
Abstract
Background
In supracondylar humerus fractures (SCHF), the most frequently used method to calculate rotation is the Gordon lateral rotation percentage (GLRP) defined by Gordon et al. However, this technique includes only typical fractures (49%–80% of all fractures) from the Johns Hopkins (J-H) fracture classification system.
Purpose
The aim of the study was to investigate (1) is Gordon criteria useful for John Hopkins subgroups of supracondylar fractures and (2) is Gordon criteria affected by internal and external rotation.
Material and Methods
This study was designed using four pediatric left humerus bones obtained from the Sawbone© company. For each bone, an osteotomy was made to mimic each of the J-H coronal fracture patterns. The cut bones were placed in a wooden rotation apparatus. The GLRP measurements were taken by five blinded observers.
Results
In the repeated measurements of the observers, <20° rotation typical and <30° medial oblique and lateral oblique fracture pattern were measured as within the limits of an acceptable amount of rotation according to the Gordon criteria. However, for high fracture pattern (HFP), ≤30° internal rotation and <60° external rotation were determined to be within the acceptable rotation criteria according to the Gordon criteria.
Conclusions
All fracture patterns have different characteristics; however, based on the data of this study, the Gordon criteria can be used safely for typical, medial oblique, and lateral oblique fracture patterns but it is necessary to lower the acceptable rate of 50% for HFP.
Introduction
Supracondylar humerus fractures (SCHF) are the most frequently seen elbow fractures in the pediatric age group (1). When the frequency of these injuries is taken into consideration, it can be seen to be important for orthopedic surgeons to understand the treatment principles for different types of SCHF (2).
One of the most commonly used classifications is by Gartland for the decision of treatment strategy. The major drawbacks against this classification are the insufficiency of assessing the fracture configuration and predicting clinical outcome (3,4). The Johns Hopkins (J-H) classification, introduced in 2007, defined four coronal patterns (typical fracture pattern [TFP], medial oblique pattern [MOP], lateral oblique pattern [LOP], and high fracture pattern [HFP]) and two sagittal patterns (low sagittal and high sagittal) (5). Bahk et al. stated that >10° coronal and >20° sagittal obliquity is correlated with a poor prognosis.
In SCHF surgery, surgeons aim for anatomical reduction and rigid fixation, but this is not always possible. It is relatively easy to measure coronal and sagittal alignment to test the acceptable values of the reduction. Assessing the rotation is more complex and can make on the lateral elbow X-ray. Fixation with rotational error is frequently encountered and remodeling is weak (6). There is no large study on assessing the amount of rotational incorrect fixation that will result in clinical problems. However, when unnoticed, malrotation of the distal fragment in the axial plane can lead to cubitus varus deformity (CVD) causing functional movement restriction, loss of strength, and posterolateral rotational instability (7–9).
Several authors have described various methods of determining rotation according to the fracture fragments; the most frequently used method to calculate rotation currently is the method defined by Gordon et al. (6,10–15). In the Gordon method, which aims to measure acceptable rotation, the Gordon lateral rotation percentage (GLRP) is calculated by dividing the absolute displacement of the proximal humerus metaphysis measured in the fracture region by the dimension of the distal humerus in the fracture region. The value obtained is multiplied by 100 to give the GLRP (11). A value <50% is defined as acceptable rotation (Gordon criteria). The GLRP is widely used as it is relatively quick, easy, and repeatable compared to other methods (6,16,17). However, the model formed by Gordon et al. only includes typical fractures (49–80% of all fractures) from the J-H fracture pattern evaluation (5,6). In addition, there is no study on whether rotation results in different values for internal and external rotation.
The aim of the present study was to investigate whether the Gordon criteria are useful for J-H subgroups of supracondylar fractures and whether the Gordon criteria are affected by internal and external rotation.
Material and Methods
The present study was approved by the Ethics Committee for Clinical Research at Marmara University Medical School. The patient and his family were informed that data from the research would be submitted for publication and gave their consent.
This study was designed using four pediatric left humerus bones obtained from the Sawbone© company. In each bone, an osteotomy was made to mimic each of the J-H coronal fracture patterns (TFP, MOP, LOP, HFP) (1) (Fig. 1).
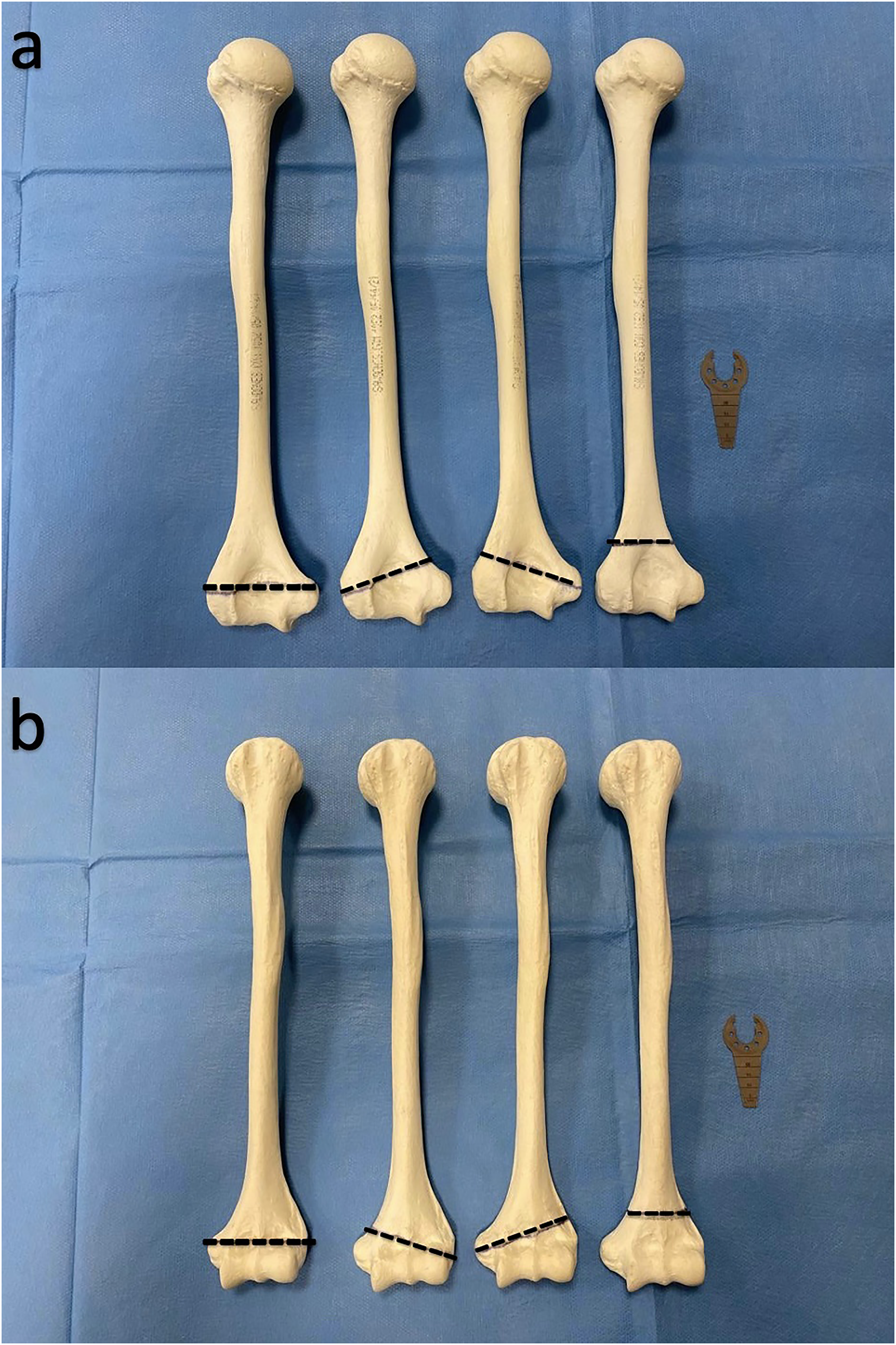
(a) Osteotomy line for the fracture patterns from posterior side. Typical fracture pattern, medial oblique fracture pattern (20° oblique), lateral oblique fracture pattern (20° oblique), and high fracture pattern from left to right, respectively. (b) Osteotomy line for the fracture patterns from anterior side. Typical fracture pattern, medial oblique fracture pattern (20° oblique), lateral oblique fracture pattern (20° oblique), and high fracture pattern from left to right, respectively.
Only one osteotomy was made on each bone (fine saw method). The bones were placed in a wooden rotation apparatus, as described in previous studies (10,17) (Fig. 2). Rotation was planned to be made from the center (pivot center) of the Sawbones©. For a clearer view in the wooden rotation apparatus, the proximal and distal fragments were fixed with rigid, radiolucent plastic rods and the rotation was performed with these rods. The position of the true lateral X-ray was determined as in the position where the teardrop shape was seen, as described by Grayson et al. (18). Only the distal fragment was positioned in a true lateral position and the proximal fragment was rotated in 5° increments from 90° internal rotation to 90° external rotation, and fluoroscopy images were obtained. As elbow radiographs are usually oriented according to the forearm, the internal or external rotation of the proximal part was simulated; therefore, the internal rotation of the distal fracture fragment was seen as an external rotation of the proximal fragment on the radiographs.

(a) Measurement of the Gordon lateral rotational percentage (GLRP). (X + Y)/Z multiplied by 100. X = anterior absolute amount of displacement of the proximal humeral metaphysis. Y = posterior absolute amount of displacement of the proximal humeral metaphysis. Z = the width of the distal humerus just distal to the fracture site. (b) INFINIX fluoroscopy device (Toshiba, Japan). (c) Wooden rotation apparatus.
The rotation model of this study was set up with rigid radiolucent plastic for fixation of the Sawbone© and a wooden rotation apparatus designed for radiological rotation measurement in SCHF. On the proximal side of the device, there is a goniometer fixed to the wooden rotation apparatus that allows the measurement of the actual degrees of rotation for radiological rotation measurement. With the adjustable angle measures on the proximal, the actual rotation was changed with 5° differences. This study is the measurement technique analysis of the rotation in the axial plane over the sagittal plane X-ray.
The images were obtained on a INFINIX fluoroscopy device (Toshiba, Japan) and evaluated on an Infinity radiology evaluation system. A consensus meeting regarding the Gordon technique of rotational measurement was held before the measurements were taken. The GLRP measurements were taken by five blinded observers (one pediatric orthopedic surgeon, one orthopedics and traumatology specialist, and three orthopedics and traumatology residents). The measurements were repeated after a six-month interval by all the observers. All four observers were blinded to the results of all their evaluations.
Previous studies have stated that 30° rotation of a Sawbone© is of no clinical importance, so 30° was taken as the threshold value for this study (14). The measurements were taken in the range of 30° internal rotation to 30° external rotation.
While the range of acceptable values stated by Gordon et al. for TFP, LOP, and MOP is 30° internal rotation to 30° external rotation, measurements were taken from 60° internal rotation to 60° external rotation for HFP as this exceeds these criteria.
Statistical analysis
Inter-observer agreement and intra-observer reliability of the repeated measurements were calculated using SPSS vn. 20.0 software (SPSS Inc., Chicago, IL, USA). While evaluating the study data, quantitative variables were reported as mean, standard deviation, median, minimum and maximum values, and qualitative variables were shown with descriptive statistical methods as frequency and percentage. The Shapiro–Wilk test and box-plot graphics were used to evaluate the conformity of the data to normal distribution. The Mann–Whitney U test was used in the comparisons of two groups of non-normally distributed variables. The results were evaluated at the 95% confidence interval (CI) and a significance level of P < 0.05.
Results
The inter- and intra-observer reliability of the measurements were >95%. The intraclass coefficient, Cronbach’s alpha, and P values of the inter- and intra-observer agreement are shown in Tables 1 and 2, respectively.
Inter-observer reliability.
CI, confidence interval; ICC, intraclass correlation coefficient.
Intra-observer reliability.
CI, confidence interval; ICC, intraclass correlation coefficient
In the repeated measurements for typical fracture pattern, if the GLRP is 20, it is consistent with 5° internal rotation and 15° external malrotation. If the GLRP is 50, it is consistent with 18° internal rotation and 18° external malrotation. These limits were found to be 20° for internal and external rotation for the typical fracture pattern (Fig. 3).

The second measurements of the observers for typical fracture pattern. Gordon lateral rotation percentage measurements. X axis, actual rotation amount; Y axis, Gordon lateral rotation percentage.
In the repeated measurements for MOP, if the GLRP is 20, it is consistent with 8° internal malrotation and 4° external malrotation. If the GLRP is 50, it is consistent with 22° internal malrotation and 16° external malrotation. In the repeated measurements for the LOP, if the GLRP is 20, it is consistent with 10° internal malrotation and 8° external malrotation. If the GLRP is 50, it is consistent with 20° internal malrotation and 20° external malrotation. In repeated measurements for medial and lateral oblique fracture patterns, observers similarly did not find 25° of external rotation and 30° of internal rotation to be within acceptable limits (Figs. 4 and 5).
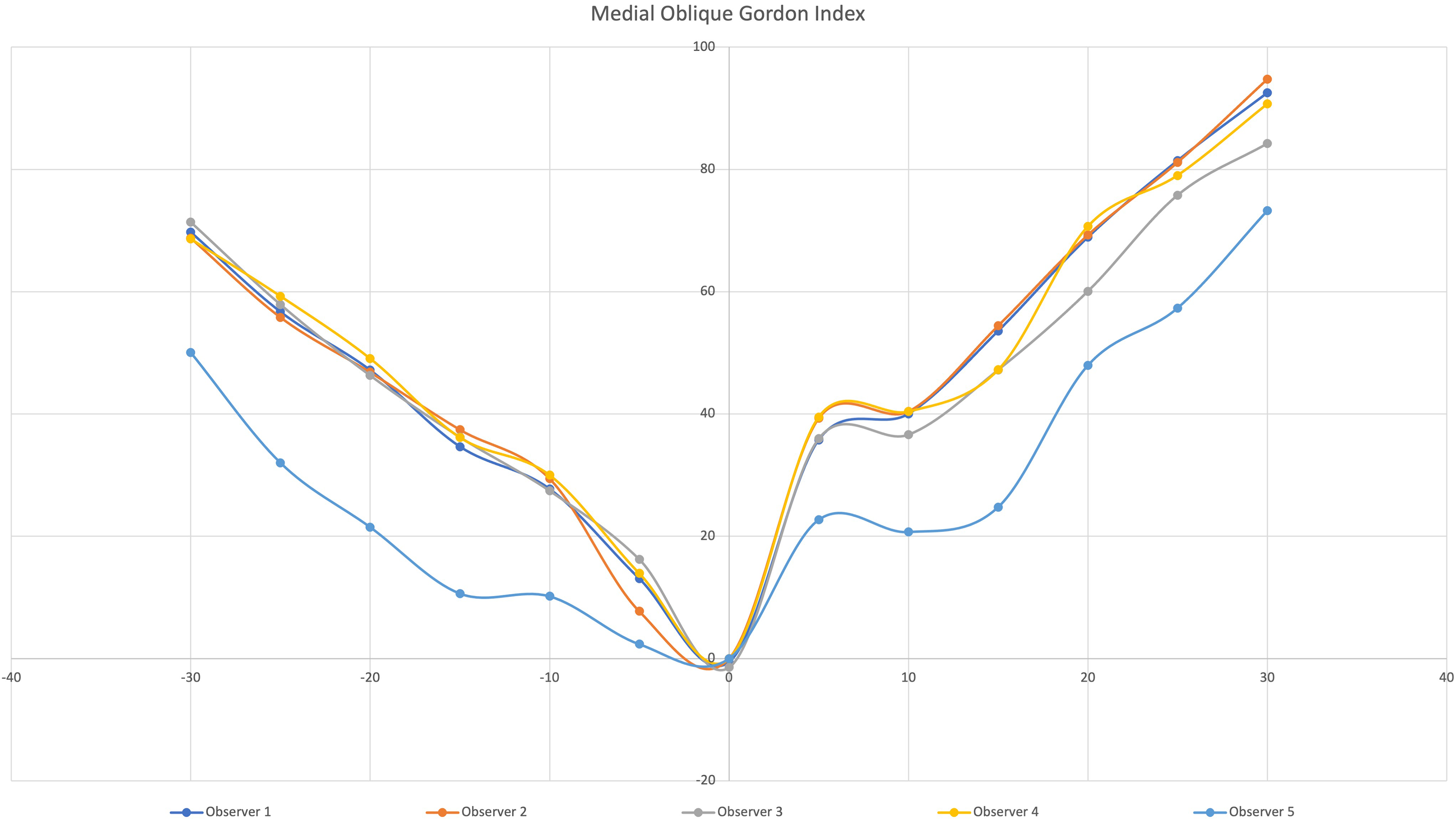
The second measurements of the observers for medial oblique fracture pattern. Gordon lateral rotation percentage measurements. X axis, actual rotation amount; Y axis, Gordon lateral rotation percentage.

The second measurements of the observers for lateral oblique fracture pattern. Gordon lateral rotation percentage measurements. X axis, actual rotation amount; Y axis, Gordon lateral rotation percentage.
In the repeated measurements for the HFP, if the GLRP is 20, it is consistent with 10° internal malrotation and 40° external malrotation. If the GLRP is 50, it is consistent with 25° internal malrotation and 50° external malrotation. According to Gordon's acceptable value of 50, all observers found 30° internal rotation and <60° external rotation to be within acceptable limits (Fig. 6).
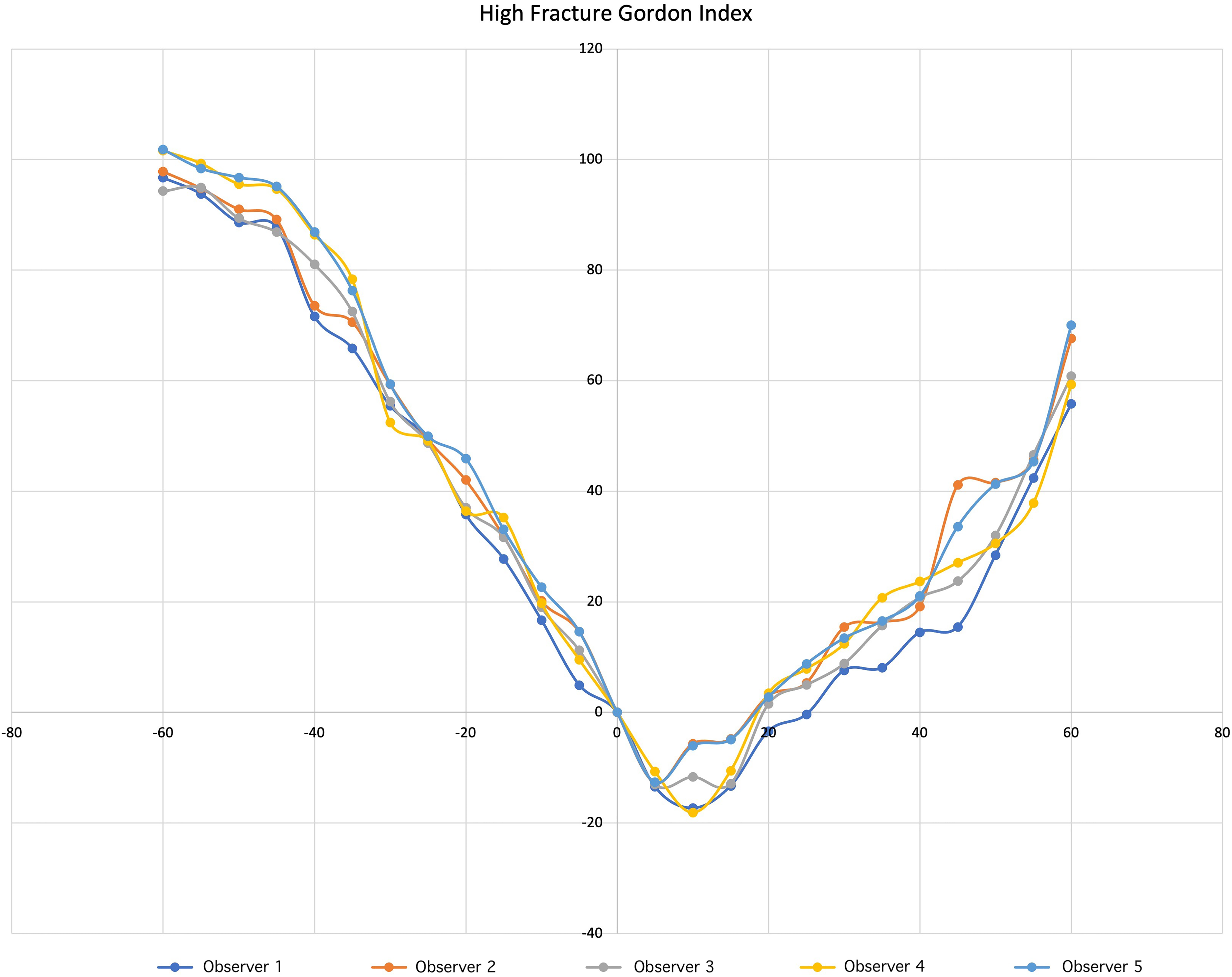
The second measurements of the observers for high fracture pattern. Gordon lateral rotation percentage measurements. X axis, actual rotation amount; Y axis, Gordon lateral rotation percentage.
The first 10° of external rotation measurement of all the observers fell to negative values for HFP.
Discussion
This study was designed to be of benefit in the intraoperative evaluation of rotational alignment. All fracture patterns have different characteristics. In the repeated measurements of the observers, ≤20° rotation for TFP and ≤30° rotation for LOP and MOP were measured as within the limits of an acceptable amount of rotation according to the Gordon criteria. However, for HFP, ≤30° internal rotation and ≤55° external rotation were determined to be within the acceptable rotation criteria according to the Gordon criteria. This is the first study to have presented the acceptable degrees of internal and external rotation of the Gordon criteria of all the J-H fracture patterns. The acceptable amounts of malrotation after closed reduction percutaneous pinning of different patterns of pediatric SCHF have not yet been defined.
In clinical practice, it is probably less important to be able to calculate the exact degree of malrotation than to notice malrotation at an unacceptably large amount. There is as yet no study in the literature that has been able to determine what degree of rotation is clinically acceptable or at how many degrees of malalignment clinical problems develop in pediatric SCHF of different patterns. However, the present study could be a guide for these kinds of studies in the future. To prevent elbow rotational malalignment, which is often seen in SCHF, intraoperative evaluation of malrotation is important. Fractures with inappropriate rotation are significantly associated with high complication rates, prolonged the need for physical therapy sessions and nerve damage (19). It should be considered a potential prognostic variable. Varus deformity may be seen in 93% of cases with internal malrotation (8). Surgeons aim for anatomical reduction, but this is not always possible. Takahara et al. stated that up to 30°–45° of malalignment in SCHF can be tolerated by the proximal humerus (20). Fixation with rotational error above these values can be a reason for cubitus varus deformity, rotation defect, and nerve damage. The different configuration of high fractures may lead the surgeon to malrotation.
In perioperative fixation during SCHF surgery, acceptable values can be determined with measurement of the Bauman angle in the coronal plane (21). For translation measurement in the sagittal plane, acceptable values are presented of the localization of the anterior humeral line (22). The situation is somewhat more complex for rotation measurement. In the studies by both Prabhakar et al. and Henderson et al., which aimed to measure rotation in SCHF, only typical fracture patterns were simulated with bone models (12,14). Henderson et al. used measurements on anteroposterior and lateral radiographs, and used the cosine equation aimed to measure actual rotation (12). Prabhakar et al. emphasized that the lateral image was sufficient (14). In the present study, the evaluations were made only on the lateral image. To the best of our knowledge, there is no other study in the literature that has given acceptable limits for different fracture patterns in both internal and external rotation.
At the end of the operation, the surgeon can calculate sagittal translation using the anterior humeral line, but there may be rotation in the bone without translation in the sagittal plane that can be overlooked. Therefore, for the measurements in the present study, the “pivot center” was taken as the center of rotation of the Sawbones©. In the model made by Prabhakar et al. using the lateral and medial centers of rotation, the anterior humeral line does not appear to cross the capitellum (14), whereas in the present study pivot center model, the anterior humeral line is seen to cross the capitellum (Fig. 7). Henderson et al. also used the pivot center. Prabhakar et al. evaluated four separate models for the medial, lateral, anterior, and posterior rotation centers, and the best measurement was obtained from the lateral pivot (intact lateral cortex). However, in clinical scenarios, the posterior cortex may be intact or there may be no intact cortex. The pivot center model was used in the present study because an image without translation could be obtained.
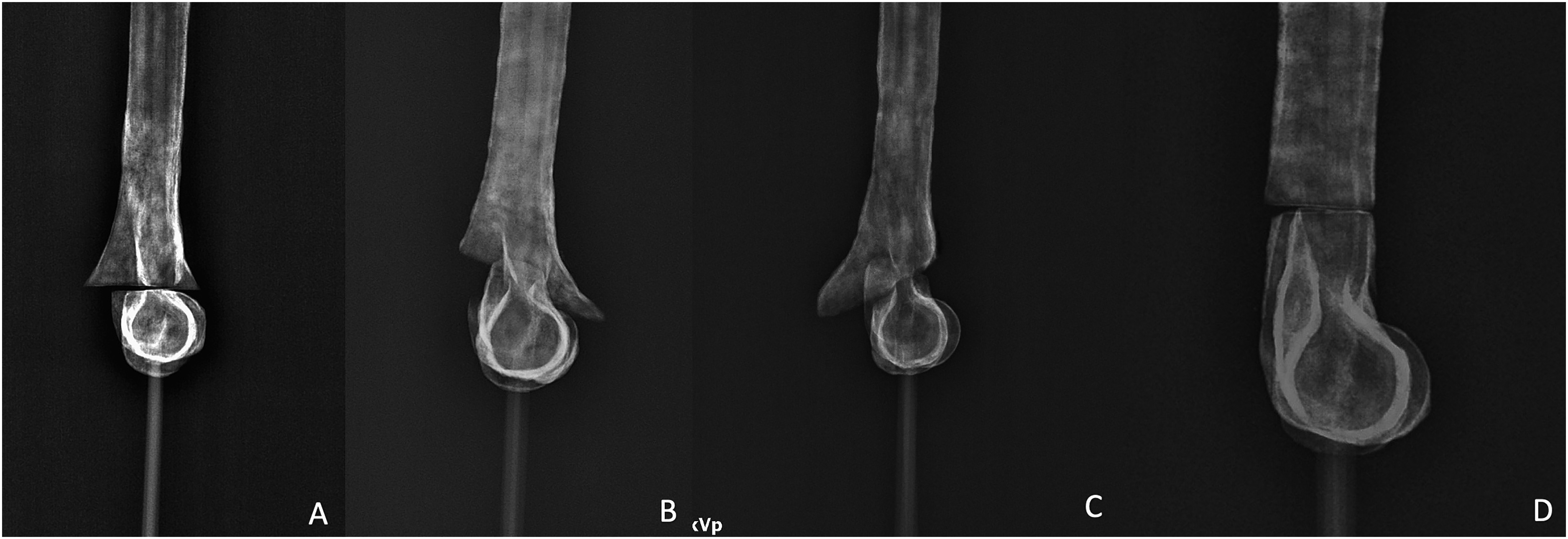
Sawbone© images in 25° external rotation. (a) Typical fracture pattern. (b) Medial oblique fracture pattern. (c) Lateral oblique fracture pattern. (d) High fracture pattern.
Prabhakar et al. used only TFP Sawbone© and reported that the radiological image of the Sawbone© would not be compatible with the clinical scenario for ≥30°; therefore, only measurements up to 30° were taken (14). In the present study, the measurements were taken at 5° intervals from 30° internal rotation to 30° external rotation, except for HFP, because it was found that higher rotation would not correlate clinically in TFP, MOP, and LOP. Thus, the measurements for HFP were evaluated at 60° internal and external rotation. This was thought to be due to the region where HFP is formed having a different distal humerus coronal-sagittal ratio from where the TFP is formed. The observers determined that the GLRP was <50°, including in 55° external rotation, for the Sawbone© simulating HFP. Rotational malalignment of 55° does not seem to have the potential for remodeling. It can be recommended that the GLRP for HFP is at lower values. The Sawbone© turned to 60° external rotation for HFP is shown in Fig. 8.

Radiological image of the Sawbone© with simulated high fracture pattern in 60° external rotation. The Gordon lateral rotation percentage values of the second measurements of the observers. Observer 1 = 54.8, Observer 2 = 57.2, Observer 3 = 58.8, Observer 4 = 61.5, Observer 5 = 57.7.
When planning the present study, it was planned to take both internal rotation and external rotation measurements as it was thought that the Gordon criteria could be different. Henderson et al., Prabhakar et al., and Berdis et al. examined rotation on only one side (10,12,14). In the present study, the position taken as the true lateral image (0° rotation) was that which clearly showed the teardrop shape. If the true lateral was determined according to the posterior cortex method defined by Skibo et al., this difference maybe would not have occurred (23). Because the posterior cortex rotates distal to the humerus, the actual lateral image of the anatomic region where HFP occurs may show overlapping of the posterior cortices. When Fig. 6 is examined, it can be seen that the lateral rotation index of the observers fell to negative values in external rotation. In other words, the observers measured more widely from the proximal of the cut, which could explain the negative values of the GLRP in the external rotation measurement in HFP. Moreover, this is valid for MOP and LOP because both images have spikes, but the measurements were different. However, this detail does not change an unacceptable malrotation in HFP. This indicates the need for clinical studies related to this subject.
Bahk et al. suggested that there could be several reasons that >10° obliquity (MOP, LOP) in the J-H fracture pattern is correlated with a poor outcome, including difficult reduction, difficult fixation, metaphyseal crush, and a non-ideal pin pattern (5). Although there was no significant difference between the observer measurements in the present study (P > 0.005), in clinical practice, rotation evaluation in oblique patterns can be made more difficult with metaphyseal crush, and this can increase the risk of fixation with rotational error. Despite no statistically significant difference, the inter- and intra-observer agreements were found to be lower for oblique fracture patterns than for TFP and HFP. This could be another reason for the relatively worse outcome of oblique fracture patterns in clinical practice.
Contrary to Berdis et al., we found that all fracture patterns have different characteristics. Berdis et al. claimed that TFP, LOP, and HFP were the three most common patterns and performed 0°–45° internal rotation measurements. As the measurements were taken of only internal rotation, different internal and external rotation values may have been overlooked (10). Berdis et al. did not state an acceptable degree of rotation and all J-H fracture patterns were not simulated. After the literature research for this study, in contrast to the measurements in the three most frequently seen patterns according to the order of frequency, medial oblique fracture has not been determined to be seen less than high fracture in any series (5,6). In the present study, the measurements were taken twice by the five observers at a six-month interval. No significant difference was determined between the measurements of the observers in this study (P < 0.005). The high intra-observer reliability demonstrates that the measurements in this study were reliable and repeatable.
The model used was similar to that designed by Özel et al. and used for the radiological measurement of rotation in femoral shaft fractures (24). Henderson et al. used a similar wooden rotation measurement apparatus as current study (12). Berdis et al., who aimed to measure rotation in SCHF, placed thick Schanz wires in the proximal and distal fragments and measured the rotation with a goniometer. However, it was mentioned as a limitation of the study that measurements taken using Schanz wires with a goniometer may provide an incorrect measurement (10). The most sensitive measurements on this topic were made by Prabhakar et al. using an electronic inclinometer (14). There are examples from previous authors of the rotation measurement of the model used in this study, and it was considered to provide an accurate measurement. In the studies by Berdis et al. and Henderson et al., a fine saw was used to osteotomize the bone, while Prabhakar et al. used bones with 3D printer osteotomy simulation obtained from the Sawbone© firm (10,12,14). In the present study, the fine saw method was used, as in the studies by Berdis et al. and Henderson et al. The method used by Prabhakar et al. (inclinometer) can be more sensitive. However, when the ratio of metaphyseal crumbling in the clinical scenario was considered, it was thought that this detail would not affect the measurements.
The present study has some limitations. As this study and those of other authors who have aimed to calculate other rotation values are not standardized, this subject of malreduction in SCHF may not be able to be examined in only one plane. Other malreduction planes (varus, valgus, flexion, or extension) are not included in the calculation in this modeling, but in clinical practice malreduction can occur in multiple planes. Rotational malalignment may not only cause a poor outcome in the long-term postoperatively but can also cause other malreduction problems. In this study, it was attempted to overcome this problem by using the pivot center. The distal third of the humerus has lower mineral density than other parts of the bone (25). Thus, there may be bone metaphyseal fragmentation and crush in SCHF, and this may be a reason for the clinical incompatibility of the current study model. No modeling has yet been developed in which metaphyseal crush is included in the calculation. Although pediatric humerus bones were used in the model, much younger patients may be seen in clinical practice. The interpretation of radiographs around this region may sometimes be difficult and unreliable because of the cartilage structure of the immature elbow. In addition, it may be possible to do the same work with 3D modeling in a way that eliminates the errors that may occur in the measurement and assembly over the software, and the radiological results of the malreduction that may occur in all three planes can be determined.
In conclusion, based on the data of this study, the Gordon criteria can be used safely for TFP, MOP, and LOP but it is necessary to lower the acceptable rate of 50% in the HFP. This value is above the limit of rotational malalignment of the distal humerus that can be tolerated by the proximal humerus, as reported by Takahara et al. (20). It can be recommended that separate evaluations are made according to fracture pattern when using the GLRP in clinical practice and in academic studies. As this has not been taken into consideration in previous studies, this information should be evaluated by readers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.