectively.
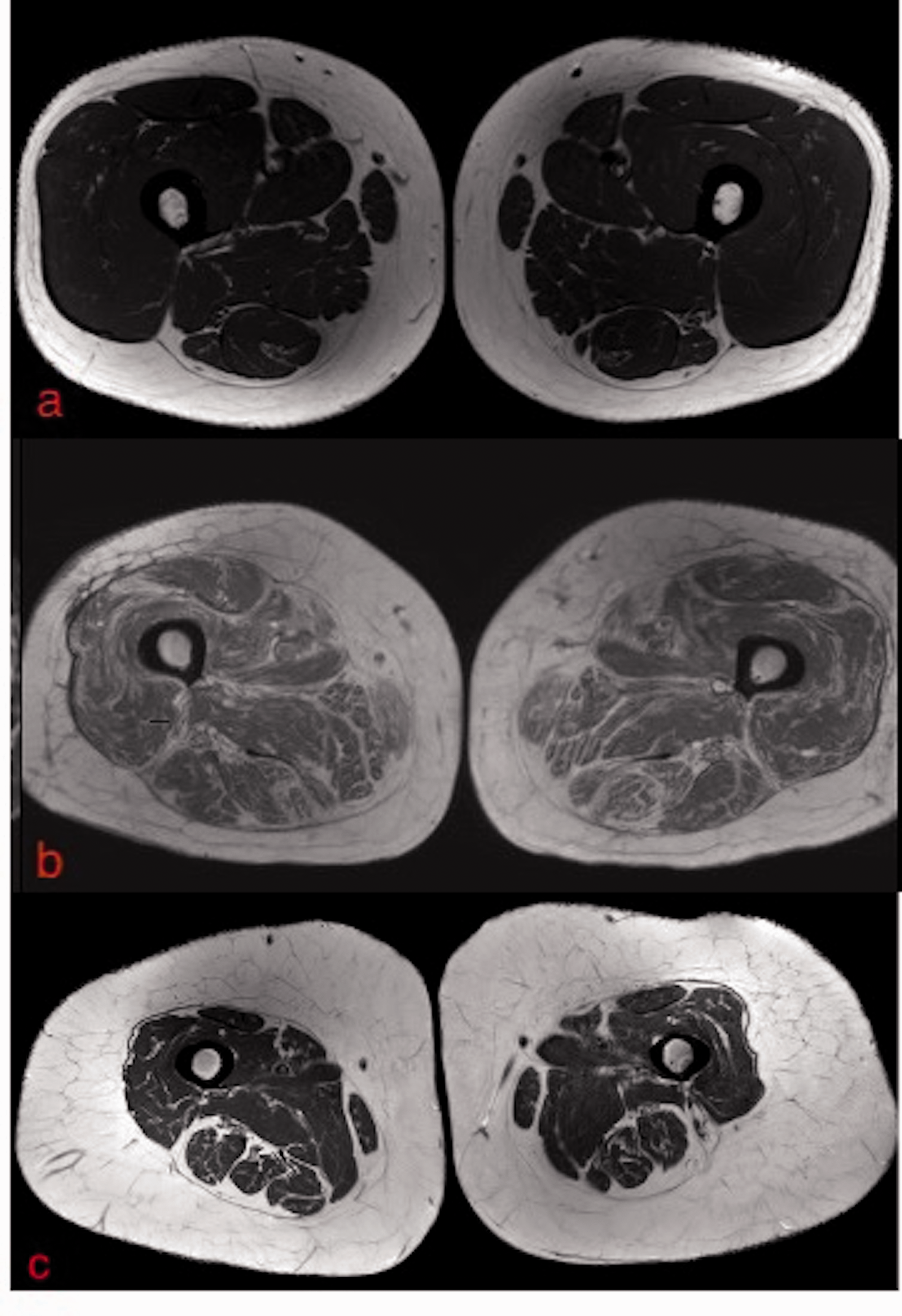
(a) Axial T1W image of both thigh in a healthy person showing normal signal and bulk of the skeletal muscles. (b) Axial T1W image of both thighs in a patient with inflammation shows diffuse symmetrical muscle atrophy with reduced muscle fibers that are replaced by fat. The overall muscle bulk and circumference is essentially unchanged. This is the typical pattern of atrophy seen in inflammatory myopathies. (c) Axial T1W image of both thighs in a 45-year-old woman with drug-induced myopathy shows diffuse symmetrical muscle atrophy with reduced muscle fibers and decreased muscle bulk and circumference. There is proliferation of the subcutaneous fat but without any fatty infiltration within the muscle bellies. T1W, T1-weighted.
Another sign of muscle atrophy is the “undulating fascia sign.” This refers to the undulating nature of the fascia between the vastus intermedius and vastus lateralis due to predominant muscle fiber volume loss (Fig. 7) (18).
(a) Axial STIR image of both thighs shows symmetrical atrophy and edema of the anterior compartment muscles with the characteristic “undulating fascia sign” (arrows). (b) Axial STIR image of both thighs shows normal anterior compartment muscles and normal and taught fascia (arrows).
This is proposed to be characteristic of acquired muscle atrophy/idiopathic inflammatory myopathies and helps differentiate congenital from acquired myopathy. In acquired/idiopathic inflammatory myopathies, unlike in congenital myopathies, the muscle atrophy sets in adult stages, after the muscles and the fascia have developed fully (18). As a result, selective muscle atrophy at this stage leaves behind a sagging and undulating fascia. This is characteristically seen in the anterior compartment muscles of the thigh where the atrophy and fatty infiltration of the vasti muscles leaves behind a sagging and undulating fascia.
However, the sign is seldom seen in cases of congenital/inherited myopathies, because the muscle development is abnormal from the birth and the fascia follows the pattern of the muscle development and develops in proportion to its bulk.
Specific MRI patterns
Though muscle biopsy is the gold standard for phenotyping the various IIMs, with the increasing use of MRI in management of the various IIMs, there has also been a growing interest in defining specific MRI patterns associated with specific phenotypes (Table 1). Multiple studies have reported these specific MRI findings in the various IIMs.
Specific MRI features of the various IIMs.

IIM, idiopathic inflammatory myositis; MRI, magnetic resonance imaging.
The various IIMs have been described as having a particular pattern/distribution of edema and atrophy. The purpose of this article is to describe these specific patterns in the three most common IIMs (DM, PM, and IBM).
Though the specificity of MRI for defining the subtype of IIM is low, it is always beneficial if a working diagnosis can be established on imaging, which will help in narrowing the differential diagnoses and in cases of high clinical–radiological concordance may obviate the need for biopsy (1). This is also of great help in differentiating IIMs such as IBM and PM where there is often a significant overlap of the clinical, biochemical, EMG, immunopathologic, as well as histopathologic features (18,29,30).
Polymyositis
PM usually involves the muscles in a symmetrical fashion. There is often isolated inflammation of the muscles without atrophy at the time of presentation (Fig. 8) (1). Though later in the course of the disease muscle atrophy with fatty infiltration is almost always seen.
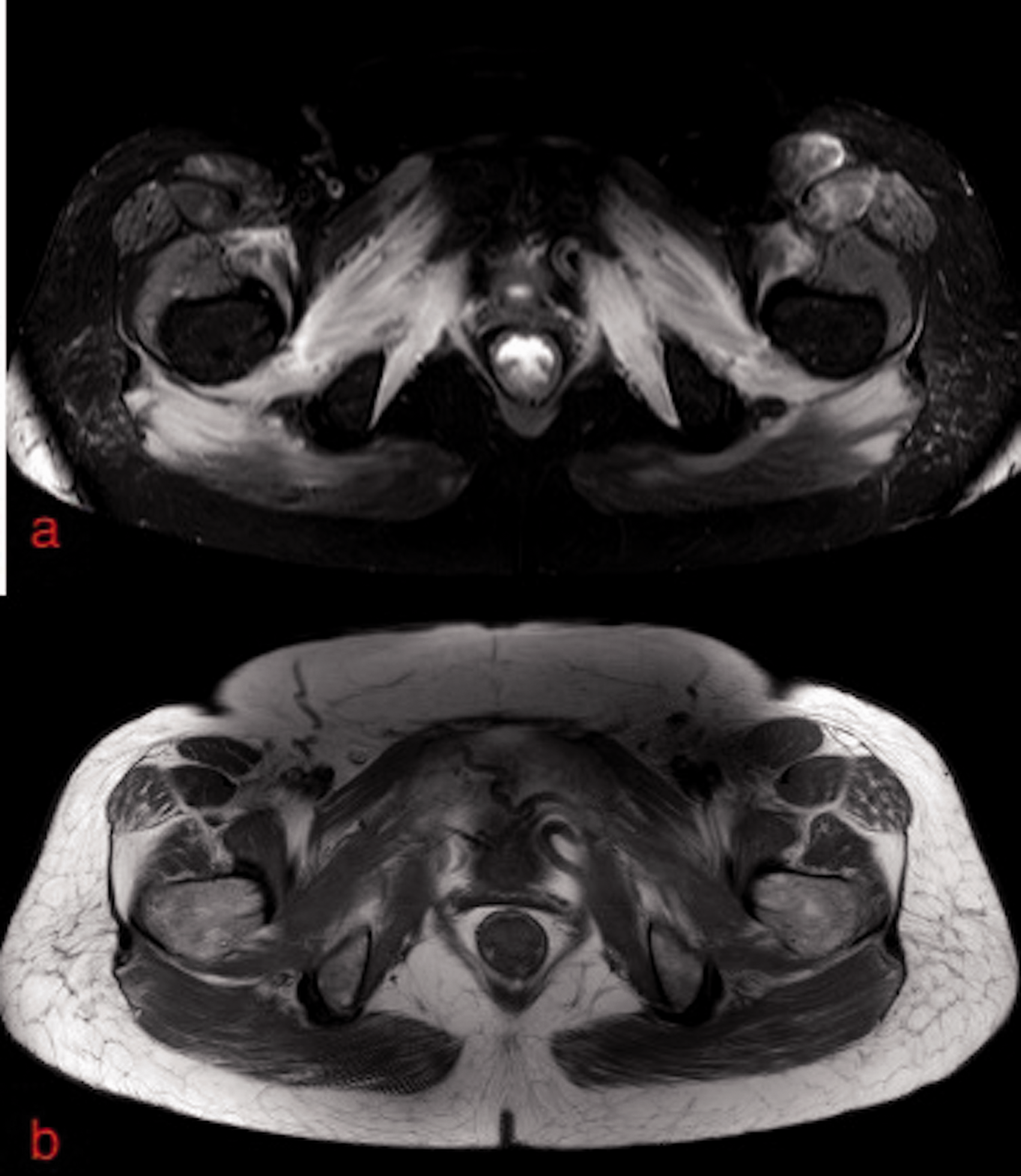
(a, b) Polymyositis: early active stage. (a) Axial STIR image of the pelvic floor shows symmetrical diffuse high signal edema. (b) Axial T1-weighted image at the same level does not show any significant muscle atrophy.
Muscle edema has a diffuse homogenous high signal pattern (Fig. 8) (1,31), likely because the disease is characterized by a diffuse immune reaction in the myofibers (10).
Fascial edema may or may not be present but is much less frequent than seen with DM (1,18). The fascial edema on MRI in PM has been reported to be associated with presence of MSAs/MAAs. Ukichi et al. (1) reported that all of their patients with PM with fascial edema on MRI were positive for MSAs/MAAs, such as anti-ARS antibodies and anti-Ku antibodies, while none of the MSAs/MAAs-negative PM patients had fascial edema on MRI (1). However, the MSAs/MAAs examined in their study were limited, and further studies are needed to validate the association. Subcutaneous fat edema is usually not seen in PM (1,31).
Muscle atrophy may or may not be accompanied with edema, depending on whether the disease is in the active or inactive stage (Fig. 9).
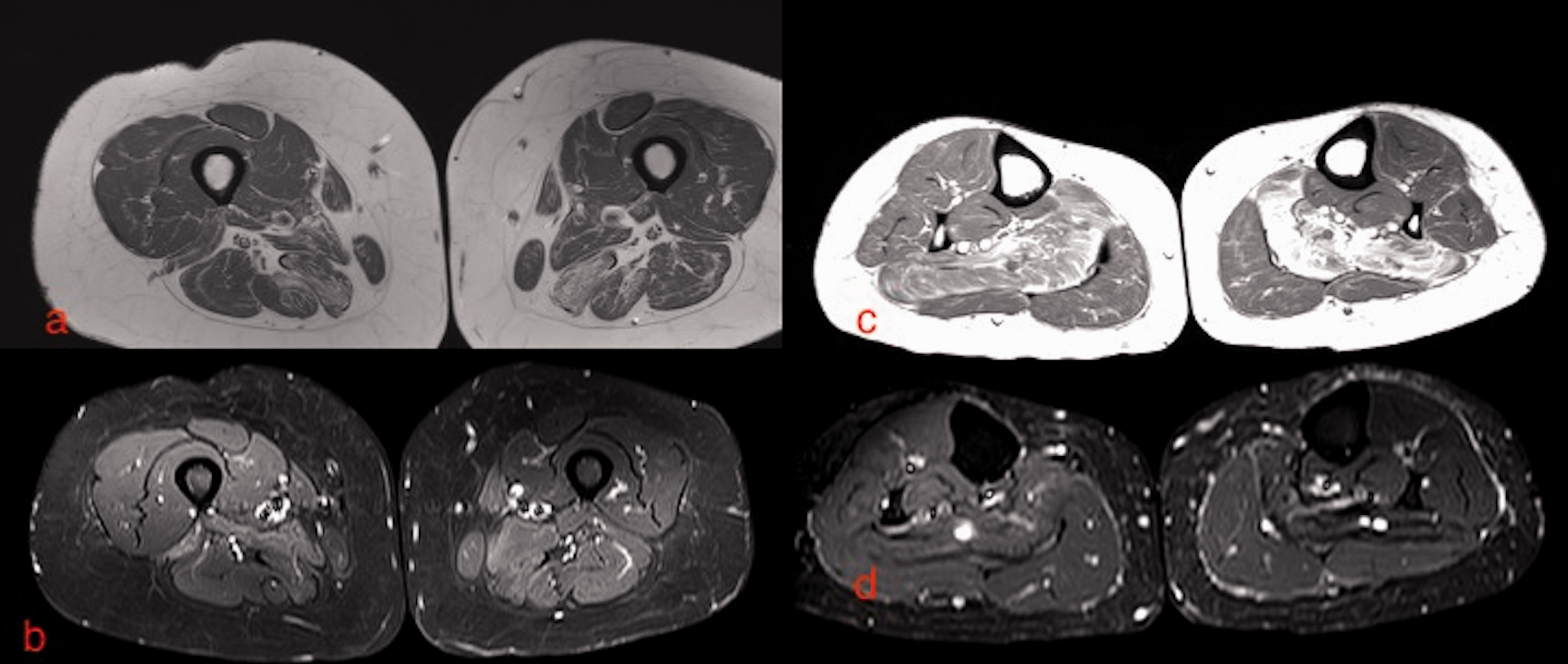
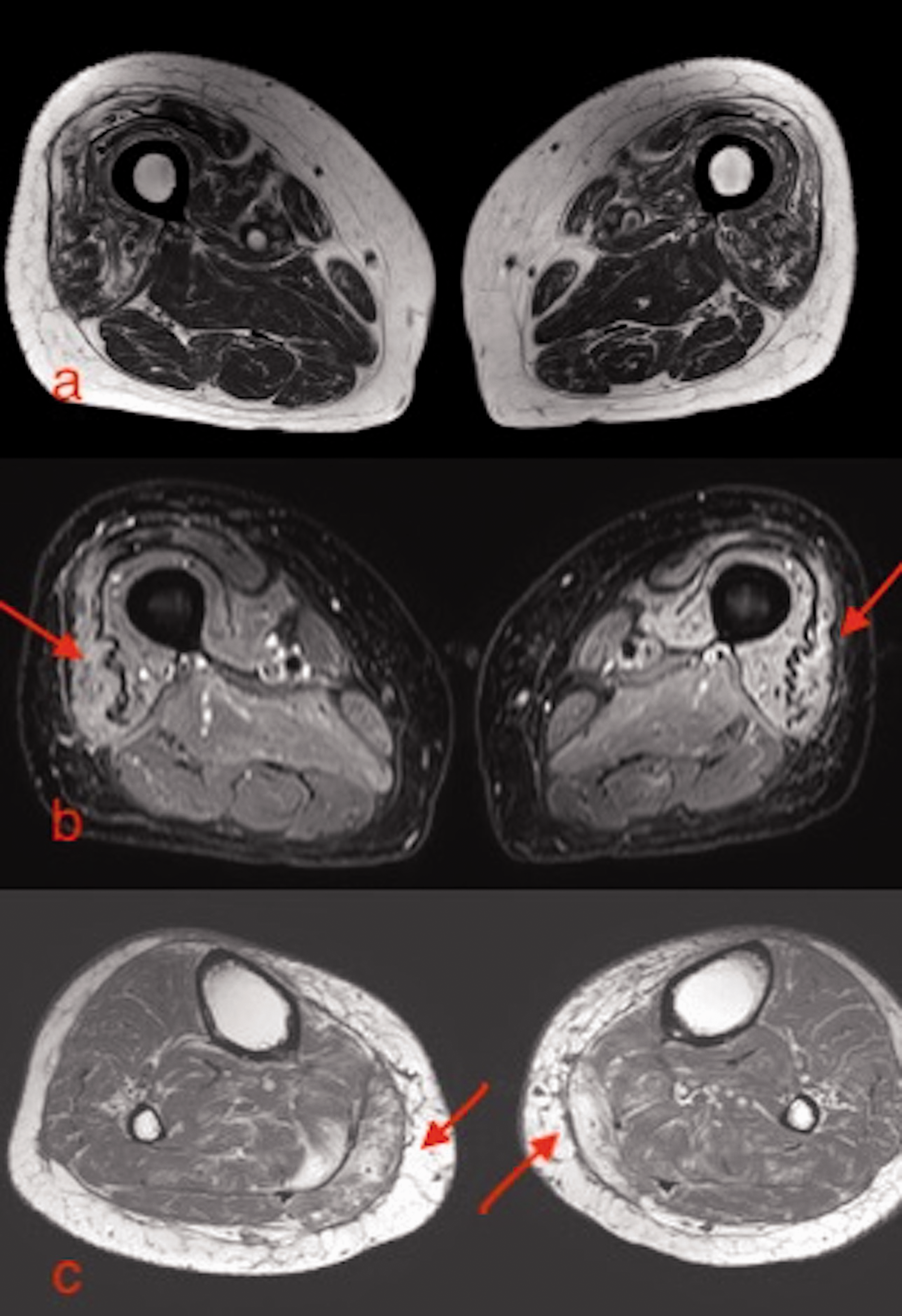
A 56-year-old woman with polymyositis in the late stage. (a) Axial T1W and (b) axial STIR images of both thighs show almost symmetrical atrophy of predominantly the posterior compartment muscles of the bilateral thigh. There is very minimal edema. (c, d) T1W and axial STIR images of both legs shows symmetrical atrophy and fatty infiltration in bilateral soleus muscle bellies. T1W, T1-weighted.
PM has a propensity to involve the proximal thigh muscles globally, or with predominant posterior compartment involvement (Fig. 9) (10,18).
Dermatomyositis
Patients with DM also have muscle involvement in a symmetrical fashion, but with the muscle edema more often showing a peripheral distribution and honeycomb pattern (perivascular).
The honeycomb pattern of edema may be explained by the propensity of the inflammatory cells in DM to infiltrate the perivascular/perifascicular sites and the interfascicular septa (Figs. 10–12) (1,2,31–34). There is also significant subcutaneous and fascial edema.
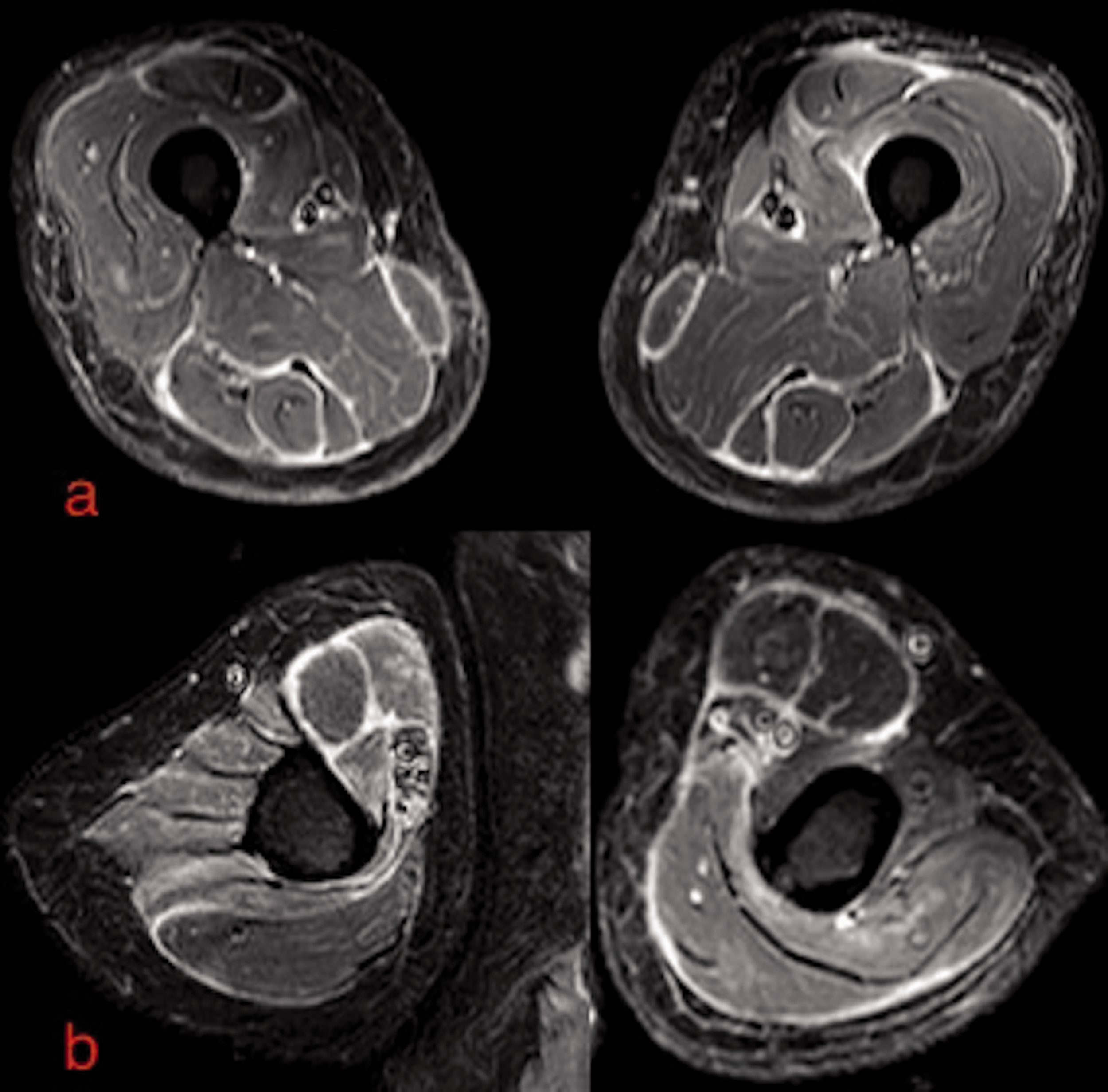
A 40-year-old woman with dermatomyositis. (a) Axial STIR image of both thighs shows almost symmetrical muscle edema with a honeycomb pattern. There is also significant subcutaneous edema in bilateral thigh. (b) Axial T1-weighted image, at the same level as (a), shows mild symmetrical muscle atrophy with mild fatty infiltration. (c, d) Axial STIR image of bilateral legs and bilateral shoulder girdle shows similar symmetrical edema pattern. The fascial edema is well appreciated on the leg images (c).

A 68-year-old woman with dermatomyositis. (a) Axial STIR image of both thighs shows almost symmetrical muscle edema with extensive fascial edema (arrows). There is also significant subcutaneous edema bilaterally. (b) Axial T1-weighted image at the same level as (a) does not show significant atrophy but the fascial edema is appreciated well.
A 61-year-old man with dermatomyositis. (a) Axial STIR image of both thighs shows characteristic fascial edema lining the muscles of both thighs symmetrically. There is also subcutaneous and muscle edema bilaterally. (b) Axial STIR images of both arms also show a similar pattern of edema.
There is frequent involvement of the quadriceps/anterior compartment thigh muscles (35). The proximal muscles are involved more than the distal.
The skin and subcutaneous calcifications characteristically associated with DM and well seen on the radiographs may not be appreciated on the MRI.
Sporadic inclusion body myositis
Sporadic IBM on MRI is characterized by isolated muscle atrophy with fatty infiltration (Fig. 13) (18). The reason is most likely the rather late presentation of this disease compared with PM, where the patient presents earlier in the course of the disease with muscle edema being the predominant imaging finding.
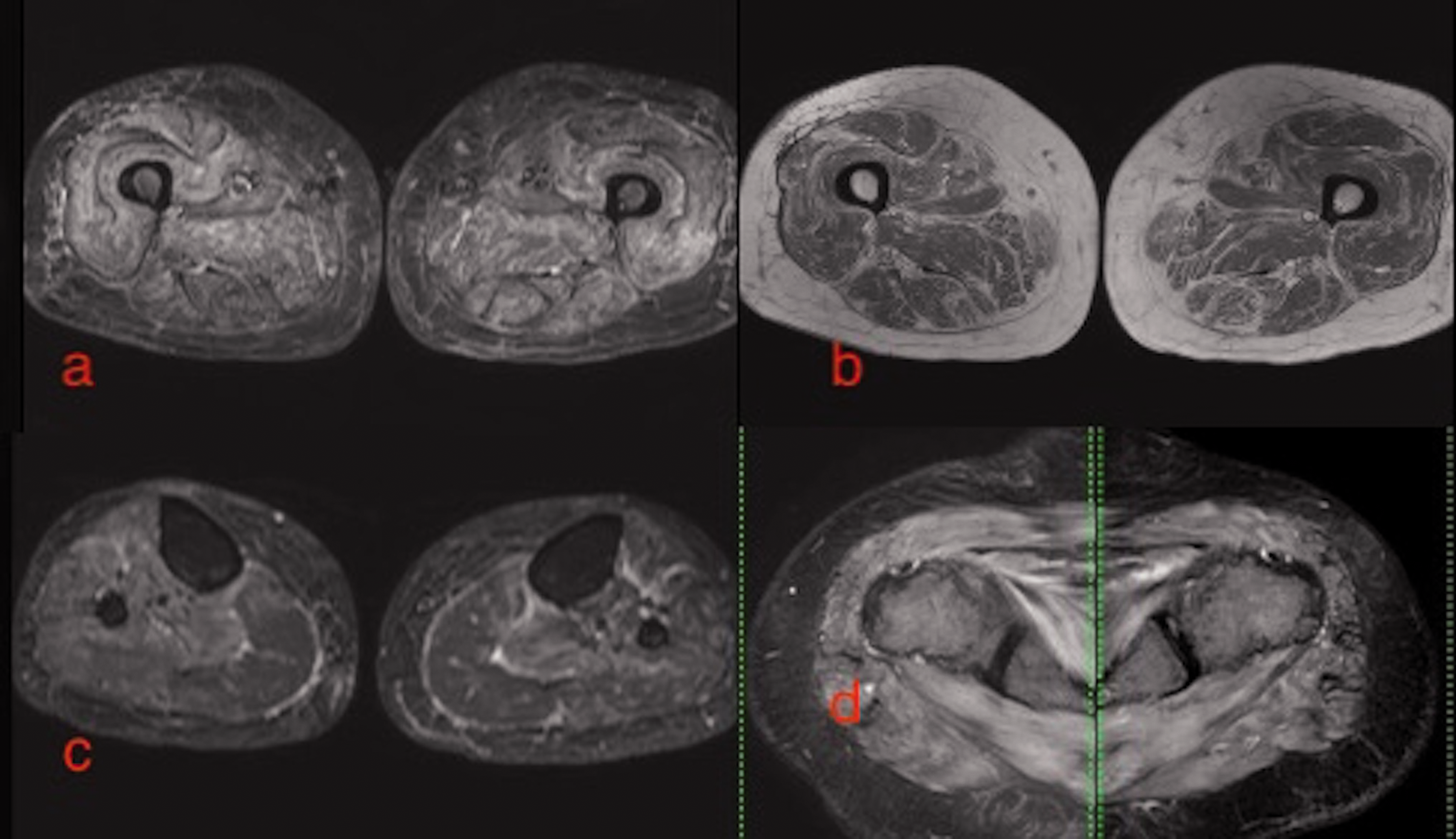
A 74-year-old woman with inclusion body myositis. (a) Axial STIR and (b) axial T1W images of both thighs at the same level shows symmetrical edema with severe atrophy and fatty infiltration of the anterior compartment muscles of both thigh (arrows). (c) Axial STIR and (d) axial T1W images of bilateral legs at the same level show mild atrophy with fatty infiltration in the medial head of the gastrocnemii in bilateral legs. There is no significant edema (arrows). T1W, T1-weighted.
Edema is less often seen as compared to fatty infiltration, but the concomitant presence of fatty infiltration, atrophy, and edema is often a feature of IBM (Figs. 13 and 14) (18). Fascial and subcutaneous edema are usually not seen. IBM shows a rather asymmetric muscle involvement (18).
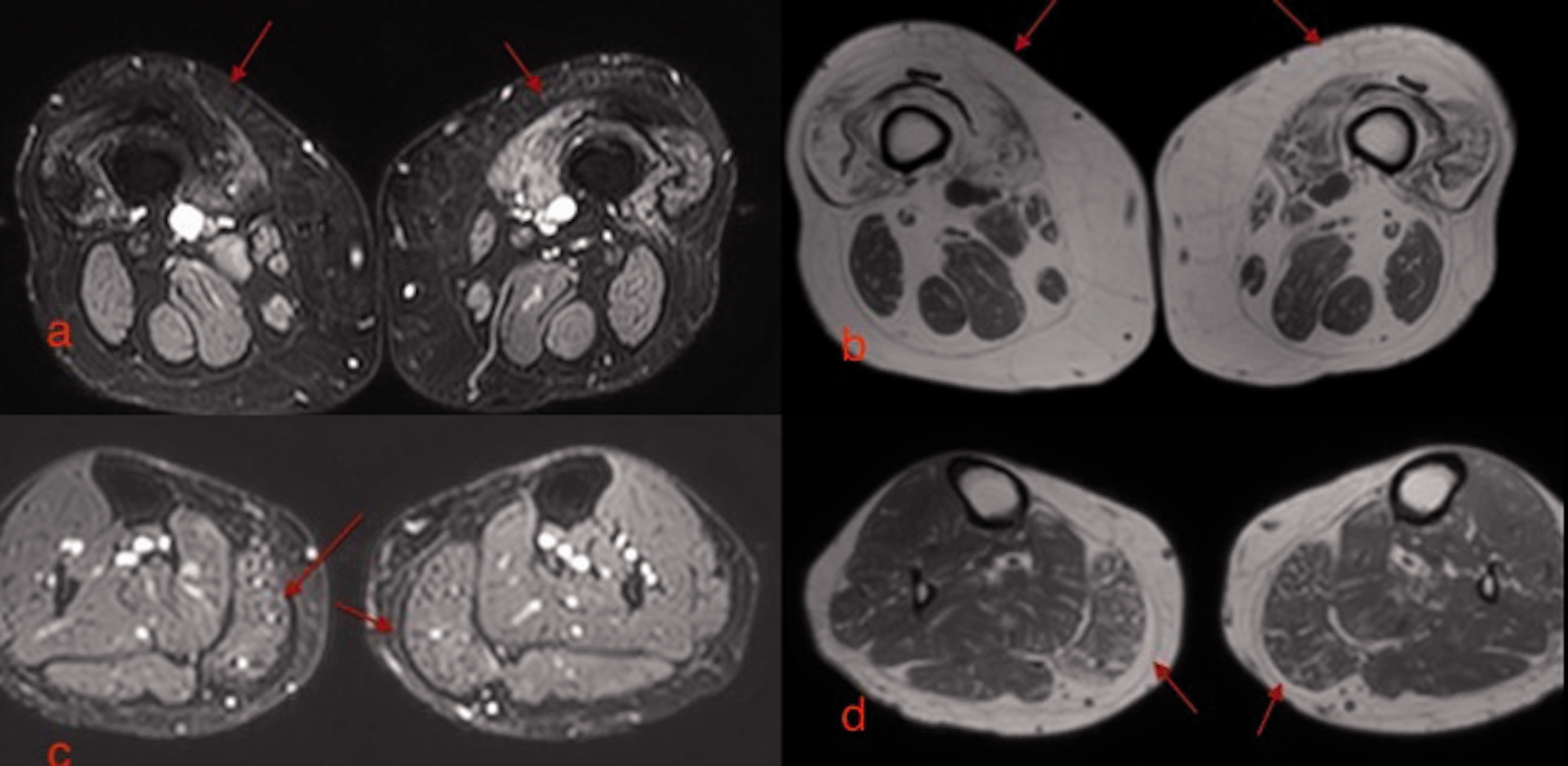
An 83-year-old man with inclusion body myositis. (a) Axial T1W image of both thighs shows symmetrical atrophy and fatty infiltration in the anterior compartment muscles. (b) Axial STIR image at the same level as (a) also shows symmetrical edema in the anterior compartment muscles. The “undulating fascia sign” is well seen (arrows). (c) Axial T1W image of bilateral legs shows selective but symmetrical atrophy with fatty infiltration of the medial head of the gastrocnemii in bilateral legs (arrows). Note that the bulk of the rest of the muscles in bilateral legs is well preserved. T1W, T1-weighted.
The anterior compartment muscles in the thigh are preferentially involved (17,18,36,37), with atrophy of the vasti muscles causing the “undulating fascia” sign (Fig. 14) (18,38). The sign is more often seen with IBM because of preferential anterior thigh muscle atrophy but is not specific and is seen with all cases of adult-onset IIMs with anterior compartment muscle atrophy. Some authors report relative sparing of the rectus femoris within the quadriceps (36,37). The distal sartorius is also commonly involved in IBM. Focal fatty replacement of the quadriceps and the distal sartorius is a feature more characteristic of IBM than of other IIMs (6,17) as the sartorius is usually spared in other adult-onset myopathies.
IBM shows a distal predominance with the distal portion of the quadriceps usually affected more, giving a “melted appearance” and the distal-proximal gradient is better appreciated in coronal sections (Fig. 15).
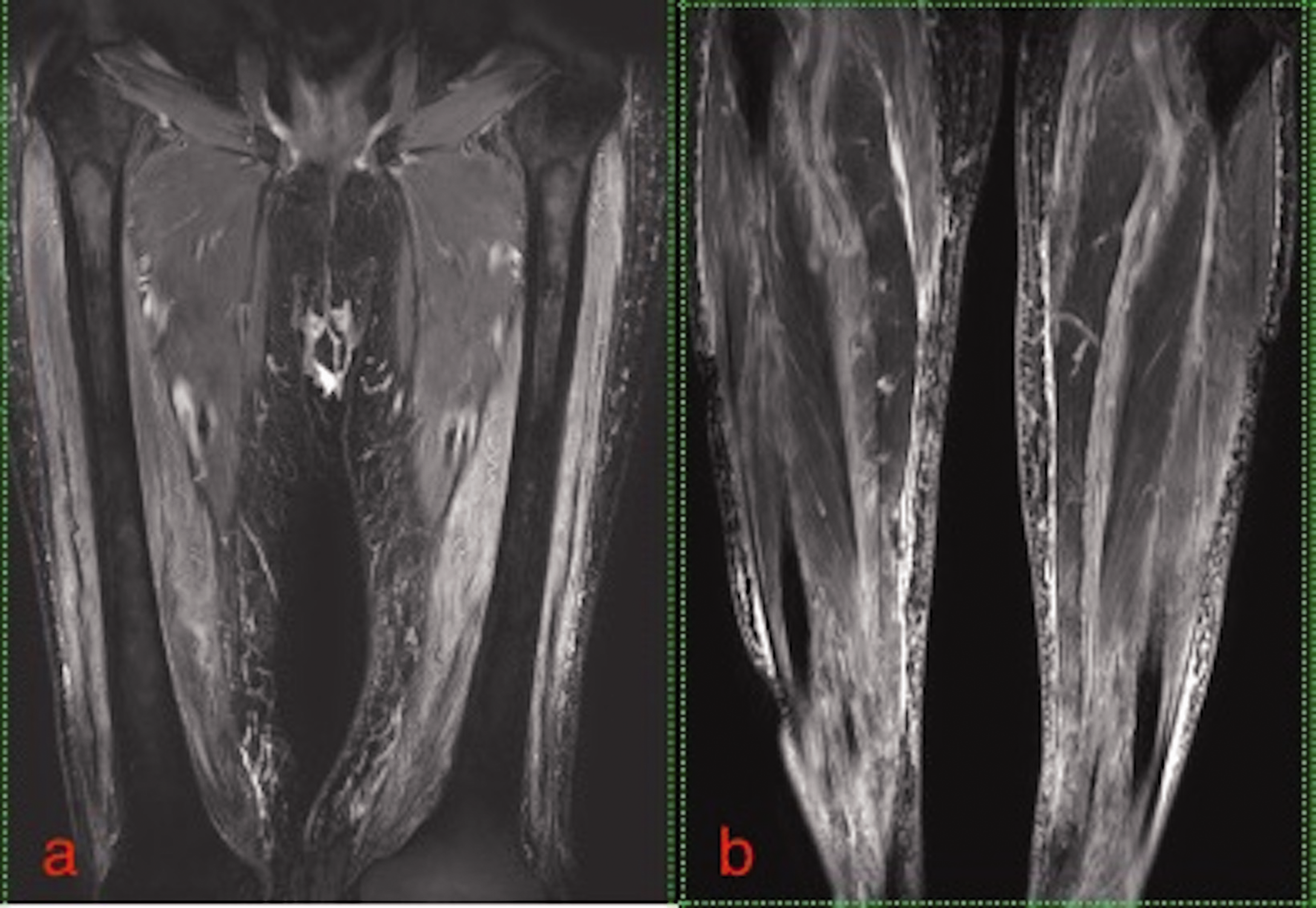
(a, b) Coronal STIR image of bilateral thighs and bilateral legs in a man with inclusion body myositis shows the distal predominance of the disease with edema and atrophy seen more prominently in the distal portions of the thigh as well as the leg.
Among the distal muscles, the medial head of the gastrocnemius (17,36–38), in the leg and the flexor digitorum profundus in the forearm, are preferentially involved and show atrophy and fatty infiltration (Figs. 13 and 14) (31,36,37).
The described selective pattern of muscle involvement can be easily recognized and is quite characteristic of IBM and may constitute an “imaging fingerprint” of IBM (38,39).
Sporadic IBM often has a very atypical clinical and histopathological presentation with a significant degree of overlap with other IIMs, particularly PM (40).
Additional tools are needed in such cases to confirm the diagnosis and a knowledge of the characteristic features of IBM and the features that differentiate it from other IIMs is of help in arriving to a confident diagnosis.
Tasca et al. (38) concluded that muscle MRI is an accurate tool for the diagnostic work-up of patients with suspected IBM and may be particularly helpful in patients with early disease or who lack the classical IBM pathology.
Summary
Muscle MRI in cases of IIMs, besides being helpful in assessing and monitoring the disease activity and in identifying the optimal site for biopsy, can provide important diagnostic clues to phenotype the various IIMs.
Through this article, we tried to create awareness of these typical MRI patterns in various IIMs. Though biopsy is often necessary to establish the diagnosis, identifying the typical MRI pattern can help us limit the broad differential diagnosis and in some cases with high clinical–radiological concordance also obviate biopsy.
A gestalt approach to reading a properly done MRI (with an adequate myositis protocol) with emphasis on analysis of the distribution and pattern of two important variables, namely, edema and muscle atrophy, has significant value in the diagnostic work-up and characterization of the various IIM subtypes.
To summarize, PM and DM show a symmetrical pattern of disease involvement, while IBM is often asymmetric as well. PM at presentation usually shows isolated inflammation with diffuse homogenous edema and shows global/posterior muscular compartment involvement in the thighs. DM has significant subcutaneous and fascial edema and shows frequent quadriceps/anterior compartment thigh involvement. The muscle edema in DM shows a peripheral distribution and honeycomb pattern.
Predominant muscle atrophy with fatty infiltration involving the anterior compartment muscles of the thigh (with distal predominance), the medial head of the gastrocnemius in the leg, and the flexor digitorum profundus in the forearm, are characteristic of IBM.
MRI pattern analysis is thus a rather simple and quick method for phenotyping at least the three most common varieties of IIMs. However, the role of MRI in the routine management of these patients and in patients with other subtypes of IIMs still remains to be established.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.