
Abstract
Background
Detecting occlusions of coronary artery bypass grafts using non-contrast computed tomography (CT) series is understudied and underestimated.
Purpose
To evaluate morphological findings for the diagnosis of chronic coronary artery bypass graft occlusion on non-contrast CT and investigate performance statistics for potential use cases.
Material and Methods
Seventy-three patients with coronary artery bypass grafts who had CT angiography of the chest (non-contrast and arterial phases) were retrospectively included. Two readers applied pre-set morphologic findings to assess the patency of a bypass graft on non-contrast series. These findings included vessel shape (linear-band like), collapsed lumen and surgical graft marker without a visible vessel. Performance was tested using the simultaneously acquired arterial phase series as the ground truth.
Results
The per-patient diagnostic accuracy for occlusion was 0.890 (95% confidence interval = 0.795–0.951). Venous grafts overall had an 88% accuracy. None of the left internal mammary artery to left anterior descending artery arterial graft occlusions were detected. The negative likelihood ratio for an occluded graft that is truly patent was 0.121, demonstrating a true post-test probability of 97% for identifying a patent graft as truly patent given a prevalence of 20% occlusion at a median 8.4 years post-surgery. Neither years post-surgery, nor number of vessels was associated with a significant decrease in reader accuracy.
Conclusion
Evaluation of coronary bypass grafts for chronic occlusion on non-contrast CT based off vessel morphology is feasible and accurate for venous grafts. Potential use cases include low-intermediate risk patients with chest pain or shortness of breath for whom non-contrast CT was ordered, or administration of iodine-based contrast is contraindicated.
Keywords
Introduction
A coronary artery bypass graft (CABG) is the gold standard treatment for severe multivessel coronary artery, left main coronary artery disease, coronary artery disease comorbid with diabetes or reduced left ventricular function (1,2). However, the principal long-term drawback is the occlusion of the anastomosed vessels. This remains a highly controversial topic in terms of graft selection and alternatives with minimally invasive coronary interventions (3). The vessel occlusion can be either acute or chronic, with the acute presentation often reminiscent of acute coronary syndrome due to acute thrombosis of the graft. Chronic occlusion remains a challenge, with long-term patencies ranging from 50% to 90% at 10 years, depending on the type of grafts used (4). Previous studies have shown increased morbidity and mortality in patients with chronic occlusion of grafts, including the need for further coronary interventions (5).
Given the potential for negative outcomes, accurate diagnoses of chronic occlusion are needed. The gold standard for diagnosis is diagnostic coronary angiography performed by an interventionalist. An absence of contrast filling in the coronary artery bypass graft is diagnostic for an occluded graft. Beginning in the early 2000s, multidetector computed tomography (CT) was used with great success for the diagnosis of occlusions using iodine-based contrast media. Reported sensitivities reached 95–100% and the use of CT angiography (CTA) became a non-invasive method of investigating the patency of coronary bypass grafts (6).
However, not all patients are eligible to undergo CTA for assessment of graft patency, nor are all patients with bypass vessels subjected to CTA as part of their chest pain evaluation. Some patients are simply evaluated with non-contrast imaging in the urgent-emergent setting, especially if their history of revascularization is not known or the pathology of their chest pain is not strongly suspected to be cardiac in etiology. These patients may be incidentally found to have prior CABG, but, currently, these patients are not evaluated for chronic occlusion on the non-contrast examination.
Alternatively, patients with underlying renal dysfunction, acute kidney injury or contrast allergy may initially get non-contrast chest CT. The current literature consensus is that the risk of contrast-induced nephropathy is low (estimated 3–6%) in patients with chronic kidney disease, but not zero (7–9). Current recommendations highlight high risk patients as those with a recent acute kidnery injury or an estimated glomerular filtration rate <30 mL/min/1.73 m2 (10). This finding is particularly important given the increased use of CTA for stable chest pain, as highlighted in the DISCHARGE study, which found similar accuracy for obstructive lesions for CTA compared to diagnostic coronary angiography, but with less complications (11). It is evident that the use of CTA will continue to grow in this area, but little has been done to alleviate the contrast question in this population at risk of kidney injury (up to 5.6%) (12).
The value of a non-contrast CT series for diagnosing chronic occlusion of coronary bypass grafts is understudied and often underestimated. Some notable pathological findings of occluded grafts include atherosclerotic luminal narrowing or collapse, intimal proliferation and fibrosis (13,14). Venous grafts are known to undergo arterialization and accelerated atherosclerosis due to a variety of factors, including differential oxidation and inherent wall structure (4,14,15). While a contrast filling defect may be the most well-known finding on CTA, other morphological characteristics of the grafts may be identifiable diagnostic even on non-enhanced CT series signs such as collapsed lumen, linear band like/calcified vessel, surgical marker without visible bypass graft.
We therefore hypothesize that some of these findings should have radiologic correlates. Patent grafts should have a circumferential lumen, and the flattening of the vessel to a linear or band-like shape with calcification may be a sign of chronic occlusion. Similarly, many surgeons add a metallic marker to the site of CABG grafts to localize bypass grafts for coronary angiographers. The absence of an easily visible vessel connected to the marker may also be a diagnostic sign of occlusion. These novel signs/findings may help reading physicians raise suspicion of bypass graft chronic occlusion on a non-contrast CT scan. The present study aimed to evaluate these signs on non-contrast CT to determine their utility and diagnostic accuracy.
Material and Methods
Ethics and privacy statement
The study protocol (Pro00116041) was approved by the local institutional review board as exempt to a full review, and the need for informed consent was waived. Patient-level data and images were collected and anonymized with removal of protected health information in accordance with the healthcare insurance portability and accountability act. A master copy of the data with patient identifiers was retained on an encrypted institutional network. Data undergoing analysis was sanitized and removed of identifiers. No data was shared with any third parties. Study data are not provided by default given inclusion of patient level data but are available from the corresponding author upon reasonable request.
Patient inclusion
Seventy-three patients who underwent non-electrocardiogram gated CTA of the chest were retrospectively identified from 2017 to 2022 and ultimately included in the study. Inclusion criteria consisted of history of CABG and simultaneous acquisition of non-contrast series prior to acquisition of the contrast angiography series as part of the protocol at our institute. Imaging exclusion criteria consisted of severe artifact (including motion or metallic artifact etc.) that rendered poor diagnostic quality. Clinical exclusion criteria included a lack of sufficient demographic and surgical history or documentation to preclude reasonable sensitivity analysis. Eighty-eight patients were found to fit the criteria. Thirteen patients were found to erroneously have a history of CABG with no bypass vessels identified on imaging. Two patients were excluded from the per-graft qualitative assessment because of inability to determine ground truth for at least one vessel due to artifact. In total, 73 patients were included in the study.
Imaging review
Two separate readers, each fellowship trained attending cardiothoracic radiologists, independently and blindly assessed each non-contrast and arterial phase series. Each reader quantified the number of grafts visualized, their respective anastomotic locations, and whether the graft was grossly patent or occluded. No alternative specification was made for grafts suspected of partial occlusions. Both readers only had access to the study at hand (as defined by unique accession number) and were not permitted to review patient history. Neither reader discussed cases with the other. Ground truth was defined by the patency of grafts as evaluated by one reader on the arterial phase series.
Diagnostic methodology
Grafts were suspected as being chronically occluded on non-contrast series if any of the following criteria were met:
The graft exhibited a “linear” or band-like morphology The graft lumen appeared collapsed There was a bypass graft marker without clear evidence of a vessel at the position.
Statistical methods and data collection
A pre-test power calculation was performed for the inter-rater reliability statistics. At least 59 patients are required to assess for a hypothesized kappa value of 0.8 ± 0.2 given a standard α of 0.05 and a conservative estimate of graft occlusion prevalence at 10%. Standard demographic data were collected including age, sex, race and body mass index (BMI). The number of CABG vessels, proportion of patients across anastomotic locations, and duration since CABG procedure were collected. Categorical data was assessed using counts and percentages while continuous data was assessed using medians and interquartile ranges. Dates of CABG procedures ranged from 1989 to 2022. Counts and frequencies of patent and occluded vessels were tabulated in confusion matrices and stratified by graft type. Accuracy statistics were calculated on a per-patient and per-graft basis using the Clopper–Pearson method for confidence intervals. Likelihood ratios were calculated using the contingency tables and sensitivity analysis was performed for both number of vessels and duration of graft placement. Inter-rater reliability was calculated using unweighted Cohen's kappa (CK). The statistics were computed based on the scores provided by reader 1 because there was near perfect agreement between the readers. All statistical analysis was performed in R, version 4.1.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
In total, 73 patients were included in the full analysis. The median ± SD age of each patient was 66.5 ± 16.5 years. The study cohort was 85.1% male and 14.9% female. Some 89.2% of patients self-identified as White or Caucasian, and 10.8% identified as Black or African American. The median ± SD BMI of patients was 30.1 ± 5.2 kg/m2. The mean ± SD number of CABG vessels grafted was 3 ± 1. Some 94.5% of patients had a left internal mammary artery to left anterior descending artery (LIMA-LAD) anastomosis, 61.6% had a saphenous vein graft to the obtuse marginal branch (SVG-OM) and 42.4% had a saphenous vein graft to the right coronary artery (SVG-RCA). The median implanted duration of CABG vessels assessed was 101 months (8.4 years) (Table 1).
Demographics and clinical summary of patients included in this study.
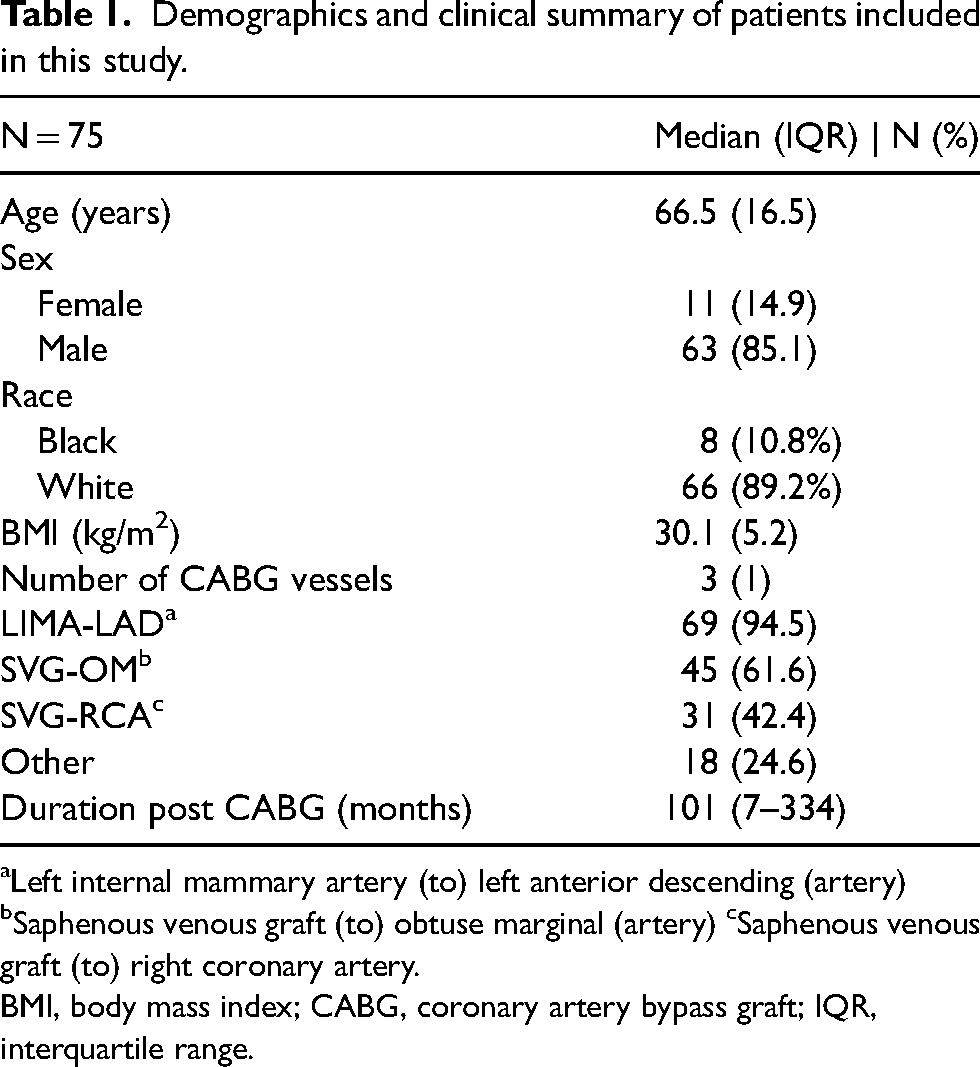
Left internal mammary artery (to) left anterior descending (artery) bSaphenous venous graft (to) obtuse marginal (artery) cSaphenous venous graft (to) right coronary artery.
BMI, body mass index; CABG, coronary artery bypass graft; IQR, interquartile range.
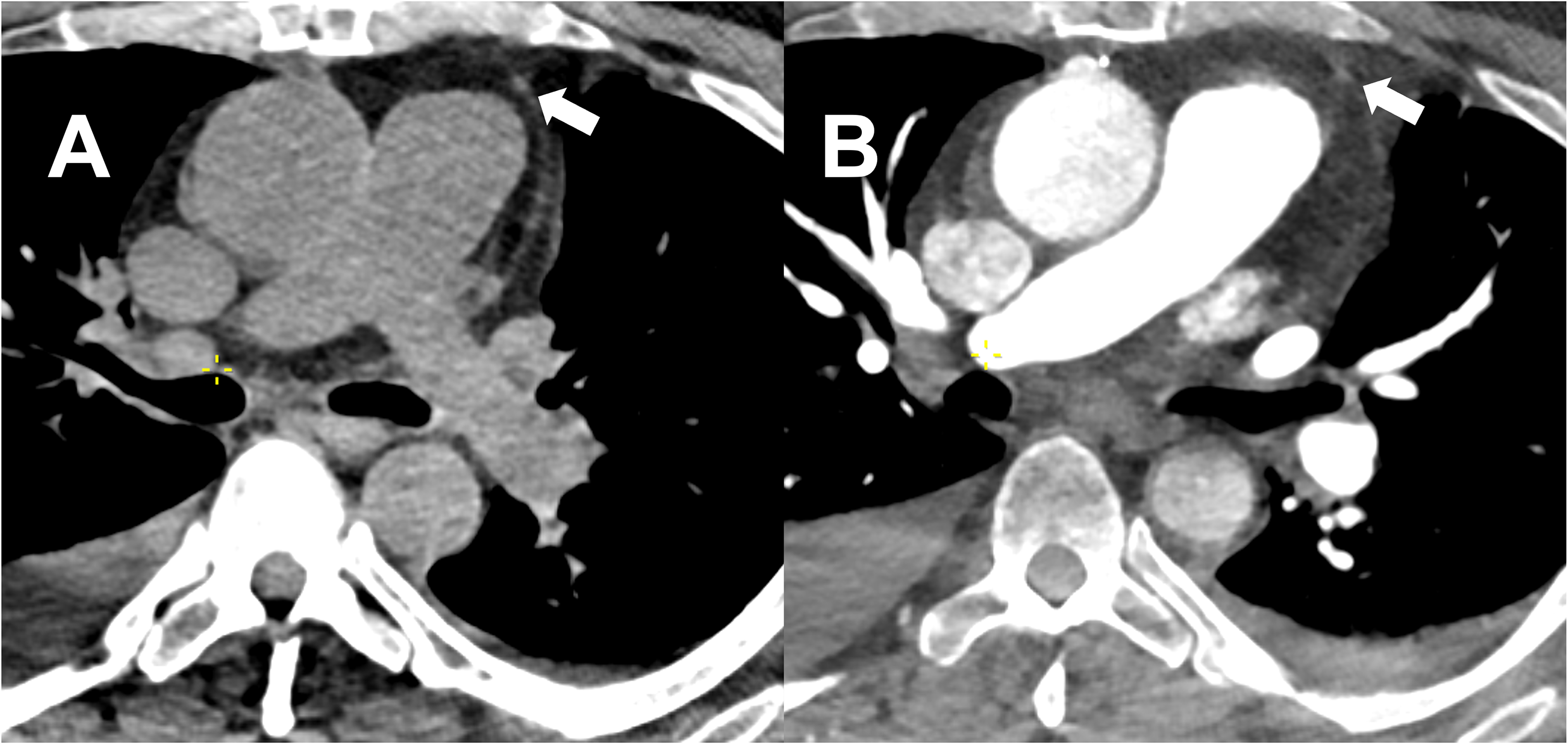
On a per-patient basis, 8/73 patients were incorrectly identified as having a patent versus occluded graft. Figs. 1 and 2 demonstrate transverse and multiplanar reconstruction (MPR) images of occluded and patent grafts, respectively. Out of the total 69 LIMA-LAD grafts, 66 grafts were accurately identified as patent. Only three LIMA-LADs were occluded in this dataset, and unfortunately none of them were identified as such on non-contrast CT scan (Fig.3). Out of the total 45 SVG-OM grafts, 36 grafts were correctly identified. Out of the total 31 SVG-RCA grafts, all of them were correctly identified (Fig. 4). The per-patient accuracy was determined to be 89.0% (95% confidence interval [CI] = 0.795–0.951). SVG-RCA grafts had a 100% (95% CI = 0.888–1.0) accuracy, followed by LIMA-LADs at 95.7% (95% CI = 0.780–0.991) and finally SVG-OM at 80% (95% CI = 0.654–0.904). All other grafts had an accuracy of 98.2% (95% CI = 0.904–1.0). Two-reader CK for inter-rater agreement demonstrated a per-patient agreement of 0.832 (95% CI = 0.692–0.972). Individual agreement was best for SVG-RCA grafts (CK = 1, perfect agreement) and worst for other grafts (CK = 0.634, 95% CI = 0−1.0). Notably, Cohen's Kappa was unable to be calculated for LIMA-LAD due to lack of occlusions called by the readers (Table 2).

Demonstration of occluded graft. (a, c) Transverse and multiplanar reconstruction (MPR) images, demonstration of occluded saphenous vein graft to the obtuse marginal branch graft (solid arrow) which has a linear band-like morphology with a collapsed lumen with surgical marker (open arrow) in place on the non-contrast phase as seen at the level of the left pulmonary artery. (b, d) Transverse and MPR images, arterial phase series of the same patient shows a lack of contrast material within the lumen confirming the diagnosis of chronic occlusion of the graft.

Demonstration of patent graft. (a, c) Transverse and multiplanar reconstruction (MPR) images, demonstration of patent saphenous vein graft to the obtuse marginal branch (SVG-OM) graft seen anterior to the main pulmonary artery at the level of the pulmonary artery bifurcation. (b, d) Transverse and MPR images, arterial phase demonstrates contrast within the lumen indicating a patent SVG-OM graft at this level.
Demonstration of occluded left internal mammary artery to left anterior descending artery (LIMA-LAD) graft. (a) Transverse non-contrast image of occluded LIMA-LAD (solid arrow) graft anterior to the main pulmonary artery. It was thought to be patent due to its small caliper and round shape (b) Transverse arterial phase image show lack of intraluminal contrast, consistent with occlusion.
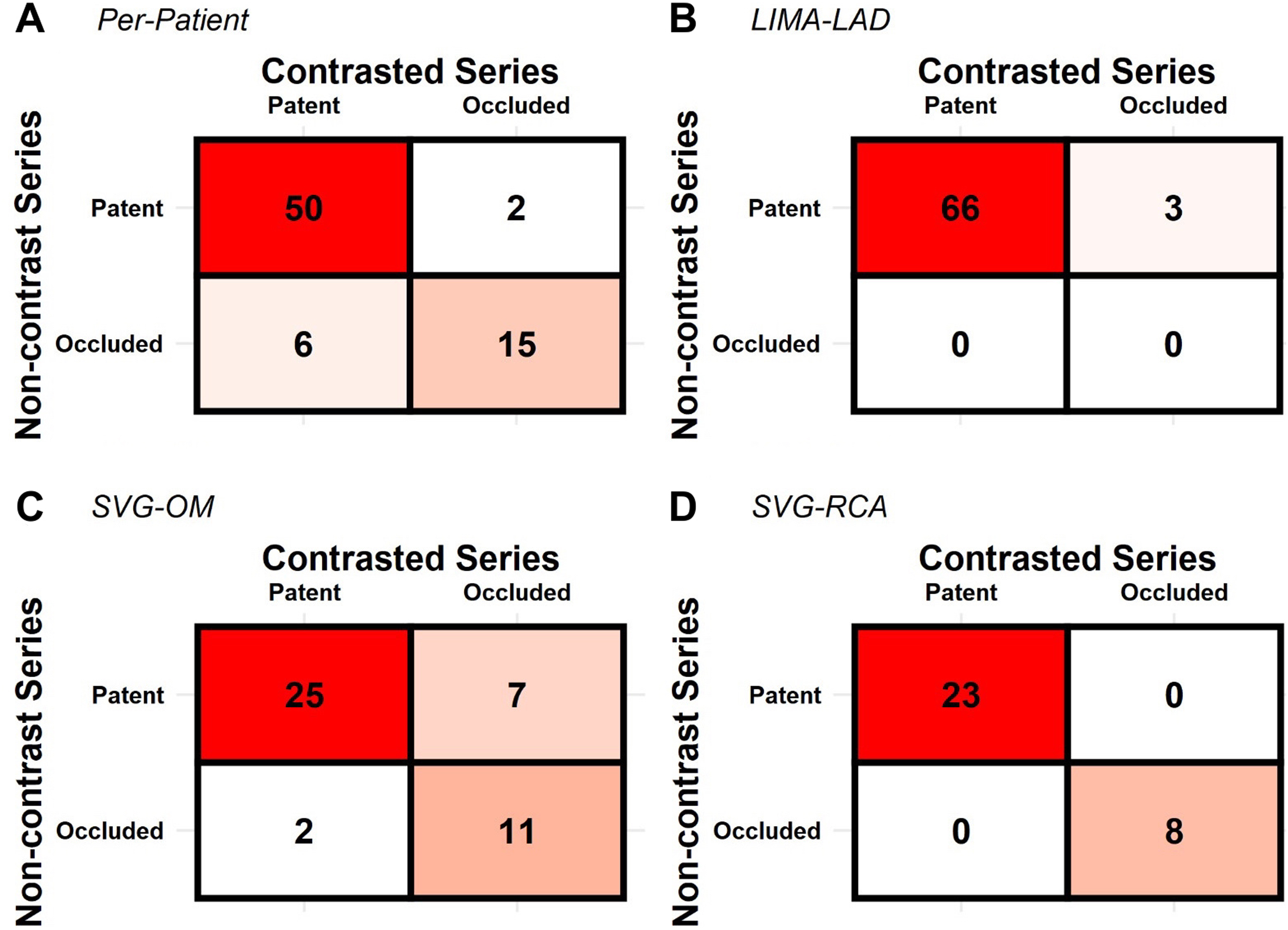
Qualitative performance of non-contrast series for identifying chronic bypass graft occlusion. (a) Two patients (2/73) were falsely diagnosed as having patent vasculature when at least one vessel was chronically occluded. (b) Almost all left internal mammary artery to left anterior descending artery (LIMA-LAD) vessels were correctly identified as patent (66/69). None of three occluded LIMA-LAD vessels was correctly identified . (c) Overall accuracy for saphenous vein graft to the obtuse marginal branch (SVG-OM) grafts was 36/45 (75%). (d) saphenous vein graft to the right coronary artery (SVG-RCA) graft patency was identified correctly 100% of the time.
Accuracy statistics by patient and vessel type for graft patency.

*Unable to calculate kappa for LIMA-LAD grafts due to lack of observed occlusion (0/3 by both readers).
CI, confidence interval; LIMA-LAD, left internal mammary artery to left anterior descending artery; NPV, negative predictive value; PPV, positive predictive value; SVG-OM, saphenous vein graft to the obtuse marginal branch; SVG-RCA, saphenous vein graft to the right coronary artery.
The prevalence of venous graft occlusions was estimated to be between 20% and 30% at 8.4 years depending on the type of graft. Using 20% as a conservative estimate, the positive post-test probability of a patent graft was 65%. The negative post-test probability for an occluded graft was 97%. Vessel accuracy did not vary with years post-CABG procedure (Fig. 5). Regarding accuracy per number of grafted vessels, the number of vessels accurately predicted was consistent amongst patients with 1–4 vessel CABG. Accuracies for these patients ranged from 85.7% to 97.4%. There was insufficient data to calculate accuracies for patients with ≥5 vessel CABG (Fig. 6).
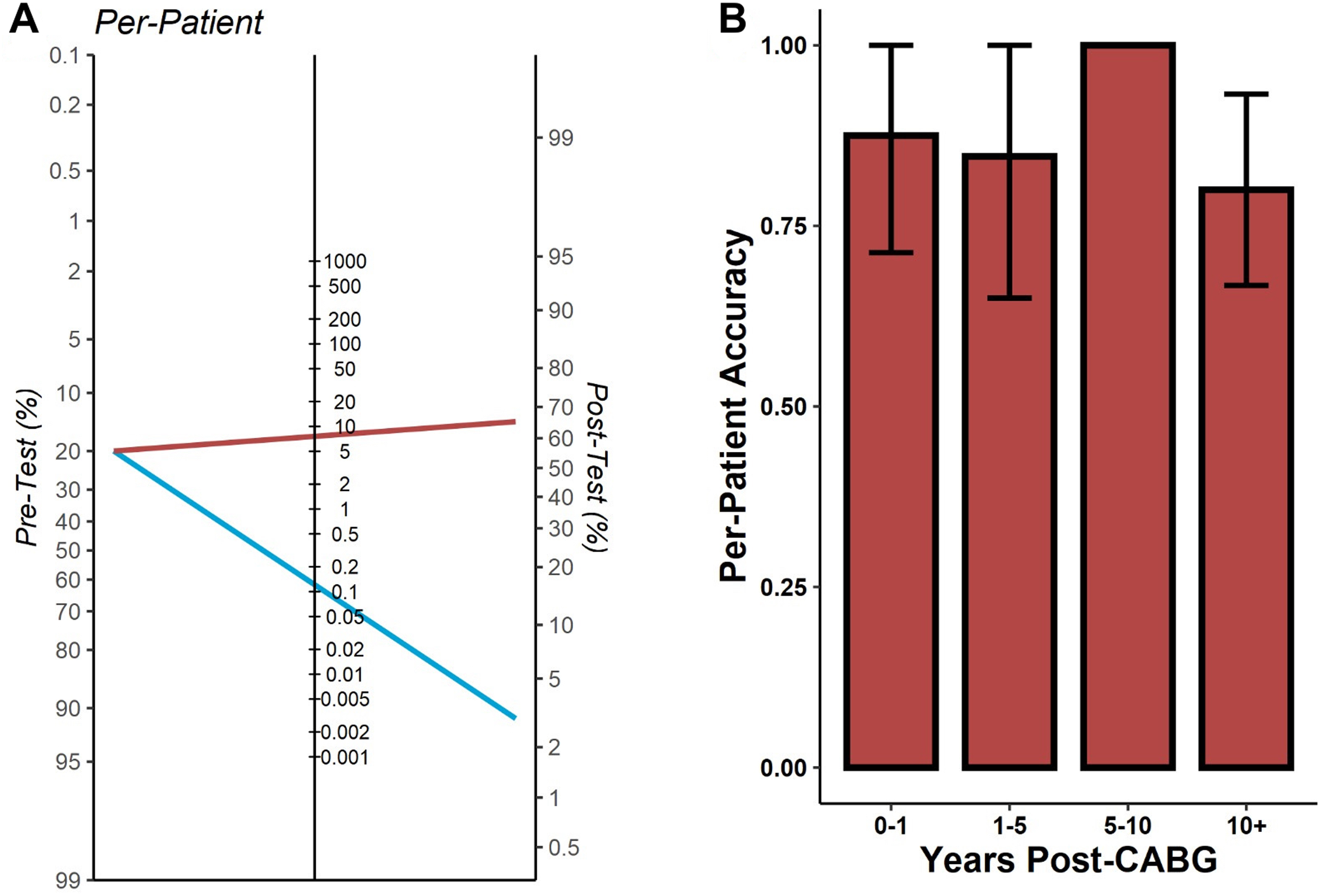
(a) Posterior probability nomogram for venous grafts occlusion on a per-patient basis. The post-test probability of correctly identifying a patent graft is 97%; inversely the post-test probability of misdiagnosing a patent graft as occluded is 3%. The post-test probability of correctly identifying an occluded graft is approximately 65%. (b) Accuracy by years’ post-coronary artery bypass graft (CABG). There is no measurable difference in per-patient accuracy by years-post graft, suggesting that diagnostic performance is not affected by length-time bias of graft occlusion occurrence.

Accuracy by number of bypass vessels. (a) Demonstration of vessels identified as patent determined by non-contrast computed tomography (CT) compared to CT angiography by number of bypass vessels. (b) Accuracy values and other diagnostic statistics demonstrating that utility of non-contrast computed tomography for diagnosis of graft occlusion is largely independent of number of vessels measured.
Discussion
The use of graft morphological characteristics to diagnose chronic venous vessel occlusion was successful and consistent across several different measurements. Per patient accuracy approached 90%, and most inaccuracies were found in patients with >4 grafts. Diagnosis of saphenous vein graft occlusion was particularly robust with perfect discrimination of SVG-RCA occlusions. The use of a nomogram with a conservative occlusion rate of 20% at 8.4 years suggests that there is a high positive predictive value for identifying patent grafts. There remains a false positive rate of 35% when identifying a graft as occluded. Sensitivity analysis demonstrated that there was no difference in accuracy as a function of years post-CABG, suggesting that these morphology assessments are largely free of any time-related bias.
The use of non-contrast CT to assess graft patency exceeded expectations for venous grafts. Overall accuracy for venous grafts was 88%, which is just below the 90–100% reported for contrast CT (6). Overall SVG patency in the present study was between 75% and 70% depending on the target vessel, in line with literature estimates for 8-year grafts (5,16,17). The same mechanisms that cause more rapid graft failure in SVGs may also contribute to their diagnostic performance; SVGs lack an internal elastic lamina which is thought to accelerate atherosclerosis and intimal remodeling (18). The same lack of elastic lamina and subsequent remodelling can be evident in distortion of normal graft architecture and forms the hypothetical basis of “flat” or linear vessels on CT, which represent chronic occlusion. Another possible explanation is the extensively studied arterialization phenomenon due to the high hydrostatic pressures that are subjected to the SVG as it branches off the aorta (15,19). The high hydrostatic pressures should lead to a round, symmetrical lumen in a patent graft, a deviation from which may be detected on non-contrast CT. The same principles can be applied to the examination of CABG markers; if an associated vein is less visible or flat at the location of the large artery anastomosis, the graft may be considered occluded. Applying the criteria for arterial grafts posed a challenge due to their smaller caliber. Moreover, arterial grafts retain their round shape on axial images, even in cases of occlusion. However, it is fortunate that arterial grafts exhibit long-term patency, 10-year patency of 90%.
The use of non-contrast CT to evaluate coronary arteries is not a new concept. The non-contrast series of coronary CT angiography has been used for calcium scoring, where it has gained the most attention, as well as for a wide range of congenital abnormalities (20,21,22). The novelty of the present study is the unexpectedly high accuracy rate for venous grafts. Ultimately, the low negative likelihood ratio for an occluded graft may have the most clinical utility. The post-test probability of having an occlusion when the read is patent is 3%, which is sufficient to rule out an occlusion in the absence of convincing clinical suspicion. This finding alone has the potential to reduce the amount of unnecessary invasive procedures and may be a reasonable tool in the emergency department for a patient with a low-intermediate pre-test probability of a CABG occlusion. Likewise, the positive likelihood ratio is sufficiently high to be suspicious of graft occlusion, but, with a post-test probability for occlusion of only 65%, these findings likely need to be confirmed with either contrast administration or invasive testing depending on the clinical situation. Regardless, the present study suggests that non-enhanced chest CT scans ordered for various reasons, including chest pain, may be helpful for the assessment of bypass graft chronic occlusion. Given the comorbidity of acute kidney injury and chronic kidney disease with multivessel coronary artery disease, there are clearly patients who could benefit from a test that is able to rule out of venous CABG chronic occlusions without the use of contrast.
The limitations of the present study stem from the low number of patients recruited with same day non-contrast and contrast CT series. It is currently not always standard to perform a non-contrast scan in advance. The present study also only employs two readers with subspecialty experience in cardiac imaging and may not apply directly to the generalist radiologist. Further studies should include a variety of readers with more patients with specific emphasis on per-graft analysis. Regarding graft numbers, there were few arterial occlusions in the LIMA-LAD category, the only arterial graft with sufficient occurrences for analysis. While LIMA-LAD grafts are renowned for their patency, 3/69 at 8 years is only an occlusion rate of 4.3%. This is a sufficiently low number for sparse-cell bias to be in effect. Notably, all three LIMA-LAD occlusions were missed by the readers but, given the small sample of occluded grafts, more study is needed in this area.
In conclusion, the present study quantified the novel feasibility of using non-contrast CT of the chest for diagnosis of chronic CABG occlusion, especially in venous graft. Specifically, the negative likelihood ratio favors the use of these criteria for ruling out chronic occlusion. The study suggests that non-contrast chest CT scans ordered for various reasons, including chest pain, might be helpful for the assessment of bypass graft chronic occlusion. There are also potential use cases, most likely in low-intermediate probability patients with concomitant renal disease, for whom administration of contrast is a roughly balanced risk–benefit discussion. The present study is principally limited by the small sample size of studies with concurrent non-contrast and contrast series, and the low rate of occlusions in the arterial cohort. Further studies are needed to validate these findings across a wide variety of patients and reader experiences.
Footnotes
Author contributions
Ismail M. Kabakus, Dhiraj Baruah, Jeremy R. Burt and Uwe Joseph Schoepf were responsible for study conception and design. Carter D. Smith and Elizabeth Van Swol were responsible for data collection. Jordan H. Chamberlin, Ismail M. Kabakus and Zain Gowani were responsible for writing the paper and analysis and interpretation of the results. Jordan H. Chamberlin, Carter Smith, Mina Gad Elsayed, Shahin C. Owji, Dhruw Maisuria and Brandon Friedman were responsible for draft manuscript preparation. All authors reviewed the results and approved the final version of the manuscript submitted for publication.
Data transparency
The authors report that they have full control of all primary data and will agree to allow the Acta Radiologica Journal to review the data if requested.
Ethics approval
The study protocol (Pro00116041) was found to be in accordance with ethical standards for studies involving human participants described by the local institutional review board. In addition, the local institutional review board determined that this study was exempt to a full review, and due to the retrospective nature of the data collection, the need for informed consent was waived.
Declaration of conflicting interests
The authors would like to declare the following financial interests/personal relationships which may be considered as potential competing interests: Uwe Joseph Schoepf and Jeremy R. Burt report a relationship with Siemens Healthineers that includes funding grants and non-financial support. Uwe Joseph Schoepf and Ismail M. Kabakus report a relationship with Elucid Bioimaging that includes consulting or advisory. Uwe Joseph Schoepf reports a relationship with Bayer that includes consulting or advisory. Uwe Joseph Schoepf reports a relationship with Bracco that includes consulting or advisory. Uwe Joseph Schoepf reports a relationship with Guerbet that includes consulting or advisory. Uwe Joseph Schoepf reports a relationship with HeartFlow Inc that includes consulting or advisory. Jeremy R. Burt reports a relationship with YellowDot Innovations that includes equity or stocks. The remaining authors have no competing interests to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.