
Abstract
Background
Ulnar-sided wrist pain is associated with the development of multiple wrist pathologies. But the anatomical etiologies have not been fully understood.
Purpose
To determine the association of three anatomical factors with ulnar-sided wrist pain, including ulnar variance (UV), distal ulnar volar angle (DUVA), and pisiform-ulnar distance (PUD).
Material and Methods
A total of 64 patients who had ulnar-sided wrist pain associated with training injuries were retrospectively studied. A control group included 64 healthy athletes from the same unit. The UV, DUVA, and PUD of each individual was measured on radiographs.
Results
The average UV and DUVA of those in the ulnar-sided pain group were 0.84 mm and 174.65°, respectively; the control group values were 0.39 mm and 175.11°. The differences between the two groups had no statistical significance (P > 0.05). The average PUD of the ulnar-sided wrist pain group was shorter than that of the control group (2.37 cm vs. 2.65 cm); the difference had statistical significance (P < 0.05). PUD had a negative correlation with ulnar-sided pain; it was an anatomical protective factor (odds ratio = 0.01; P < 0.00; 95% confidence interval=0.00–0.05). Both UV and DUVA had no significant correlations with ulnar-sided wrist pain (P > 0.05).
Conclusion
PUD has a significant correlation with ulnar-sided wrist pain. It is the anatomical protective factor. Both the UV and DUVA have no statistical association with ulnar-sided wrist pain, but we cannot ignore their potential pathogenic effects on wrists, and further studies are needed to confirm the results.
Keywords
Introduction
Ulnar-sided wrist pain is a frequently encountered complex problem. The causes are divided into different sections according to the anatomical origin of the pain: soft tissue, bone, or neurovascular. Soft-tissue factors include triangular fibrocartilage complex tears, tendinopathy, ligament injuries, and instability (1–3). Bony pathologies encompass ulna-carpal impingement, Kienböck's disease, and malunion of distal radius fractures (4–7). Neurovascular causes, such as compression of the ulnar nerve in Guyon's canal syndrome, can also result in ulnar-sided wrist pain (8). However, some surgical procedures report good short-term efficacy, such as ulnar shortening osteotomy, partial capitate shortening osteotomy, and arthroscopic debridement of triangular fibrocartilage complex (TFCC) tear (9–12). There remain many unsolved problems including poor long-term outcome, delayed or nonunion of the fracture, traumatic arthritis, and chronic pain (13–17). Probing the anatomical etiologies may contribute to solving these problems.
Ulnar variance (UV), the difference in height between the joint surfaces of the distal radius and ulnar, has been regarded as an anatomical etiology for many wrist injuries. Positive UV may result in bone marrow edema, necrosis, or TFCC tears (18–20). Negative UV may play roles in the etiology of Kienbock's disease (21–23). From a biomechanical perspective, Ozer et al. concluded that an increase of >1 mm in UV was suggestive of longitudinal instability or TFCC pathology (24). However, Greybe et al. confirmed that lengthening the ulna slightly reduced the contact pressure at the distal radioulnar joint and caused a substantial decrease in contact area. Shortening the ulna had the opposite effect (25). The two studies above showed opposite results. Whether UV is the real cause of ulnar-sided wrist pain and whether there are other anatomical factors remain questions that need further etiological research.
Clinically, we found that some patients with ulnar-sided wrist pain had different pisiform-ulnar distance (PUD). The PUD of a painful wrist is relatively short, but the contralateral side without wrist pain has a longer PUD. Theoretically, a shorter PUD will increase the risk of impingement between the distal ulnar and pisiform or triquetrum, resulting in local soft or osseous structure damages and wrist pain. However, whether there is a statistical correlation between PUD and ulnar-sided wrist pain requires further research. In addition, we also found some interesting phenomena in clinical practice. Some people have a large distal ulnar volar angle (DUVA), but some have a small one. Theoretically, when performing sports activities such as vaulting, the greater the DUVA, the greater the component force transmitted to the distal ulna, the greater the load on the ulnar-wrist joint, and the greater the risk of ulnar-sided wrist injury, which may lead to ulnar-sided pain. However, further studies are needed to determine whether there is a statistical correlation between the volar angle of the distal ulna and ulnar-sided wrist pain.
The aim of the present study was to investigate the relationship between ulnar-sided wrist pain and anatomical factors including UV, DUVA, and PUD. It was hypothesized that UV was associated with ulnar-sided wrist pain only when it increased to a certain extent. The DUVA and PUD had negative correlations with ulnar-sided wrist pain.
Material and Methods
The present study was approved by the local ethics committee. Written informed consent was signed by all patients. The Medical Ethics Committee of the 980th Hospital of the PLA Joint Logistic Support Forces approved the study design (approval number: 2021-KY-52).
A total of 64 male athletes from one unit who had ulnar-sided wrist pain associated with training injuries were studied. The control group included 64 healthy male athletes from the same unit who participated in training during the same period. Patients were included if they met the following criteria: (i) patients who had acute or chronic ulnar-sided wrist pain; (ii) the ulnar-sided wrist pain was caused by athletic training; (iii) ulnar-sided wrist injuries included lunate bone contusion, TFCC injury, soft-tissue contusion, ulnar impaction syndrome, extensor carpi ulnaris tendinitis, and so on; (iv) anteroposterior and lateral wrist X-rays were available; and (v) there were no systemic diseases that involved the skeletal muscle system. Exclusion criteria included the following: (i) the location of wrist pain was not on the ulnar side; (ii) patients had suffered from distal radius, ulnar, or proximal carpal fractures; (iii) patients had received wrist, elbow, or forearm surgeries; (iv) infectious disease, tumor, or arthritis were observed in the painful wrist joints; and (v) patients had skin disturbances.
All participants had plain radiographs of the wrist joint in the posteroanterior (PA) and lateral views. UV was measured on standard PA X-ray. The standard PA X-ray was obtained with the wrist in a neutral position, elbow in 90° of flexion, and shoulder in 90° of abduction. The measurements of the PUD and DUVA were performed on lateral X-rays. Pisiform was not always easy to see. In order to clearly outline the pisiform and ulna, standard lateral X-rays must be taken with the wrist and forearm in a neutral position, the elbow in 90° of flexion, and the shoulder in 0° of abduction. The standard lateral X-ray shows that the distal ulnar and radius overlap, the angle of capitate, lunate, and radius should be as small as possible, and the palmar aspect of the pisiform is at the central third of the interval between the volar cortex of the scaphoid tubercle and the volar capitate. In addition, to further ensure the accuracy of measurement, not only do experienced radiologists need to adjust the radiation dose to improve the quality of the radiographs, but also at least two orthopedic specialists with special training were required to interpret the radiographs. Each index was measured twice with an interval of two weeks. The average of the two measurements was taken as the final value to be analyzed.
UV measured by perpendicular method was defined as the distance between carpal articular surface of the ulna and the radius. UV was classified as neutral (both articular surfaces had the same length), positive (ulnar surface is longer than radius), and negative UV (radius surface is longer than ulnar) (26) (Fig. 1a and 1b).
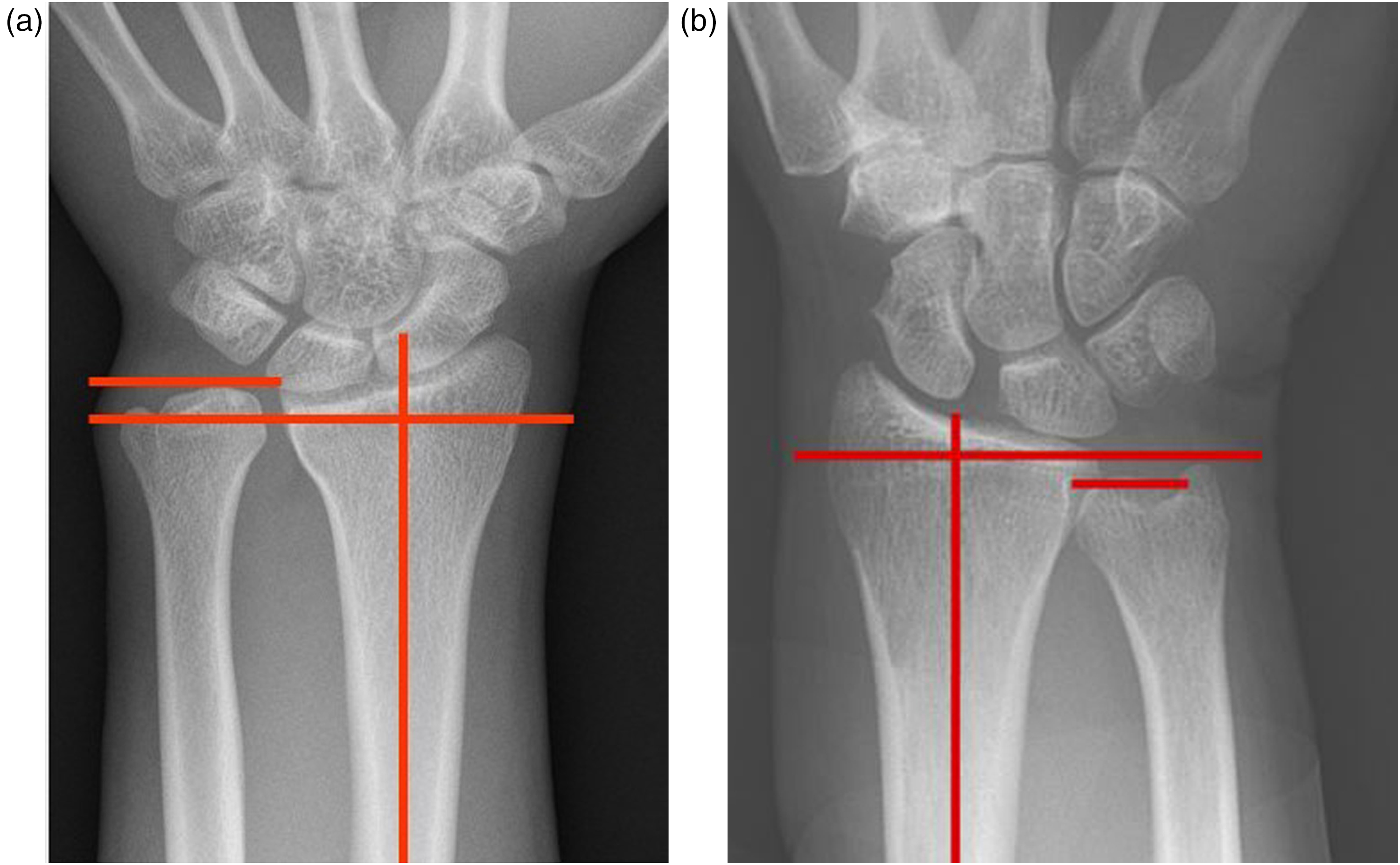
The UV measurement is shown on AP wrist X-ray of patients with (a) positive and (b) negative UV. AP, anteroposterior; UV, ulnar variance.
The PUD, a new concept, was measured on lateral X-ray. A perpendicular line (A) was first drawn through the volar rim of the pisiform, then the second line (B), parallel to line A, was outlined through the dorsal rim of the ulnar. The PUD was determined as the distance between A and B (Fig. 2).
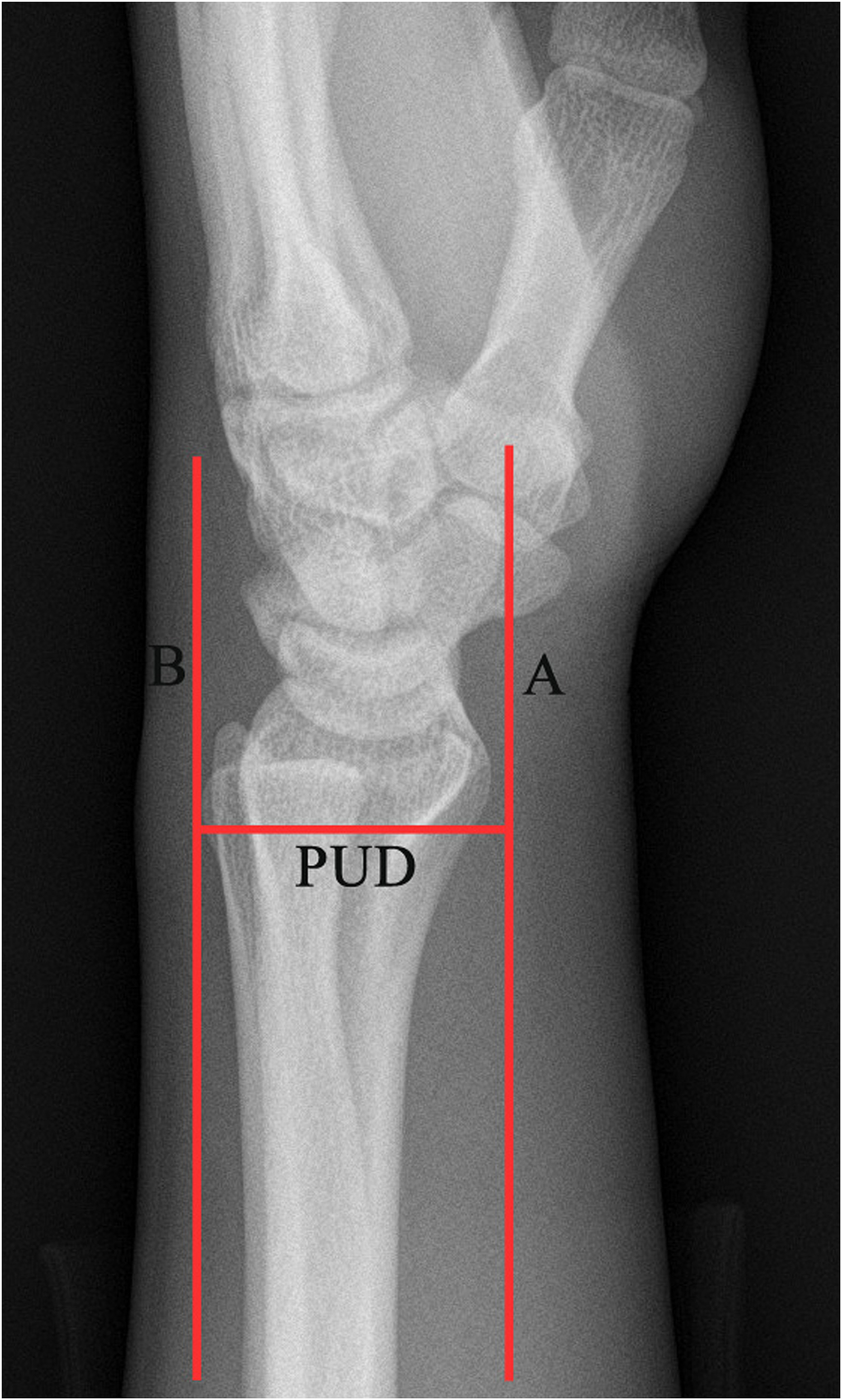
The PUD measurement is shown on lateral wrist X-ray. PUD, pisiform-ulnar distance.
The DUVA, a concept as new as PUD, was also measured on lateral X-ray. A line (C), parallel to the articular of the distal ulnar, was drawn through the most prominent point of the distal ulnar, so the ulnar was divided into proximal and distal sections. A longitudinal axis was drawn through the proximal section (D), and a longitudinal axis (E) was drawn through distal section. The angle between D and E was taken as the DUVA (Fig. 3).
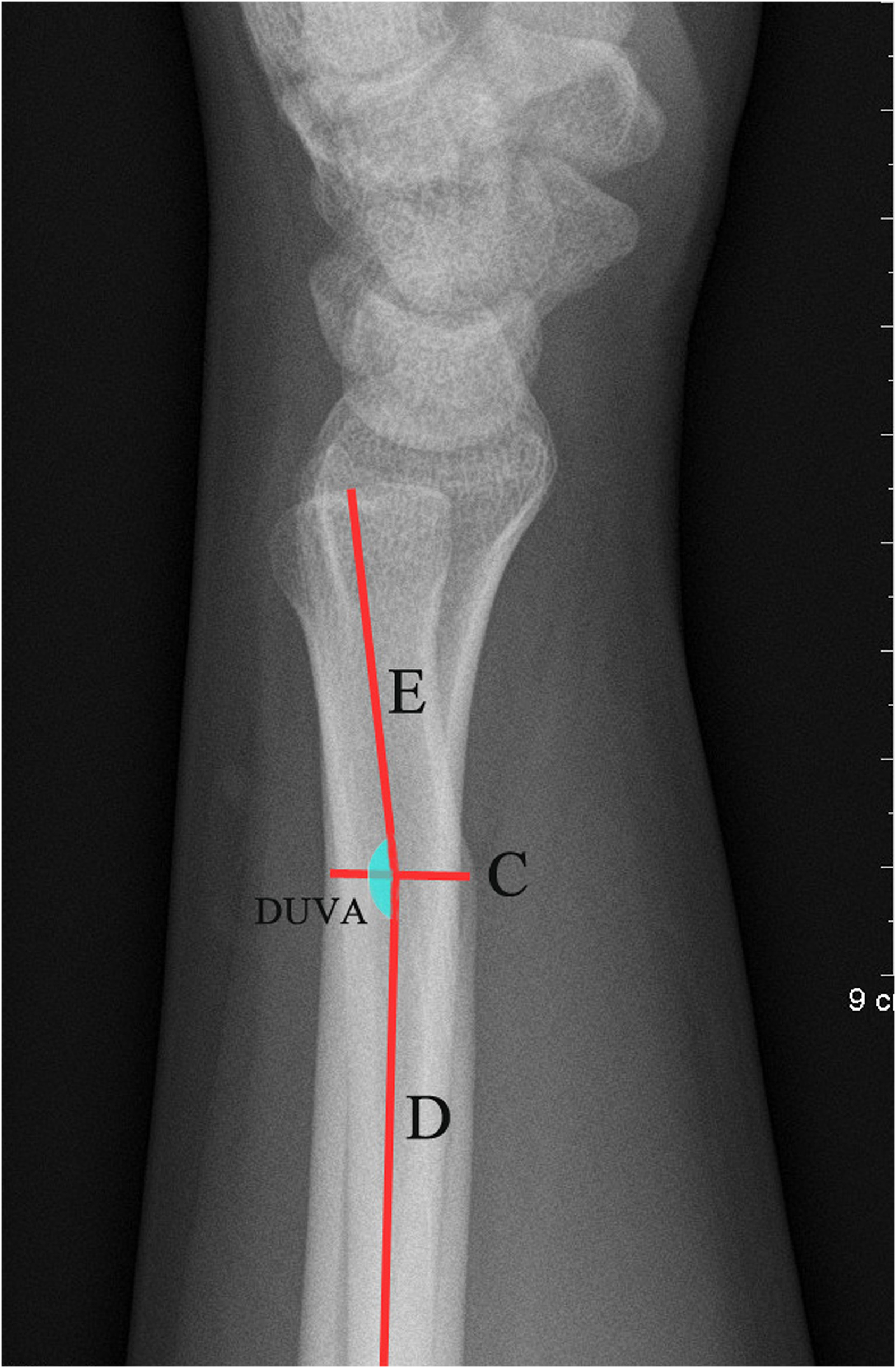
The DUVA measurement is shown on lateral wrist X-ray. DUVA, distal ulnar volar angle.
Statistical analysis
Quantitative variables were shown as mean ± standard deviation. Categorical variables were expressed as frequencies. Comparisons of quantitative variables were performed using two independent samples t-tests. Pearson’s chi-square test was used to analyze categorical variables. The binary logistic regression model was applied to analyze the association between ulnar-sided wrist pain and the three anatomical factors above including UV, PUD, and DUVA. Statistical analysis was performed with SPSS version 23.0 (SPSS, Chicago, IL, USA). Statistical significance was set at P < 0.05.
Results
The present study consisted of 64 participants with ulnar-sided wrist pain, of whom 31 were lateral wrists and 33 were right wrists. All 64 individuals had a history of athletic injury on the wrist, of which 25 were cases were injured during single- or parallel-bar training, 19 cases were doing push-ups, 12 cases were throwing events, and eight cases were basketball training. The wrist injuries included soft-tissue contusions (STCs) in 22 (34.38%) cases, TFCC injury in 12 (20.31%) cases, ulna impaction syndrome (UIS) in 8 (12.5%) cases, and other injuries in 21 (32.81%) cases. STC, TFCC injury, and UIS were the three main causes of ulnar wrist pain in the present study. In the cases of TFFC injury and UIS, the average UV were 3.14 mm and 2.29 mm, respectively, both of which were >2 mm. while in the cases of STC, the average UV was 0.27 mm, which was <2 mm. In the cases of TFCC injury, UIS, and STC, the average PUDs were 2.29 cm, 2.58 cm, and 2.55 cm, respectively, which were <2.65 cm (Table 1). The average duration from injury to visiting a doctor was 1.5 months (range = 0.5–3 months). The control group also had 64 individuals without wrist pain, of which 28 were lateral wrists and 36 were right wrists. No significant differences were observed in age, height, body weight, or body mass index between the two groups (Table 2).
The list of measurement and pathology of ulnar wrist pain group.

DRUJI, distal radioulnar joint instability; ECUT, extensor carpi ulnaris tendinitis; FCUT, flexor carpi ulnaris tendinitis; LBC, lunate bone contusion; LON, lunate osteonecrosis; LTLI, lunotriquetral ligament injury; PBC, pisiform bone contusion; STC, soft tissue contusion; TBC, triquetral bone contusion; TFCI, triangular fibrocartilage complex injury; UIS, ulnar impaction syndrome.
Basic demographic factors of the ulnar wrist pain group and control group.
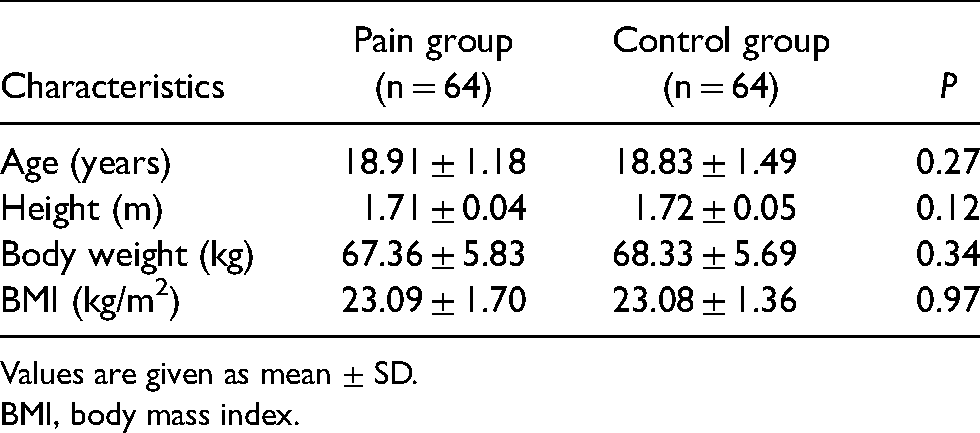
Values are given as mean ± SD.
BMI, body mass index.
The group with ulnar-sided wrist pain exhibited lower values of PUD than the control group (P < 0.05); no statistical differences were found at UV and DUVA between the ulnar-sided wrist pain group and the control group (P > 0.05). The results are presented in Table 3.
Anatomical indexes of the ulnar wrist pain group and control group.

Values are given as mean ± SD.
DUVA, distal ulnar volar angle; PUD, pisiform-ulnar distance; UV, ulnar variance.
The group with ulnar-sided wrist pain had more individuals with neutral UV and fewer individuals with negative and positive UV, but there were no statistical differences between the two groups. To further study the relationship between ulnar-sided wrist pain and positive UV, the positive UV was further classified into three subgroups: 0 mm < UV ≤ 1 mm; 1 mm < UV ≤ 2 mm; and UV > 2 mm. Statistical analysis showed that the subgroup of UV > 2 mm had more individuals than the control group (P < 0.05). The results are shown in Tables 4 and 5.
The distribution of UV of the ulnar wrist pain group and control group.
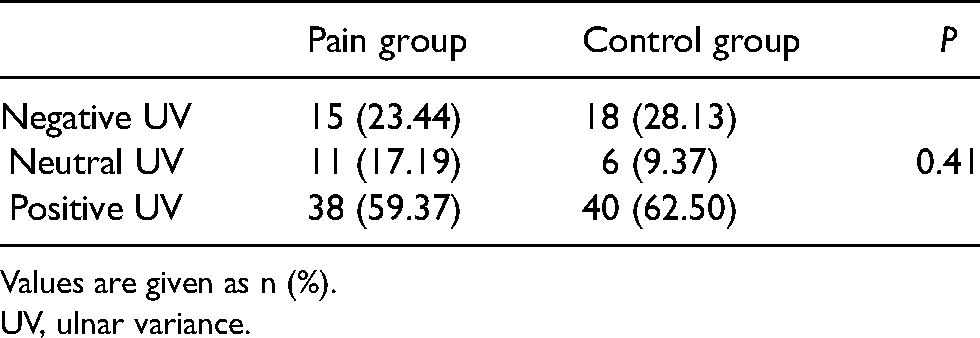
Values are given as n (%).
UV, ulnar variance.
Subgroup analysis of UV.
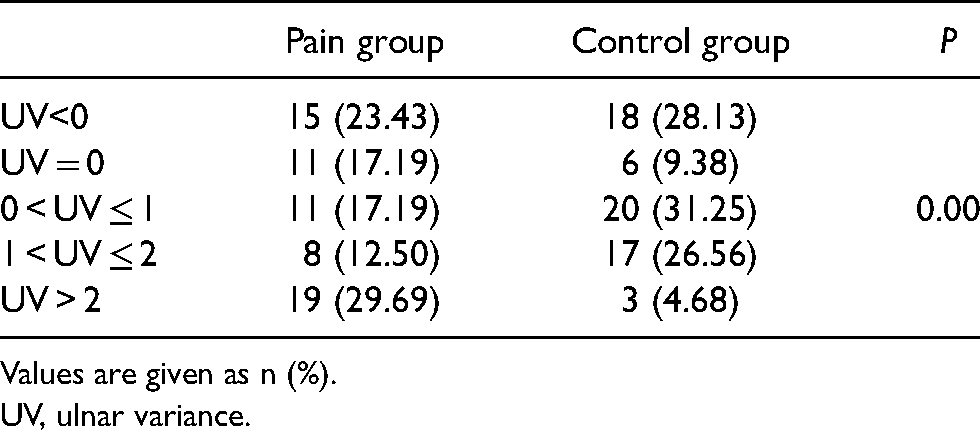
Values are given as n (%).
UV, ulnar variance.
Binary logistic regression analysis for evaluating the association between ulnar-sided wrist pain and the anatomical factors of UV, PUD, and DUVA demonstrated that PUD had statistical correlation with ulnar-sided wrist pain, it was a protective factor (odds ratio [OR] = 0.01; P < 0.001; 95% confidence interval [CI] = 0.001–0.046), the value of 2.65 cm is a cutoff point, and people with PUD <2.65 cm were at risk for ulnar wrist pain. Neither UV nor DUVA had statistical correlation with ulnar-sided wrist pain (P > 0.05). The results are shown in Table 6.
Regression analysis of correlations between anatomic indexes and ulnar wrist pain.
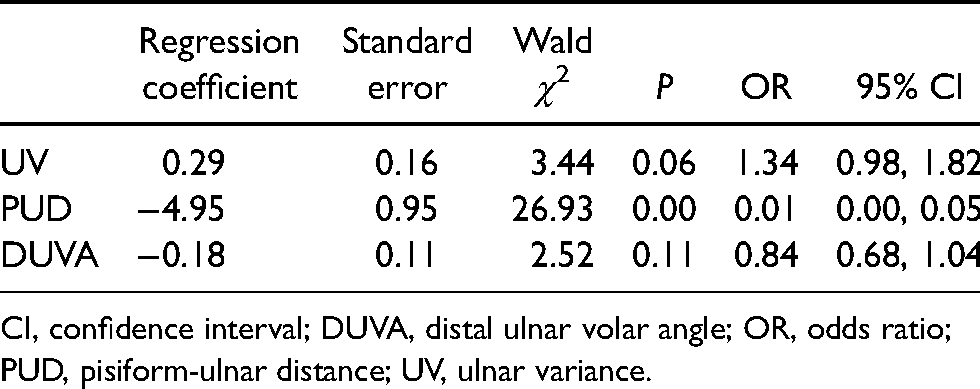
CI, confidence interval; DUVA, distal ulnar volar angle; OR, odds ratio; PUD, pisiform-ulnar distance; UV, ulnar variance.
Discussion
Positive UV can cause more axial load borne by the ulnar carpus and TFCC, increasing the risk of TFCC tear and impingement between the distal ulnar and ulnar carpus (27,28). Negative UV increases the probability of impingement between the ulnar head and lunate resulting in repetitive microtrauma of the lunate, then causing avascular necrosis of the lunate (29). Theoretically, UV should have significant correlation with ulnar-sided wrist pain. The present study demonstrates that there is no significant association between UV and ulnar-sided wrist pain. Although the difference of the proportion of UV > 2 mm between the group with ulnar-sided wrist pain and the control group had statistical significance, this significance did not remain in multivariable analysis of binary logistic regression model. The results are in accordance with the fact that not all patients with UV develop ulnar-sided wrist pain. However, we still advise the athletes with UV > 2 mm to attach importance to safeguard procedures for protecting the wrists from injuries.
Given that not all patients with UV develop ulnar-sided wrist pain, other anatomical etiological factors may be involved. Kluge et al. reported two cases of ulnar-sided wrist pain with impingement between the pisiform and ulnar styloid process after a proximal row carpectomy (30). The mechanism was that when the wrist was ulnopalmar flexion with or without a certain amount of forearm rotation, contraction of the flexor carpi ulnar muscle would apply a palmar ulnar deviation force. In the presence of proximal row carpals, the force contributed to the maintenance or stabilization of the proximal row carpals with normal PUD. In the absence of proximal row carpals, the force pushed the pisiform dorsally towards the ulnar styloid process, shortening the PUD and causing the pisiform to impinge with the ulnar styloid process, and thus the ulnar-sided wrist pain developed. The present study demonstrated that the group with ulnar-sided wrist pain had a shorter PUD than the control group. Multivariable analysis showed a negative correlation between PUD and ulnar-sided wrist pain. The mechanism might be that a shorter PUD corresponds to the dorsal movement of pisiform and triquetrum. This heightens the risk of impingement between the distal ulnar and pisiform or triquetrum with wrist flexion and/or forearm rotation. Therefore, if an athlete is found to have a PUD of <2.65 cm in a routine physical examination, he/she should pay great attention to developing ulnar-sided wrist pain and to protecting their wrists from injuries.
Clinically, we find that every patient has a different DUVA from each other, which may influence the transmission of the axial loading from the forearm to the ulnar wrist potentially causing ulnar wrist pathologies and ulnar-sided wrist pain. Nevertheless, the present study showed that the group with ulnar-sided wrist pain indeed had a different average value of DUVA with the control group; however, the difference had no statistical significance. Further research may be needed to confirm the results.
The present study has some limitations. One limitation is that the study only involved male athletes with ulnar-sided wrist pain and did not consider female athletes and the common population with ulnar-sided wrist pain. This confines the applicability of the results. Another limitation is that the sample of the study was not very large. The negative results, including the correlation of ulnar-sided wrist pain and UV and the relationship between ulnar-sided wrist pain and DUVA, are needed to be further confirmed by studies with larger samples.
In conclusion, the PUD has a significant correlation with ulnar-sided wrist pain. It is an anatomical protective factor. UV and the DUVA both have no statistical association with ulnar-sided pain, but their potential pathogenic effects on wrists cannot be ignored. Further studies are needed to confirm the results.
Footnotes
Acknowledgements
We thank Professor Qian Yuhang of the orthopedic department for his support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was granted by PLA Logistics scientific research project (Grant No. 19LBJ1005A) and supported in part by Key Research and Development Project of Hebei Province (Grant No. 21377758D) and Hebei medical science research project plan (Grant No. 20210557).