
Abstract
Background
A non-invasive, reliable imaging modality that characterizes cavernous sinus dural arteriovenous fistula (CSDAVF) is beneficial for diagnosis and to assess resolution on follow-up.
Purpose
To assess the utility of 3D time-of-flight (TOF) and silent magnetic resonance angiography (MRA) for evaluation of CSDAVF from an endovascular perspective.
Material and Methods
This prospective study included 37 patients with CSDAVF, who were subjected to digital subtraction angiography (DSA) and 3-T MR imaging with 3D TOF and silent MRA. The main arterial feeders, fistula site, and venous drainage pattern were evaluated, and the results were compared with DSA findings. The diagnostic confidence scores were also recorded using a 4-point Likert scale.
Results
Silent MRA correlated better for shunt site localization and angiographic classification (86% vs. 75% and 83% vs. 75%, respectively) compared to TOF MRA. The proportion of arterial feeders detected was marginally significant for silent MRA over TOF MRA sequences (92.8% vs. 89.5%; P=0.048), though for veins both were comparable. Sensitivity of silent MRA was higher for identification of cortical venous reflux (CVR) (90.9% vs. 81.8%) and deep venous drainage (82.4% vs. 64.7%), while specificity was >90% for both modalities. The overall diagnostic confidence score fared better for silent MRA for venous assessment (P < 0.001) as well as fistula point identification (P < 0.001), while no significant difference was evident with TOF MRA for arterial feeders (P=0.06).
Conclusion
Various angiographic components of CSDAVF could be identified and delineated by 3D TOF and silent MRA, though silent MRA was superior for overall diagnostic assessment.
Keywords
Introduction
Cavernous sinus dural arteriovenous fistulas (CSDAVF) are abnormal arteriovenous connections between the cavernous sinus and the dural branches of the internal and external carotid arteries in the vicinity of the cavernous sinus. These fistulas tend to resolve spontaneously on conservative management and with manual carotid compression and the intervention is usually necessitated if patient has intractable or aggressive clinical symptoms. Intra-arterial digital subtraction angiography (DSA) is the gold standard for the diagnosis of CSDAVF as it accurately characterizes the fistula, its arterial feeders, and venous drainage, and helps in therapeutic planning (1). However, DSA is invasive, and associated with a small but significant morbidity of 0.1%–0.5% and mortality of 0.06% (2,3). Therefore, a non-invasive, reliable imaging modality that characterizes CSDAVF is beneficial for the triaging of these patients and assessing the resolution on follow-up. There are only a few studies on the utility of advanced magnetic resonance angiography (MRA) techniques like 3D time-of-flight (TOF) MRA and susceptibility-weighted imaging (SWI) with DSA for the evaluation of cranial dural arteriovenous fistulas (dAVF), but none for CSDAVF (1,4). Silent MRA is a recently introduced non-contrast MRA technique that employs ultrashort echo time (TE = 0.016 ms) and arterial spin labelling (ASL) methods to obtain angiographic images. Ultrashort TE helps to decrease the magnetic susceptibility and the ASL technique helps to visualize even small changes in the flow signal (5,6). Though the applications of silent MRA have been published for evaluation of cerebral aneurysms, its role in CSDAVF is not yet reported. Slow flow, susceptibility effects from proximity of the sphenoid bone, tortuous, and small feeders are some of the challenges unique to CSDAVF imaging, and it is unknown how these aspects will influence the detailed analysis of fistula from therapeutic perspective. Hence, in this report, we prospectively compared the utility of silent MRA and TOF MRA for the evaluation of various angiographic components of CSDAVF. If found reliable, these non-invasive MRA techniques could be a potential alternative to DSA, especially on follow-up imaging.
Material and Methods
All consecutive patients referred to our institution with the high suspicion of ophthalmological diagnosis of CSDAVF from October 2017 to June 2019 were prospectively enrolled. Patients with contraindications for magnetic resonance imaging (MRI) due to metallic implants or pacemakers were excluded. The institute ethics committee approved the study and informed written consent was obtained from all the participants.
All patients were initially scanned on a 3-T MR scanner (Discovery MR750 W; GE Healthcare, Milwaukee, WI, USA) using a 24-channel head coil. The MRI protocol included the following sequences: 3D TOF MRA (TR/TE = 19/2.9 ms, flip angle = 15°, field of view [FOV] = 200 × 200 mm, matrix = 416 × 192, section thickness = 1.2 mm, number of excitations [NEX] = 1, bandwidth = ± 41.7 kHz, acquisition time = 3 min 31 s); and silent MRA (TR/TE = 1116.4/0.016 ms, flip angle = 5°; FOV = 180 × 180 mm, matrix = 150 × 150, section thickness = 1.2 mm, NEX = 1.5, bandwidth = ± 20 kHz, acquisition time = 7 min 40 s). Apart from these two sequences, routine MR sequences such as diffusion-weighted imaging (DWI), fluid attenuation inversion recovery (FLAIR), and T2-weighted imaging were also obtained. All these patients subsequently underwent cerebral angiogram on a biplane flat panel DSA unit (Innova 3131; GE, Milwaukee, WI, USA). Diagnostic angiograms were performed under local anesthesia and selective angiograms of bilateral internal carotid arteries, external carotid arteries, and vertebral arteries were obtained. Super selective injections from the specific external carotid artery feeders were also obtained when deemed necessary. The temporal resolution of the acquisition was 4 frames/s. All DSA examinations were performed within two weeks of initial MR evaluation.
Image analysis
The two types of MRA images were assessed separately after a gap of four weeks to minimize bias. MR images were read in consensus by two neuroradiologists (SKK and SK with 10 and 2 years of experience, respectively) blinded to the actual diagnosis. Source images, maximum intensity projection (MIP) images, and multiplanar reformatted (MPR) images were evaluated for fistula site, number of arterial feeders, and draining veins of the CSDAVF. Fistulous point was recognized by identifying the sac, where the arterial feeders were seen to converge. Venous drainage was classified as superficial venous drainage (ophthalmic veins or inferior petrosal sinus), deep venous drainage (brainstem veins, uncal veins), and cortical venous reflux (CVR). The main arteries that were feeding into the fistula were counted and correlated with DSA. Angiographic types of CSDAVF were defined as proliferative, restrictive, and late restrictive pattern, based on the extent of the feeder supply (7). DSA findings were retrieved from the radiology reports and were independently verified by a neuroradiologist (JER) not involved in the MR analysis.
The diagnostic quality of the MRA were reviewed subjectively using a modified 4-point Likert scale as follows: 1 = not visible; 2 = poor (slightly visible but with significant blurring or artifacts, not diagnostic); 3 = good (good quality diagnostic information with minimal blurring or artifacts); or 4 = excellent (excellent quality diagnostic information; the depiction is nearly equal to that of DSA).
Statistical analysis
Intermodality agreement between MR and DSA with respect to the fistula site, main arterial feeder, and venous drainage was determined by weighted kappa (κ) statistic (<0.20 = poor, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = good, 0.81–0.90 = very good, and >0.90 = excellent agreement). Wilcoxon signed-rank test was used for assessment of the difference in proportion of arteries or veins detected using both MRA modalities. Diagnostic accuracy indicators such as sensitivity and specificity were calculated for draining veins. Difference in diagnostic confidence score was evaluated using Friedmann test for all three parameters. P < 0.05 was considered statistically significant. Statistical analysis was performed using R statistical software version 3.6.1.
Results
A total of 37 patients (6 men, 31 women; age range = 45–80 years; mean age = 59.5 ± 9.5 years) were included in this study. Most patients presented with orbital symptoms (86.4%) and cranial nerve palsies were noted in 78% of patients. Of the 37 patients, 34 were of Barrows type D, two were of type C, and one was of type B. In total, 31 patients had bilateral arterial supply and six patients had unilateral arterial supply. The most common site of fistula was the posteromedial location (45%), followed by posterolateral (28%), anterior (12%), and midline or intercavernous sinus locations (15%). In four patients, the site of fistula could not be made out clearly. The findings are summarized in Table 1.
Demographic and clinical data of the patient population.
Values are given as n (%) or mean (range).
ILT, inferolateral trunk; IOP, iraocular pressure; MHT, meningohypophyseal trunk
Localization of fistula
For the identification of the site of fistula, the TOF MRA was concordant with DSA in 28 (75%) cases (kappa = 0.66; P < 0.001). The discordance was more for fistula located in the midline or intercavernous sinus, which were mistaken for posteromedial location in three cases. Silent MRA was concordant with DSA in 32 (86%) cases, with a kappa value of 0.82 (P < 0.01).
Angiographic classification
The TOF MRA was concordant with DSA in 28 (75%) cases (kappa = 0.66; P < 0.001), while silent MRA was concordant in 31 (83%) cases, with a kappa value of 0.75 (P < 0.01). The discordance was observed in restrictive and late restrictive patterns of CSDAVF, which was higher for TOF MRA (12% and 8%, respectively) compared to silent MRA (10% and 4%, respectively).
Arterial feeder detection and characterization
A total of 210 arterial feeders were identified in 37 patients on DSA. Most common arterial feeders were from distal branches of the internal maxillary artery (IMA) (94.5%), followed by cavernous branches of the ICA (89%).
TOF MRA correctly identified 89.5% (188/210) of the arteries, while it was higher for silent MRA (92.8%, 195/210). However, the difference in proportion of arterial feeders detected for silent MRA compared to TOF MRA was not significant (P = 0.09). The intermodality correlation between TOF MRA and DSA was moderate, with a kappa value of 0.595 (P < 0.01), while the correlation between silent MRA and DSA was good, with a kappa value of 0.719 (P < 0.01) (Table 2). Most of the missed feeders were from tiny dural branches (meningohypophyseal trunk and inferolateral trunk) of the cavernous ICA in silent (3.8%) and TOF MRA (5.7%).
Diagnostic performance parameters for different angiographic parameters of cavernous sinus dural arteriovenous fistula.

Values are given as n (%) unless otherwise indicated.
MRA, magnetic resonance angiography; TOF MRA, time-of-flight.
Venous drainage
There were 74 draining venous channels identified on DSA in this study. Cortical venous reflux was observed in 22 (59%) patients, while deep venous reflux was seen in 17 (54.8%) patients. Of these venous channels, 90% were correctly identified on silent MRA, while the accuracy was 85% on TOF MRA. The proportion of veins observed between two MR modalities was, however, not significant (P = 0.12). The intermodality correlation between TOF MRA and DSA was moderate, with a kappa value of 0.43 (P < 0.001). The intermodality correlation between silent MRA and DSA was good, with a kappa value of 0.68 (P < 0.001). Sensitivity and specificity of the silent MRA identification of CVR and deep venous drainage was higher for silent MR, compared to TOF MRA (Table 2).
Evaluation of diagnostic scores across modalities
The median diagnostic score was 4 across different architectural aspects such as fistula point evaluation, arterial feeder, and venous drainage assessment for silent MRA, while it was 3, 4, and 4, respectively, for TOF MRA. A significant difference in diagnostic score was evident for fistula point identification (P < 0.001) and venous drainage assessment (P < 0.001). However, there was no significant difference noted between TOF MRA and silent MRA for arterial feeder identification (P = 0.0625).
Representative cases demonstrating the core features like arterial feeders, venous drainage, and fistulous point are illustrated in Figs. 1–3, respectively.
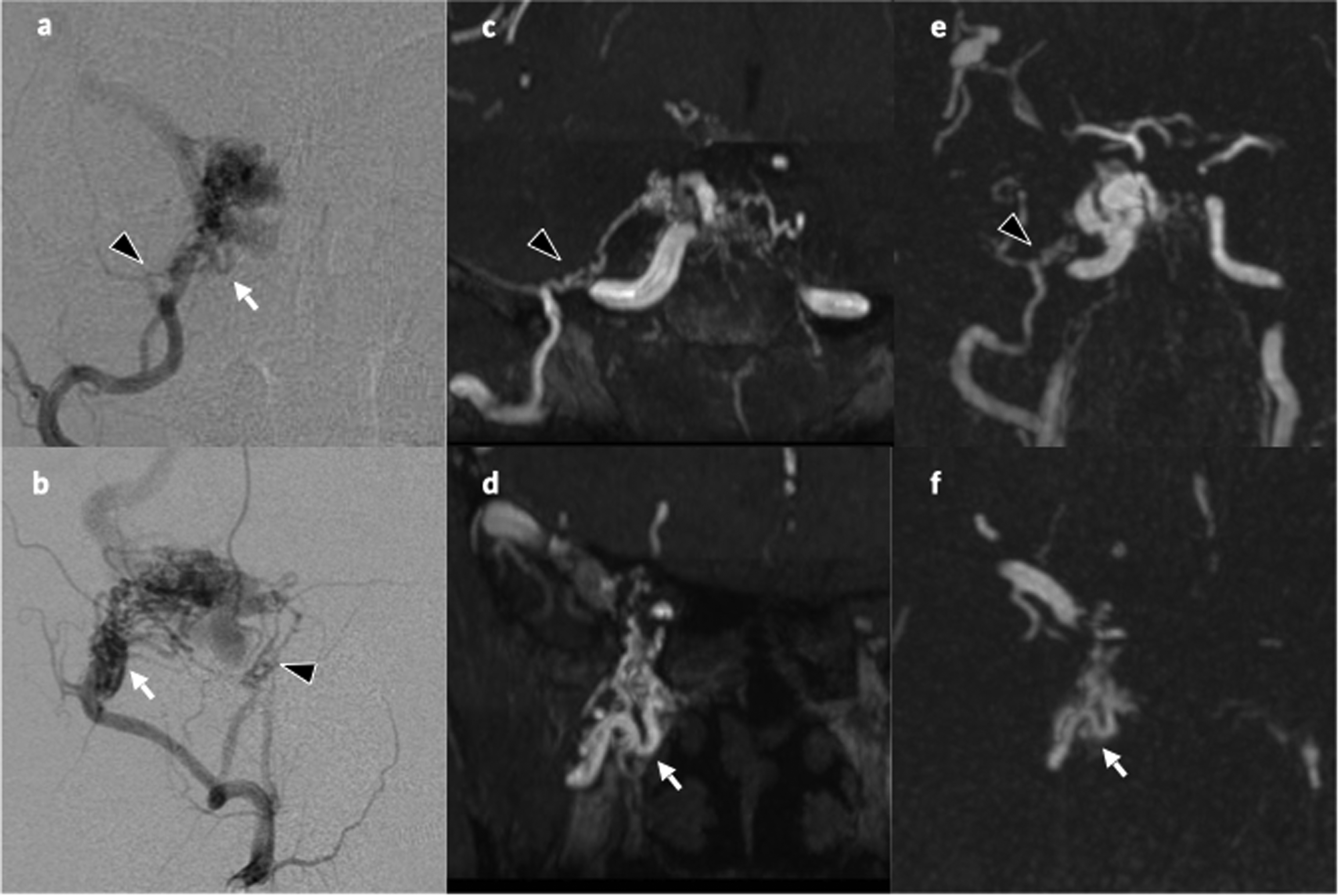
Angiogram of the right external carotid artery (a) frontal and (b) lateral view shows a cavernous sinus dural arteriovenous fistula on the right side with arterial feeders from middle meningeal arterial branches (arrowhead) and internal maxillary branches (arrow). (c, d) TOF MRA coronal MIP image reveals middle meningeal arterial branches (arrowhead) and internal maxillary branches (arrow); (e, f) these feeders are well demonstrated in silent MRA as well. Diagnostic confidence score was 4 for TOF MRA and 4 for silent MRA. MIP, maximum intensity projection; MRA, magnetic resonance angiography; TOF, time-of-flight.
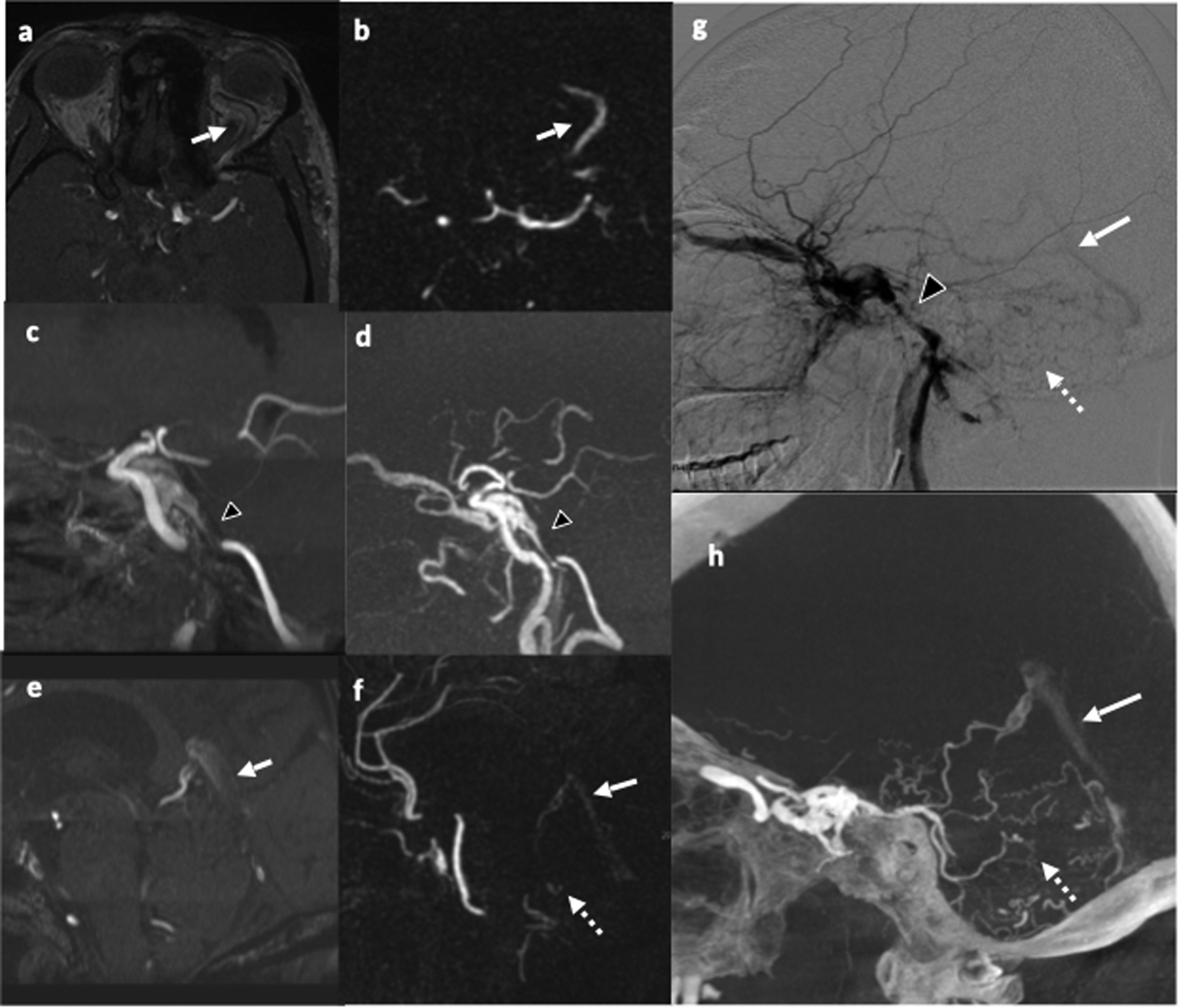
A case of left cavernous sinus dural fistula, presented with diplopia under evaluation. (a) TOF MRA axial source image reveals a dilated left superior orbital vein (arrow), but appears hypointense due to saturation effect in SOV. (b) Prominent and dilated left SOV can be readily appreciated in a corresponding silent MRA axial partial MIP image. (c) Sagittal TOF MRA partial MIP image, inferior petrosal sinus (arrowhead) shows reduced signal loss compared to silent MRA (arrowhead in d). (e) Similarly, sagittal reconstruction of MIP of TOF MRA shows faint visualization of the posterior fossa veins (arrow), which however can be appreciated without difficulty in (f) silent MRA. (g) Corresponding DSA and (h) 3D rotational angiographic images confirm these drainage pathways (IPS = arrowhead, deep venous drainage = arrow, and cortical venous reflux = dotted arrow). Diagnostic confidence score was 3 for TOF MRA and 4 for silent MRA. IPS, XX; MIP, maximum intensity projection; MRA, magnetic resonance angiography; SOV, supeior ophthamic vein; TOF, time-of-flight.

(a) Axial source image from TOF MRA shows the shunted pouch (arrow) is located posteromedially to the cavernous sinus, which is also well demonstrated in (b) silent MRA. (c) The location was confirmed on 3D rotational angiogram. Diagnostic confidence score was 3 for TOF MRA and 4 for silent MRA.
Discussion
In this study, we evaluated several angio-architectural components of CSDAVF that have relevance to angiographic assessment and therapeutic planning. Our results showed that the diagnostic performance of silent MRA was better across all the parameter evaluations of CSDAVF compared to TOF MRA and a distinct difference was noted for the characterization and localization of CSDAVF. In addition, the diagnostic confidence score was higher for silent MRA in the evaluation of venous characteristics and locating shunt point, while the performance was similar for both sequences for arterial feeder detection.
The studies on the usefulness of non-invasive advanced MRA in the evaluation of CSDAVF are limited and much of the studies are focused on cranial DAVF. The value of MRI (3D TOF MRA and contrast-enhanced MRA) in detecting and describing DAVF was assessed by Bink et al. in 19 patients and reported that with MRI, DAVF can be detected reliably with high sensitivity, specificity, and accuracy (8). Using 3-T MRI, Azuma et al. compared gross characterization of intracranial DAVF between 3D TOF MRA and DSA in 26 patients (1). They evaluated main arterial feeders, fistula site, and venous drainage pattern on MRA and DSA images and found that inter-observer agreement was excellent for fistula site (κ = 0.919), good for main arterial feeders (κ = 0.711), and very good for venous drainage (κ = 0.900). Intermodality agreement was excellent for fistula site (κ = 0.968) and good for main arterial feeder (κ = 0.809) and venous drainage (κ = 0.837). They concluded that gross characterization of intracranial DAVF was similar for both imaging modalities. Studies on time-resolved contrast-enhanced MRA (CE-MRA) have shown that these techniques can provide hemodynamic information regarding intracranial DAVFs but were not a reliable tool for assessing main arterial feeders of DAVF (9,10). Using 3D pseudo-continuous arterial spin-labeling MRI, the identification of the venous arterial spin-labeling signal had a high sensitivity (94%) and specificity (88%) for the presence of a DAVF; in addition, it improved the diagnostic confidence (11). With reference to CSDAVF, Takahashi et al. reported that the most fistulous points of CSDAVF were detected in the posterior portion of the cavernous sinus or in the posterior portion of the intercavernous sinus by contrast-enhanced MRI (12). Even though non-contrast MRA is shown to be reliable for the diagnosis of the cavernous fistula, potential misdiagnosis with benign jugular venous reflux can occur, which can be differentiated by careful radiological interpretation (13,14).
In our study, we observed that the silent MRA was marginally better for the evaluation of arterial feeders. The vessel diameter of the arterial feeders is generally small in CSDAVF compared with the voxel size of the MRA images and hence the spatial resolution of the sequences is decisive for their clear depiction. In TOF MRA, the visualization of vascular structures is depended on their alignment to the scan plane. If it is along the flowing blood, the signal may be lost as the spins are exposed to saturating radiofrequency pulses (1). On the contrary, silent MRA is insensitive to the saturation effects of the flowing spins and thus it may have an apparent advantage over TOF MRA due to the better background suppression (15). However, the present study reports that TOF MRA is nearly comparable, which may be the result of its superior spatial resolution at higher magnetic field strength. With respect to the assessment of venous drainage, silent MRA was found to be superior to TOF MRA, especially for CVR and deep venous drainage. The difference in performance might be attributable to the fundamental difference in image generation that exists between the two sequences and hemodynamic characteristics of CSDAVF. Due to the lack of capillary bed in CSDAVF, there is no tissue water extraction, and the transit time of the labeled water is significantly shortened, leading to high venous ASL signal intensity (16). In contrast, the effect of technical factors on the venous signal attenuation are greater in TOF MRA. The saturation effects due to slow flow might be more pronounced in CSDAVF, especially in slow flow CSDAVF such as restrictive or late restrictive types, leading to the greater signal loss. Inclination of superior ophthalmic vein in relation to TOF saturation band may also play a role in signal attenuation. The majority of the fistulous points in our study were located in the posterior or posterior medial aspect of cavernous sinus or in the intercavernous sinus, which was consistent with previous reports (17,18). Silent MRA was clearly advantageous over TOF MRA for shunt point identification. The magnitude of the silent MRA signal depends on the number of labeled spins traversing the fistula, and the precise timing of sequence acquisition (both labeling time and post labelling delay) (16). In CSDAVF, all the labelled spins from the feeding arteries converge into a single shunt point, thereby leading to its enhanced visualization. Background suppression and subtraction of control from label images yields improved contrast-to noise ratio, which will also magnify the apparent contrast difference. Unlike TOF MRA, silent MRA may better visualize small and slow-flow vessels, as it is insensitive to saturation effects and not influenced by vessel direction (5). The utility of silent MRA in visualizing flow in stents and residual flow in the aneurysms after coiling has been reported (6,19–21).
Other advantages of silent MRA include markedly better background suppression, sagittal acquisition, and a square FOV, which allows for the coverage of neck vessels in addition to intracranial circulation. Acquisition of both carotid and intracranial vessels in a single silent MRA protocol could save imaging time, with a superior image quality than with conventional techniques (22). Compared to TOF MRA, the source images however provide poor anatomical information due to low background signal. This issue could be resolved by fusing any volumetric MR acquisition with the silent MRA sequence using standard vendor provided fusion software. Since both the sequences generate volumetric data, the images could be evaluated in multiple planes using multiple formats such as MIP, partial MIP, or volume-rendered images; further, DSA-like images could also be derived for detailed analysis. Trade-off between increased scan time and superior anatomical visualization is an important factor that needs to be taken into account while using silent MRA; however, it is clinically justifiable as the information yielded might be sufficient for therapeutic decision making in select cases. Reducing the number of excitations, phase encoding steps, or increasing the bandwidth can potentially decrease the scan time, though its effect on signal-to-noise ratio needs to be evaluated.
The modest number of a relatively rare disease, uniform study protocol, and prospective design are some of the strengths of our study. Some of the limitations of the study include data from a single-center experience, non-inclusion of follow-up patients as these patients were routinely monitored for resolution by their clinical/ocular symptoms, and non-assessment of interrater concurrence. Since considerable expertise is needed to read DSA and subsequent translation of the observations into MRA in CSDAVF, only consensus opinion was used for analysis. Being a tertiary care center, all the patients referred with high clinical suspicion of CSDAVF diagnosis were eventually proved to have fistula, and this a priori knowledge would have possibly biased the investigators towards a thorough image analysis. Nevertheless, our study highlighted the applicability and performance of non-contrast advanced MRA techniques in the evaluation for various components of CSDAVF.
In conclusion, various angiographic components of CSDAVF were better delineated by 3D TOF and silent MRA, though silent MRA had better overall diagnostic performance. Non-contrast enhanced MRA techniques can evaluate CSDAVF from interventional perspective and could be considered for patients requiring multiple follow-up studies.
Footnotes
Availability of data and material
All relevant data are included in the study; further data could be shared upon request to the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.