
Abstract
Background
Endovascular thrombectomy (EVT) is performed for acute ischemic stroke (AIS) caused by large vessel occlusion; therefore, preoperative visualization of the occluded invisible vessel course reduces complications and ensures success. Three-dimensional (3D) proton density-weighted (PDW) vessel wall imaging (VWI) using variable refocusing flip angle pulse-turbo spin-echo sequences (VRFA-TSE) with 3.0-T magnetic resonance imaging (MRI) can provide this information.
Purpose
To assess the effectiveness of 3D PDW-VWI using 1.5-T MRI without VRFA function.
Material and Methods
Five consecutive patients with AIS caused by large vessel occlusion underwent EVT in our institute. VWI with 1.5-T MRI using 3D PDW-fast spin echo (FSE) technique was added to conventional brain imaging.
Results
PDW-FSE was successfully performed in all cases. 3D PDW-FSE was useful to visualize both the anterior and posterior circulations by clearly revealing invisible vessels but could not demonstrate the length and size of the clot in all five cases.
Conclusion
3D PDW-FSE with 1.5-T MRI without VRFA could clearly depict the course of the invisible occluded artery and might support favorable outcomes after EVT in patients with AIS.
Keywords
Introduction
Endovascular thrombectomy (EVT) using a clot retrieval device is a safe and highly effective treatment for acute ischemic stroke (AIS) in patients with large vessel occlusions (1). Recanalization using a stent retriever requires advance of a micro guidewire and a micro catheter across the clot. This procedure must be done blindly and consequently carries various hemorrhagic complications due to vascular dissection, perforation, or unidentified aneurysms (2,3). Therefore, obtaining rapid and reliable information about the invisible vessel course, including the clot before EVT, is useful to reduce the intraprocedural complications and increase the success rate of procedure.
Currently, the effectiveness of three-dimensional (3D) proton density-weighted (PDW) sequences with high-resolution vessel wall imaging (VWI) using variable refocusing flip angle pulse and turbo spin-echo sequences (VRFA-TSE) with 3.0-T magnetic resonance imaging (MRI) has been demonstrated for the visualization of the occluded invisible lesion before EVT in patients with AIS (4). The superiority of 3.0-T MRI to 1.5-T MRI for brain imaging has been established, but 1.5-T MRI, which does not have the function of VRFA, is still commonly used. Furthermore, 1.5-T MRI is safer than 3.0-T MRI for patients who have implants or other devices, and emergent patients whose information is not available on arrival at the hospital.
The aim of the present study was to evaluate the effectiveness of PDW-fast spin echo (FSE) for depicting the cerebral vessels, including occluded lesions, in patients with AIS using 1.5-T MRI without VRFA.
Material and Methods
Five consecutive patients with AIS caused by large vessel occlusion underwent EVT after MRI in our institute. MRI was performed using a 1.5-T unit (ECHELON Vega; FUJIFILM, Tokyo, Japan) in the order of diffusion-weighted imaging, cerebral time-of-flight MR angiography (TOF MRA), PDW-FSE, fluid-attenuated inversion recovery imaging, T2 star imaging, and cervical TOF MRA.
The imaging parameters of PDW-FSE were as follows: sequence = 3D FSE; slice plane = sagittal; TR/TE = 1000/30 ms; flip angle = 90°; field of view = 256 × 256 mm; matrix size = 256 × 256 mm; voxel size (acquired) = 1.0 × 1.0 × 1.1 mm; TSE factor = 32; RAPID factor = 4.0; number of signals averaged = 1; driven equilibrium pulse = on; and scan time = 6 min 17 s. Standard coronal reformation (slice thickness/interval = 1 mm/1 mm; number of slices = 80) of this acquisition was directly performed at the MRI console for multiplanar reconstruction. The PDW-FSE data were transferred to image creation software (Ziostation2; Ziosoft, Inc., Tokyo, Japan) and combined with cerebral TOF MRA for 3D reconstruction. The total time for MRI and time from data transfer to 3D reconstruction were measured, and the thrombolysis in cerebral infarction (TICI) grade was assessed in all cases.
To evaluate the accuracy of 3D PDW-FSE, the vascular course involving the M1 to M3 segments of the middle cerebral artery (MCA) in cases of anterior circulatory obstruction, and the P1 to P3 segments of the posterior cerebral artery (PCA) in the case of posterior circulatory obstruction was compared with that on angiography after treatment. All images were anonymized, and the image quality was retrospectively evaluated as excellent, good, or poor by two neuroendovascular treatment specialists. Excellent image quality clearly showed the occluded vessel from the occluded segment to the next segment. Good image quality showed only the occluded segment. Poor image quality did not show the occluded segment.
The study protocol was approved by the ethics review board of our hospital (Ethical examination/approval no. 01; approved on 6 January 2023).
Results
The lesions causing acute thromboembolic occlusion were located in the M1 segment of the MCA in two patients, the M2 distal in two patients, and the P1 segment of the PCA in one patient. 3D PDW-FSE without VRFA was successfully performed in all cases. 3D PDW-FSE without VRFA was useful to visualize both the anterior and posterior circulations (Figs. 1–3). The vessel courses demonstrated by 3D PDW-FSE without VRFA before treatment were compared with digital subtraction angiography after recanalization in all cases by evaluators 1 and 2. The assessments by the two evaluators were consistent in all five patients in Table 1. Both evaluators regarded the accuracy of 3D PDW-FSE without VRFA as “excellent” in the two patients with M1 occlusions and the patient with P1 occlusion, whereas the accuracy of 3D PDW-FSE without VRFA was “good” in the two patients with M2 occlusions. The vascular courses from the M1 to M2 and from the P1 to P2 were visualized with 3D PDW-FSE without VRFA. Successful recanalization of TICI 2b–3 was achieved in all cases (TICI 2b in one case, TICI 2c in two cases, and TICI 3 in two cases). PDW-FSE without VRFA could not demonstrate the length and size of the clot in all cases. The total MRI scan time was 19 min 15 s. The average time from data transfer of PDW-VWI without VRFA to 3D reconstruction was 8 min 24 s.

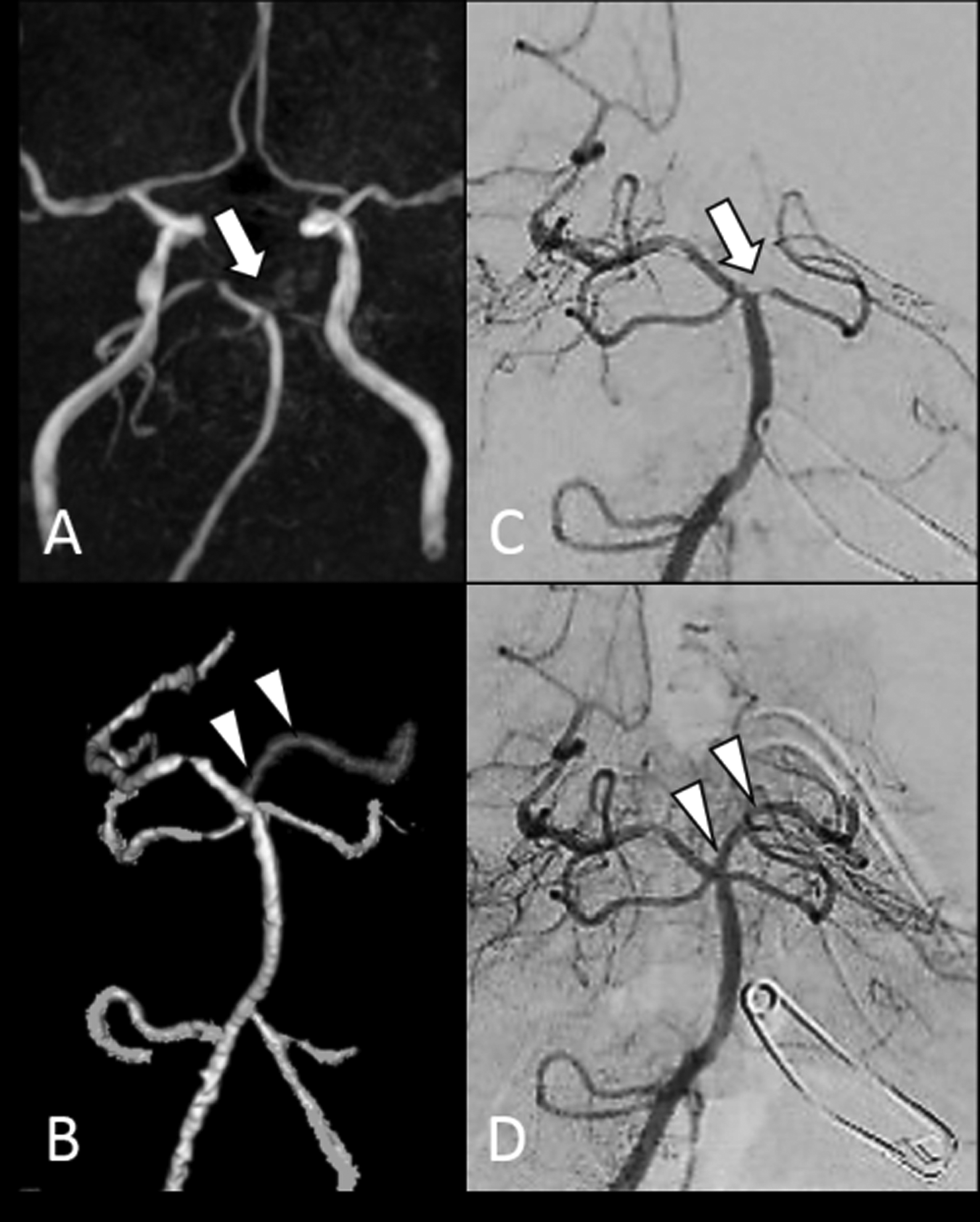
Case 1, an 82-year-old man with sudden onset of consciousness disturbance and right hemiparesis. (a) Time-of-flight MR angiogram showing left MCA occlusion. (b) 3D proton density-weighted MRI with fast spin echo showing the occluded MCA from the proximal to the distal area. (c, d) Left internal carotid angiograms before and after thrombectomy. Arrowheads indicate the cerebral vessels and arrows indicate the clot. MCA, middle cerebral artery; MRI, magnetic resonance imaging.
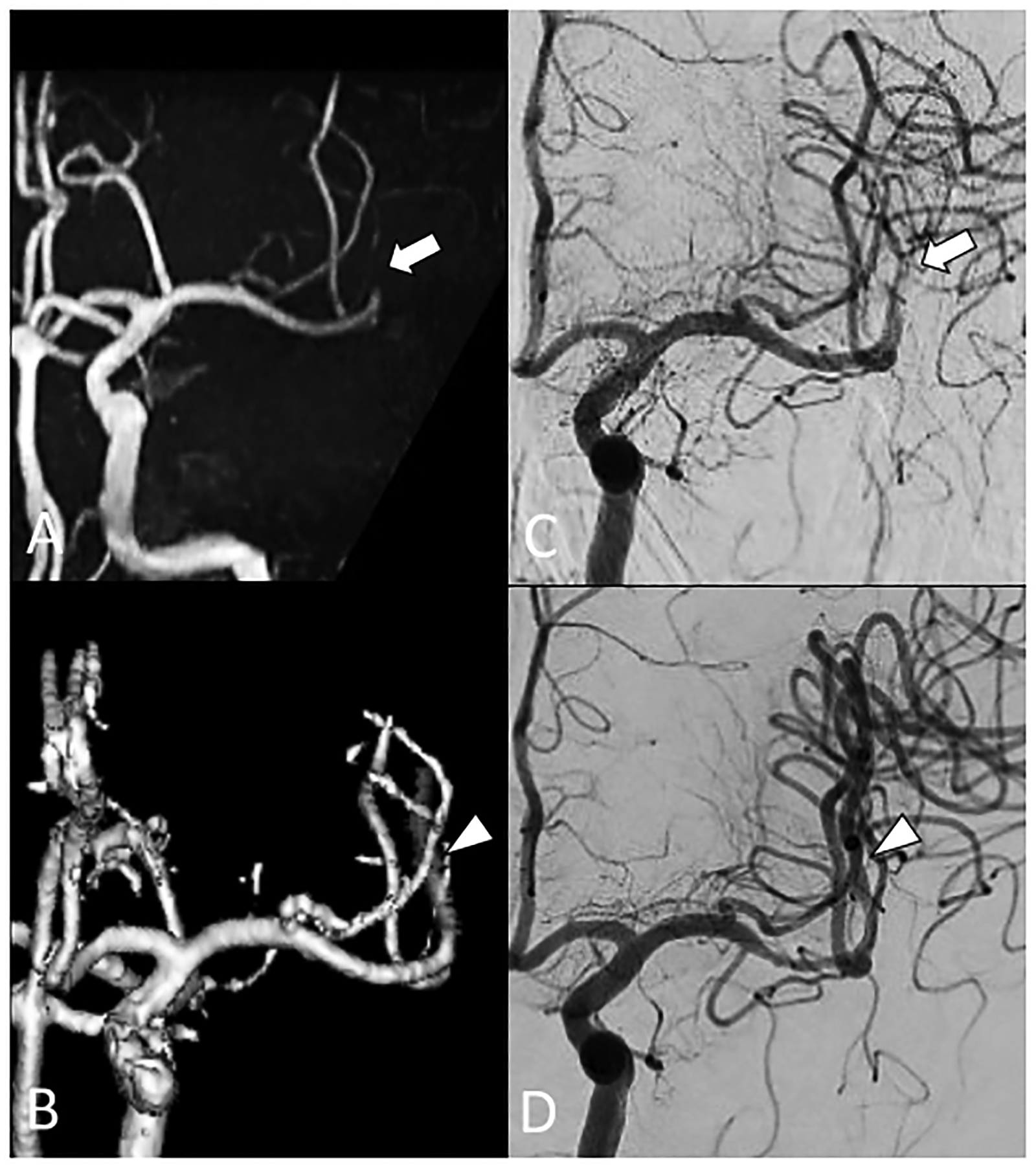
Case 2, an 85-year-old woman with sudden onset of consciousness disturbance. (a) Time-of-flight MR angiogram showing left PCA occlusion. (b) 3D proton density-weighted MRI with fast spin echo showing the occluded PCA from the proximal to the distal area. (c, d) Right vertebral angiograms before and after thrombectomy. Arrowheads indicate the cerebral vessels and arrows indicate the clot. MRI, magnetic resonance imaging; PCA, posterior cerebral artery.
Case 3, a 72-year-old man with sudden onset of dysarthria and right hemiparesis. (a) Time-of-flight MR angiogram showing occlusion of the second segment of the left MCA occlusion. (b) 3D proton density-weighted MRI with fast spin echo showing the occluded second segment from the proximal to the distal area. (c, d) Left internal carotid angiograms before and after thrombectomy. Arrowheads indicate the cerebral vessels and arrows indicate the clot. MCA, middle cerebral artery; MRI, magnetic resonance imaging.
Discussion
The present study demonstrated that 3D PDW-VWI with FSE using 1.5-T MRI without VRFA could also depict the cerebral vessels, including occluded lesions, as 3D PDW-VWI with VRFA-TSE using 3.0-T MRI could do.
During EVT, intraprocedural complications of subarachnoid hemorrhage involving vessel perforation, dissection, or aneurysmal perforation caused by the micro guidewire or micro catheter occurred in 0.6–5.5% of cases (2,3). Visualizing the division and direction of vessels, or the presence of unruptured aneurysm, is expected to contribute to a safe and more effective EVT. Several techniques using computed tomography or MRI have been demonstrated for visualization of the occluded invisible lesion before EVT in patients with AIS (4–6). Recent developments in VWI techniques using MRI include 2D or 3D, or T2-weighted (T2W) or PDW imaging. 3D is better than 2D for 3D and structural evaluation of the visible and invisible cerebral vessels (7). Furthermore, PDW-VWI could clearly depict the cerebral vessels, including occluded lesions, better than T2W VWI, because the blood vessels and surrounding tissue, such as brain parenchyma and cerebrospinal fluid, have different intensities. Thus, the effectiveness of 3D PDW-VRFA-TSE with 3.0-T MRI was recently demonstrated for visualization of the invisible occluded lesion before EVT in patients with AIS (4). However, the present study found that 3D PDW-FSE demonstrated good visualization of invisible vessels, including even the distal MCA, and contributed to good recanalization. On the other hand, the disadvantages of this method were lower quality of imaging and additional examination time compared to 3D PDW-VRFA-TSE using 3.0 T MRI.
3D VRFA-TSE provides a wide range of images with high resolution by reducing image blurring and can evaluate the lesion from various aspects based on the high spatial resolution and reformatting into multiplanar images with a short scan time (7), whereas 1.5-T MRI without VRFA is likely to suffer blurring. In this study, various innovations including optimization of echo time, pre-saturation pulse added to the eyeballs, and multiplanar reconstruction were performed and lead to better quality of imaging. However, the thrombus size and length could not unfortunately be depicted clearly in all five cases in this study, unlike with 3.0-T MRI. There might be reasons other than blurring, so further investigation is needed.
The scan time for PDW-FSE using 1.5-T MRI was 6 min 18 s, and total MRI scan time including PDW-FSE was 19 min 15 s. In contrast, the scan time for PDW-VRFA-TSE using 3.0-T MRI (Ingenia; Philips Medical Systems, Milwaukee, WI, USA) in our institute in accordance with the previously reported protocol (4) was 3 min 15 s, and the total MRI scan time including PDW-VRFA-TSE was 12 min 47 s. Time is the most important factor for the treatment of patients with AIS, so further imaging techniques such as narrowing the range of PDW-FSE imaging are needed to reduce the scan time.
New models of 1.5-T MRI with VRFA have already been developed and marketed. This new model (ECHELON Smart, FUJIFILM; MAGNETOM Avanto, Siemens Healthcare GmbH, Erlangen, Germany; SIGNA Explorer, GE Healthcare, Chicago, IL; Achieva, Philips Medical Systems) has the possibility of resolving these disadvantages, including the quality of imaging, scan time, and visualization of thrombus size and length. The usefulness of modified 3D T1-weighted imaging with VRFA-TSE using 1.5-T MRI for clearly depicting the cerebral vessels, including the occluded invisible lesion, has already been reported, but again the thrombus size and length could not be depicted clearly (8). Further investigations with 3D PDW-VRFA-TSE using 1.5-T MRI are needed.
The present study has some limitations. This study was carried out in a relatively small number of patients, but PDW-FSE using 1.5-T MRI provided additional detail about the occluded vessels similar to that provided by 3.0-T MRI. However, the length and size of the clot could not be clearly shown using this method. Further studies are needed to improve the efficacy and safety of this approach.
In conclusion, 3D PDW-FSE with 1.5-T MRI without VRFA could clearly depict the course of the invisible occluded artery, so might support favorable outcomes after EVT in patients with AIS.
List of five cases.
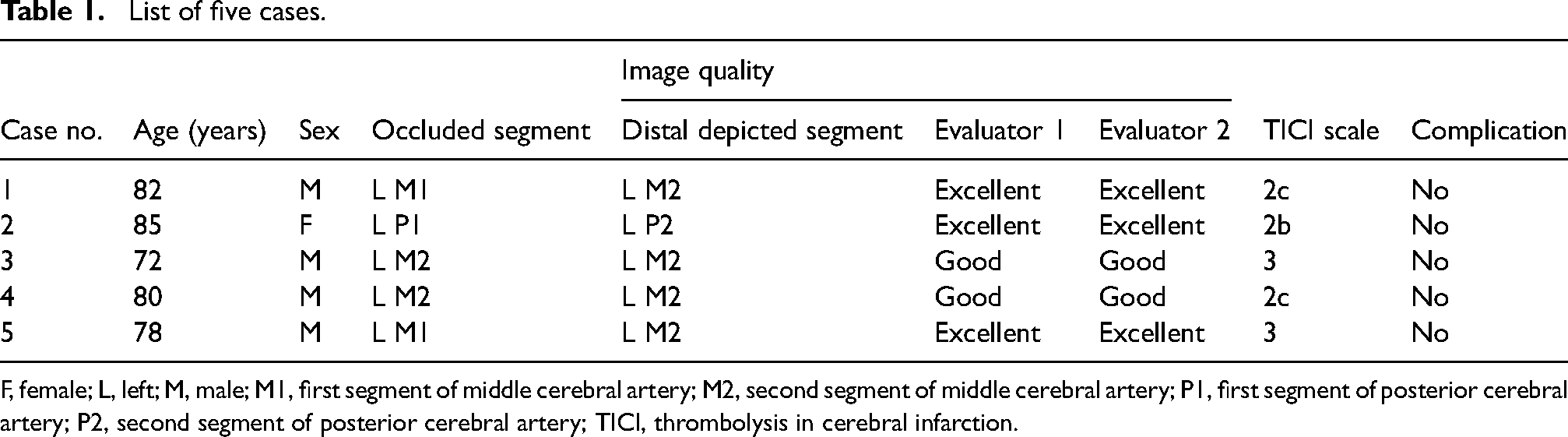
F, female; L, left; M, male; M1, first segment of middle cerebral artery; M2, second segment of middle cerebral artery; P1, first segment of posterior cerebral artery; P2, second segment of posterior cerebral artery; TICI, thrombolysis in cerebral infarction.
Footnotes
Acknowledgements
We thank Aries Publication Support for English proofreading.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.