
Abstract
Background
High-resolution computed tomography (HRCT) scans can help identify subsets of asthma patients who show rapid decline in lung function.
Purpose
To evaluate high-resolution computed tomography (HRCT) findings in adult patients with asthma, obtain quantitative measurements of air trapping on expiratory scans, and correlate the findings with pulmonary function tests (PFTs).
Material and Methods
Thirty adults with asthma with persistent-mild, persistent-moderate, and persistent-severe categories as per standard clinical guidelines were evaluated with inspiratory and expiratory HRCT for various imaging features of bronchial asthma. Expiratory HRCT scan were used to quantify degree of air-trapping, and their values quantified as “pixel index,” using a special “density' mask” software. Complete spirometry and body plethysmography were performed on each patient within 0–2 days of HRCT scans. HRCT findings were correlated with the clinical severity groups and the CT pixel indices (PI) were correlated with the PFT results using correlation coefficients and linear regression analysis.
Results
The inspiratory CT findings did not correlate with increase in disease severity. Expiratory scans accurately quantified areas of air trapping. CT-PI correlated well with PFT values indicative of airway obstruction and airflow limitation, which helped differentiate patients with asthma with increasing severity from those with milder forms of the disease.
Conclusion
Expiratory thin-section CT is a useful objective method to quantify air-trapping in people with asthma. The air-trapping score measured in “pixel indices” correlates well with PFT results and can successfully identify patients with severe asthma. Further studies are needed to confirm if this parameter can serve as a potential marker for airway remodeling and declining lung function.
Introduction
Bronchial asthma is a chronic inflammatory airway disorder that leads to variable airflow obstruction. The aim of the present prospective study was to evaluate high-resolution computed tomography (HRCT) findings in adult patients with asthma, obtain quantitative measurements of air-trapping on expiratory scans and correlate the findings with pulmonary function tests (PFT), to identify a subset of patients who show accelerated decline of pulmonary function and poor reversibility of airway obstruction.
Material and Methods
A total of 30 adults with asthma (14 men, 16 women; age range = 20–50 years; mean age = 34.6 years), who had never smoked and had no active respiratory infection, were grouped into persistent-mild (n = 12), persistent-moderate (n = 10), and persistent-severe (n = 8) categories on the basis of frequency of clinical symptoms (wheezing, breathlessness, and chest tightness) and documented reversible airflow limitation (1). Chest CT was performed with Somatom HiQ scanner (Siemens, Erlangen) using a high spatial frequency algorithm. Inspiratory scans were acquired from the lung apices through the lung bases. Axial images (thickness of 1.5 mm, intervals of 10 mm) were viewed at a window-level of −700 Hounsfield Units (HU) and window-width of 1200 HU. Expiratory scans were obtained at the levels of the aortic arch and above the domes of diaphragm. The percentage of pixels below −910 HU was calculated on expiratory scans (“pixel index” [PI]), using the “density mask” software (2,3). Complete spirometry (Morgan Spiroflow, PK Morgan Ltd., Kent, UK) and body plethysmography (Morgan Autolink Body Plethysmograph) was performed on each patient within 0–2 days of CT. Written informed consent was obtained from all patients. The study was approved by the institutional review board. Inspiratory CT findings were correlated with disease severity using the chi-square test. Unpaired Student's t-test (two-tailed) was applied to compare age, PFT, and PI values among the three categories of patients. Finally, PI values were correlated with PFTs using Pearson's coefficient of correlation and linear regression analysis. A probability value of <0.05 was taken as statistically significant.
Results
The inspiratory CT features included the following: hyperlucency and mosaic attenuation (16/30 = 53%); ground-glass or consolidation (12/30 = 40%); bronchial wall thickening (12/30 = 40%); bronchial dilatation and bronchiectasis (8/30 = 27%); normal scans (8/30 = 27%); and mucoid impaction, tree-in-bud, and subsegmental atelectases (6/30 = 20%) (4). None of these findings correlated with disease severity, though the extent of hyperlucency was more in severe disease on visual estimation (Table 1).
Thin-section CT findings in bronchial asthma.

Values are given as n (%).
HRCT, high-resolution computed tomography.
PI values calculated on expiratory scans taken at the level of arch of aorta showed significant correlation with PFT parameters suggestive of airflow limitation such as peak expiratory flow rate (PEFR) and FEV1, and to a lesser extent with residual volume/total lung capacity (RV/TLC) and forced vital capacity (FVC) (P < 0.05). PI values above the domes of diaphragm showed more significant correlation with PFT parameters suggestive of air-trapping such as RV and RV/TLC, as well as airflow limitation such as PEFR, FEF25-75, and FEV1 (all with P < 0.01) as well as to a lesser extent with FVC, FEV1/FVC, and RawEx (P < 0.05) (Tables 2 and 3).
The three groups of patients.
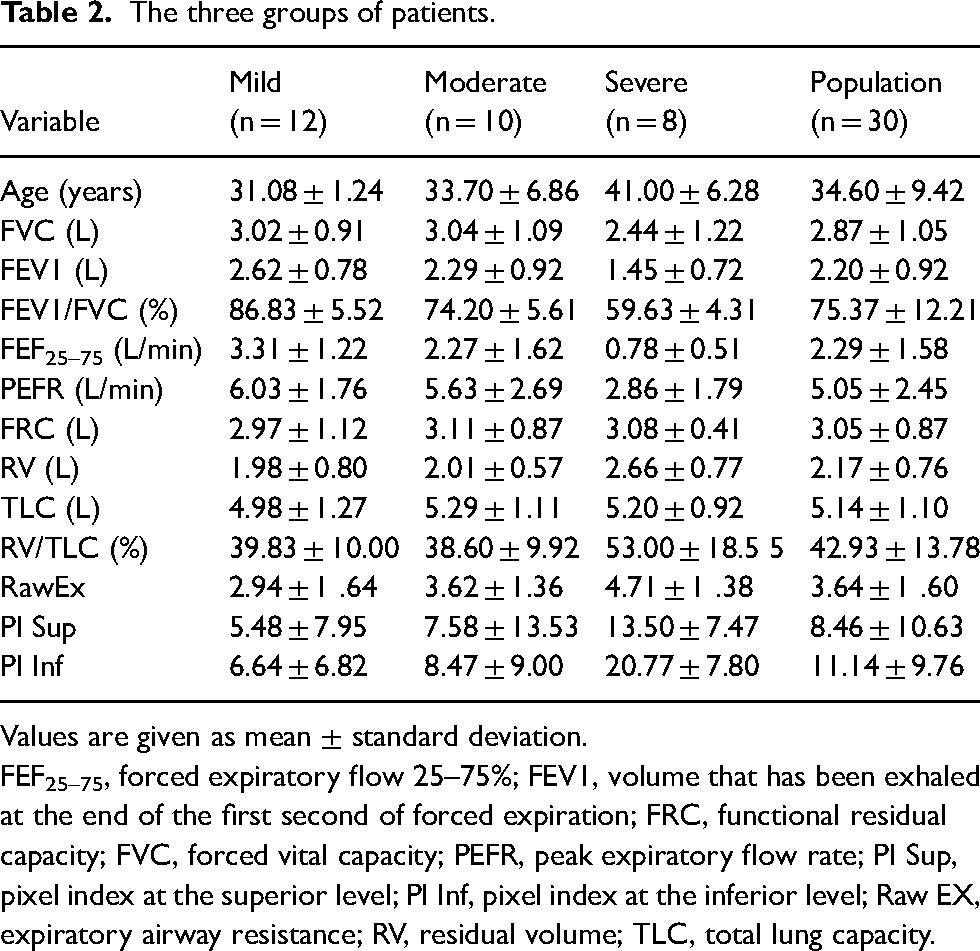
Values are given as mean ± standard deviation.
FEF25–75, forced expiratory flow 25–75%; FEV1, volume that has been exhaled at the end of the first second of forced expiration; FRC, functional residual capacity; FVC, forced vital capacity; PEFR, peak expiratory flow rate; PI Sup, pixel index at the superior level; PI Inf, pixel index at the inferior level; Raw EX, expiratory airway resistance; RV, residual volume; TLC, total lung capacity.
Correlation of PI values with pulmonary function tests.
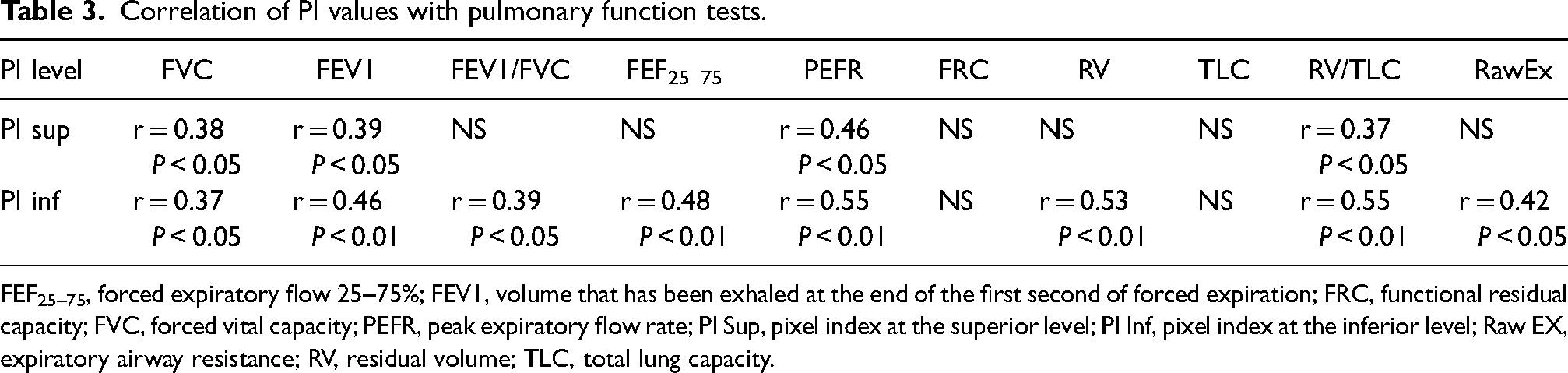
FEF25–75, forced expiratory flow 25–75%; FEV1, volume that has been exhaled at the end of the first second of forced expiration; FRC, functional residual capacity; FVC, forced vital capacity; PEFR, peak expiratory flow rate; PI Sup, pixel index at the superior level; PI Inf, pixel index at the inferior level; Raw EX, expiratory airway resistance; RV, residual volume; TLC, total lung capacity.
Discussion
Several studies have shown that a subset of patients with asthma demonstrate an accelerated decline in FEV1 values, presumably due to mechanical change and remodeling of the lungs (5). Although spirometry, including techniques such as low-density gas spirometry, and measurements of closing volumes can quantify functional impairments, they are unable to highlight the anatomic location and pathologic nature of the actual remodeling process. Improved spatial resolution offered by HRCT using narrow collimation (1–2 mm) and high spatial frequency algorithm makes it an ideal non-invasive method of illustrating the site and nature of these changes. Consequently, it is possible to identify patients most at risk of remodeling and worsening of lung function, so that early therapeutic interventions can be instituted in them. Pressure changes occurring in small airways (<2 mm), which represent one-sixth of the total airway resistance are not correctly reflected by the plethysmography values measured at the mouth of patients with elevated airway resistance. This disparity increases with increase in bronchospasm. Air-trapping occurs due to closure of peripheral airways. It is seen on HRCT scans as areas of low attenuation. It may be seen in healthy as well as in individuals with asthma. However, it is the extent of air-trapping that is important, being much more in patients with asthma. Inflammation of the peripheral airways leads to narrowing of their lumen, resulting in their closure at much higher volumes in asthmatic lungs. The hyperlucent areas could also represent decreased perfusion in under-aerated areas of the lungs. Although measurement of bronchial wall thickness using CT has been used as a research tool for “direct” assessment of airway remodeling, the resultant functional impairments of airflow limitation and air-trapping are more easily quantifiable using expiratory CT and can easily be integrated into routine clinical usage (6).
Lung density can be measured using CT attenuation values, with normal values falling between −700 and −800 HU on inspiration. The lung attenuation in normal individuals increases on expiratory scans. The “density mask” software highlights pixels (picture elements of a CT image) that have low attenuation values. A previous study by Newman et al., which used −900 HU as the cutoff, showed that it is possible to quantify areas of abnormal decreased lung attenuation in expiratory scans; this was subsequently validated by other studies. The authors found that the results of the quantitative CT (QCT) scans, expressed in terms of pixel index values, correlated significantly with PFTs that reflect air trapping and airflow limitation (2,3). Newman et al., in their study of 18 non-smoking adults with asthma and 22 adult controls, performed QCT in all individuals at the same two levels at both end-inspiration and end-expiration. Collimation scans of 10 mm and 1.5 mm were taken at each level. The percentage of pixels below −900HU were calculated in each of the QCT axial images. The pixel index values of expiratory HRCT scans at the two levels were 5.07 and 10.03, respectively. These results are comparable with our own, with the corresponding values being 8.46 and 11.14, respectively.
The present study has some limitations, including its small sample size. The rationale for choosing a total of 30 patients (10 per group) was to validate “proof of concept” in a pilot study. We wished to see if the PI and “density mask” software would work in a small pilot project, and intentionally limited the number of patients to the minimum needed to reach statistical significance. We wanted to be extremely cautious before subjecting any more patients to CT ionizing radiation if the results of our small pilot project were inconclusive. We believe that the results of the present study would enable us and other researchers to plan larger prospective studies to evaluate these results and build on our conclusions.
Moreover, expiratory scans were obtained at only two preselected levels and then correlated with PFTs, which reflect changes in the entire respiratory tract. Spirometry-gated CT was not performed to verify optimal scanning at end-inspiration or expiration. Our method of obtaining expiratory scans at two levels, one at the level of the aortic arch and the other ∼2 cm above the diaphragm, has some benefits. First, there is significant saving in radiation dosage compared to scanning the entire chest twice (inspiration and expiration), which becomes even more significant knowing that many of our patients are relatively young and female. The second benefit is in patient compliance with breathing instructions. Patients with asthma who are dyspneic can barely hold their breath in expiration for the entire duration of the scan when scanning the whole chest. Many end up breathing during the scan, which causes significant distortion of image quality and make density mapping extremely difficult. Air-trapping in asthma occurs throughout both lungs with possible regional variations. By scanning at two representative levels of the chest, it is possible to ensure patient compliance, reduce radiation exposure, and at the same time adequately sample a phenomenon that is representative of the rest of the lungs. As opposed to spirometry-gated CT, which may not be routinely in use, the two-level expiratory scan method using density mapping can be easily added to routine clinical protocols. Since the sampled values on expiratory CT correlate with PFT values reflective of air-trapping and airflow limitation, we suggest that this relatively easy scanning method may serve as a potential imaging biomarker for a subset of individuals with asthma who suffer progressive decline. Our patients were not statistically age-matched (age could influence PI), and comparison with healthy volunteers was not performed, which could enable better distinction of normal from abnormal parameters.
In conclusion, HRCT was both subjectively and objectively used to outline anatomic and pathophysiologic details of asthmatic lungs. The subjective findings did not correlate with disease severity. These included the following: hyperlucency and areas of air-trapping; bronchial wall thickening; bronchial dilatation and bronchiectasis; normal scans; mucoid impaction with or without areas of collapse or consolidation; and mosaic pattern of lung attenuation (in decreasing order of frequency). Expiratory CT scans objectively quantified areas of air-trapping in asthmatic lungs. Their values as expressed in pixel indices correlated well with PFT results indicative of air trapping and airflow limitation. These values helped differentiate patients with asthma with increasing severity from those with milder forms of the disease. Further larger studies are needed to validate if this can be used as a potential marker of airway remodeling and an indicator for early therapeutic intervention (7). Studies using hyperpolarized Xenon-129 MRI of the lungs, a technique that does not involve ionizing radiation, shows future promise for accurate quantification of airflow limitation and air-trapping in asthma (8).
Footnotes
Acknowledgements
The author thanks Madhu Gulati, former Associate Professor of Radiology and Ashutosh N Aggarwal, Professor and Head of the Department of Pulmonary Medicine, both at the Postgraduate Institute of Medical Education and Research, Chandigarh, India 160012, for serving as guide and co-guide during completion of the author's thesis project.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.