
Abstract
Background
Computed tomography (CT)-guided percutaneous transthoracic needle biopsy (PTNB) is highly affected by respiratory motion; however, respiratory motion of target nodule during the PTNB and its effect on CT-guided lung biopsy have not been studied.
Purpose
To investigate the effect of the respiratory motion of pulmonary nodules on CT-guided PTNB.
Material and Methods
We retrospectively reviewed the procedural CT scans of 426 pulmonary nodules that underwent PTNB during quiet breathing. Maximal and average respiratory motions were measured using the difference of table position of the targeted nodule between multiple procedural scans. Diagnostic performance, complications, and technical factors of PTNB in nodules with large motion (maximal motion >1 cm) were compared with those in nodules with small motion (≤1 cm).
Results
The mean maximal and average respiratory motions between tidal volume breathing were 5.4 ± 4.4 and 2.7 ± 2.6 mm, respectively. Sensitivity and accuracy were 93.1% and 96.1% in nodules with large motion, compared with 94.7% and 95.9% in nodules with small motion, respectively. Respiratory targeting (P < 0.001), needle modulation (P < 0.001), motion artifact of target (P < 0.001), target disappearance from scans (P < 0.001), and number of performed CT scans (P < 0.001) were significantly higher in the large motion group, with no significant difference in radiation dose and complications between the groups.
Conclusion
The respiratory motion of pulmonary nodules during CT-guided PTNB may cause technical difficulties but does not affect diagnostic performance nor complications associated with PTNB.
Introduction
Computed tomography (CT)-guided percutaneous transthoracic needle biopsy (PTNB) is still the most widely used modality in the acquisition of lung nodule tissue (1). Given that CT biopsy is not a real-time examination, it can be affected by respiratory motion when targeting the nodule. The measurement of respiratory movement of pulmonary nodules has been widely studied in the radiotherapy or positron emission tomography (PET)/CT era, where accurate anatomic localization of tumors is required (2,3). CT-based measurements of the respiratory movement of nodules show that it is larger in the lower compared to the upper lung, and larger in the left compared to the right lung, because of heart motion (2,4,5). In the CT-guided lung biopsy field, motion is known to be problematic in targeting nodules (6–8) Thus, many studies have been conducted on the performance of nodule biopsy in the presence of large respiratory motion, including small nodules or juxtaphrenic nodules (6,9,10). Although these studies’ participants are supposed to have nodules with large motion, the actual measurement of nodule motion during the PTNB and its effect on CT-guided lung biopsy have not been studied.
In CT-guided PTNB, breath holding minimizes respiratory motion and reduces complications (11–14). Otherwise, given that breath holding does not guarantee the reproducibility of the diaphragm position, a free-breathing procedure may be suggested for lesions with an upper lung location and with large sizes (11,15,16) and in patients who require sedation (17–19). The performance and complication of quiet-breathing biopsy was acceptable in a recent study (20). We have been performing PTNB under quiet-breathing conditions to achieve stable and regular breathing while the patient is comfortable, thereby reducing the tension of both the patient and the operator. Although it is difficult to measure respiratory movement in the breath-holding procedure, the movement of the nodule performed during quiet breathing can be measured retrospectively. The aim of the present study was to measure the respiratory motion of targets during PTNB under quiet breathing and to investigate the effect of the respiratory motion of targets during a PTNB procedure.
Material and Methods
This retrospective study was approved by our institutional review board (approval no. 2022-04-033). The requirement for informed consent was waived because of the retrospective nature of the study. From January 2018 to October 2019, 457 consecutive CT-guided PTNBs of lung lesions were performed at our institution and were included in this study. Mediastinal, pleural, or chest wall lesions were not included. Among the 458 procedures in 440 patients, we excluded nine procedures in which the CT scans of a needle puncturing the pleura were skipped. One case was excluded because pneumothorax occurred at the first puncture and the target location could not be evaluated. Another 21 procedures experienced an indeterminate diagnosis and were excluded. A total of 426 procedures performed in 410 patients were finally included. Ten procedures were re-biopsies for the same lesions.
Procedure
All biopsies were performed by two thoracic radiologists with 20 and 5 years of experience. We obtained a low-dose axial scan with 80 kVp, 12–15 mA per scan, and collimation of 12 × 0.6 mm on a 64-multidetector CT scanner (Somatom Perspective; Siemens Healthcare, Erlangen, Germany). In eight cases, CT images were acquired with 110 kVp to check detailed vessels in the chest wall. We ensured that the patient breathed comfortably without sighing or taking deep breaths during the procedure. The operator observed the patient's breathing via 2–3 preprocedural scans and then decided whether to perform respiratory targeting. Respiratory targeting is a technique whereby an operator inserts a needle at the end of the inspiratory or expiratory phase when the movement is significant; the center of the target was out of the range of performed scans, or the entry point was intervened by the overlying ribs (Fig. 1) (20). If the respiratory movement was minimal in the preprocedural scans, the intervention proceeded. The operator selected either the expiratory or the inspiratory phase for needle insertion to provide a safer and shorter route. A biopsy was conducted using a semi-automatic 21-gauge cutting needle (Stericut; TSK, Tochigi, Japan). Postprocedural CT scans were obtained to identify complications.
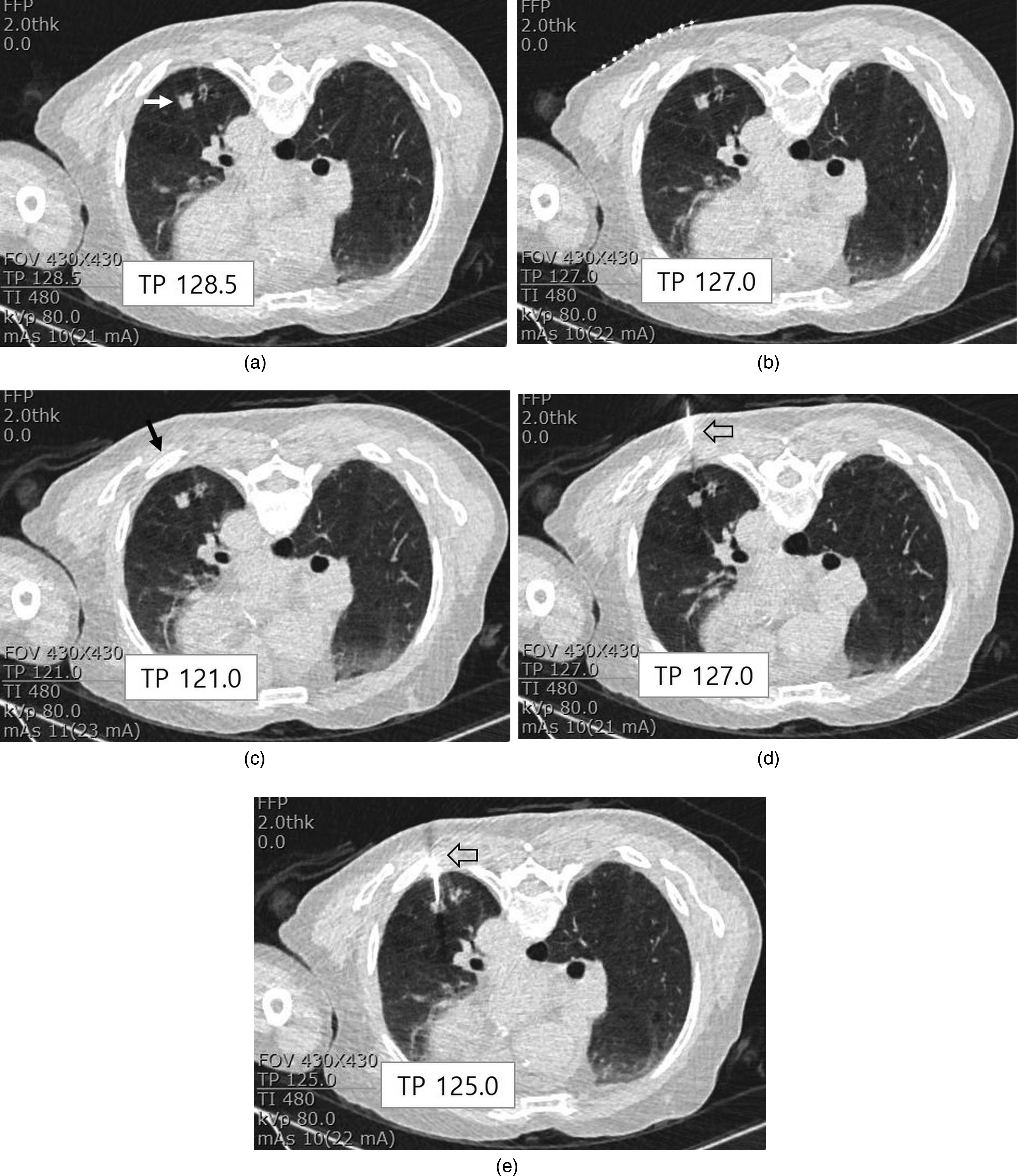
Measurement of the respiratory motion of the target nodule (squamous cell carcinoma) in five serial CT scans during PTNB. (a) A 13-mm target nodule was located at the left lower lobe (white arrow). The TP at the targeting point was 128.5 at the first scan. (b) The TP at the same targeting point in panel (a) was 127.0 in the second scan. (c) The TP at the same targeting point in the third scan was 121.0, which was quite different from previous scans. The third scan was presumed taken at the expiratory phase. The shortest approach course was hampered by the rib (black arrow) of the chest wall. (d, e) The needle (open arrows) was inserted at the inspiratory phase (respiratory targeting performed). The serial TP was 127.0 and 125.0 at the targeting point. The maximal respiratory motion was measured as 7.5 mm (128.5–121.0 = 7.5), and the average motion was measured as 4.7 mm (7.5 + 6 + 0 + 6 + 4 / 5 = 4.7). CT, computed tomography; PTNB, percutaneous transthoracic needle biopsy; TP, table position.
Final diagnosis of the targeted nodule
Non-diagnostic results, such as insufficient specimen, were defined as a technical failure. Among technically successful cases, the final diagnosis for each target nodule was identified as follows (21). First, if the lesion was surgically resected, the diagnosis was based on a surgical pathologic report. Second, if it showed a specific malignant or benign result in non-surgical biopsy, it was accepted for the final diagnosis. Third, non-specific benign lesions were considered benign when they showed decreases or rapid increases (within four weeks) or were stable for at least one year. Fourth, if the lesions were non-specific benign lesions but showed obvious malignancy, they were identified as malignant. Non-specific benign lesions that did not fit the criteria were considered indeterminate and were excluded.
Data collection and image review
A thoracic radiologist who performed the procedures also reviewed the medical records and CT scans to collect data on patient information, nodule characteristics, technical details, dose length product (DLP), technical failure, and complications.
The reviewed CT images were reconstructed axial images with a slice thickness of 2 mm. Respiratory movement of the nodule was measured by the difference of the table position of the targeting point of nodules between multiple CT scans (3–10 scans) performed during tidal volume breathing. The targeting point was determined by one of the operators as the shortest needle route from the skin to the lesion at the patient's position. The level where the nodule is the largest within the shortest distance from the skin was determined as the target point. The maximal respiratory motion was measured by subtraction between the highest and lowest table positions of the targeting point among multiple CT scans (Fig. 1). The average respiratory motion was the average difference between each table position and the lowest table position among multiple scans. The last CT scan after removing the needle and the scans performed after the development of pneumothorax were not included in the measurement. We defined the large respiratory motion to be maximal respiratory motion >1 cm because a previous study observed the motion of lung tumors that are unlikely to exceed 1 cm during quiet breathing (22). The lesions with maximal motion <1 cm were defined as having small motion. Distance from the pleura was measured as the shortest measured distance from the surface of the nodule to the pleura at the corresponding procedural position.
Needle modulation was defined when the table position for the needle puncturing the pleura was changed from that of the first needling scan. The motion artifact was defined when the ghosting of the target nodule was detected on the CT image.
Statistical analysis
The maximal and average respiratory motions according to nodule size, location, and procedural position were assessed by the Mann–Whitney U test or Kruskal–Wallis test. Differences in technical factors, radiation dose, complications, and diagnostic performance between lesions with large motion (maximal respiratory motion >1 cm) and small motion (maximal respiratory motion ≤1 cm) were compared using Pearson chi-square tests, Fisher's exact test, and the Mann–Whitney U test. Sensitivity and diagnostic accuracy were assessed for diagnostic performance. Diagnostic failure was defined as the sum of false negatives, false positives, and technical failures. Technically failed cases (insufficient biopsy specimen) and indeterminate cases (the final result could not be confirmed) were not included when assessing diagnostic performance. To evaluate other factors for technical failure, univariate and multivariate logistic regression analyses were performed using nodule size, location, and position as independent variables. Statistical analyses were performed using SPSS software version 27.0 (IBM Corp., Armonk, NY, USA). P values <0.05 were considered statistically significant.
Results
The characteristics of the 426 pulmonary lesions on which PTNB was performed are summarized in Table 1. The size of the target lesions was 32.0 ± 19.0 mm (range = 5 − 113 cm), and the distance from the pleura was 9.7 ± 12.5 mm (range = 0–69.0 cm). The number of performed CT scans for each procedure was 6.8 ± 2.0 (range = 4–15). The complications after the PTNB procedure included 85 (20.0%) cases of pneumothorax and 38 (8.9%) cases of hemoptysis. Chest tube insertion or immediate aspiration was performed in 6 (1.4%) cases.
Characteristics of targeted pulmonary nodule in percutaneous transthoracic needle biopsy.
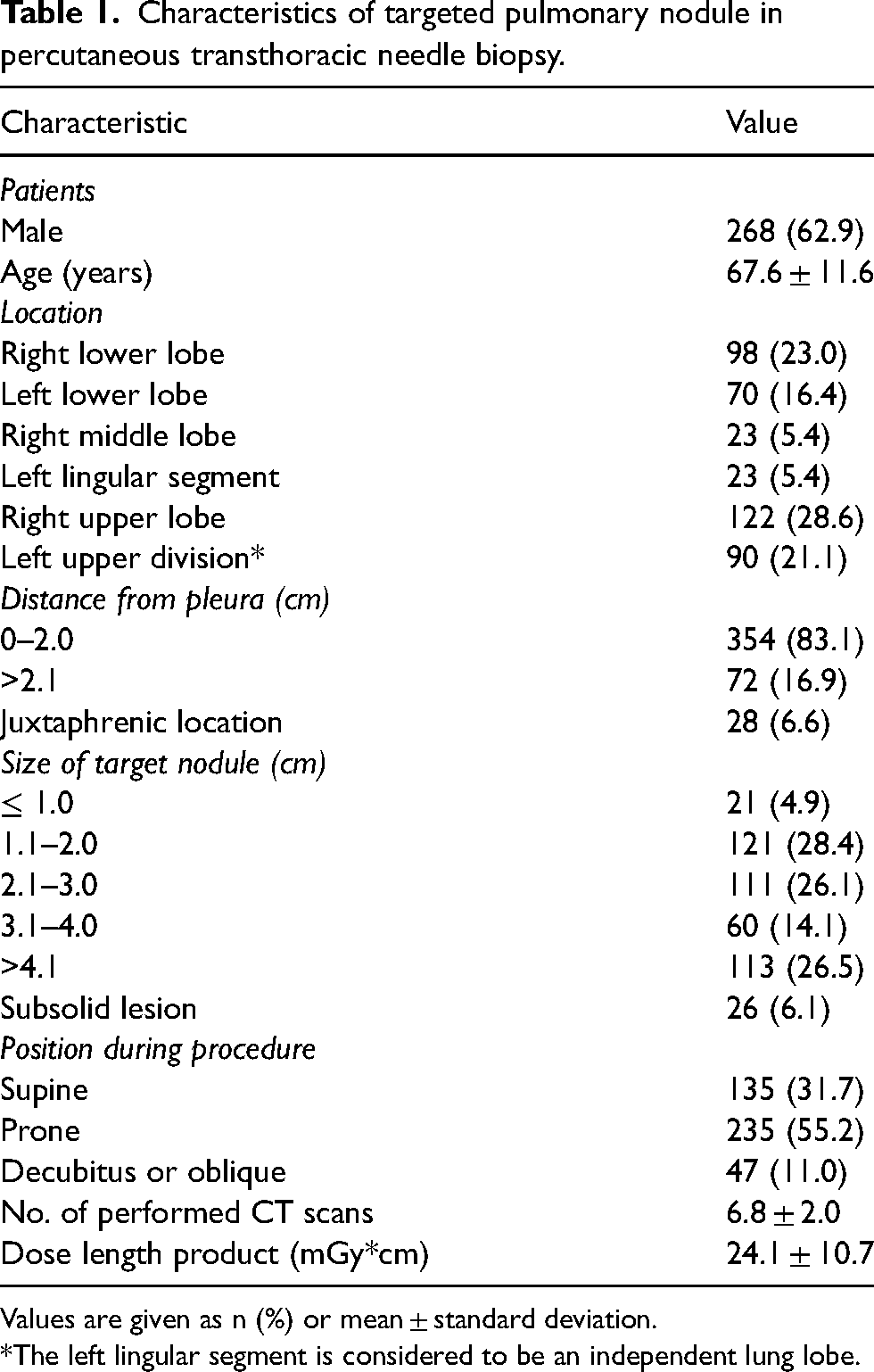
Values are given as n (%) or mean ± standard deviation.
*The left lingular segment is considered to be an independent lung lobe.
Among the 426 procedures, 417 (97.9%) cases were technically successful. Among the 417 lesions, target lesions were confirmed as malignant in 312 cases (269 non-small-cell lung cancer [NSCLC], 16 small-cell lung cancers, 2 lymphomas, 24 metastases from extrapulmonary origin, and 1 radiologically malignant lesion) and benign in 105 cases (62 radiologically benign lesions, 19 tuberculous or non-tuberculous mycobacterial granulomas, 6 hamartomas, 4 fungal infections, 3 inflammatory pseudotumors, 3 organizing pneumonias, 2 schwannomas, 2 sclerosing pneumocytomas, 2 solitary fibrous tumors, 1 lipoid pneumonia, and 1 rheumatoid nodule). Malignant lesions were confirmed by surgical excision (n = 51), specific malignant biopsy following PTNB (n = 254), specific biopsy done by another modality (n = 6), and radiological progression (n = 1). Benign lesions were confirmed radiologically (n = 62) or by specific benign biopsy (n = 40) or surgical excision (n = 3). Among 62 radiologically diagnosed benign lesions, 35 lesions showed improvement on follow-up CT, 26 showed no significant change during the period over one year, and one showed rapid increase in one week.
The mean maximal respiratory motion of all lesions between tidal volume inspiration and expiration among multiple CT scans was 5.4 ± 4.4 mm (range = 0–40). The mean average motion among multiple scans was 2.7 ± 2.6 mm (range = 0–16.0). The maximal motion within 5 mm consisted of 267 (62.7%) lesions, and the average motion within 5 mm consisted of 368 (86.4%) lesions (Fig. 2). The maximal and average respiratory motions of lesions were significantly different according to location (P < 0.001 and P < 0.001, respectively), size (P = 0.006 and P = 0.036, respectively), and position during procedure (P = 0.001 and P = 0.001, respectively (Table 2).

Distribution of the maximal (a) and average (b) respiratory motion measurements in 426 PTNB lesions.
Respiratory motion of nodule according to the size and the location.
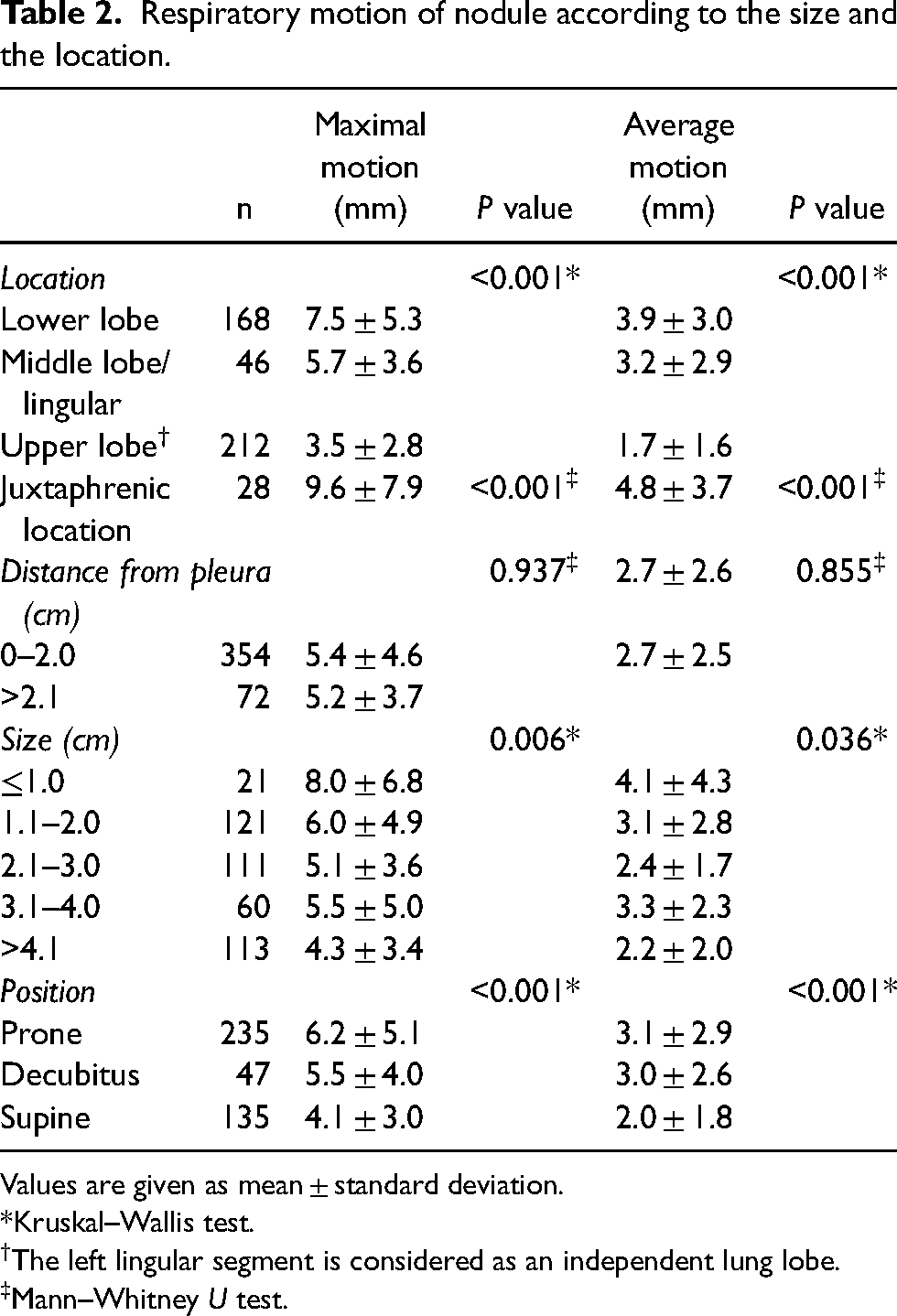
Values are given as mean ± standard deviation.
*Kruskal–Wallis test.
The left lingular segment is considered as an independent lung lobe.
Mann–Whitney U test.
The difference between the lesions with large and small motion is shown in Table 3. The rate of technical failure was 5.6% (3/54) in lesions with large motion, which is higher than 1.6% (6/372) in lesions with small motion (P = 0.093). Respiratory targeting (P < 0.001) and needle modulation (P < 0.001) were required significantly in the lesion with large motion. The number of performed scans was larger in the lesion with large motion (P < 0.001), but the radiation dose (DLP) did not show a statistical difference (P = 0.227). There was no significant difference with regard to complications. The sensitivity and accuracy were 93.1% and 96.1% in the lesion with large motion, respectively, compared with 94.7% and 95.9% in the lesion with small motion, respectively.
Differences of PTNB between large and small respiratory motion.

Values are given as n (%) or mean ± standard deviation. Data in parentheses are percentages.
*Mann–Whitney U test.
Fisher's exact test.
Diagnostic failure was defined as the sum of false negatives, false positives, and technical failures.
CT, computed tomography; PTNB, percutaneous transthoracic needle biopsy.
Logistic regression was used to investigate the effect of various factors on technical failure. Nodules with small sizes (≤10 mm) (P = 0.003), in a juxtaphrenic location (P = 0.005), subjected to respiratory targeting (P = 0.026), and with large motion (10.1–15.0 mm) were independent factors for technical failure in univariate analysis. Small size (odds ratio [OR] = 7.351; 95% confidence interval [CI] = 1.204–44.877; P = 0.031) and juxtaphrenic location (OR = 8.053; 95% CI = 1.598–40.579; P = 0.011) were independent factors in multivariate analysis (Table 4). In a subgroup analysis of nodules ≤30 mm in size, juxtaphrenic location was the only influencing factor for technical failure (OR = 7.800; 95% CI = 1.370–44.413; P = 0.021) (Table 5).
Univariate and multivariate logistic regression analysis for technical failure.

CI, confidence interval; OR, odds ratio.
Univariate logistic regression analysis for technical failure in nodule (≤30mm in size, n = 253).

CI, confidence interval; OR, odds ratio.
Discussion
In this study, the respiratory motion of pulmonary lesions was significant in the lesions in the lower lobe and those with small sizes and in prone position. Large respiratory motion was related to technical difficulties but did not affect diagnostic performance nor complications.
The maximal and average respiratory motion nodules between tidal volume breathing were 5.4 ± 4.4 mm and 2.7 ± 2.6 mm, respectively. Past studies have reported the maximal movement of lung tumors during radiation therapy in the Z direction as in the range of 7.3–12.5 mm, measured in full inhalation–exhalation tidal volume breathing (3,5,23,24). The average movement of quiet breathing in multiple cine scans was measured as 5.0 mm in 166 tumors (22). Free-breathing biopsy is affordable because the respiratory motion under calm breathing status is not significant. Liu et al. (22) stated that tumor motion is unlikely to exceed 1.0 cm during quiet normal breathing, except for small lesions located in the lower half of the lung. We found that lesions of maximal and average motions >1 cm comprise 12.7% and 3.3% of all lesions, respectively. However, in the situation of full inspiration, pulmonary nodules possibly moved up to 25.3 mm (4).
The lower lobe location of nodules driven by diaphragm motion was significantly large, consistent with many studies (4,5,22,23). In the present study, by directly measuring the movement of the nodule, it was confirmed that the movement and variation of juxtaphrenic and small nodules were large, but 79.6% of the juxtaphrenic nodules and 87% of the small-sized lesions showed maximal respiratory motion <10 mm.
Respiratory motion affected the technical problems of the procedure during quiet-breathing biopsy. Respiratory targeting and needle modulation were required frequently in this group. Technical difficulties, such as motion artifact of target and disappearance of target during multiple scans, were also common in large motion groups. These factors led to an increase in the number of procedural scans, potentially lengthening the procedure time. However, these results did not result in an increase of radiation dose nor pneumothorax. We speculate that this is due to our routine biopsy CT scan performed at a low-dose of 80 kVp with 12–15 mAS per slice CT, which has less radiation dose than conventional CT biopsy (15). The incidence of pneumothorax in nodules with large motion (24.1%) was within the acceptable range when compared with that of previous reports (21.7%–28.6%) (1,17,25). We suggest that a nodule with large motion is unlikely to have a major influence on the occurrence of complications.
Despite technical difficulties, the PTNB of large motion did not lower the performance of PTNB. It is apparent that PTNB is a procedure that requires dynamism and agility because the patient and lung parenchyma move (15). Biopsy is possible even during free breathing with large motion: breathing is regular and movement is predictable. Connolly et al. (26) reported that PTNB under general anesthesia was successful because of the consistency of nodule positioning in the chosen respiratory phase. Sedation can help patients to be motionless, have regular shallow respiration, and decrease anxiety (17–19).
According to our multifactorial analysis, nodules of small size or in a juxtaphrenic location were found to be independent factors even when large motion was included in the variables. Even in small nodules, juxtaphrenic location was the only influencing factor for technical failure. Large motion in itself was not the influencing factor for technical failure. It can therefore be inferred that when the target is close to the diaphragm, in addition to large motion, other factors also make the procedure difficult. We speculated that the difficulty in targeting nodules with small sizes or in juxtaphrenic locations was not only due to large motion but also large variation. Standard deviations of maximal motion of target nodules with small size or juxtaphrenic location were higher than other nodule conditions. The incidence of diagnostic failure or non-diagnostic pathologic results are reported to be high even in breath-holding or real-time procedures (9,10,24). When patients are asked to hold their breath, they tend to breathe deeply or perform Valsalva maneuvers (8), resulting in significant variations in nodule motion between different respiratory phases (4). In addition, if the patients are anxious, the possibility of targeting failure increases because the breathing pattern becomes irregular and unpredictable (27). Avoiding the diaphragm and accurate targeting of small nodules might be challenging tasks regardless of respiratory movement.
The present study has some limitations. Owing to its retrospective nature, there was a lack of standardization among operators and variables. Respiratory motion measurement was not automatic. However, this study is focused on the motion of a PTNB target and not of a whole tumor. The tumor approach strategy may vary at the discretion of the operator. Second, the performance and complications of quiet-breathing biopsy were not compared with those of standard breath-holding biopsy. Further studies are necessary to confirm the effect of free-breathing puncture. Another limitation was the presence of 15 indeterminate cases for which diagnoses could not be confirmed.
In conclusion, respiratory motion may affect some technical difficulties in CT-guided lung biopsy. However, the diagnostic performance and complication rate were acceptable regardless of motion in quiet-breathing biopsy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by 2021 Inje University Busan Paik Hospital research grant.
Correction (February 2023):
This article has been updated to correct the funding statement since its original publication.