
Abstract
The portal vein is the largest vessel supplying the liver. A number of radiological interventions are performed through the portal vein, namely for primary pathologies of the portal vein, for inducing liver hypertrophy or to treat the sequelae of portal hypertension among others. The routes used include direct transhepatic, transjugular, and, uncommonly, trans-splenic and through subcutaneous varices. Portal vein embolization and transjugular intrahepatic portosystemic shunt are among the most common portal vein interventions that are performed to induce hypertrophy of the future liver remnant and to treat complications of portal hypertension, respectively. Other interventions include transhepatic obliteration of varices and shunts, portal vein thrombolysis, portal vein recanalization, pancreatic islet cell transplantation, and embolization of portal vein injuries. We present a detailed illustrative review of the various radiological portal vein interventions.
Keywords
Introduction
The portal vein (PV) is a large hepatic vascular structure supplying 70%–80% of the blood to the liver (1). The portal vein can provide safe access for a wide variety of vascular interventions in treating many diseases that may or may not affect the PV itself (2,3). Most of these procedures are required for chronically sick patients with underlying liver disease, ascites, and malignancy thereby increasing the risk of complications of these interventions. This calls for a cautious approach and highly skilled interventional radiologist. This pictorial review comprehensively discusses the various radiological interventions that are performed through the PV (Table 1).
List of radiological interventions performed through portal vein.
Approaches for PV access
There are various routes to access the PV. The most commonly used routes include the transhepatic and transjugular routes (3).
In the transhepatic route, a peripheral branch of the PV is directly punctured using a 21/22-G needle under ultrasound guidance followed by wire and sheath placement. Once the required intervention is performed, the tract is embolized using coils, gelfoam, or n-butyl cyanoacrylate (NBCA).
In the transjugular route, the central segment of the PV is punctured through fluoroscopy (using wedge venography or wire marker in the PV) or ultrasound guidance (transabdominal or intravascular). Once inside the PV, the planned procedure is performed. This procedure is safe in the presence of ascites.
The trans-splenic approach to access the PV is an infrequently used technique for PV interventions (4,5). This route is used when the extra or intrahepatic PV is narrowed or blocked or when the transjugular or transhepatic route is infiltrated by tumors (5). A peripheral branch of the splenic vein is punctured with a 21/22-G needle under fluoroscopy or ultrasound guidance (4,5). Once the access is established, the required PV intervention is performed. The tract is then embolized using gelfoam slurry or NBCA-lipiodol.
The transhepatic or trans-splenic route is avoided in the presence of moderate to severe ascites due to a higher risk of bleeding complications from the puncture site. With the trans-splenic route, the incidence of intraperitoneal bleeding is in the range of 6.5%–27% (4,5). The use of anticoagulation during the procedure increases the risk. It can be reduced by embolizing the tract. In cases of post-procedure bleeding, management varies from close monitoring to embolization depending on the severity (3). Bile leak may also occur, which is managed by percutaneous aspiration or drainage of biloma (3).
Other uncommon routes to access the PV include transmesenteric vein (requires minilaparotomy) and through recanalized para-umbilical vein and para-stomal varices (6,7).
Portal vein embolization
Portal vein embolization (PVE) is a well-established procedure performed to increase the volume of the future liver remnant (FLR) before major liver resection with the aim of decreasing the risk of developing acute liver failure postoperatively (8). With the increasing incidence of hepatobiliary malignancies and improved surgical techniques employed in their management, patients are frequently offered curative surgical treatment, which often necessitate excision of large volumes of the healthy liver parenchyma to achieve negative margins. Even though multiple factors are responsible for liver failure after hepatic surgeries, the volume of FLR has been shown to be an independent predictor (9). Preoperative PVE provides an opportunity to perform extensive hepatic surgeries with curative intent.
The pathophysiology of hypertrophy after PVE is based on the regenerative capacity of hepatocytes (hyperplasia or true increase in cell number) after injury by toxins, trauma, or vascular occlusion (10). Both hemodynamic (increased portal blood flow to non-embolized liver) and metabolic (trophic factors from hepatic and extrahepatic sources) changes trigger the regenerative process in the liver (11). However, patients with poor hepatic reserve (fatty liver or cirrhosis) show poor response to portal blood flow changes and metabolic factors compared to patients with normal liver and require more time for regeneration (12). Once PVE is performed, hepatocyte regeneration occurs at the rates ranging from 21 cm3/day at two weeks to 11 cm3/day at four weeks (13). Major liver resection is usually planned after 4–6 weeks, since no significant hypertrophy is seen after six weeks (10).
Indications and contraindications
The indications of PVE are primary or secondary hepatic malignancies requiring extensive hepatic resection and with insufficient volume of FLR. Insufficient FLR is defined as computed tomography (CT) volume <20% in normal livers, <35% in steatohepatitis or on chemotherapy, and <40% in cirrhosis (14). The relative contraindications include involvement of PV by tumor and coagulation disorders (10). Biliary drainage of the FLR is necessary if there is biliary obstruction, as it affects liver hypertrophy (15). Cross-sectional imaging with multiphase CT scan or magnetic resonance imaging are used to define the tumor and its resectability, the volume of FLR, anatomic variations of the PV, and contraindications to the procedure.
Procedure
PVE is performed through a percutaneous transhepatic approach, either ipsilateral (through the lobe of liver requiring PVE) or contralateral (through the FLR) (Fig. 1) (16). The former approach is frequently preferred to avoid injury to the PV branch of the FLR. This approach may be technically challenging, mainly because of the acute angulation of segmental branches, which may necessitate the use of reverse curve catheters (Fig. 2) (16). Furthermore, traversing through the tumor should be avoided. Uncommonly, a trans-splenic approach may also be performed safely when the ipsilateral route is challenging (17). Irrespective of the approach of gaining access into the PV, the steps of the procedure remain the same. After puncturing a peripheral branch of PV, access is secured by a vascular sheath. A diagnostic portogram is performed to define the anatomy and to provide a roadmap for embolization. Subsequently the branches are selectively catheterized and embolized using standard or microcatheters. Finally, the percutaneous tract is embolized with coils, gelfoam, or glue.

(a, b) PVE with contralateral approach in a 50-year-old man with HCC. (a) Initial portogram. (b) Portogram after PVE with glue and vascular plug (arrow). (c–f). PVE with ipsilateral approach in a 37-year-old man with hilar cholangiocarcinoma, planned for right extended hepatectomy. (c) Initial portogram. (d) Portogram after PVE with glue. (e) Pre-embolization volume of future liver remnant was 210 mL (16% of total), which increased to 356 mL (27%) after four weeks of PVE (f). HCC, hepatocellular carcinoma; PVE, portal vein embolization.
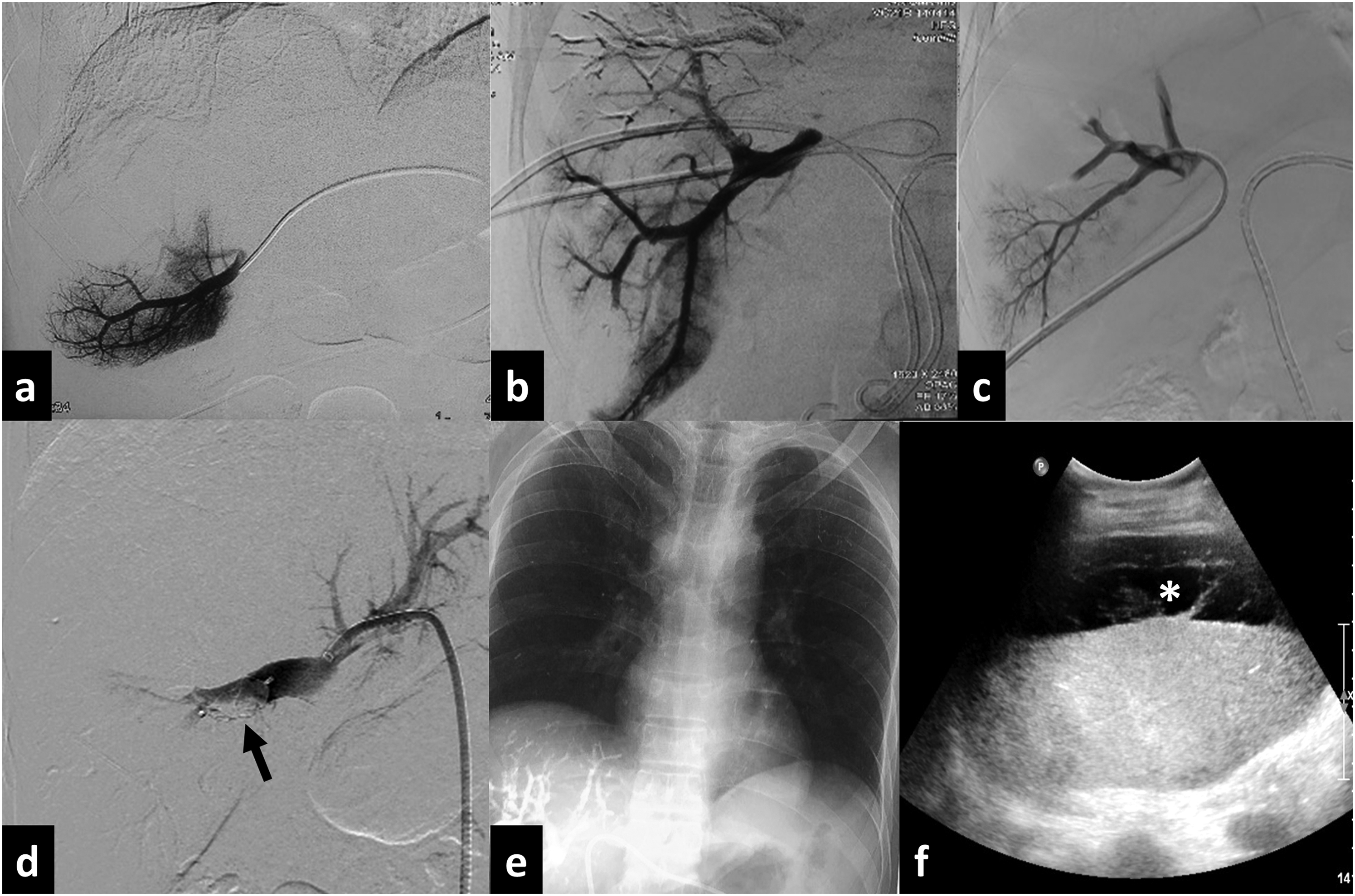
PVE. (a) Branch portogram with contralateral approach using forward curve catheter. (b) Branch portogram with ipsilateral approach using reverse curve catheter (arrow). (c) Branch portogram with ipsilateral approach using forward curve catheter. (d) Portogram after PVE using polyvinyl alcohol particles and vascular plug (arrow). (e) Chest radiograph after PVE showing reflux of glue into pulmonary arterial branches due to inadvertent puncture of right hepatic vein. (f) Ultrasound image one day after PVE shows perihepatic hematoma (asterisk). PVE, portal vein embolization.
Various embolic agents used in PVE include gelatin sponge, polyvinyl alcohol (PVA) particles, N-Butyl cyanoacrylate (NBCA), microspheres, absolute ethanol, ethylene vinyl alcohol copolymer, and metallic coils (Figs. 1 and 2d) (11,18). A recent review indicated that NBCA and absolute alcohol resulted in more hypertrophy than other agents (18). However, alcohol injection requires occlusion balloon catheters to avoid reflux (13). Luz et al. showed that NBCA produced significantly higher and faster hypertrophy than PVA particles with coils (absolute hypertrophy of FLR: 57% vs. 37% at four weeks) (19). Combination of agents like PVA and coils or vascular plugs also have been shown to induce significantly higher hypertrophy of FLR than particles alone (20). Care should be taken while injecting embolics, especially after near total occlusion of target branch, to prevent inadvertent non-target embolization of PV radicles of FLR. Occlusion balloon catheters may help in avoiding this complication.
Complications and outcomes
The technical success rate is close to 100% (21). PVE is considered a safe procedure. Guidelines recommend rates of <25% for minor and <5% for major complications as acceptable (15,16). Transient derangement in liver function tests is encountered in approximately 50% (11). The complications may be related to puncture or embolization (Fig. 2e and 2f). Puncture-related complications include vascular injuries leading to hepatic arterial pseudoaneurysm, arterio-venous fistula or venous leak (hepatic or portal vein), and bile leak due to intrahepatic or extrahepatic bile duct injury. The latter may cause biliary peritonitis or biloma. Embolization-related complications include migration and non-target embolization of embolics, parenchymal infarction, abscess, and portal hypertension. The outcomes of some of the studies of PVE are shown in Table 2.
Details and outcomes of studies on portal vein embolization.
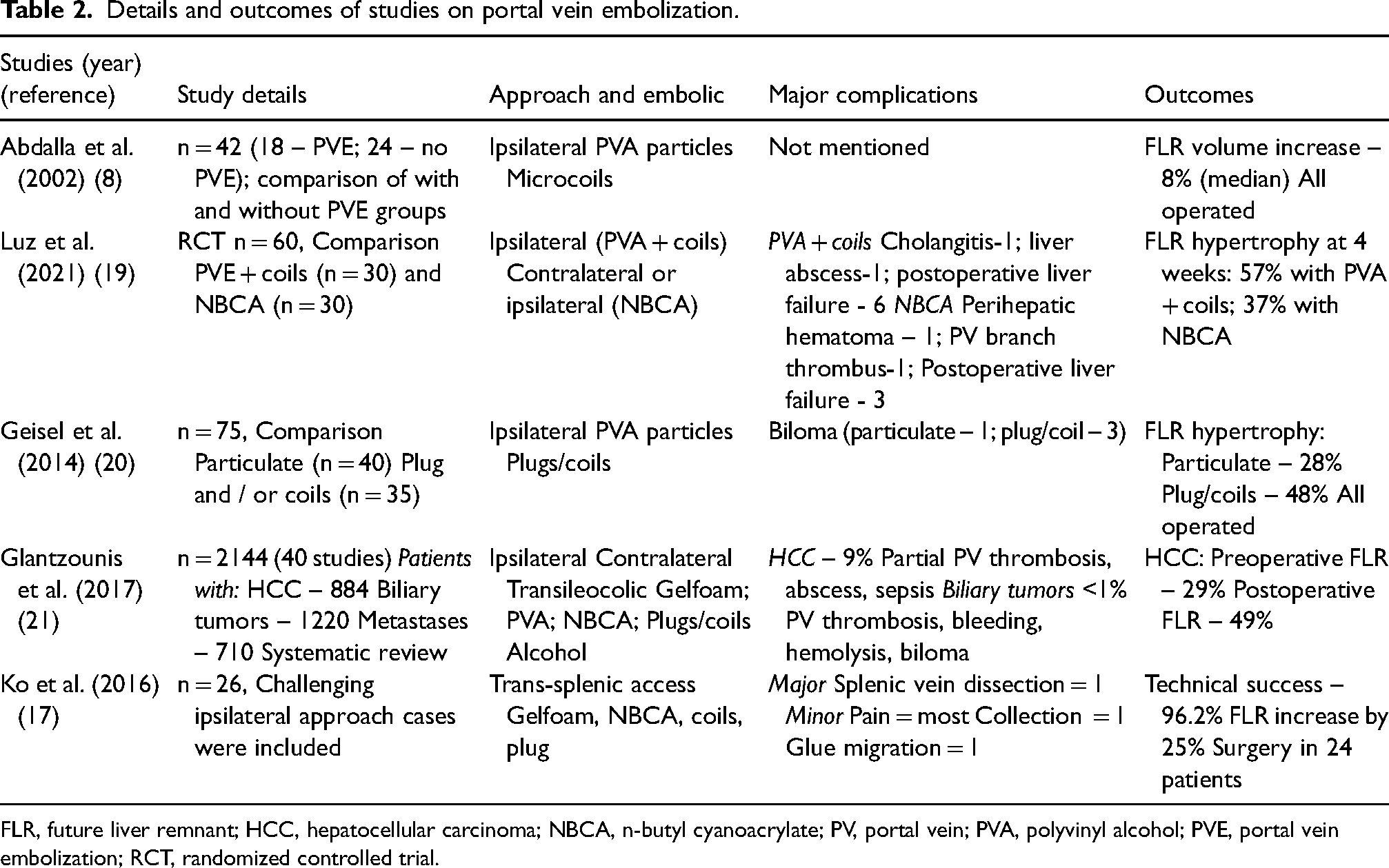
FLR, future liver remnant; HCC, hepatocellular carcinoma; NBCA, n-butyl cyanoacrylate; PV, portal vein; PVA, polyvinyl alcohol; PVE, portal vein embolization; RCT, randomized controlled trial.
Modified techniques in PVE
In patients where the hypertrophy of the FLR is insufficient after the standard PVE, few modifications or additional procedures have been suggested to improve hypertrophy (16) (Table 3). Additional hepatic arterial or hepatic vein embolization can improve hypertrophy of the FLR due to the additional incited inflammatory response (22). In cases of hepatocellular carcinoma, transarterial chemoembolization followed by PVE improves the feasibility of major hepatic resections by inducing significantly higher hypertrophy (23,24). Selective hepatic vein embolization of the tumor bearing liver using coils or vascular plugs has also been shown to improve hypertrophy (25). Embolization of segment 4 of the PV is another strategy that could improve hypertrophy (26). However, the clinical benefit of this additional step is doubtful. Another novel approach to improve FLR hypertrophy is to infuse autologous bone-marrow derived stem cells into the FLR (27,28).
Details and outcomes of studies on modified techniques of portal vein embolization.
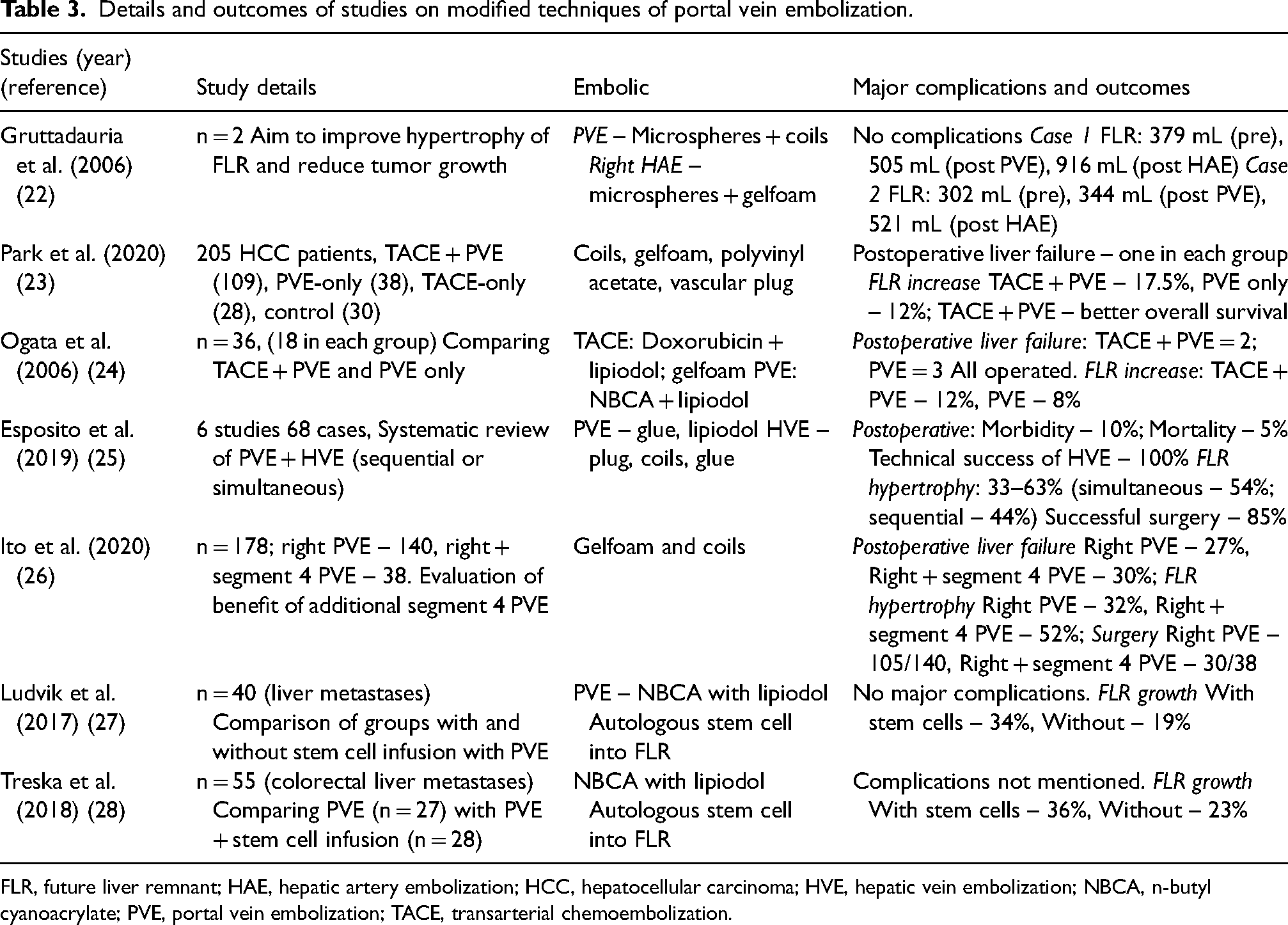
FLR, future liver remnant; HAE, hepatic artery embolization; HCC, hepatocellular carcinoma; HVE, hepatic vein embolization; NBCA, n-butyl cyanoacrylate; PVE, portal vein embolization; TACE, transarterial chemoembolization.
Transjugular intrahepatic portosystemic shunt
Transjugular intrahepatic portosystemic shunt (TIPS) is a minimally invasive interventional procedure performed to reduce portal pressure in patients with portal hypertension, thereby reducing the incidence of potentially life-threatening complications such as variceal bleeding and ascites (29). This procedure consists of a creation of a side-to-side shunt between the intrahepatic portions of the hepatic vein (HV) and the PV. This diverts the blood from the mesenteric circulation into the systemic circulation and reduces the portal pressure by about 50% (30). In addition, TIPS results in other hemodynamic changes like increased central blood volume and cardiac pressures, increased renal perfusion, and increased compensatory hepatic arterial flow. These changes result in improvement of ascites, renal function, and hepatorenal syndrome, and reduction of intestinal bacterial translocation and systemic inflammation (30). At the same time, there is hepatic hypoperfusion due to the shunt, which leads to the deterioration of the liver function and may compound the risk of developing hepatic encephalopathy (HE) caused by the shunt.
Indications and contraindications
Two most common indications of TIPS are uncontrolled acute variceal bleeding and recurrent ascites (30). In cases of variceal bleeding, TIPS is indicated when the bleeding is not controlled by medical and endoscopic methods (rescue TIPS), there is rebleeding within five days, there is failure of secondary prophylaxis by drugs and endoscopy, and as an initial procedure (early TIPS) in patients with acute bleeding and high risk of treatment failure (Child-Pugh B with active bleeding or Child-Pugh C with score <14) (31). Other indications include Budd-Chiari syndrome, hepatorenal syndrome, hepatic hydrothorax, and PV thrombosis (when clubbed with PV thrombolysis) (30,31).
The absolute contraindications for TIPS include cardiac failure, pulmonary artery hypertension, undrained biliary obstruction, systemic sepsis, multiple hepatic cysts, and tumor between HV and PV (30,31). Relative contraindications are severe renal failure, serum bilirubin>3 mg/dL, persistent or recurrent HE, model for end-stage liver disease (MELD) score >18, coagulopathy, and chronic PV thrombosis.
Procedure
The procedure is performed through the internal jugular vein, preferably the right. Initially, the right HV is cannulated with an angled catheter (Fig. 3). Subsequently, an angled sheathed metallic cannula is inserted over a stiff guidewire into the right HV. Then, the direction of the cannula is adjusted towards the right PV (the target being 1 cm distal to the bifurcation of main PV). This is often performed with the help of a transabdominal or infrequently with intravascular ultrasound (IVUS) or by wedged hepatic venography using iodine contrast or carbon dioxide (31).
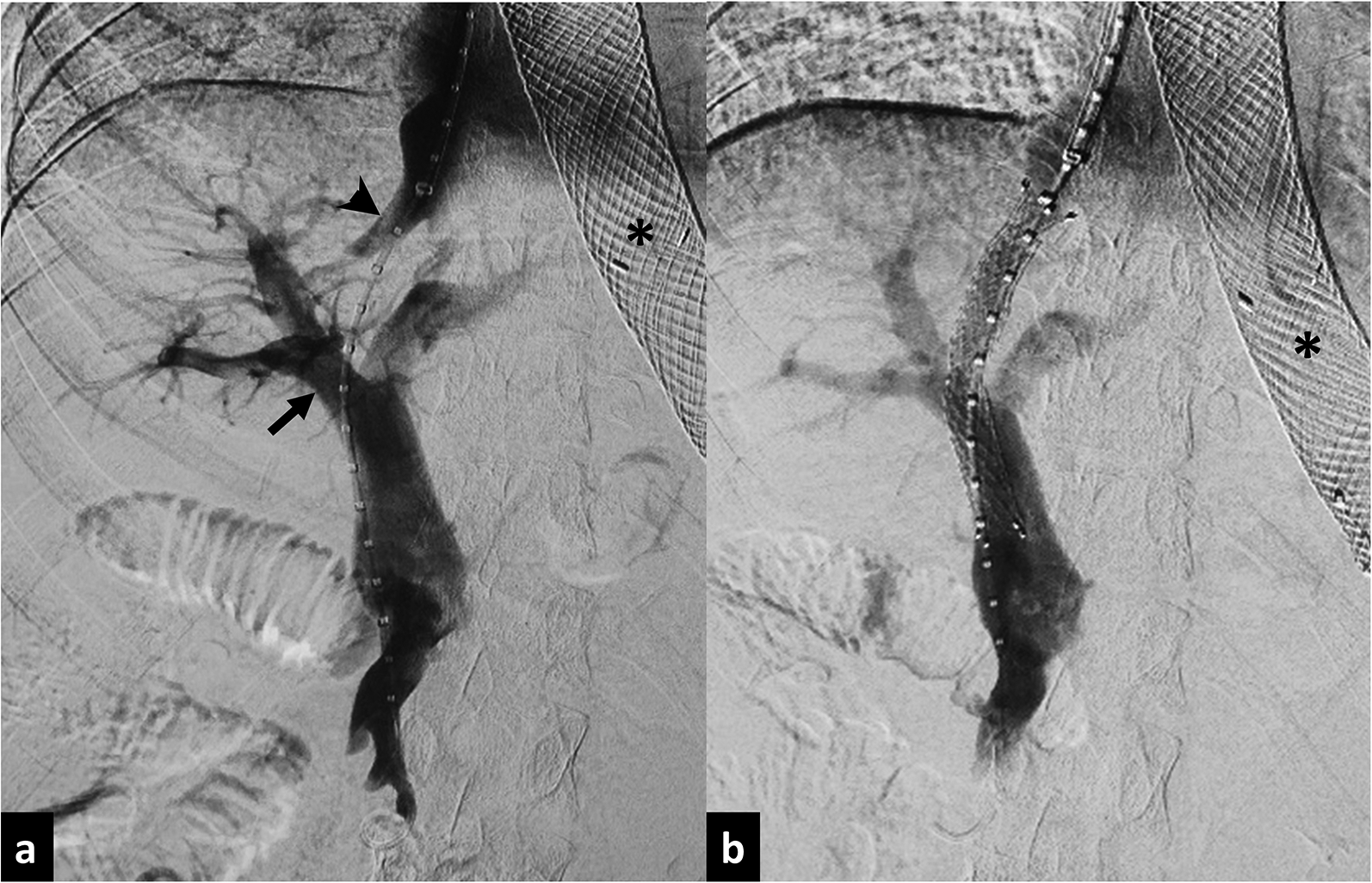
TIPS. A 50-year-old man with alcoholic cirrhosis presenting with uncontrolled hematemesis and requiring emergency TIPS. (a) Portogram after entering the PV shows the tract between the right hepatic vein (arrowhead) and right PV (arrow). (b) Final portogram after placement of stent. Asterisk: covered stent in the gastroesophageal junction placed to control incessant bleeding from esophageal varices. PV, portal vein; TIPS, transjugular intrahepatic portosystemic shunt.
Then a stylet-catheter is inserted into the cannula to puncture the right PV through the liver parenchyma. The main PV or left PV may also be punctured in difficult cases. After entering the PV, the liver tract is dilated with a balloon catheter (8–12 mm diameter) followed by insertion of a hybrid stent (covered-uncovered) or overlapping covered and uncovered stents (8–12 mm diameter). The covered portion of the stent is positioned in the liver parenchyma and the uncovered segment in the PV. Pressure gradient between the PV and HV or inferior vena cava (IVC) is measured before and after the procedure. The target gradient is usually 5–12 mmHg. In cases of Budd-Chiari syndrome, the HV are chronically thrombosed and a direct intrahepatic portosystemic shunt is performed (Fig. 4a and 4b). Here, the right PV is targeted through the supra or intrahepatic IVC directly.
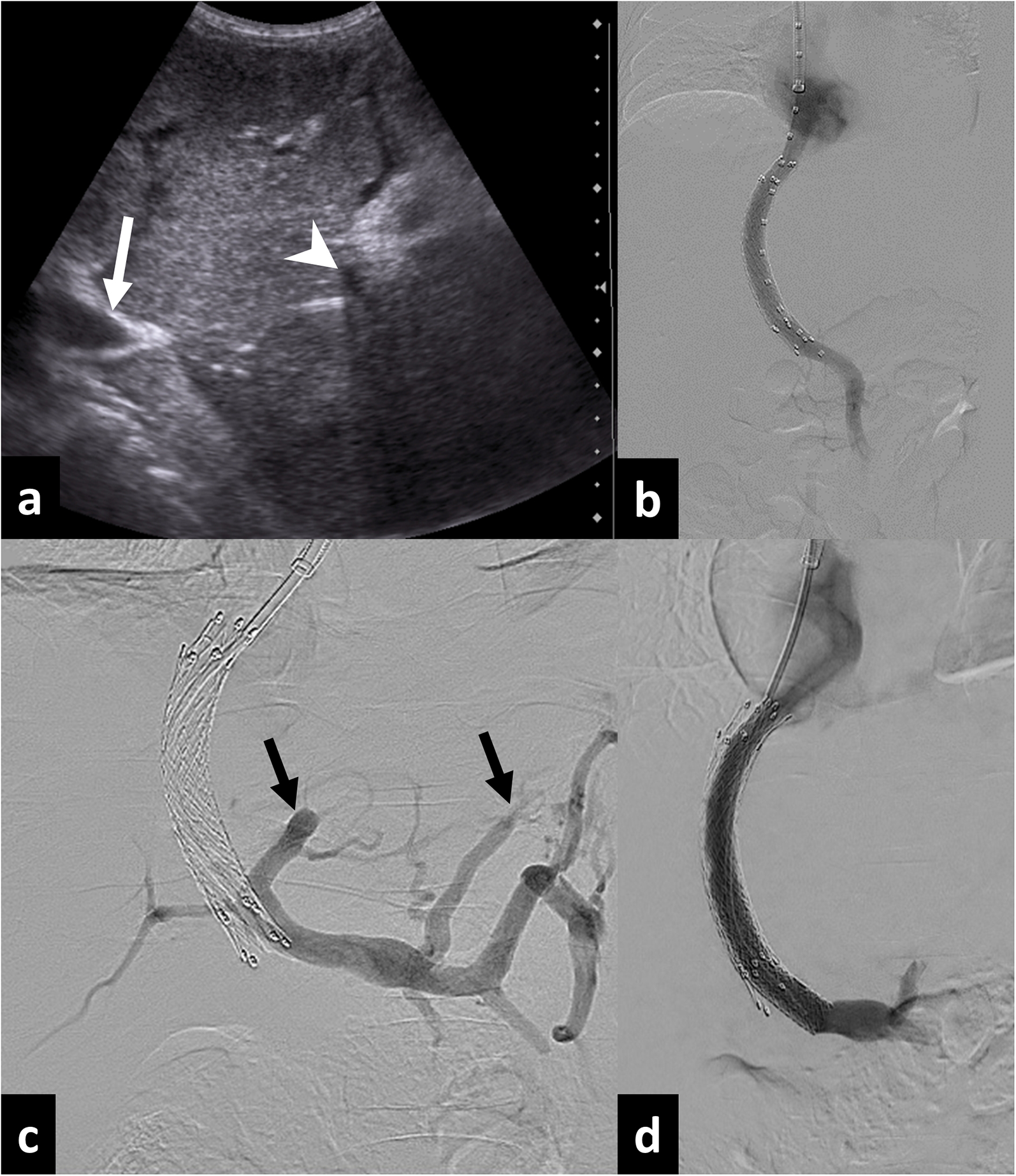
DIPS in a 5-year-old patient with chronic Budd-Chiari syndrome. (a) Transabdominal ultrasound image showing needle passed from inferior vena cava (arrow) to the right portal vein (arrowhead). (b) Final portogram after stent placement. (c, d) The follow-up color Doppler ultrasound image after one year showed thrombosis in the stent. (c) Portogram after traversing the stent shows complete occlusion of the stent with prominent collaterals (arrows). (d) Portogram after balloon dilatation and overlapping stent placement restored patency. DIPS, direct transjugular intrahepatic portosystemic shunt.
Complications and outcomes
The intra-procedure complications include liver capsule perforation, extrahepatic PV puncture, intraperitoneal bleeding, liver laceration, hepatic artery injury, biliary injury, neck hematoma, cardiac arrhythmias, and pneumothorax. The incidence of these complications are in the range of 0.5%–4.3% (32). Complications developing after the procedure include stent dysfunction due to stenosis at PV or HV end or thrombosis (Fig. 4c), HE, cardiac overload, and liver dysfunction. Shunt thrombosis requires revision, which involves mechanical thrombectomy and identification of the cause, which often requires placement of an overlapping stent (Fig. 4d). The incidence of HE is in the range of 15%–48% (33). In most patients, medical management with branched chain amino acids, lactulose, and rifaximin is successful.
Shunt reduction may be necessary in refractory cases of HE (34). Methods of shunt reduction include the following: (i) parallel placement of a balloon-mounted stent and a stent graft in which the latter is constrained by the stent; (ii) placement of a constrained stent graft, constrained by either a suture or by incomplete balloon inflation; and (iii) placement of a tapered stent graft (34). Occasionally, complete occlusion may be necessary. Maleux et al. performed shunt reduction by the parallel technique and reported improvement in symptoms of encephalopathy in 76% of patients (35). In a study by Fanelli et al., TIPS shunt reduction by an hourglass-shaped balloon expandable stent graft resulted in rapid improvement of encephalopathy (mean time = 22.3 h) and no recurrence after a mean follow up of 73.9 weeks (36). One patient required dilatation of the stent-graft due to ascites. The outcomes of TIPS are described in Table 4.
Details and outcomes of studies on transjugular intrahepatic portosystemic shunt.
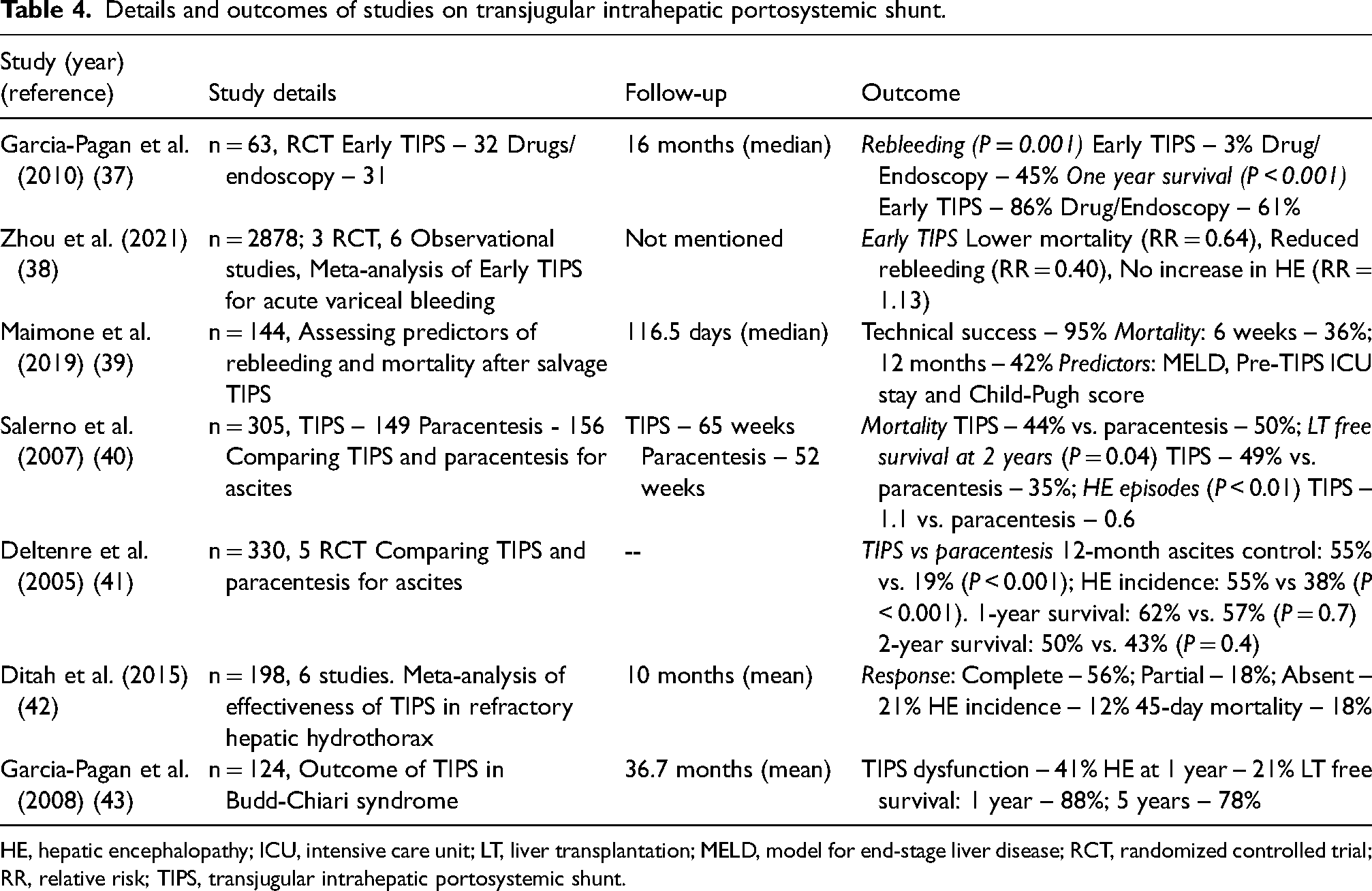
HE, hepatic encephalopathy; ICU, intensive care unit; LT, liver transplantation; MELD, model for end-stage liver disease; RCT, randomized controlled trial; RR, relative risk; TIPS, transjugular intrahepatic portosystemic shunt.
Although MELD score is used as a prognostic predictor of TIPS, a large recent study showed survival benefit of early TIPS with acute variceal bleeding even with a MELD score >19 (44). Hence, the role of the MELD score is still controversial.
Modified techniques of TIPS
IVUS assists in puncturing the PV when a transjugular route is used (45,46). The IVUS catheter, when positioned in the retrohepatic IVC through the femoral vein, shows the HV and PV thereby assisting in the puncture. A catheter with lower frequency (5–10 MHz) allows better visualization of pericaval tissues. IVUS results in a significantly reduced number of needle passes, contrast medium usage, radiation dose, and procedure time (46).
Another technique assisting in PV puncture is the use of a transhepatic PV wire (47). This step helps in targeting the PV fluoroscopically during TIPS leading to decreased fluoroscopy and procedure times. Haskal et al. described the “gun-sight” technique as an option in patients with small or occluded HV (48). Here, two snares are placed, one each in the PV and IVC. Then, a puncture is made through the snares and wire pulled from the caval side. Another type of transhepatic TIPS is the “double wire technique” described by Yu et al. (49). Here, the right PV and right HV are punctured in line, transhepatically, and the wire is snared through jugular route. This is followed by placement of another wire through the jugular route into the PV.
An additional step during TIPS is variceal embolization. Although there are no current recommendations, varix embolization with TIPS reduces the incidence of recurrent bleeding (50). Although dependent on the operator, one study suggested variceal embolization when they are opacified after TIPS or when the pressure gradient is >12 mmHg (51).
In some patients, the portosystemic pressure gradient remains high even after TIPS and the symptoms persist (52). In such cases, a second or parallel TIPS may be performed. In this procedure, another TIPS stent is placed from the right HV or IVC to the PV. This procedure is effective in further reducing the portal pressure and the symptoms (52). Parallel TIPS has also been performed safely and effectively in patients who have TIPS dysfunction (53).
Balloon-occluded retrograde transvenous obliteration (BRTO)
BRTO is an interventional procedure performed to embolize bleeding gastric varices that cannot be managed by endoscopy with sclerotherapy and large shunts causing recurrent HE (54,55). However, a standard BRTO, usually requires the presence of one or two large efferent vein of the gastric varices, typically the gastrorenal shunt, which is accessed through the jugular or the femoral veins (54). When there is no gastrorenal shunt or when the standard BRTO fails, the gastric or ectopic varices may be accessed transhepatically through the PV (percutaneous transhepatic obliteration [PTO]) or through the TIPS stent and the efferent or afferent veins or both may be occluded successfully by BRTO and balloon-occluded antegrade transvenous obliteration (BATO), respectively (56).
Anatomy of gastric or ectopic varices
The gastric varices are considered a high-volume, high-pressure system and are usually seen in patients with liver cirrhosis. They may also be associated with splenic vein thrombosis (left-sided or sinistral portal hypertension). In patients with cirrhosis, the afferent veins of gastric varices are the left, posterior, and short gastric veins, and the efferent channel is mainly the gastrorenal shunt and, uncommonly, gastrocaval and gastrophrenic shunts (56). In splenic vein thrombosis, the short gastric veins are the afferent and the left and right gastric veins and the gastroepiploic veins become the efferent vein, bypassing the thrombosed segment of the splenic vein (57). In ectopic varices, depending on the location, one of the PV tributaries becomes the afferent channel and the efferent vein drains into the systemic circulation through single or multiple veins (58). A good-quality pre-procedure CT portography is necessary for a detailed analysis of the venous structures and appropriate planning (59).
Procedure
The initial steps to access the PV is similar to that of PVE (for PTO) or TIPS. Through the PV, the target vein(s) is identified and a standard or balloon occlusion venogram is performed to outline the venous anatomy and flow dynamics (Fig. 5). This procedure typically involves antegrade occlusion of the afferent veins (usually the left, posterior, and short gastric veins) of the gastric varices (BATO). The smaller veins are occluded by coils and the largest vein is balloon-occluded followed by injection of sclerosant (56). The sclerosants commonly used include ethanolamine oleate, sodium tetradecyl sulphate, polidocanol, and sometimes NBCA. This method may be combined with the standard BRTO through the systemic venous route for better results (60). The transhepatic or trans-TIPS route may also be used for the treatment of large varices associated with HE (Fig. 6) (58). In cases of bleeding gastric varices due to chronic splenic vein thrombosis, a transhepatic BRTO may be performed through the efferent left gastric vein, if this only partially accounts for drainage of the spleen (61).
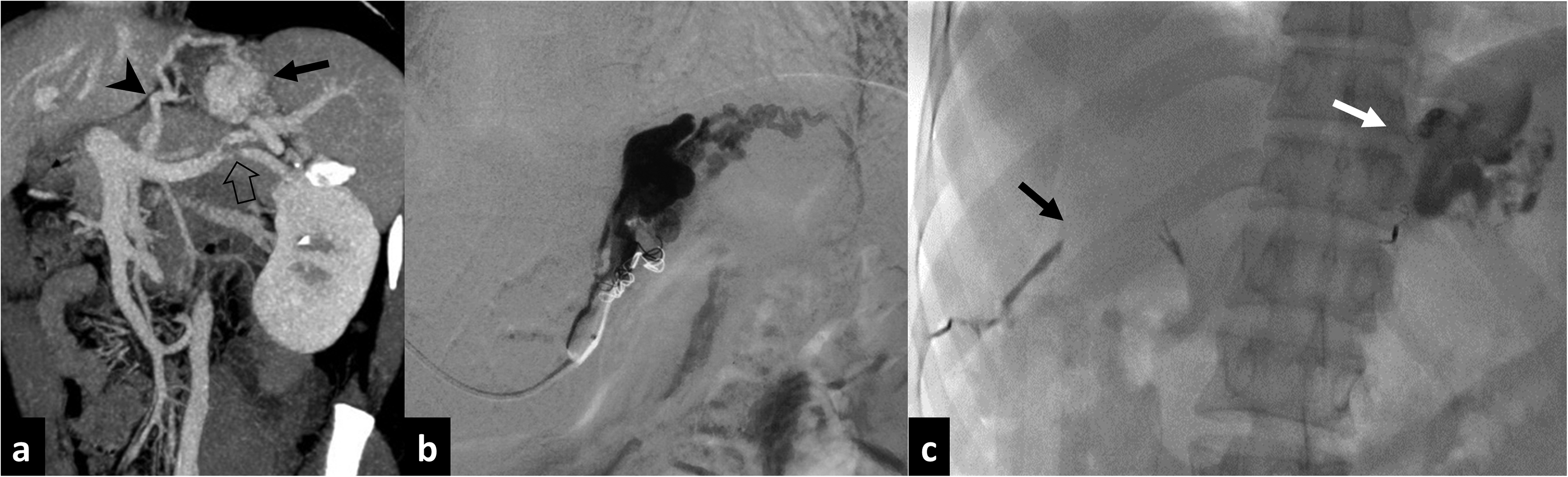
Transhepatic variceal obliteration in a 33-year-old woman presenting with hematemesis due to gastric fundal varices developing as a result of chronic splenic vein thrombosis. (a) Coronal maximum intensity projection CT image shows stenosis in the mid splenic vein (block arrow) with gastric fundal varices (arrow) draining into left gastric vein (arrowhead). There was no gastrorenal shunt. (b) Transhepatic balloon-occluded venogram of the left gastric vein shows the varices. (c) Fluoroscopy spot after the procedure shows the sclerosant (sodium tetradecyl sulphate with ethiodized oil) in the gastric varices (white arrow) and gelfoam used to embolize the transhepatic tract (black arrow). CT, computed tomography.

(a, b) TIPS with transjugular obliteration of varices in a 33-year-old man with chronic viral hepatitis and cirrhosis, presenting with recurrent hematemesis. (a) Portogram after TIPS stent placement shows persistence of gastroesophageal varices (arrows). (b) Portogram after embolization with microcoils (arrow) and glue (arrowheads) showing complete occlusion of the varices. (c, d) Transhepatic obliteration of portosystemic shunt in a 20-year-old man with cirrhosis and presenting with recurrent hepatic encephalopathy. (c) Volume-rendered image of CT portogram shows two large dilated and tortuous paraumbilical portosystemic shunts (arrows) arising from left portal vein and draining into the external iliac vein. (d) Transhepatic portogram (lateral view) of left portal vein after occlusion of the shunts with vascular plugs (arrows) and coils (arrowhead) showed reduced distal flow. The shunt was completely thrombosed at follow-up ultrasound after one month. CT, computed tomography; TIPS, transjugular intrahepatic portosystemic shunt.
Complications and outcomes
Few studies have shown PTO to be a relatively safe procedure. Two important complications are aggravation of esophageal varices (14%–68%) and increase in ascites (0%–44%) (55). The former is mostly managed by endoscopic therapy. Rarer complications include pulmonary embolism, duodenal varices, hydrothorax, and PV thrombosis. Transhepatic route may result in peri-hepatic bleeding complications.
Wang et al. performed PTO in 30 patients with a technical success of 100% (62). However, the authors combined all procedures with balloon occlusion of the gastrorenal shunt with the aim to embolize the afferent veins with 2-octyl cyanoacrylate. At one year, only one patient had recurrence. Arai et al. showed that PTO (in failed BRTO cases) was technically successful in 44% of cases (technical success was defined as thrombosis of gastric varices on CT scan performed one week later) and when combined with standard BRTO, the success rate reached 100% (60). Sporadic case reports and case series have shown that this procedure is also effective in the treatment of ectopic varices (63,64).
Interventions in portal vein thrombosis and stenosis
Acute PV thrombosis is caused by a variety of conditions, common among them being cirrhosis, hepatobiliary malignancies and surgeries, abdominal infections, and inflammation and hypercoagulable states (65). Uncommonly, it can be idiopathic. Stenosis or occlusion of the PV is a complication associated with hepatopancreaticobiliary malignancy, hepatobiliary surgeries, and liver transplantation, with its incidence in the range of 3%–20% (66–68).
Clinical presentation is variable, ranging from patients being asymptomatic to presentation with abdominal pain, ascites, symptoms and signs of intestinal ischemia, peritonitis, and even death. Chronic thrombosis and stenosis lead to the development of features of portal hypertension. Imaging plays an important role in detecting the thrombosis and its etiology, defining its extent, identifying associated complications, and planning radiological interventions (2).
Indications
Treatment in acute PV thrombosis depends on the etiology, extent of thrombosis, type (bland vs. malignant) and the time of presentation, maintaining candidacy for liver transplantation with treatment goals being improvement in symptoms, and prevention of mesenteric ischemia and progression of the thrombus (69). Surgical thrombectomy and bowel resection is required if there is associated mesenteric ischemia with intestinal infarction or perforation (70). In other cases, minimally invasive procedures are preferred due to higher morbidity, mortality, and recurrence of thrombosis with surgery (71). Patients with minimal thrombus, without any symptoms and thrombosis caused by inflammatory conditions (pancreatitis, surgery, infections) usually do not need any active treatment (69). Although there are no recommendations, the general consensus is to use systemic anticoagulation and catheter-directed treatment in indicated patients. Systemic anticoagulation involves administration of warfarin (with a target international normalized ratio of 2–3) or low molecular weight heparin for 3–6 months.
PV angioplasty is usually indicated in chronic thrombosis, postoperatively, and in liver transplantation, particularly in the pediatric setting (72). The PV stent is placed in malignancies and in cases of failed angioplasty (68,73).
Procedure
Catheter-directed treatment options include transhepatic or transjugular-transhepatic thrombolysis (mechanical or pharmacological), balloon angioplasty and stenting (71) (Figs. 7 and 8). Puncturing a thrombosed PV may be challenging but using ultrasound for guidance is useful. The TIPS route is often preferred as the patient frequently has ascites and is being treated with systemic anticoagulation, both of which increase the risk of bleeding from the transhepatic puncture site (Fig. 7) (75). Further, this route reduces the incidence of recurrent thrombosis by providing an outflow via placement of the TIPS stent, reduces the chances of developing portal hypertension, and provides access for the interventional treatment of the varices (71). Once the PV is accessed, a venogram is obtained from either the splenic or superior mesenteric vein to define the extent of the thrombus. Pharmacological thrombolysis includes an initial bolus dose followed by infusion of thrombolytic agents (urokinase or tissue plasminogen activator) along with heparin. The thrombolytic infusion may be performed for up to 48 h with regular assessment by venograms every 12 h. In cases where thrombolytic agents are contraindicated (recent history of stroke or surgery, active bleeding, recent trauma), mechanical thrombectomy is preferred. This procedure involves maceration of the thrombus by balloon catheter or various suction devices. The procedure may be combined with pharmacological thrombolysis for better results (76). A stent may be placed when there is a stenosis or persistent thrombosis (Fig. 8). Finally, the transhepatic tract is embolized and a TIPS stent may be placed through the transjugular route (71).
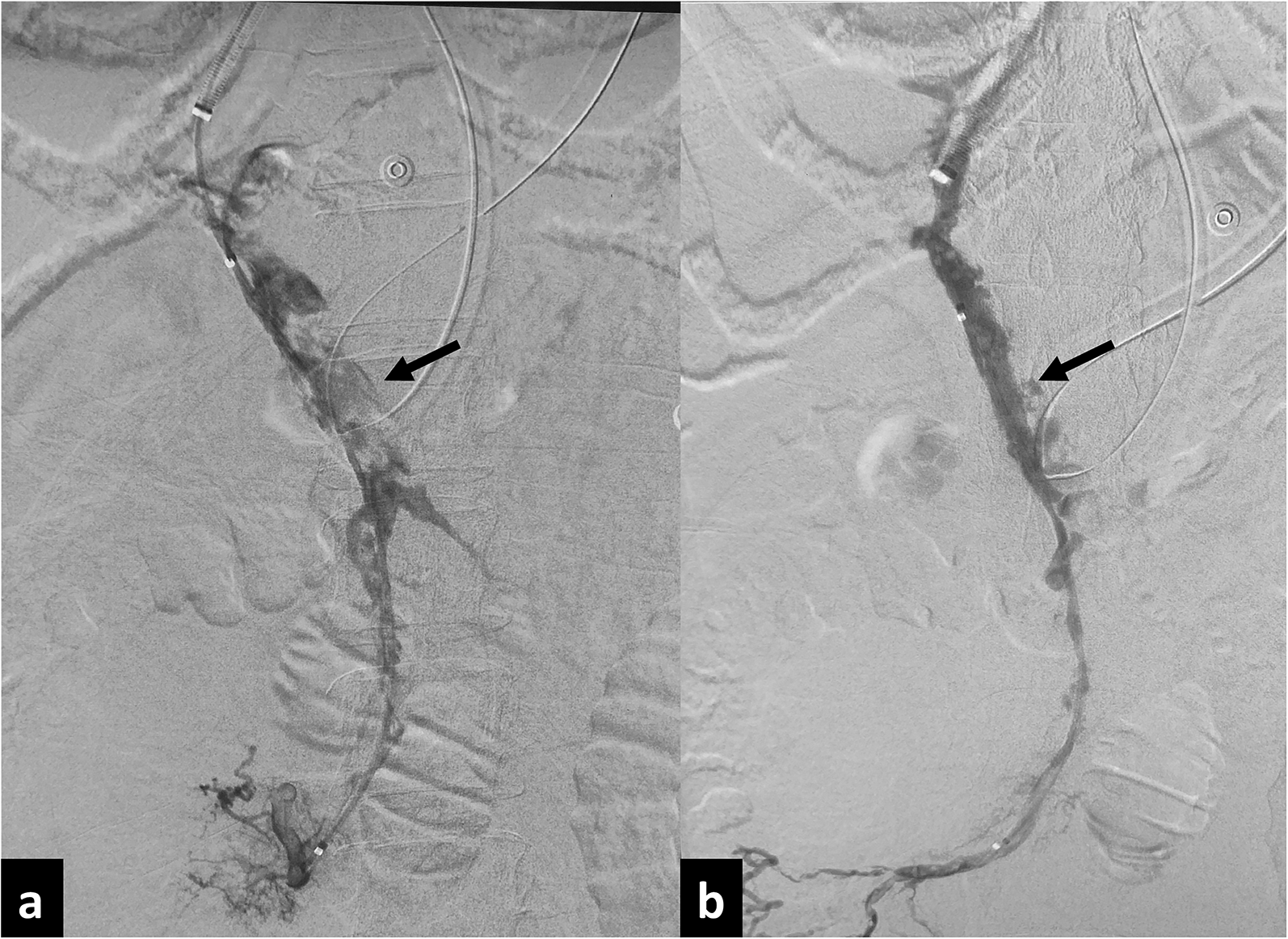
Transjugular portal vein thrombolysis in a 48-year-old woman with spontaneous portal vein thrombosis. (a) Initial portogram through transjugular route shows filling defects within the portal vein (arrow). (b) Portogram after balloon angioplasty and 72 h of pharmacological thrombolysis using urokinase shows near complete recanalization of the portal vein (arrow).
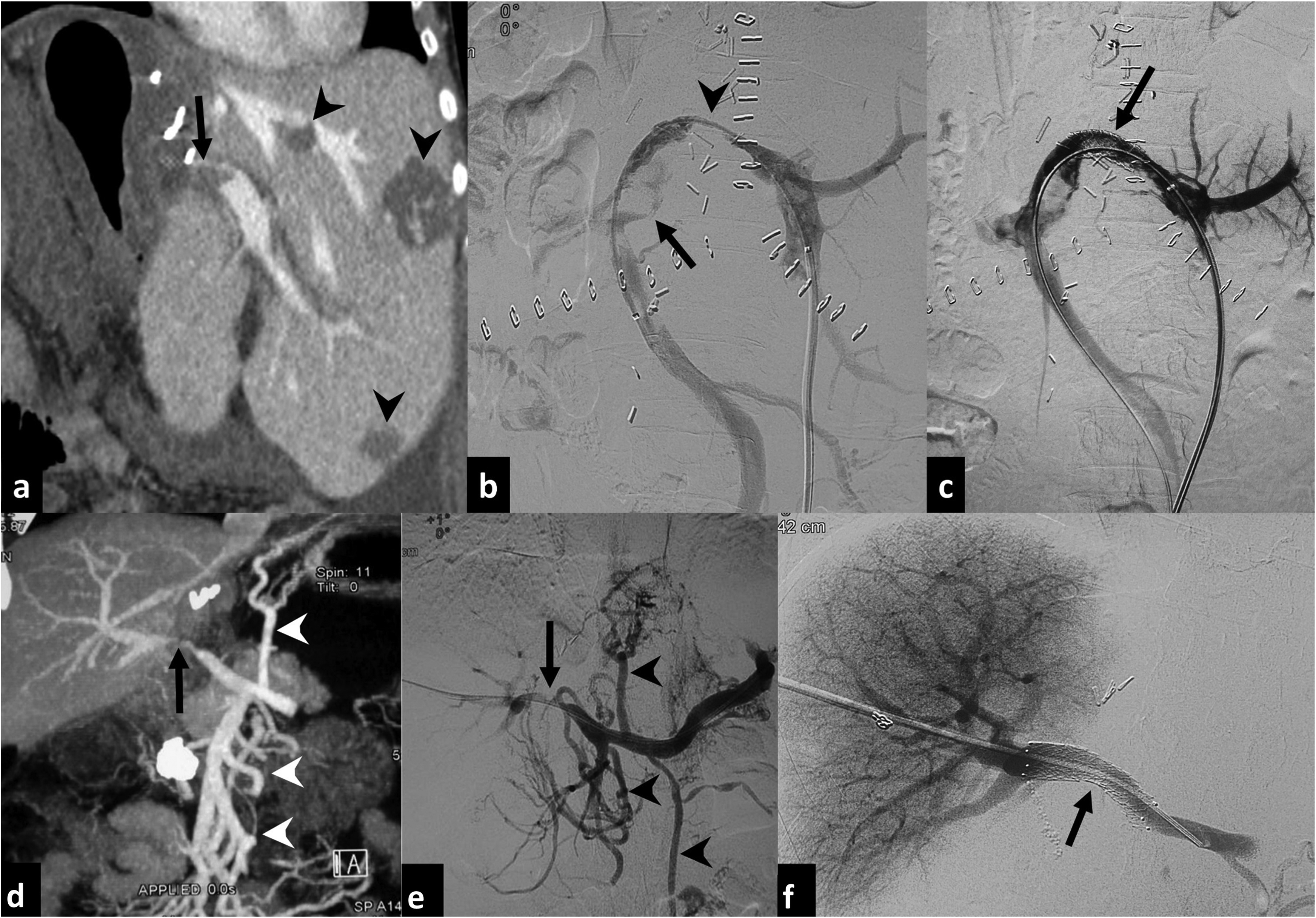
(a–c) Transhepatic PV thrombolysis and stenting in a 55-year-old woman for PV thrombosis after right hepatectomy for hemangiomatosis. (a) Coronal CT image shows thrombosis of the proximal left PV (arrow). Smaller hemangiomas are seen in the left lobe (arrowheads). (b) Transhepatic portogram shows narrowing and irregularity (arrowhead) of left PV with filling defects (arrow) due to thrombosis. (c) Portogram after mechanical thrombolysis and stent placement shows improved patency of left PV (arrow) with residual filling defects. (d–f) Transhepatic PV angioplasty and stenting in a 45-year-old woman with PV occlusion after hepatectomy for cholangiocarcinoma. (d) Coronal maximum intensity projection image shows short segment stenosis of the PV (arrow) with multiple portosystemic collaterals (arrowheads). (e) Transhepatic portogram confirms the PV stenosis (arrow) and the collaterals (arrowheads). (f) Portogram after stent placement (arrow) due to failure of initial venoplasty shows normal flow with disappearance of collaterals. CT, computed tomography; PV, portal vein. [Reproduced from Madhusudhan et al. (74)]
In cases of PV stenosis or occlusion, angioplasty or stenting is performed through transhepatic route (Fig. 8). Additional trans-splenic access may help in difficult cases (77). Anticoagulation with heparin is required during the procedure and is continued for 3–5 days. Subsequently, anticoagulation is maintained by either oral warfarin or combination of acetyl salicylate and clopidogrel (67,68).
A novel and promising technique worth mentioning is percutaneous retroperitoneal splenorenal shunt (PRESS) creation (78,79). This is performed in patients with porto-splenic vein thrombosis to reduce portal hypertension with a minimally invasive approach. This procedure may become an alternative to a surgical lienorenal shunt when TIPS is difficult or not possible.
In situations where PV recanalization is not possible, surgical shunts like mesocaval, portocaval, or meso-atrial shunts may be necessary for the relief of symptoms (80).
Complications and outcomes
Major complications of thrombolysis are seen in about 7%, making it a safe therapeutic option (81). Balloon venoplasty has technical success rates of 66%-78% and restenosis rate of 28%–30% in contrast to stenting (78%–100% and 0%–28%, respectively) (82,83). The outcomes of some studies are shown in Table 5.
Details and outcomes of studies on portal vein thrombolysis, angioplasty, and stenting.
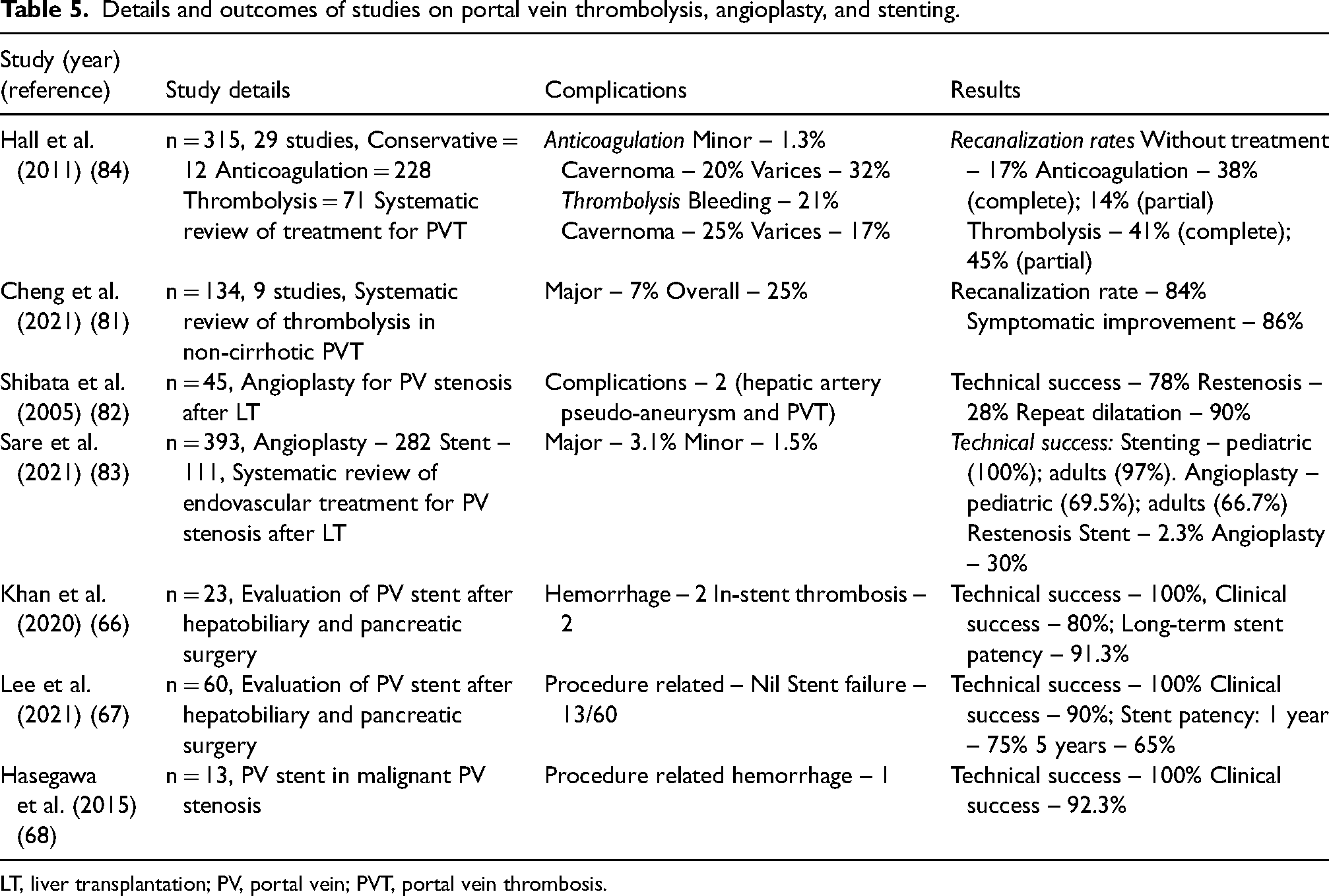
LT, liver transplantation; PV, portal vein; PVT, portal vein thrombosis.
Pancreatic islet cell transplantation
Pancreatic islet cell transplantation (PICT) is a type of treatment that provides better glycemic control and is performed in patients with type 1 diabetes mellitus and chronic pancreatitis (85,86).
Indications and contraindications
In type 1 diabetes, PICT is currently indicated for recurrent severe hypoglycemic episodes, impaired awareness of hypoglycemia, significant glycemic variability, and microvascular complications (84). Here, cadaver-derived islet cells are transplanted (allogenic transplantation) into the recipient. This is better than total pancreas transplantation as it avoids a major surgery and associated complications. In cases of chronic pancreatitis, total pancreatectomy and PICT are performed by isolating islet cells from the surgically removed pancreas (auto transplantation). Since it is an auto-transplantation, immunosuppression is not necessary.
Some of the absolute contraindications for PICT are diabetes duration <5 years, residual C-peptide secretion, untreated diabetic retinopathy, portal hypertension, active infection, history of alcohol or substance abuse, and positive pregnancy test or intent for future pregnancy (87).
Procedure
The procedure involves infusion of isolated islet cells, which contain the insulin-producing beta cells, into the PV percutaneously (Fig. 9) (88,89). Before PICT, the pancreas is retrieved, followed by its processing and isolation of the islet cells (90). The initial steps are similar to PVE. Once a vascular sheath is placed, portal venous pressure is measured. A pressure value of >20 mmHg is a contraindication for PICT due to the increased incidence of PV thrombosis (90). Subsequently, the islet cells are infused, either using a syringe or by gravity flow. Portal vein pressure should be monitored during infusion and any increase >22 mmHg should prompt the termination of the infusion. Finally, the access track is embolized using gelfoam or coils. After the procedure, patients are monitored closely. Anticoagulation with heparin is required during and after PICT for one week (90). Monitoring the glucose levels will assess the response to PICT.
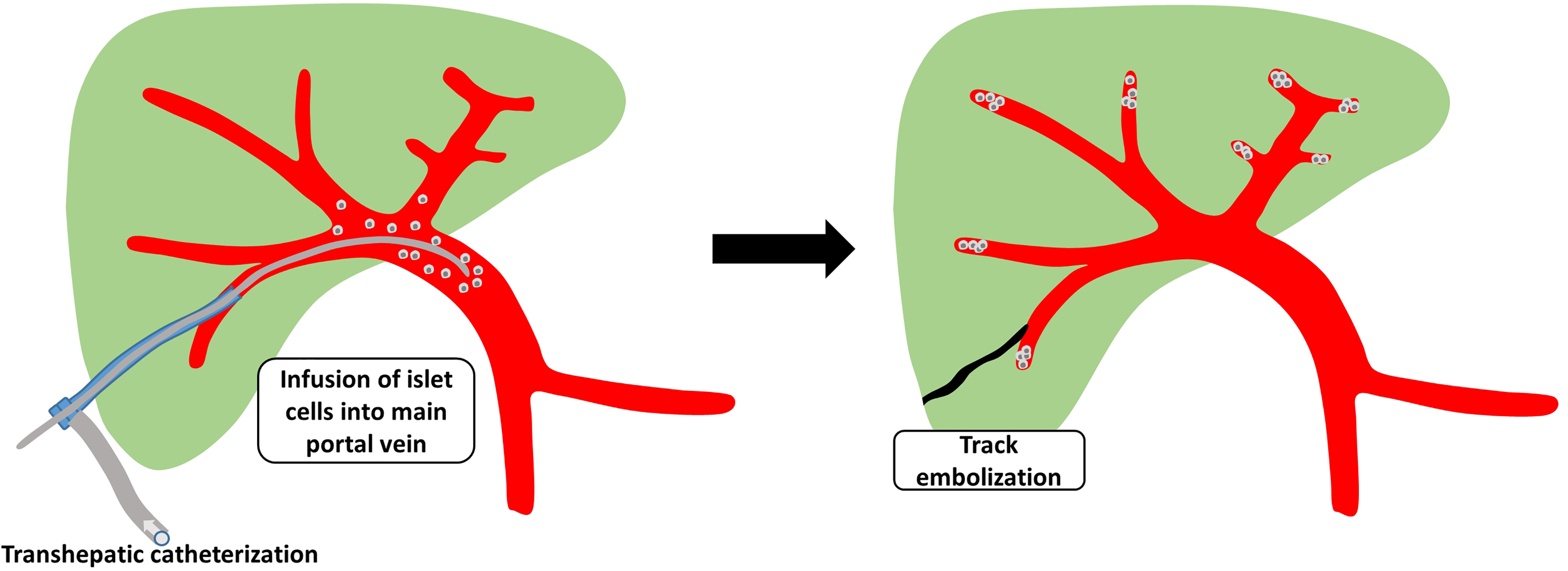
Schematic diagram showing the procedure of islet cell transplantation. The steps include transhepatic catheterization of the PV with infusion of islet cells into the main PV and removal of the catheter followed by track embolization. PV pressure is monitored during the procedure and pressure >22 mmHg is an indication to stop infusion. PV, portal vein.
Complications and outcomes
Bleeding is the most common complication after PICT, with the incidence at 13% (91,92). Other complications include hepatic steatosis (19%) and partial PV thrombosis (<5%) (88). Portal hypertension may develop rarely in whom the PV thrombosis becomes chronic. Advancements in the technique of islet cell isolation, organ preservation, and the protocol of immunosuppression have improved the outcomes of this procedure, with one year insulin independence reaching 80% (90,91). However, this declines to 30%–40% at three years due to graft loss. In PICT performed for chronic pancreatitis, the pancreas is often atrophic and obtaining an adequate amount of islet cells is difficult. Hence only one-third of patients are insulin-independent (93). However, the majority of the patients will still have better glycemic control.
Other PV interventions
Other uncommon PV interventions include embolization of the vein in cases of traumatic or iatrogenic rupture, and interventions for a PV fistula (either with the hepatic artery or bile ducts) and aneurysm. Congenital or acquired fistula or shunts may occur between PV and HV or IVC, requiring interventions (2).
The procedure is usually the standard percutaneous transhepatic approach through the contralateral lobe. For active extravasation, the involved vein is embolized with gelfoam, coils, or NBCA (Fig. 10) (95). In cases of a porto-biliary fistula or a pseudoaneurysm, stent graft is usually necessary to close the fistula or exclude the pseudoaneurysm from the circulation (2).

PVE for trauma in a 56-year-old woman who presented with shock after accidental displacement of the percutaneous transhepatic biliary drainage catheter after 10 days of its placement. (a) Coronal CT image shows active contrast extravasation from a peripheral PV branch into the peritoneal cavity (arrow) causing gross hemoperitoneum (*). (b) Portal venogram after embolization of the bleeding branch with glue (arrow). CT, computed tomography; PVE, portal vein embolization. [Reproduced from Pulappadi et al. (94)].
Conclusion
Various percutaneous radiological interventions can be performed through the portal vein using different approaches. A thorough knowledge of the indications, contraindications, and techniques of these procedures are necessary to ensure safety and favorable clinical outcome.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.