
Abstract
Background
There have been conflicting outcomes regarding the use of lidocaine to reduce pain after uterine artery embolization (UAE).
Purpose
To investigate the efficacy of intra-arterial lidocaine injection for pain and inflammatory response control within 24 h of UAE for symptomatic uterine fibroids.
Material and Methods
Of 1530 patients who underwent UAE for uterine fibroids in 2007–2021, 5 mL of 1% lidocaine was injected into each uterine artery immediately after UAE in 23 patients. A disease-matched control group (n = 23) who did not receive intra-arterial lidocaine was generated from the same registry. The pain score, white blood cell (WBC) count, C-reactive protein (CRP), neutrophil/lymphocyte ratio (NLR), and fentanyl consumption were compared before and after UAE. Complete infarction of the dominant fibroid was assessed using magnetic resonance imaging.
Results
Significantly lower WBC count, CRP level, and NLR were noted 24 h after UAE in the lidocaine group. No statistically significant difference was noted in the pain score between groups at 0–24 h. The cumulative fentanyl dose administered during the first 24 h after UAE was not significantly different. After embolization, fibroid-related symptoms resolved in all patients. No significant difference was observed in the rate of complete infarction of the dominant fibroid.
Conclusion
Lidocaine administration immediately after UAE resulted in a significant reduction in the inflammatory response. However, such a difference in the inflammatory reaction did not contribute to significant reductions in pain scores or fentanyl consumption.
Introduction
Uterine artery embolization (UAE) is a well-established treatment modality for symptomatic fibroids and has been offered to women who wish to retain their uterus (1,2). However, post-embolization syndrome occurs in most patients undergoing UAE. In particular, postprocedural pain usually peaks 6–8 h after UAE and persists for up to 24 h (3,4). This has been attributed to the inflammatory response induced by ischemia of the fibroids and uterine tissue (5–7). Various attempts, such as patient-controlled analgesia (8) and superior hypogastric nerve block (9), have been made to minimize patient discomfort after the procedure.
Notably, the efficacy of intra-arterial lidocaine injection after UAE has been investigated in previous studies (10–13). However, conflicting outcomes exist regarding the use of lidocaine to reduce postprocedural pain. A recent meta-analysis reported that postprocedural pain at 4 h and narcotic dose after UAE were significantly decreased by lidocaine injection use (14). In contrast, Kastumori et al. reported no such benefits in their retrospective analysis (15). In addition, the impact of lidocaine on the inflammatory response after UAE has not been thoroughly investigated. In our study, we analyzed the inflammatory markers, such as C-reactive protein (CRP) levels, white blood cell (WBC) count, and neutrophil-to-lymphocyte ratio (NLR), which were collected to evaluate the inflammatory response after UAE.
The aim of the present study was to retrospectively evaluate the efficacy of intra-arterial lidocaine injection in reducing fentanyl consumption, pain, and inflammatory response during the first 24 h after UAE.
Material and Methods
Patient selection
This study was approved by the institutional review board, and the requirement for informed consent was waived because of the retrospective nature of the study. Between January 2007 and December 2021, 1530 patients underwent UAE for symptomatic fibroids. Data of patients who received intra-arterial lidocaine administration after embolization of the uterine artery were extracted from our UAE registry, and their medical records were collected (n = 23). A disease-matched control group who did not receive intra-arterial lidocaine was also generated from the same registry (n = 23).
Procedure details
UAE was performed by a single radiologist with 25 years of experience in interventional radiology. The unilateral right femoral artery was accessed in all patients. A 5-F catheter (RHR catheter, Cook Medical, Bloomington, IN, USA) was placed into the internal iliac artery, and a 2.3-F microcatheter (Radiomate, S & G, Yongin, Korea) was co-axially advanced into the uterine artery. Embolization was performed with the catheter tip placed distal to the cervicovaginal branch using polyvinyl alcohol particles (PVA) (Bearing, Merit medical, Utah, USA).
PVA particles were mixed in a ratio of 1:1 with a 60-mL solution of normal saline and a contrast agent. In total, 1–2 vials of 355–500 PVA particles were injected at the beginning of the procedure into each uterine artery, and the size of the PVA was increased to 500–700 towards the endpoint. The endpoint of embolization was the complete cessation of blood flow in the uterine artery for 10 cardiac beats. In the lidocaine group, 5 mL (50 mg) of 1% lidocaine was slowly injected into the uterine artery immediately after the endpoint of embolization was achieved. The same technique was applied to the contralateral side. A total dose of 100 mg of lidocaine was administered. All patients received intravenous (IV) patient-controlled analgesia (PCA) (Accumate1100; Wooyoung Medical, Seoul, Republic of Korea) 24 h after the procedure. The PCA regimen included fentanyl (Hana Pharm, Seoul, Republic of Korea) and 0.3 mg ramosetron, all of which were mixed with normal saline solution to a total volume of 150 mL. The bolus dose was 2 mL at a basal infusion rate of 1 mL/h, with a lockout interval of 10 min. Therefore, fentanyl was delivered at a rate of 10 µg/h, with a bolus dose of 20 µg.
Technical success was defined as successful embolization of the bilateral uterine arteries. Clinical success was defined as an improvement or resolution of preprocedural symptoms after UAE. Complete infarction was defined as no evidence of perfusion of the leiomyoma on contrast-enhanced magnetic resonance imaging (MRI). Follow-up visits were scheduled at three weeks and three months after UAE.
MRI
All patients underwent a preprocedural MRI (3-T Signa HD/HDx; GE Healthcare, Waukesha, WI, USA) of the pelvis and a follow-up MRI three months after UAE. Enhanced MRI was performed 2 min after the IV infusion of 10 mL gadolinium chelate (Dotarem, Guerbet, France).
Data collection
Patient characteristics, including age, sex, predominant tumor diameter, and uterine volume (length × width × height × 0.5233) (16), were recorded. Pain was evaluated using an 11-point pain score. Before the procedure, the patients were instructed to express their pain on a scale of 0–10 (0 = no pain at all; 10 = worst pain imaginable). Pain scores at 0, 1, 2, 4, 6, 8, 12, and 24 h after the procedure were recorded. Data on inflammatory markers, such as WBC count, NLR, and CRP, were collected before the procedure (1 day before UAE) and after the procedure at 24 h. The postprocedural doses of IV fentanyl were measured at 6, 12, 18, and 24 h using a PCA device (in which the quantities of the drug delivered were automatically recorded every 30 min, and later the data were transferred to a computer for analysis). Adverse events were classified as minor or major according to the reporting standards for UAE (17).
Statistical analysis
All statistical analyses were performed using SPSS version 26 (IBM Corp., Armonk, NY, USA). Normality of distribution was tested using a q-q plot and the Shapiro–Wilk test. Parametric data were analyzed using the independent t-test, and non-parametric data were analyzed using the Mann–Whitney U test. Categorical variables were evaluated using the chi-square or Fisher's exact test when appropriate. A repeated-measures analysis of variance was performed to compare repeated-measures variables (fentanyl consumption and pain score), with Bonferroni correction for multiple comparisons. All values are expressed as the mean ± SD, median, or number of patients. P values less than .05 were considered to indicate a statistically significant difference.
Results
There were no significant differences in baseline characteristics between the two groups (Table 1). Bilateral embolization of the uterine arteries was successfully performed in all patients. All patients experienced improvement or resolution of symptoms. The mean uterine volume and rate of complete necrosis of the dominant fibroids were not significantly different at three months (Table 2). One patient experienced bradycardia and transient loss of consciousness when she received the lidocaine injection. She regained consciousness and was stabilized immediately after atropine administration.
Baseline characteristics.
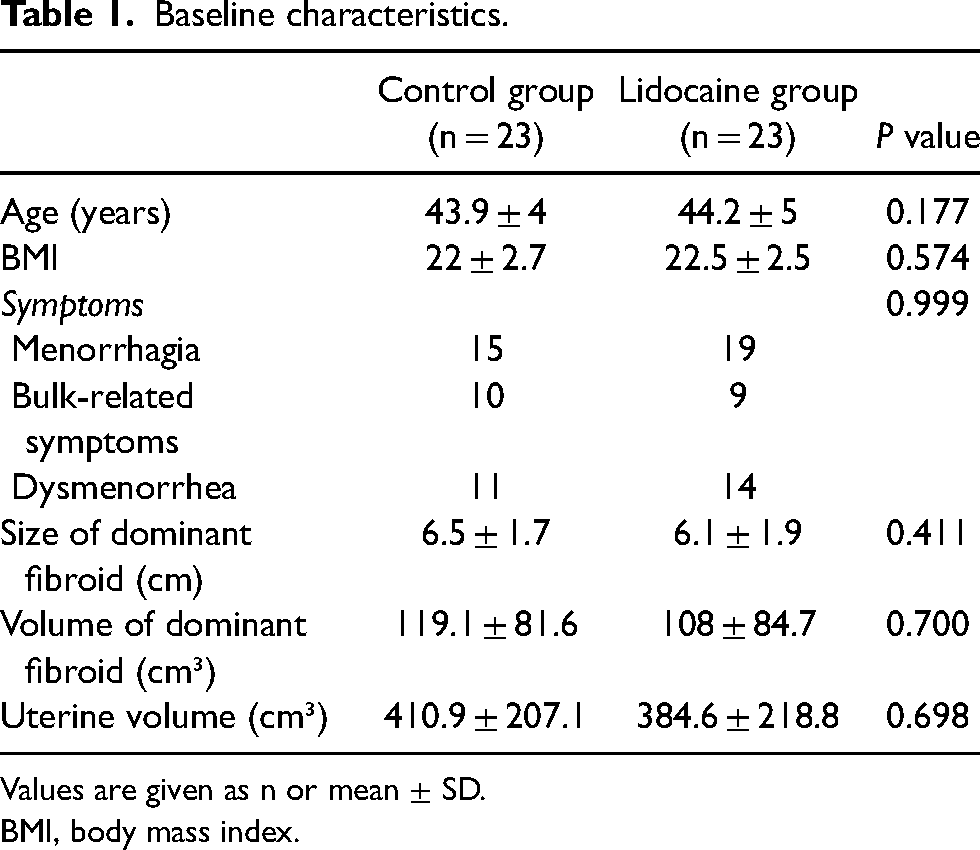
Values are given as n or mean ± SD.
BMI, body mass index.
Procedural data.
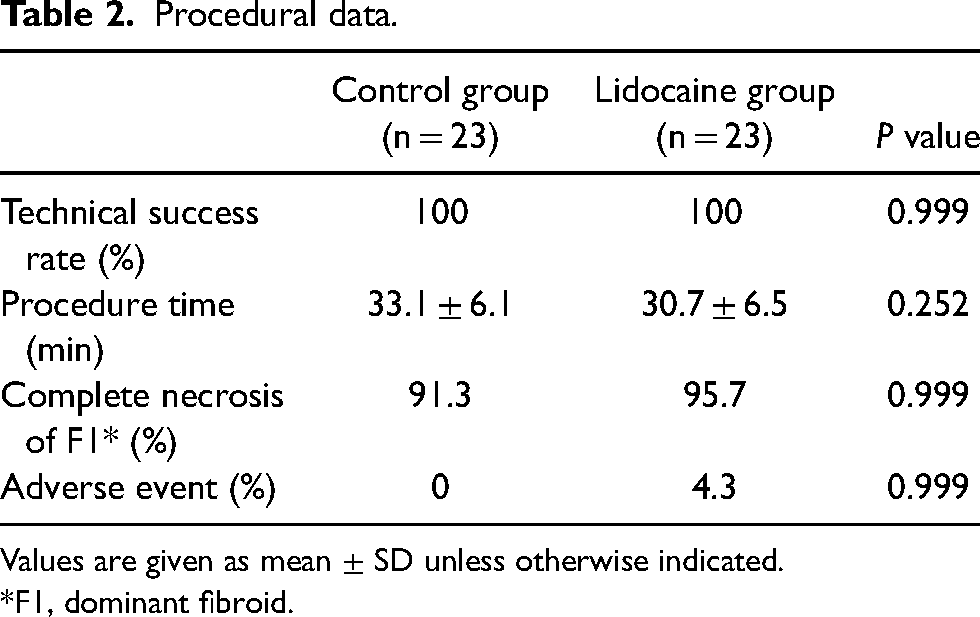
Values are given as mean ± SD unless otherwise indicated.
*F1, dominant fibroid.
Differences in inflammatory response
Inflammatory markers, such as CRP, WBC count, neutrophil percentage, lymphocyte percentage, and NLR, were not significantly different between the two groups before UAE. CRP values at 24 h were lower in the lidocaine group than in the control group (17.4 ± 11.1 vs. 6.8 ± 7.4; P = 0.001). The WBC count at 24 h was lower in the lidocaine group than in the control group (10,883 ± 3159 vs. 8872 ± 2980; P = 0.043). NLR was lower in the lidocaine group than that in the control group (8.3 ± 3.4 vs. 6.5 ± 2.3; P = 0.049) (Fig. 1).

Inflammatory markers before and 24 h after UAE. Bar graphs illustrate changes in (a) white blood cell (WBC) count, (b) C-reactive protein (CRP), and (c) neutrophil-to-lymphocyte ratio (NLR) from before UAE to 24 h after the procedure. *P<0.05 , versus the control group. UAE, uterine artery embolization.
Pain score and medication
No statistically significant differences were observed in the pain score at each time point between the control and lidocaine groups at 0, 1, 2, 4, 6, 8, 12, and 24 h (Fig. 2). The cumulative fentanyl dose during the first 24 h after UAE was not significantly different between the two groups (1037 ± 573 μg in the lidocaine group vs. 881 ± 419 μg in the control group; P = 0.338).

Graphs show the pain score (0–10) for pain ≤24 h after uterine artery embolization.
Discussion
The present study showed that intra-arterial administration of lidocaine immediately after UAE with non-spherical PVA particles led to significant reductions in the inflammatory response 24 h after UAE but did not contribute to significant reductions in pain scores or the quantity of narcotics used.
Lidocaine is a widely used amino-amide-type local anesthetic that exerts anti-inflammatory effects in the acute postoperative setting by inhibiting the release of pro-inflammatory cytokines, such as leukotriene B4 and histamine (18). A reduction in postprocedural pain after UAE in prior studies was assumed to be associated with the anti-inflammatory effect of lidocaine. However, the effect of intra-arterial lidocaine injections on the inflammatory response after UAE has not been thoroughly investigated. In the present study, various inflammatory markers, such as the WBC count, CRP level, and NLR, were collected. In particular, NLR has not been investigated in prior studies and it is known to be a more sensitive marker of the extent of inflammation than measures of either neutrophil or lymphocyte alone as it reflects changes in both cell types (19). The levels of these markers were not significantly different before the procedure. However, 24 h after UAE, there were significant differences in inflammatory markers, suggesting the anti-inflammatory effect of intra-arterial lidocaine injection in UAE.
Neither pain scores at different time points nor the highest pain score during the first 24 h after UAE were significantly different between groups, and no significant reduction in the cumulative amount of narcotic agent was observed in this study. Patients in the lidocaine group experienced non-significantly less pain at 1 h in this study, which is in line with the findings of Katsumori et al., who found lower pain scores in the lidocaine-treated group at 3 h that failed to reach statistical significance (15). In contrast, both Duvnjak et al. and Noel-Lamy et al. reported significant pain reduction in the lidocaine group in the first hours after UAE (11,13). A possible explanation for such discrepancies is that the dose of lidocaine (100 mg) administered in this study was lower than that reported in other studies that reported significant pain reduction. However, Zhan et al. reported a significant reduction in pain in the lidocaine group with a 40-mg lidocaine injection (10). Thus, the dose of lidocaine did not seem insufficient in the present study, and further studies are warranted to determine the optimal lidocaine dose.
In addition, procedure techniques, including the embolization endpoint and types of embolic agents (microspheres vs. PVA), also differ between studies. In particular, the inflammatory responses after UAE using PVA and microspheres were not equal (7), which might have affected the intensity of postprocedural pain. Different pain management protocols, other than intra-arterial lidocaine, could be another reason for the different outcomes. While morphine was primarily used by other investigators, IV fentanyl was primarily used for pain control in the present study (10–12).
Severe vasospasm has been reported to occur when lidocaine is administered into the uterine artery before embolization (12). In a study by Noel-Lamy et al., patients who received lidocaine mixed with PVA particles showed a significantly lower rate of complete infarction on the three-month follow-up MRI. Vasospasm caused by lidocaine is assumed to impede the effective delivery of embolic material to fibroids. The rates of complete infarction and symptom improvement were not significantly different between groups. This is in accordance with previous studies in which lidocaine was injected immediately after UAE (11,15).
The present study has some limitations. First, this was a non-randomized retrospective analysis with a small sample size. However, the effect of lidocaine on the inflammatory response after UAE has been rigorously evaluated with various inflammatory markers. Second, additional non-narcotic analgesics were used along with IV PCA, which might have masked the differences in pain between groups after the procedure.
In conclusion, the present study showed that intra-arterial lidocaine administration into the uterine artery immediately after embolization was equally effective for symptomatic fibroids and resulted in significant reductions in the levels of various inflammatory markers. However, such differences did not translate into significant differences in pain scores and the amount of narcotic analgesic used after the procedure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.