
Abstract
Background
Computed tomography (CT)-guided percutaneous transthoracic needle biopsy (PTNB) is not recommended as the diagnostic modality of choice for anterior mediastinal lymphoma, despite its advantages of minimal invasiveness and easy accessibility.
Purpose
To identify the modifiable risk factors for non-diagnostic results from CT-guided PTNB for anterior mediastinal lymphoma.
Material and Methods
This retrospective study identified CT-guided PTNB for anterior mediastinal lesions diagnosed as lymphoma between May 2007 and December 2021. The diagnostic sensitivity and complications were investigated. The appropriateness of PTNB targeting was evaluated using positron emission tomography (PET)/CT and images from intra-procedural CT-guided PTNB. Targeting was considered inappropriate when the supposed trajectory of the cutting needle was within a region of abnormally low metabolism. The risk factors for non-diagnostic results were determined using logistic regression analysis.
Results
A total of 67 PTNBs in 60 patients were included. The diagnostic sensitivity for lymphoma was 76.1% (51/67), with an immediate complication rate of 4.5% (3/67). According to the PET/CT images, PTNB targeting was inappropriate in 10/14 (71.4%) of the non-diagnostic PTNBs but appropriate in all diagnostic PTNBs (P <0.001). Inappropriate targeting was the only significant risk factor for non-diagnostic results (odds ratio = 203.69; 95% confidence interval = 8.17–999.99; P = 0.001). The number of specimen acquisitions was not associated with non-diagnostic results (P = 0.40).
Conclusions
Only inappropriate targeting of the non-viable portion according to PET/CT was an independent risk factor for non-diagnostic results. Acquiring PET/CT scans before biopsy and targeting the viable portion on PET/CT may help improve the diagnostic sensitivity of PTNB.
Keywords
Introduction
Lymphomas are the second most common tumors arising in the anterior mediastinum, accounting for approximately 25% of tumors (1). They often show cystic and necrotic changes (2), making it challenging to accurately diagnose and differentiate them from other anterior mediastinal tumors. Even in cases of high suspicion of lymphoma based on clinical and imaging features, it is still necessary to obtain tissue. In anterior mediastinal lymphoma, tissue analysis is mandatory for setting the optimal treatment regimen according to the tumor phenotyping (1,3).
For tissue acquisition, surgical excisional biopsy is recommended in the current guidelines (4–7), despite its invasiveness and the requirement for general anesthesia and longer hospitalization. This is because lymphoma cells may be only sparsely present within the substantial sclerotic background (Hodgkin lymphoma), or because dense fibrosis within the mass (mediastinal large cell non-Hodgkin lymphoma) makes diagnosis with core needle biopsy difficult (1). In particular, necrosis and heterogeneous enhancement within lymphomas on computed tomography (CT) (8) can hamper targeting and obtaining a diagnostic portion. In fact, a recent meta-analysis reported that mediastinal lymphoma has a negative effect on the diagnostic yield of CT-guided percutaneous transthoracic needle biopsy (PTNB) (9). Nevertheless, given the lower invasiveness, higher safety, and short procedural time of PTNB in comparison with surgical biopsy, CT-guided PTNB could be attempted as a first-line diagnostic method.
To date, the diagnostic sensitivity of PTNB for anterior mediastinal lymphoma has been reported in some studies with small populations and was found to be moderate, ranging from 59% (13/22) (10) to 71.4% (30/42) (11). Although the low diagnostic yield for lymphoma is associated with the inherent limitations of PTNB, it is necessary to check whether there are other strategies to improve its accuracy besides multiple specimen acquisitions (3–5 times) (3); operators usually attempt to obtain more tissue to avoid the low diagnostic rate when lymphoma is suspected in routine clinical practice. Further investigation of the risk factors for non-diagnostic results could help improve the diagnostic sensitivity of PTNB. Therefore, the aim of the present study was to identify the modifiable risk factors for non-diagnostic results from PTNB for anterior mediastinal lymphoma.
Material and Methods
This retrospective study was approved by our institutional review board, which waived the requirement for informed patient consent (approval number: 2022-0347).
Study population
Between May 2007 and December 2021, a total of 433 consecutive CT-guided PTNBs (415 CT-guided core biopsies and 18 CT-guided aspirations) were performed in 404 patients for the diagnosis of anterior mediastinal lesions. Among them, those procedures performed in patients with pathologically confirmed lymphomas were finally included in this study.
Biopsy procedures
CT-guided PTNB was performed by dedicated thoracic radiologists (fellows under supervision or staffs). PTNBs were performed only with core needle biopsy when lymphoma was suspected. Two types of commercial CT scanners (HiSpeed iPro, GE Healthcare, Chicago, IL, USA; Somatom Definition AS, Siemens Healthineers, Erlangen, Germany) were used, and the CT parameters were as follows: 100 or 120 kVp; reference = 25 mA; collimation = 1.2 mm; and axial slice thickness = 1.5 or 3 mm.
Standard core needle biopsy was performed using the coaxial technique with a 20-gauge semi-automated biopsy gun (Stericut; TSK Laboratory, Tochigi, Japan). During the procedure, CT scans were obtained to confirm the pathway of the coaxial introducer. After confirmation of the proper location of the coaxial introducer at the target lesion, biopsy was performed using a cutting needle. A post-procedure CT scan was acquired to detect immediate complications. A chest radiograph was also obtained 4 h after the procedure to detect later complications.
Chest CT and PET/CT
Chest CT was performed using a multi-detector row CT system from one of two different manufacturers (Somatom Force, Definition, and Sensation-16, Siemens Healthineers; Lightspeed 16, Lightspeed VCT, and Discovery, GE Healthcare) with the following acquisition parameters: 120 kVp; 150–200 mA; pitch = 0.875–1; and collimation = 1–1.25 mm. Images were reconstructed using a sharp reconstruction kernel with a slice thickness/interval of 1/1 or 1.25/1.25 mm. The scanning covered the area from the base of the lungs to the level of the thoracic inlet. Contrast enhancement was performed in all patients via intravenous injection of contrast medium (90–120 mL iopromide [Ultravist, 300 mg I/mL; Bayer AG, North Rhine-Westphalia, Germany]) at a rate of 3 mL/s, with scanning beginning after a delay of 50 s.
Positron emission tomography (PET)/CT was performed for staging, usually after a pathological diagnosis of lymphoma; however, in patients highly suspected of having lymphoma, it was rarely performed before pathological diagnosis owing to an availability in the examination schedule. Images were obtained using one of several different scanners (Biograph Sensation 16 or Biograph TruePoint 40, Siemens Healthineers; Discovery PET/CT 690, 690 Elite, or 710, GE Healthcare). Patients were instructed to fast for 6 h before scanning. A dose of 370–555 MBq (0.2 mCi/kg) of 18F-fluorodeoxyglucose (FDG) was administered 60 min before scanning. The scanning covered the range from the skull base to the mid-thigh area, and a subsequent CT scan was obtained without contrast enhancement. Images were analyzed by nuclear medicine physicians using vendor-supplied software. The standardized uptake value (SUV) was measured by drawing a volume of interest to represent the tumor, and the highest SUV within the volume of interest (SUVmax) was reported.
Image analysis
Two thoracic radiologists (Yura Ahn and Sang Min Lee, with 5 and 14 years of experience in chest imaging, respectively) who were blinded to the PTNB results reviewed the pre-procedural chest CT and PET/CT images. On the chest CT, the two readers determined the presence of heterogeneous enhancement and necrosis of the target lesion. Heterogeneous enhancement was defined as non-uniform enhancement with variable attenuation on post-contrast scans, whereas necrosis was defined as an internal low-attenuation area of 10–30 Hounsfield units (12).
The appropriateness of PTNB targeting was evaluated using both intra-procedural CT-guided PTNB and PET/CT images. Comparing the intra-procedural CT scan showing the final position of the introducer needle to the PET/CT scan, the targeting was considered inappropriate when the supposed trajectory of the cutting needle was within a metabolic defect on the PET/CT. Otherwise, when the supposed trajectory of the cutting needle was within the area showing avid FDG uptake, the targeting was considered appropriate. A consensus was made via discussion for any discrepancies occurring during image analysis.
Clinical and pathological data collection
Patient characteristics, including demographics (age and sex) and history of lymphoma diagnosis and treatment, and procedural data, including the lesion size (largest diameter on axial images), needle size, approach type (parasternal vs. transpleural), distance from the skin to the target, and number of specimens acquired, were recorded. PTNB-related complications were also recorded by reviewing the procedural CT scans.
The pathological results of the PTNBs and surgical biopsies were recorded, and the pathological diagnosis was made on the basis of the latest lymphoma classification available at the time of diagnosis. To evaluate the diagnostic sensitivity of PTNB, we considered the results indicating lymphoma to be true positive, and all other results (e.g. fibrosis, necrosis, or atypical cells) to be non-diagnostic.
Statistical analysis
Continuous variables were compared using the independent t-test or the Mann–Whitney U test. Categorical variables were compared using Pearson's chi-square test or Fisher's exact test. Diagnostic accuracy was calculated using a definition in a previous study (diagnostic accuracy = precise diagnosis of the malignancy or benignity/all determinate results) (9). The risk factors for non-diagnostic PTNB results were determined using logistic regression analysis with Firth's penalized maximum likelihood estimation to reduce possible overfitting with relatively small sample sizes. Variables with P values <0.10 in the univariable analysis were used as input variables in the multivariable analysis. All statistical analyses were performed using MedCalc (version 20.009) and R (version 3.3.0), with P values <0.05 defined as statistically significant.
Results
Patient characteristics
Among the 433 PTNBs for anterior mediastinal lesions, a total of 67 PTNBs from 60 patients (38 men; mean age = 35 ± 15 years) revealed a final diagnosis of lymphoma (Fig. 1). On a per-patient basis, the most common final classification of lymphoma was primary mediastinal B-cell lymphoma (n = 16/60, 26.7%), followed by Hodgkin lymphoma (n = 15/60, 25.0%), T-lymphoblastic leukemia/lymphoma (n = 14/60, 23.3%), and diffuse large B-cell lymphoma (n = 12/60, 20.0%).
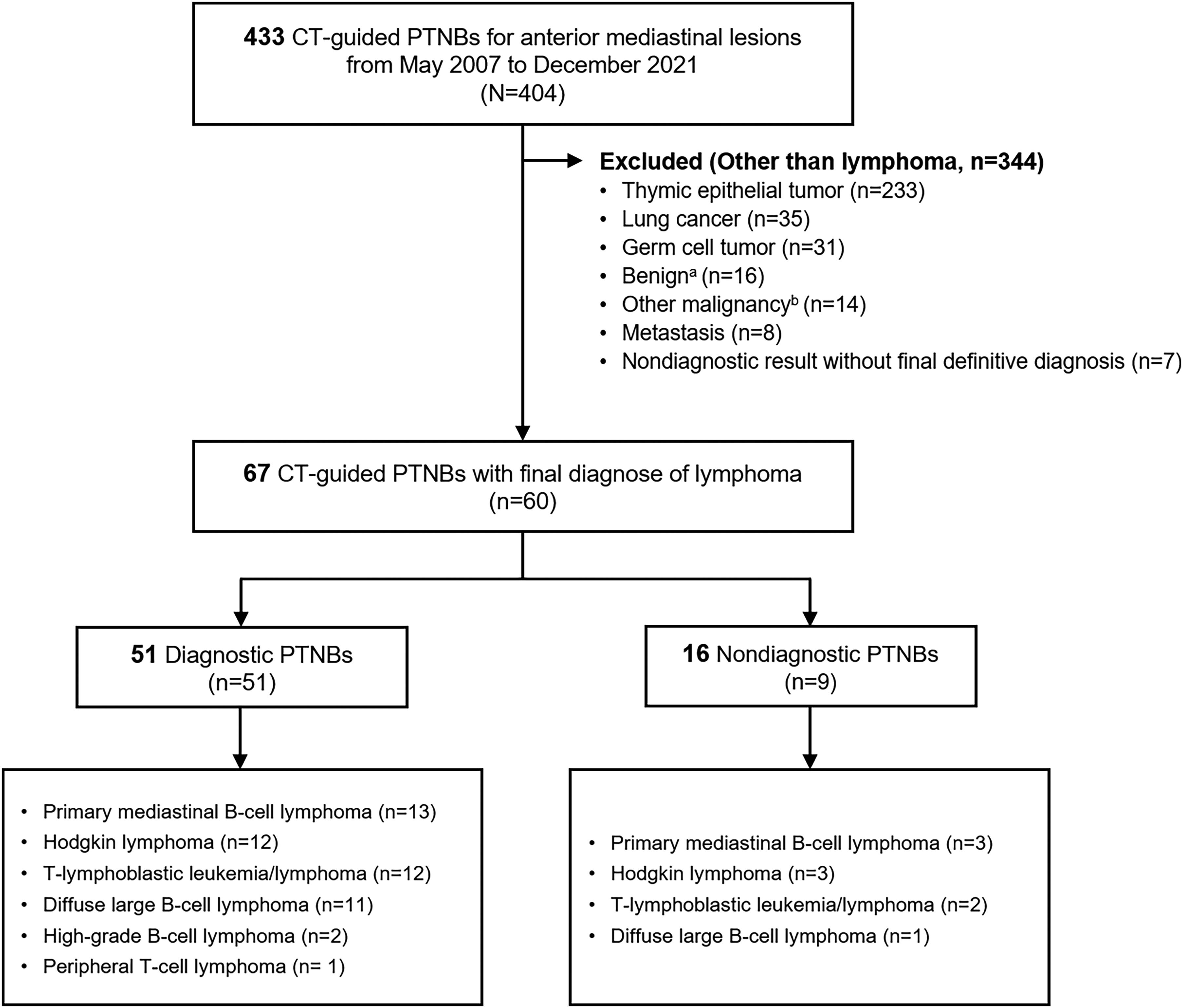
Flow diagram. aIncluding abscess, schwannoma, ectopic thyroid, lymphatic malformation, cyst, and non-specific benign result (e.g. chronic granulomatous inflammation). bIncluding neuroendocrine tumor, sarcoma, poorly differentiated carcinoma, melanoma, mesothelioma, and malignant peripheral nerve sheath tumor. CT, computed tomography; PTNB, percutaneous transthoracic needle biopsy.
Seven repeated PTNBs were performed in six patients because of non-diagnostic results (n = 4) or clinically suspected disease progression (n = 2). Among them, one patient underwent PTNB three times. On a per-patient basis, the final diagnosis was obtained with PTNB in 52/6 (86.7%) patients, surgical biopsy for anterior mediastinal lesions in six patients, and surgical biopsy for lymph nodes in two patients. Table 1 summarizes the characteristics of the study population.
Characteristics of the study population.
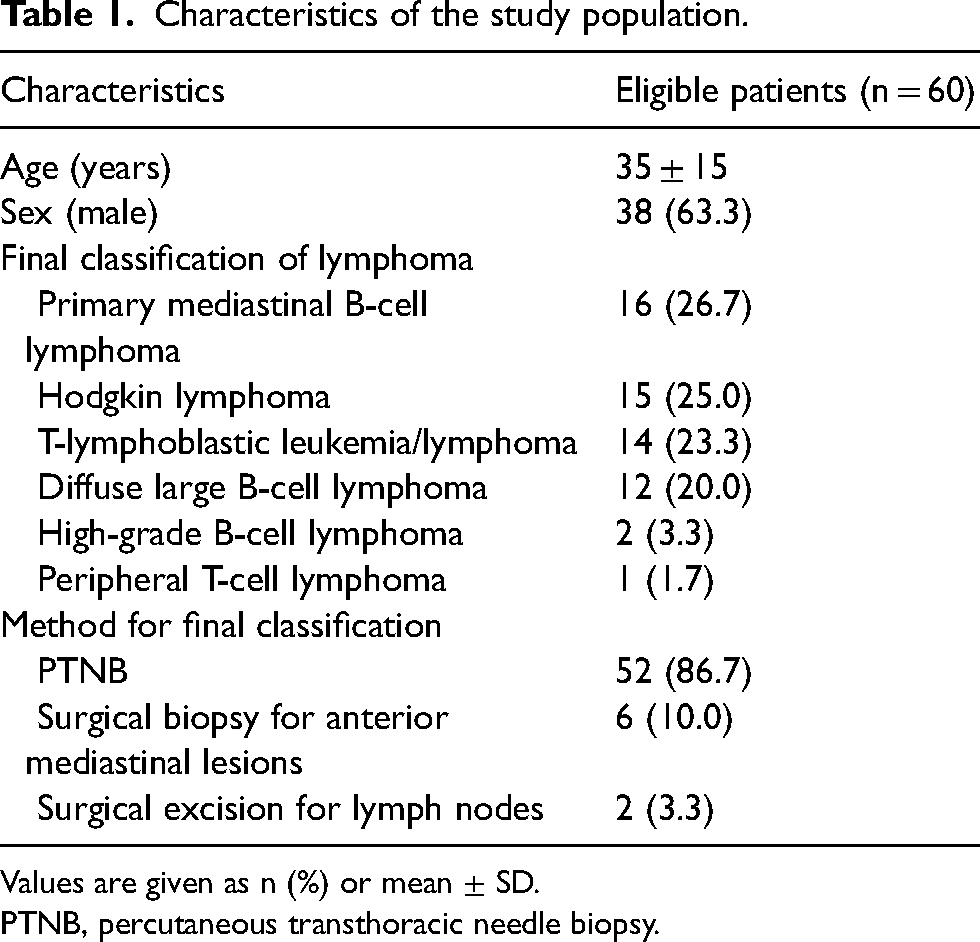
Values are given as n (%) or mean ± SD.
PTNB, percutaneous transthoracic needle biopsy.
Procedure details and lesion characteristics
On a per-procedure basis, the median target lesion size was 9.1 cm (range = 3.3–20.0 cm). The median distance of the needle pathway from the skin to the target was 4.0 cm (range = 2.3–8.7 cm). Most PTNBs were performed via the parasternal approach (n = 59/67, 88.1%). The median number of specimen acquisitions was 3 (range = 1–7), with specimens being obtained three times or more in 55/67 (82.1%) PTNBs, twice in 11 PTNBs, and once in one PTNB. The median procedural time was 13 min (range = 5–25 min). Immediate complications occurred in 3 (4.5%) procedures, with these all being a small pneumothorax that was managed conservatively without chest tube insertion. No later complication was reported.
On the chest CT scans, either heterogeneous enhancement or necrosis was shown in half of the target lesions (n = 34/67, 50.7% and 36/67, 53.7%, respectively). Both heterogeneous enhancement and necrosis were slightly more frequently observed in the patients with non-Hodgkin lymphomas than in those with Hodgkin lymphoma (25/47, 53.2% vs. 9/20, 45.0%; 27/47, 57.4% vs. 9/20, 45.0%, respectively). Enlargement of mediastinal lymph nodes was identified in 18/67 (26.8%) procedures, and enlargement of supraclavicular lymph nodes in 12/67 (17.9%). Pre-procedural PET/CT scans were available before PTNB for only 15/67 (22.4%) procedures. A total of 63 procedures had PET/CT scans obtained before induction therapy for the target lesion, with the median interval between procedure and PET/CT being 1 day (range = 0–36 days), and the mean SUVmax being 12.8 ± 5.6 (range = 1.8–25.8). In the comparison between intra-procedural CT and PET/CT, the targeting of PTNB was inappropriate in 10/63 (15.9%) procedures with PET/CT.
Diagnostic performance
Of the 67 PTNBs, 51 (76.1%) procedures were diagnostic for lymphoma (Fig. 2), whereas the other 16 (23.9%) procedures were non-diagnostic (14 non-specific benign pathologies and two misdiagnoses of malignancy other than lymphoma). All correct PTNB diagnoses provided detailed histological information on the specific lymphoma type, enabling prompt decisions regarding treatment. Among the total of 433 consecutive CT-guided PTNBs performed in 404 patients for the diagnosis of anterior mediastinal lesions, with the exception of seven non-diagnostic PTNBs without a final definite diagnosis, the overall accuracy for specific diagnosis was 86.6% (n = 369/426) and the sensitivity for lymphoma diagnosis was 76.1% (n = 51/67).
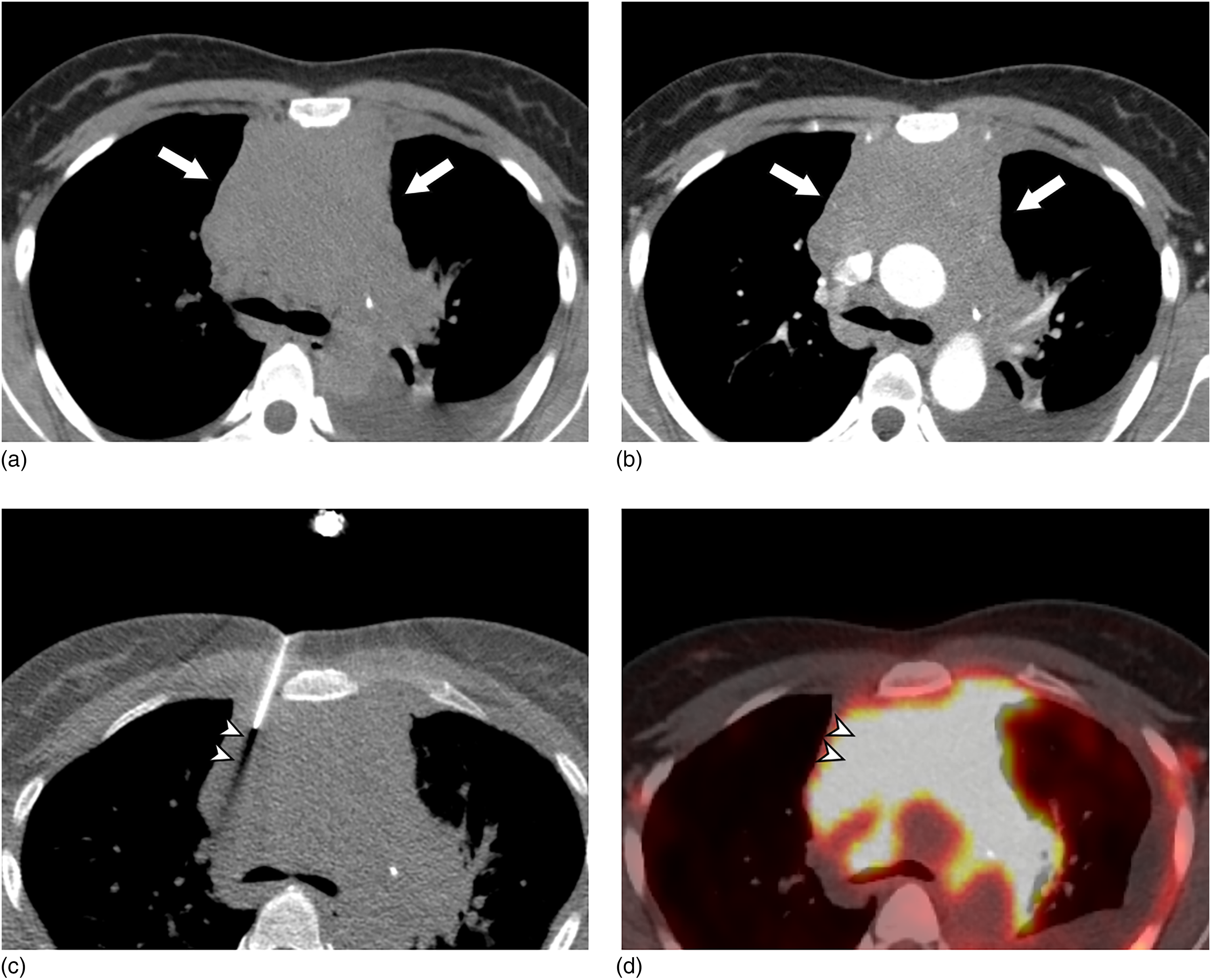
Diagnostic CT-guided PTNB for an anterior mediastinal mass in a 35-year-old woman. (a, b) Pre-contrast- and contrast-enhanced CT scans nine days before PTNB show an 8.5 cm solid mass with homogeneous enhancement in the anterior mediastinum (arrows). (c) During PTNB, the introducer needle was advanced via the parasternal approach and the trajectory of the cutting needle was supposed (arrowheads). Specimen acquisition was performed three times, and no immediate complication occurred. (d) Fused axial PET/CT scan acquired four days after PTNB shows diffuse avid FDG uptake in the mass (SUVmax = 12.7), including the supposed trajectory of the cutting needle (arrowheads); therefore, the targeting was determined as appropriate. The pathological diagnosis by PTNB was T-lymphoblastic leukemia/lymphoma. CT, computed tomography; FDG, fluorodeoxyglucose; PTNB, percutaneous transthoracic needle biopsy; SUV, standardized uptake value.
The final diagnoses of the non-diagnostic PTNB results were Hodgkin lymphoma (n = 8), primary mediastinal large B-cell lymphoma (n = 4), diffuse large B-cell lymphoma (n = 2), and T-lymphoblastic leukemia/lymphoma (n = 2). Four non-diagnostic PTNBs were performed for relapse or progression of treated Hodgkin lymphoma. Most non-diagnostic results were fibrosis with or without necrosis. For two diffuse large B-cell lymphomas, malignancy other than lymphoma was initially diagnosed on PTNB, with these being sarcomatoid carcinoma and germ cell tumor.
In the comparison between diagnostic and non-diagnostic PTNBs (Table 2), the median size of the target lesions was smaller in non-diagnostic PTNB than in diagnostic PTNB (8.1 vs. 9.4 cm, P = 0.02). There was no significant difference in the number of specimen acquisitions between them. Heterogeneous enhancement was more frequently observed in non-diagnostic PTNB than in diagnostic PTNB (75.0% [12/16]) vs. 43.1% [22/51]). In terms of PET/CT, there was no significant difference in the availability of pre-procedural PET/CT scans between the two groups. The SUVmax was significantly lower in non-diagnostic PTNB than in diagnostic PTNB (9.6 ± 4.7 vs. 13.8 ± 5.5, P = 0.01). According to the PET/CT scans, the targeting of PTNB was inappropriate in 10/14 (71.4%) of the non-diagnostic PTNBs (Fig. 3) and appropriate in all diagnostic PTNBs (P <0.001). Non-diagnostic PTNBs were more frequent in those procedures for progressed or relapsed lymphoma than in initially diagnostic procedures (4/16, 25% vs. 1/51, 2.0%). Hodgkin lymphoma was observed approximately twice more frequently in non-diagnostic PTNB than in diagnostic PTNB (8/16, 50.0% vs. 12/51, 23.5%, P = 0.04).
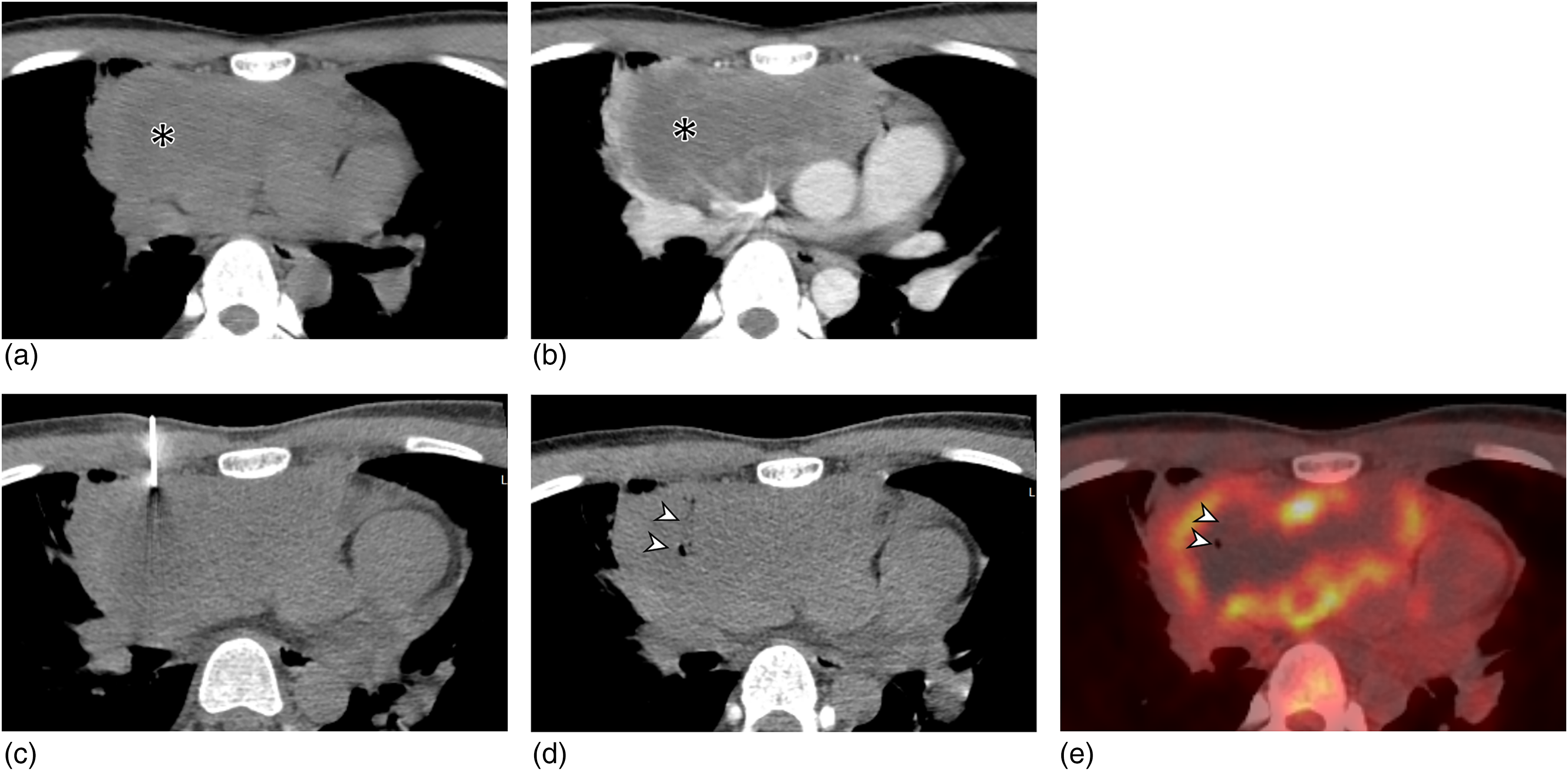
Non-diagnostic CT-guided PTNB with inappropriate targeting of an anterior mediastinal mass in a 19-year-old man. (a, b) Pre-contrast- and contrast-enhanced CT scans 10 days before PTNB show a 10.8 cm solid mass with heterogeneous enhancement and necrosis (asterisk) in the anterior mediastinum. (c) During PTNB, the introducer needle was advanced via the parasternal approach. Specimen acquisition was performed three times, and no immediate complication occurred. (d) The post-procedural scan shows air density along the supposed trajectory of the cutting needle (arrowheads). (e) Fused axial PET/CT scan acquired two days after PTNB shows peripheral FDG uptake in the mass (SUVmax = 8.7) with an internal metabolic defect with an air density, which was the supposed trajectory of the cutting needle (arrowheads). The targeting was determined as inappropriate. The pathological diagnosis by PTNB was a non-diagnostic result of fibrosis and necrosis. After two additional sequential PTNBs, the patient was finally diagnosed with Hodgkin lymphoma. CT, computed tomography; FDG, fluorodeoxyglucose; PTNB, percutaneous transthoracic needle biopsy; SUV, standardized uptake value.
Comparisons of the procedural records and characteristics of chest CT and PET/CT between diagnostic and non-diagnostic PTNBs.
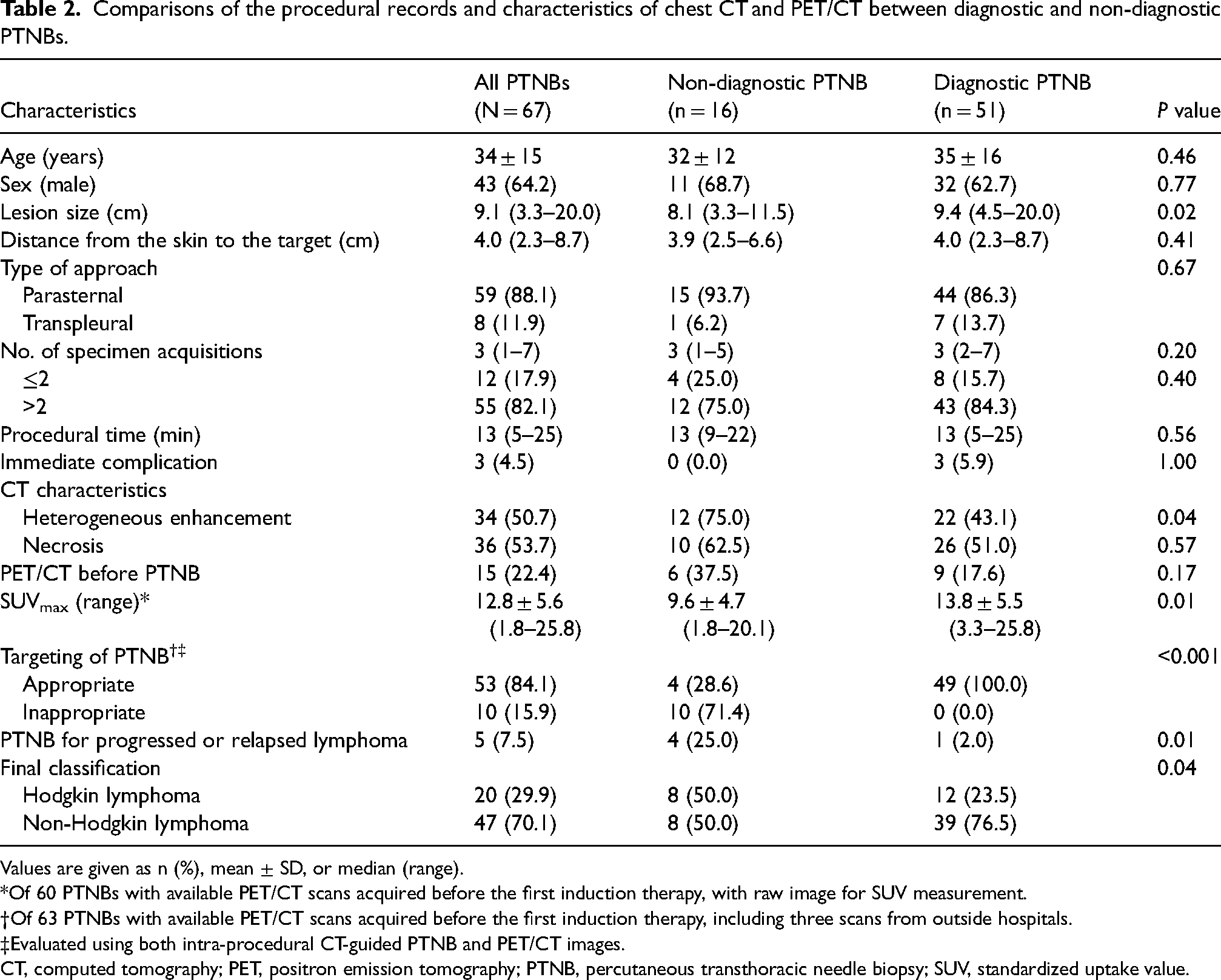
Values are given as n (%), mean ± SD, or median (range).
Of 60 PTNBs with available PET/CT scans acquired before the first induction therapy, with raw image for SUV measurement.
Of 63 PTNBs with available PET/CT scans acquired before the first induction therapy, including three scans from outside hospitals.
Evaluated using both intra-procedural CT-guided PTNB and PET/CT images.
CT, computed tomography; PET, positron emission tomography; PTNB, percutaneous transthoracic needle biopsy; SUV, standardized uptake value.
Risk factors for non-diagnostic results
In the univariable analysis of the risk factors for non-diagnostic PTNB results, lesion size (odds ratio [OR] = 0.97, 95% confidence interval [CI] = 0.95–0.99, P = 0.02), heterogeneous enhancement (OR = 3.95, 95% CI = 1.12–13.94, P = 0.03), SUVmax (OR = 0.86, 95% CI = 0.75–0.97, P = 0.02), inappropriate targeting of PTNB (OR = 230.91, 95% CI = 10.09–999.99, P <0.001), PTNB for progressed or relapsed lymphoma (OR = 12.12, 95% CI = 1.46–100.82, P = 0.02), and Hodgkin lymphoma (OR = 3.71, 95% CI = 1.12–12.37, P = 0.03) were associated with non-diagnostic PTNB results (Table 3) (13). In the multivariable analysis, inappropriate targeting of PTNB (OR = 203.69, 95% CI = 8.17–999.99, P = 0.001) was the only risk factor for non-diagnostic PTNB for lymphoma.
Risk factors for non-diagnostic PTNB results.
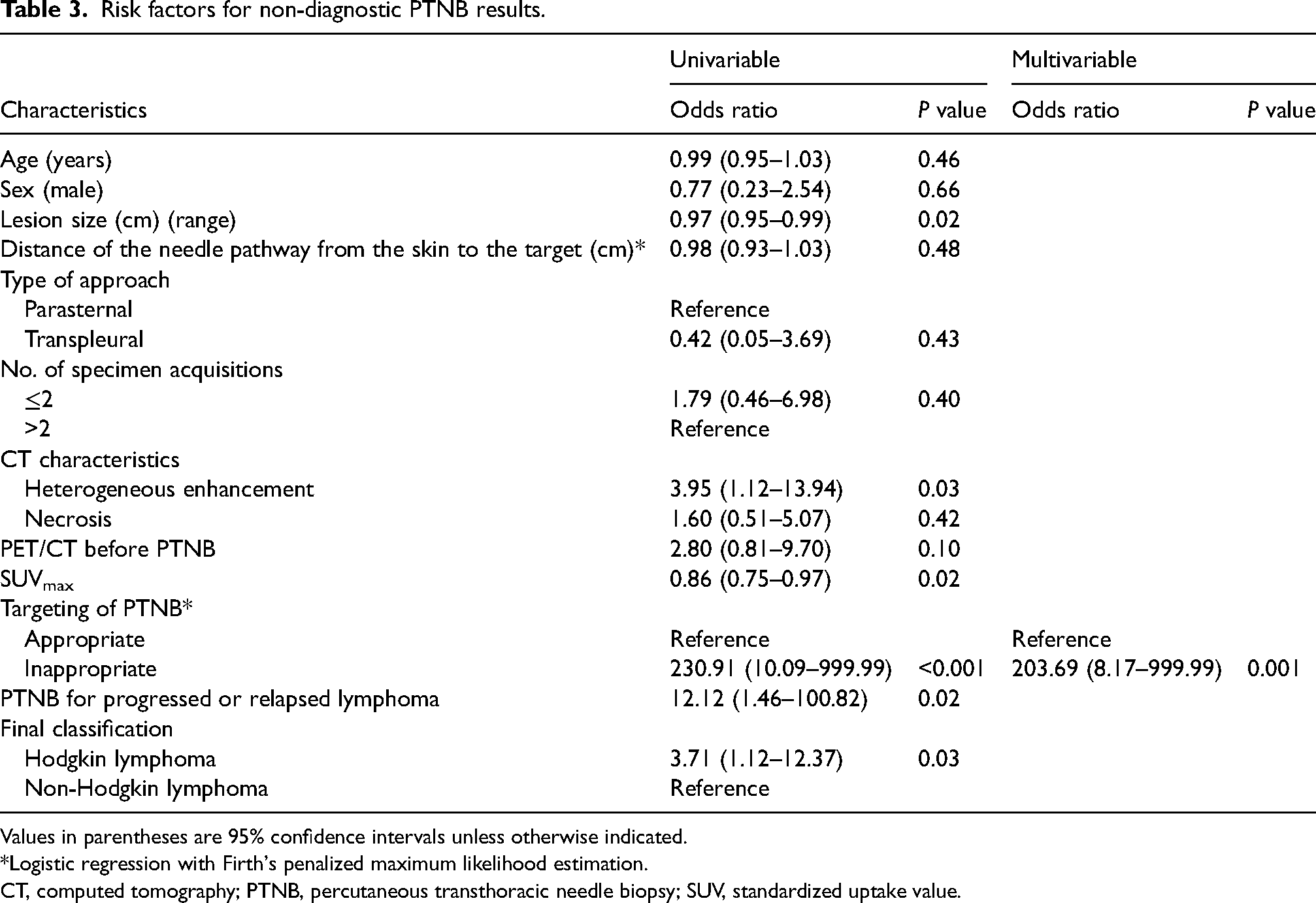
Values in parentheses are 95% confidence intervals unless otherwise indicated.
Logistic regression with Firth's penalized maximum likelihood estimation.
CT, computed tomography; PTNB, percutaneous transthoracic needle biopsy; SUV, standardized uptake value.
Discussion
Given its relatively low sensitivity, CT-guided PTNB is not recommended as the diagnostic modality of choice for anterior mediastinal lymphomas, despite its advantages of minimal invasiveness and easy accessibility. Non-diagnostic results are considered inherent limitations of needle biopsy, and modifiable risk factors have not been identified. In our study, PTNB showed a moderate sensitivity of 76.1% (n = 51/67), and inappropriate targeting of PTNB judged according to PET/CT scans was the only risk factor for non-diagnostic results (OR = 203.69, 95% CI = 8.17–999.99, P = 0.001).
In general, PTNB is widely accepted as a diagnostic method for mediastinal lesions, and it showed a high diagnostic yield (92%) in a recent meta-analysis (9). However, its sensitivity for anterior mediastinal lymphoma remains relatively low, in the range of 59%–76.1% (including the results of our study). The sensitivity values for core needle biopsy are an improvement on the sensitivity of 42.3% (n =11/26) reported for fine needle aspiration (14). Anterior mediastinal lymphoma commonly presents as a large mass on CT (2,3). Therefore, an advanced technique is not usually required to target the lesion itself. The low sensitivity of PTNB is thus considered to be mainly attributable to the heterogeneous distribution of viable lymphoma and non-viable portions (e.g. fibrosis or necrosis) within the lesion (1,15), which typically presents as heterogeneous enhancement on CT. Targeting of the viable portion is therefore necessary, and for this, CT may be insufficient to distinguish the viable portion from the nonviable portion.
FDG PET/CT shows differences in the glucose metabolism of tissues before overt structural change develops (16), thereby helping to distinguish the viable portion from the non-viable portion within heterogeneous tumors, lymph nodes, and pulmonary nodules (17–19). A study found that PET/CT-guided biopsies for various malignancies achieved high diagnostic accuracies in the range of 92%–94.3% (20,21), and yielded more diagnostic results than CT-guided biopsies with similar rates of adverse events (13). Currently, PET/CT is an essential modality for staging and response evaluation of lymphoma (22). Although several low-grade non-Hodgkin lymphomas (e.g. mucosa-associated lymphoid tissue lymphoma or mantle cell lymphoma) often show negative PET/CT results (23), most malignant lymphomas, including Hodgkin lymphoma or diffuse large B-cell lymphoma, which constitute the majority of anterior mediastinal lymphomas, show avid FDG uptake (23,24). As in other PET/CT-guided biopsies, identifying the site of avid uptake in large anterior mediastinal masses can help operators target the site most likely to be diagnostic. Indeed, all the diagnostic PTNBs in our study targeted the portion with FDG uptake, whereas 10/14 (71.4%) non-diagnostic PTNBs targeted metabolic defects. Although our results may seem obvious, no studies have actually demonstrated these findings in cases of anterior mediastinal lymphoma. We believe that appropriate targeting of PTNB according to PET/CT scans can actually improve its sensitivity and help diagnose patients with suspected lymphoma when PTNB is used as the first diagnostic method. In fact, in our institution, the final diagnosis was obtained with PTNB in most patients with suspected anterior mediastinal lymphoma (n = 52/60, 86.7%).
In addition, the number of specimen acquisitions was not associated with non-diagnostic results. This is because the specimen would be non-diagnostic if the trajectory of the cutting needle was in the non-viable portion, regardless of the number of times the specimen was obtained. Our results suggest that appropriate targeting should be achieved before obtaining an adequate amount of tissue.
Of 14 non-diagnostic PTNBs with available PET/CT scans, four failed to yield the final diagnosis despite appropriate targeting. Half of these PTNBs were in patients with Hodgkin lymphoma, with one of them being a clinically suspected relapse of treated lymphoma; all were finally diagnosed via surgical biopsy of mediastinal lesions or excisional biopsy of neck lymph nodes. Hodgkin lymphoma can be a diagnostic challenge, despite appropriate targeting of the viable portion, because with a limited amount of specimen it is often difficult to detect the Reed–Sternberg cells in the inflammatory background containing abundant benign lymphocytes (25). Furthermore, when relapse or progression is suspected in treated lymphoma, inflammation after treatment also shows increased FDG uptake (23), mimicking the viable portion. Therefore, surgical biopsy should be considered when results are suspected to be false-negative despite appropriate targeting.
The present study has some limitations. First, we included a relatively small number of PTNBs because of the rarity of anterior mediastinal lymphomas. Second, our determination of the appropriateness of targeting was partly based on assumptions. This is an inherent limitation of the CT-guided procedure because the CT scans were not acquired during the firing of the cutting needles. Therefore, the trajectory of the cutting needle was supposed from the final position and direction of the introducer needle. Finally, we retrospectively evaluated the PTNBs, and therefore could not assess the effect of pre-procedural PET/CT on the diagnostic sensitivity of PTNB. Pre-procedural PET/CT scans were available in only 15/67 (22.4%) PTNBs, and with the retrospective design, we did not determine whether the operator referred to the PET/CT scans to target the viable portion before the procedure. Further large cohort prospective studies are needed to evaluate the role of pre-procedural PET/CT on the diagnostic performance of PTNB.
In conclusion, only inappropriate targeting of the non-viable portion on PET/CT was an independent risk factor for non-diagnostic results. Acquiring PET/CT scans before biopsy and targeting the viable portion on PET/CT may help improve the diagnostic sensitivity of PTNB.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.