
Abstract
Background
Central catheter-related thrombosis (CRT) is the most common catheter-related complication in patients with end-stage renal disease (ESRD) but is often underappreciated and misdiagnosed by radiologist.
Purpose
To find the computed tomography angiography (CTA) characteristics of central CRT, then raise the diagnosis of this disorder.
Material and Methods
A total of 301 eligible patients with ESRD who experienced both chest multi-phase multidetector CTA (MDCTA) and digital subtraction angiography were enrolled in the final analysis. The location, shape, and related signs of the central CRT in MDCTA images were evaluated. Independent-samples T test, chi-square test, and binary logistic regression were analyzed using SPSS software.
Results
In total, 166 patients were found to have CRT using MDCTA, and this was verified by DSA. Central CRT was usually irregular in the superior vena cava segment, and the angle of the contact area between central CRT and catheter was <180° (all P < 0.05). Age, collateral circulation, and venous stenosis were shown to have significant differences when compared to patients without CRT (all P < 0.05), but there were no significant differences about the sex or catheter insertion site. In addition, age and collateral circulation were the factors found to be significantly associated with thrombosis (P < 0.05). In particular, the thrombosis was 2.213 times more likely to be found in those patients with collateral circulation (odds ratio = 2.213, 95% confidence interval = 1.236–3.961).
Conclusion
Chest multi-phase MDCTA can effectively reduce the missed diagnosis and misdiagnosis of central CRT. It is worth paying more attention to the central CRT especially when the collateral circulation is observed.
Keywords
Introduction
Central venous catheters (CVCs) are the most common invasive procedures applied in hemodialysis therapy for end-stage renal disease (ESRD) (1). As the use of CVCs has increased, so too have the complications associated with them. More than 15% of patients with CVCs have significant complications (2). Catheter dysfunction due to occlusion/thrombosis is found to be the most common catheter-related complication in hemodialysis patients (3). The rates of catheter-related thrombosis (CRT) were found to be in the range of 10%–80%, based on patient population, risk factors assessed, and study methodology (4). In addition, the presence of thrombosis on a catheter provides a fertile microenvironment for bacteria to grow, increasing rates of bacterial colonization (5) and catheter-related sepsis (6,7). Other uncommon complications, such as pulmonary embolism, right heart thromboembolism, superior vena cava syndrome, and paradoxical embolism to the systemic circulation, are yet potentially to threaten the patients’ life (8,9). Therefore, the incidence of central CRT impacts on patient morbidity and mortality.
The diagnosis of central CRT can have important consequences for patients and confront clinicians with important clinical management dilemmas including the decision to keep or remove the CVCs, type of treatment, and duration of anticoagulation (9). In addition, when extubation is required, a clear diagnosis of CRT before extubation can indicate the risk of secondary pulmonary embolism in advance. Digital subtraction angiography (DSA) was considered the gold standard in detecting thrombosis, particularly in patients with CVCs. However, this method is not applicable as a routine procedure because of its invasiveness. DSA is suggested in cases only where imaging is negative but clinical suspicion is high (10) . Nowadays, there are several imaging methods that are widely used in the diagnosis of CRT. Vascular ultrasonography is a common method of assessing CRT of anatomically accessible veins such as the jugular, axillary, and distal subclavian veins, but is inappropriate in the superior vena cava (SVC) due to the overlying bones and lungs (4). Magnetic resonance angiography can assess vascular problems but with a long scan time, the metal of the catheter interferes (11). Multidetector computed tomography angiography (MDCTA) is a common examination for CRT because it can provide information detailed about the catheters and veins (11,12), especially the wide use of low-dose computed tomography (CT) in recent years. As some studies about central CRT have reported (13–16), appropriate window values and multi-plane CT reconstructions were found useful in the diagnosis of catheter-related complications and reduced the missed diagnosis of thrombosis (14,16). However, central CRT is still underappreciated and misdiagnosed when evaluated by CT. One reason is that the catheter artifacts and the heterogeneous density caused by the contrast material in the clinic make the diagnosis of central CRT difficult for the radiologist. Another reason is that the image characteristics of central CRT are unclear due to the limited image studies. The image characteristics of central CRT still need to be summarized.
The aim of the present study was to retrospectively review and analyze the location, shapes, and related signs of central CRT evaluated by MDCTA with multi-phase scanning in patients with ESRD. We hope these findings can help clinicians and radiologists to raise correct the diagnosis of this disorder and reduce the use of DSA. This is also helpful for the selection of treatment methods.
Material and Methods
This retrospective study was conducted at our institution. The institutional review board approved the study before data collection. Patients were enrolled between January 2014 and December 2021 using the following criteria: (i) patients on maintenance hemodialysis through tunneled-cuffed catheters admitted with catheter dysfunction; and (ii) patients who received both MDCTA and DSA. For those patients with repeated MDCTA exams, only the first obtained MDCTA study of the chest was considered for each patient to simplify the subsequent data analysis. The exclusion criteria were severe multi-system disease, poor image quality, and device tip not included in the scanned field.
All patients were scanned using MDCTA (Somatom Definition; Siemens Medical Solutions, Forchheim, Germany) with 64- or 128 × 2 detector rows. A 20-gauge needle was punctured at the antecubital vein for injections of 70–80 mL of mixed contrast material (370 mg/mL; Bracco Sine Pharmaceutical Corp. Ltd., Shanghai, PR China) at 4 mL/s by a dual-head power injector (Stellant; Medrad, Indianola, PA, USA) followed by 20 mL saline flush. Multi-phase scanning protocols (100–120 kV, 70–80 mAs), including non-contrast phase, pulmonary arterial phase, and pulmonary venous phase, were employed for data acquisition. Scanning was triggered automatically with bolus tracking and the region of interest was placed in the pulmonary trunk, with a threshold of 100 Hounsfield units, and a waved delay scanning about 14 ± 6 s for the venous phase was employed for data acquisition.
The raw data were transferred to an online workstation (Leonardo; Siemens Medical Solutions), and then loaded into three-dimensional software (Syngo 3D; Siemens Medical Solutions) on the workstation. Reconstruction images were built using multi-planar reformation (MPR), maximum density projection (MIP), and the volume-rendering technique (VRT). The CT images were reviewed by a primary radiologist and a senior radiologist, blinded to the primary diagnosis. The discrepancy in analysis was resolved by consensus after another senior radiologist reviewed the images.
Continuous variables were expressed as mean ± standard deviation. Differences between the groups were examined in terms of continuous variables via independent-samples T test. Categorical variables were expressed as absolute numbers (percentage) and analyzed with the chi-square test and non-parametric test. The binary outcomes of thrombosis (= 1) and no thrombosis (= 0) were employed as the dependent variable. The independent variables were age, sex, catheter insertion site, catheter tip location, collateral circulation, and vascular stenosis. In this study, vascular stenosis was defined as moderate to severe stenosis of vein lumen. Data with P < 0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 23.0.
Results
A total of 301 eligible patients were enrolled in the final analysis. In total, 166 patients with thrombosis were found using both MDCTA and DSA, and 135 patients without thrombosis were verified by both MDCTA and DSA as the control groups. Among the patients with thrombosis, 38.6% were retrospectively found to have CRT but were missed at the initial clinical diagnosis. Typical patients with thrombosis are shown in Fig. 1. Tables 1 and 2 present the comparisons of the patients’ baseline data and the characteristics of thrombosis.
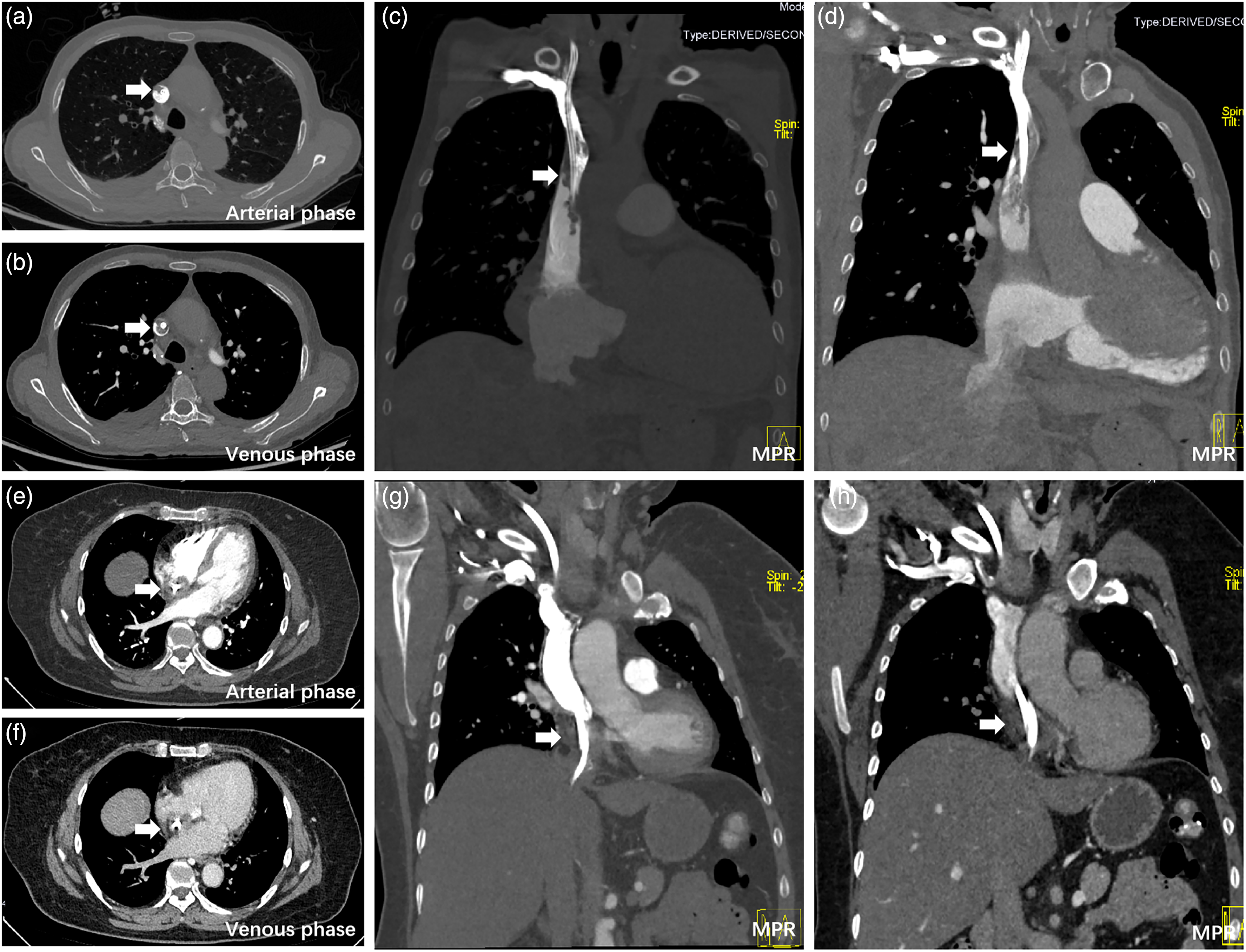
Typical chest multi-phase MDCTA images in different patients with central CRT. (a–d) Patient 1, in whom the central CRT is located in the SVC, (a, c) The same arterial phase; (b, d) the same venous phase. (a, c) A smaller thrombosis range caused by the heterogeneous density of contrast is observed. (e–h) Patient 2, in whom the central CRT is located in the RA. (e, g) The same arterial phase; (f, h) the same venous phase. Arrows show the central CRT. CRT, catheter-related thrombosis; MDCTA, multi-phase detector computed tomography angiography; RA, right atrium; SVC, superior vena cava.
Comparisons of the baseline data of patients with and without thrombosis.
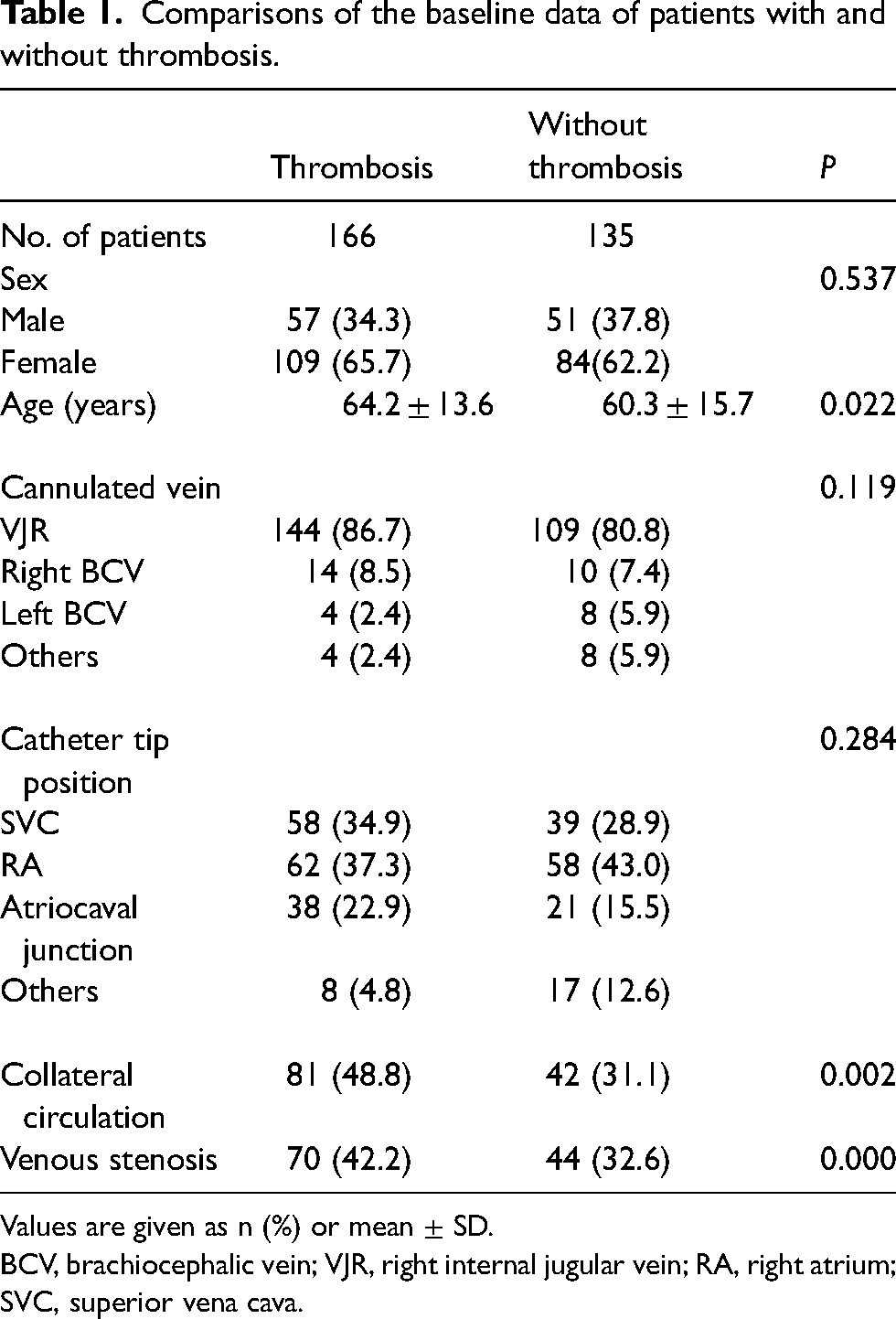
Values are given as n (%) or mean ± SD.
BCV, brachiocephalic vein; VJR, right internal jugular vein; RA, right atrium; SVC, superior vena cava.
The imaging characteristics of central CRT.
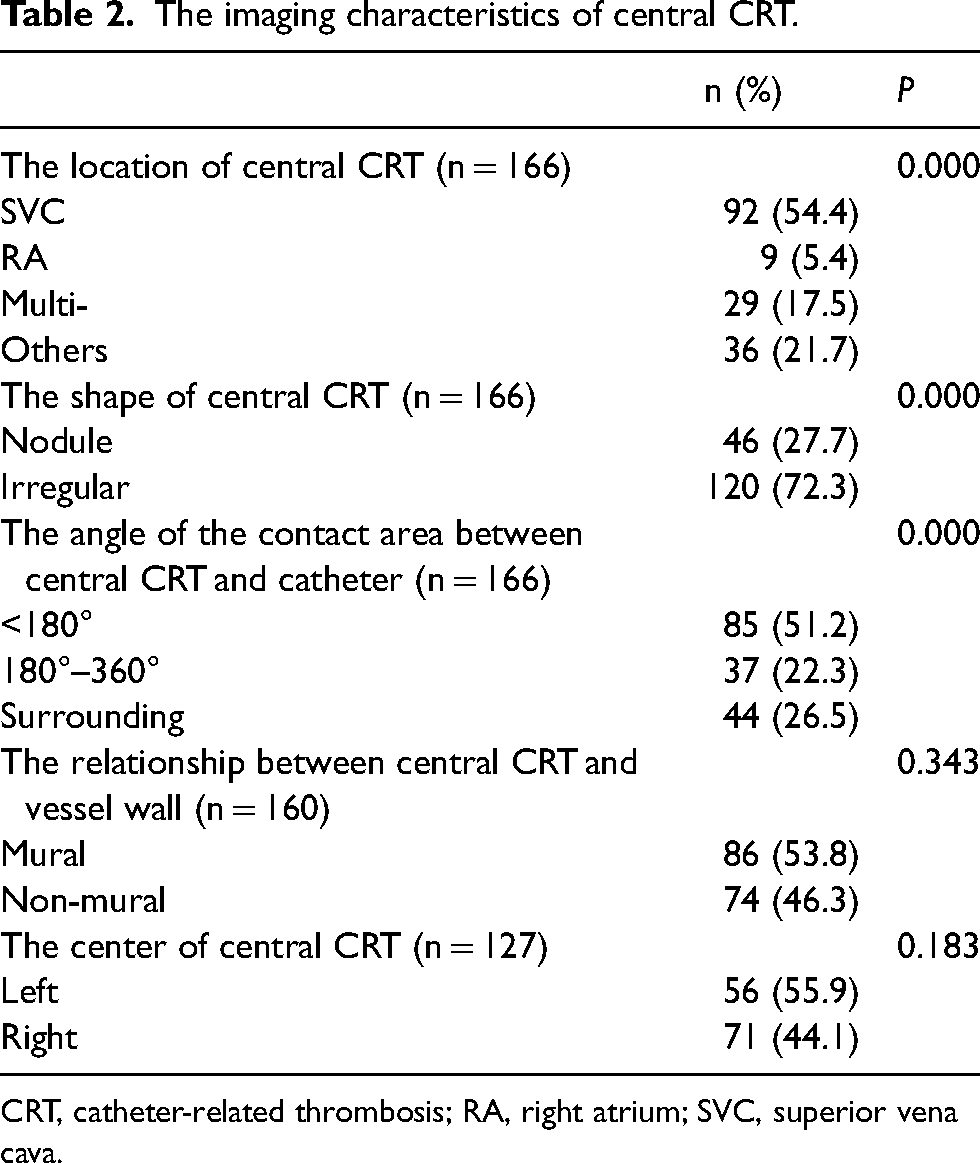
CRT, catheter-related thrombosis; RA, right atrium; SVC, superior vena cava.
Of the patients shown in Table 1, the age, collateral circulation, and venous stenosis showed significant differences when comparing the patients with thrombosis to the patients without thrombosis (P = 0.022, 0.002, and 0.000, respectively). There were no significant differences with regard to sex, the cannulated vein, and catheter tip position between the patients with thrombosis and without.
For the characteristics of thrombosis detected using chest MDCTA (Table 2), the thrombosis was mainly found in the SVC (P = 0.000), the shape of thrombosis was mostly irregular (P = 0.000), and the angle of the contact area between the central CRT and catheter was usually <180° (P = 0.000). There was no statistical difference where the thrombosis was mural (P = 0.343) or where the center of thrombus was left or right (P = 0.183).
Overall, the binary logistic regression model was able to evaluate the related factors of thrombosis (chi-square = 19.968, P = 0.003) (Table 3) and explained the variability of 62.5% of thrombosis occurring. Age and collateral circulation were the factors found to be significantly associated with thrombosis (P < 0.05). In particular, the thromboses were 2.213 times more likely to be found in collateral circulation (odds ratio [OR] = 2.213, 95% confidence interval [CI] = 1.236–3.961) (Fig. 2).

Two patients with thrombosis, venous stenosis, and collateral circulation. Arrows show the central catheter-related thrombosis, arrowheads show the venous stenosis, and white star shows the collateral circulation. (a–c) Patient 1; (d–f) patient 2.
Logistic regression predicting likelihood of thrombosis based on sex, age, cannulated vein, catheter insertion location, collateral circulation, and venous stenosis.

CI, confidence interval; OR, odds ratio; SE, standard error.
Discussion
MDCTA has been used to evaluate venous thrombosis for many years. In total, 65%–75% of thrombus were missed at the initial clinical diagnosis (14,17) but were retrospectively found by changing the window setting. In the present study, 38.6% of thromboses were noticed retrospectively but missed at initial clinical diagnosis. We further confirm multi-phase MDCTA of the chest is helpful to diagnosis central CRT. The number of misdiagnoses was also decreased due to more information obtained to identify the extent and size of the thrombosis. CRT was considered when a relatively stable low density or mixed density surrounded the catheter in both the arterial and venous phases. The problems—such as not enough enhanced blood to reach the veins containing the catheter, the mix of unenhanced blood coming from a vein, and the enhanced blood coming from another confluent vein (14)—were effectively avoided when setting appropriate window values in the both phases.
In the present study, the characteristics of the central CRT from CT images were found to be mostly located in the SVC, usually irregular, and with an angle <180° between the central CRT and catheter in the contact area. These would also be helpful for the diagnosis of central CRT. Moreover, the lack of experience and ignorance of a central CRT diagnosis were also the main reasons for the missed diagnosis of CRT in the initial clinical diagnosis. Radiologists should always carry out a complete thoracic and vascular assessment in the population with CVCs, especially in those patients with ESRD who experience catheter dysfunction.
In the present study, collateral circulation was found to be the most significant factor associated with thrombosis. When collateral circulation is observed around the neck and upper thorax, it is 2.213 times more likely to find thrombosis. The reason might be that the vein developed stenosis to some extent after insertion of the CVC (11). The major intrathoracic veins (subclavian vein, brachiocephalic vein, and SVC) were affected with central vein stenosis (8), which might result in the opening of the collateral circulation. The central CRT could increase the extent of stenosis, and even embolism (18), and then increase the risk and extent of collateral circulation (19). In another study, Phadke et al. found that patients presenting with venous collateralization might be more susceptible to recurrent thrombosis (20). It is worth paying more attention to the central CRT when collateral circulation is observed. We also found that older patients were more likely to have thrombosis. Previous studies agreed that age was one of the strongest risk factors for venous thromboembolism (4), and the risk of thrombosis was found to increase exponentially with age in both adult men and women (21).
Some studies found that catheter tip location was one of the important predictors of CRT (10,22,23). However, catheter tip location was not one of the key factors for thrombosis in our study. We thought there were serval reasons. First, our model increased two factors, collateral circulation and venous stenosis, which were shown to be more significantly associated with thrombosis, and may probably reduce the importance of catheter tip location. Second, in some previous studies, the catheter tip locations were only divided into the SVC and right atrium, which did not subdivide to the right atrium and atriocaval junction (13). Third, we did not assess the relationship between intra-catheter thrombosis and catheter tip position due to the limitation of the intraluminal thrombosis observed by CT, which might lead to some differences compared to the other studies. In addition, we found there was the highest incidence of central CRT when the catheter tip was located in the right atrium in this study without a statistical difference. This might be due to that the catheter tips in this study were mostly located in the right atrium in patients with ESRD. Considering the adverse events when the tip was located in the right atrium—such as myocardial perforation, cardiac tamponade, and severe arrhythmias (10,24)—we thought it would be best to avoid the tip located at the right atrium to minimize the risk of thrombosis and cardiac complications. Radiologists need to remind the clinician about the catheter tip location to avoid possible complications.
The present study has some limitations. First, we only analyzed the thrombosis surrounding the catheter because of the limitation of the intraluminal thrombosis observed by CT. Second, the metal artifact produced by the catheter will inevitably interfere with our image observation, so other techniques are needed. For example, demetallization imaging using dual-energy imaging helps us reduce the artifacts caused by the catheter, which is more conducive to accurately determine whether there is thrombosis. In addition, for patients with CRT undergoing repeated CT examinations, the changes after thrombosis treatment are also needed for comparison, which can help the clinician change the treatment plan in a timely manner.
In conclusion, chest multi-phase MDCTA can clearly display the characteristic CTA findings of central CRT in patients with ESRD, help to reduce the missed diagnoses and misdiagnoses of central CRT, and is helpful for the selection of clinical treatment methods. In particular, when collateral circulation is observed, it is worth paying more attention to recognize central CRT on MDCTA. Multi-phase MDCTA of the chest is recommended when central CRT is highly suspected clinically, or when ultrasound or magnetic resonance imaging has been performed but no cause of catheter dysfunction has been found. With the reduction of missed diagnoses and lower rate of misdiagnoses, it may substantially reduce the use of DSA or other imaging to some extent, as well as removing the catheter unnecessarily.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.