
Abstract
Background
Despite thorough preoperative work-up for cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC), so called open-close (OC) procedures as a result of irresectable disease remain common. Currently, diagnostic laparoscopy (DLS) is considered the gold standard, and consequently overrules the results of computed tomography (CT) scans; however, certain regions of the abdomen are difficult to assess and postoperative adhesion formation may further compromise staging during DLS.
Purpose
To determine whether better clinical assessment could be achieved by combining the results of DLS and preoperative CT scans during a multidisciplinary team (MDT) meeting.
Material and Methods
All patients who were eligible for CRS-HIPEC after DLS, but eventually underwent an OC procedure between 2010 and 2018 were selected. Radiological reassessment of CT scans was performed and combined with assessment of the DLS during a MDT meeting. The MDT was blinded for the outcome of the procedure (OC vs. CRS-HIPEC).
Results
The majority of the OC procedures (69%) was correctly predicted by the MDT. In most patients (88%), this conclusion was based on the combination of the radiological and surgical peritoneal cancer index (PCI). CT was particularly accurate for detection of larger tumor deposits in the abdominal regions, as 84%–86% was detected. Assessment of lesions in the small bowel regions is troublesome; 72% of lesions are missed on the preoperative CT scan.
Conclusions
A combination of radiological and surgical assessment of the PCI may lead to improved preoperative patient selection for CRS-HIPEC.
Keywords
Introduction
The combination of cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS-HIPEC) is associated with improved survival and is used as treatment for patients with limited colorectal peritoneal metastases (PM) (1,2). CRS-HIPEC is an invasive procedure with considerable postoperative morbidity and mortality (3). Therefore, adequate patient selection is important (4,5).
The peritoneal cancer index (PCI) is an internationally validated scoring system, used to report on patients’ intraperitoneal tumor load found during (diagnostic) surgery (6–8). The PCI is calculated by giving 13 abdominal regions a score in the range of 0–3, according to the presence and size of lesions, resulting in a total PCI score (in the range of 0–39) (6). In the Netherlands, patients are generally deemed ineligible for CRS-HIPEC when the PCI is above 20.
Radiological findings in patients with peritoneal metastases can be non-specific and small peritoneal implants are usually not visible (9,10). Furthermore, as a result of previous surgery and/or diffuse intraperitoneal anomalies, interpretation of radiological findings can be challenging. Therefore, radiological assessment frequently leads to underestimation of the PCI (11).
To accurately estimate the intra-abdominal extent of disease and to determine eligibility for CRS-HIPEC, diagnostic laparoscopy (DLS) is currently the standard of care in the Netherlands. With the implementation of DLS, unnecessary laparotomies, so called open-close (OC) procedures in patients who have extensive peritoneal disease (PCI >20), may be prevented (12,13). Obtaining a complete overview of all abdominal regions during DLS can be challenging due to adhesions resulting from prior surgery and/or tumor invasion in adjacent organs or tissues. Moreover, some regions are more difficult to visualize than others, in which the body composition and anatomy of the patient may play a role. As a result, in approximately 27% of patients, the overview obtained during DLS is incomplete, which contributes to inadequate staging of the PCI (12).
The aim of the present study was to determine whether systematic radiological PCI assessment is of additional value and whether combining the radiological PCI with the surgical PCI (DLS) in a multidisciplinary team (MDT) meeting could contribute to better patient selection for CRS-HIPEC, and therefore prevent OC procedures.
Material and Methods
Patient selection
The present study was conducted in two tertiary referral centers in the Netherlands. All consecutive patients who underwent a DLS during preoperative work-up, but eventually underwent an OC procedure, between 2010 and 2018 were identified. Furthermore, a random selection of patients who underwent complete CRS-HIPEC after DLS were selected as a control group to blind the MDT for any predetermined outcomes. Patients who had a PCI score >20 during the work-up for CRS-HIPEC or in whom irresectable disease was found during DLS were excluded from this study. The MDT was blinded for the outcome of the procedure (OC vs. successful CRS-HIPEC) and distribution of patients between the control group and OC group.
Patient demographics, perioperative characteristics, and tumor characteristics were extracted from the medical records after formal approval by the institutional medical ethics committee was obtained (registration number MEC-2018-1286).
Standard preoperative work-up
Preoperative screening
All patients underwent thorough preoperative screening. This included a physical examination, preoperative screening by an anesthesiologist, and radiological assessment computed tomography (CT) with intravenous contrast of the chest and abdomen to rule out systemic metastases. General contraindications for CRS-HIPEC were presence of >3 liver metastases and/or other (extra-)abdominal metastases.
Diagnostic laparoscopy
During the DLS, the abdominal cavity was accessed and the extent of peritoneal disease was scored using the PCI according to Sugarbaker. The PCI was calculated by giving 13 abdominal regions a score between 0 and 3, according to the presence and size of lesions, resulting in a total PCI score (in the range of 0–39) (6). If the total PCI found during DLS was ≤20 and complete cytoreduction seemed feasible, patients were planned for an elective CRS-HIPEC procedure.
Intended CRS-HIPEC
After abdominal access via laparotomy, a thorough assessment of the abdomen was performed and the PCI was scored again. Occasionally, adhesiolysis had to be performed in order to create a complete overview of all abdominal regions. In case of a PCI >20 or irresectable disease, the operation was discontinued and the abdomen was closed without further resection (OC procedure).
Simulated multidisciplinary team meeting
In a simulated MDT meeting, in which two radiologists specialized in colorectal malignancies, two CRS-HIPEC surgeons and two researchers participated; all patients (both patients having undergone an OC procedure and controls) were reviewed. All participants were blinded for the outcome of surgery.
Radiological reassessment of all preoperative CT scans
Two radiologists scored each abdominal region according to the PCI scoring system: region 0 = central – midline abdominal incision, entire greater omentum, transverse colon; region 1 = right upper – superior surface of the right lobe of the liver, undersurface of the right hemidiaphragm, right retrohepatic space; region 2 = epigastrium – left lobe of the liver, lesser omentum, falciform ligament; region 3 = left upper – undersurface of the left hemidiaphragm, spleen, tail of pancreas, anterior and posterior surfaces of the stomach; region 4 = left flank – descending colon, left abdominal gutter; region 5 = left lower – pelvic sidewall lateral to the sigmoid colon, sigmoid colon; region 6 = pelvis – female internal genitalia with ovaries, tubes, uterus, bladder, Douglas pouch, rectosigmoid colon; region 7 = right lower – right pelvic sidewall, cecum, appendix; region 8 = right flank – ascending colon, right abdominal gutter; region 9 = upper jejunum; including both bowel and its mesentery; region 10 = lower jejunum – including both bowel and its mesentery; region 11 = upper ileum – including both bowel and its mesentery; and region 12 = lower ileum – including both bowel and its mesentery (Fig. 1).
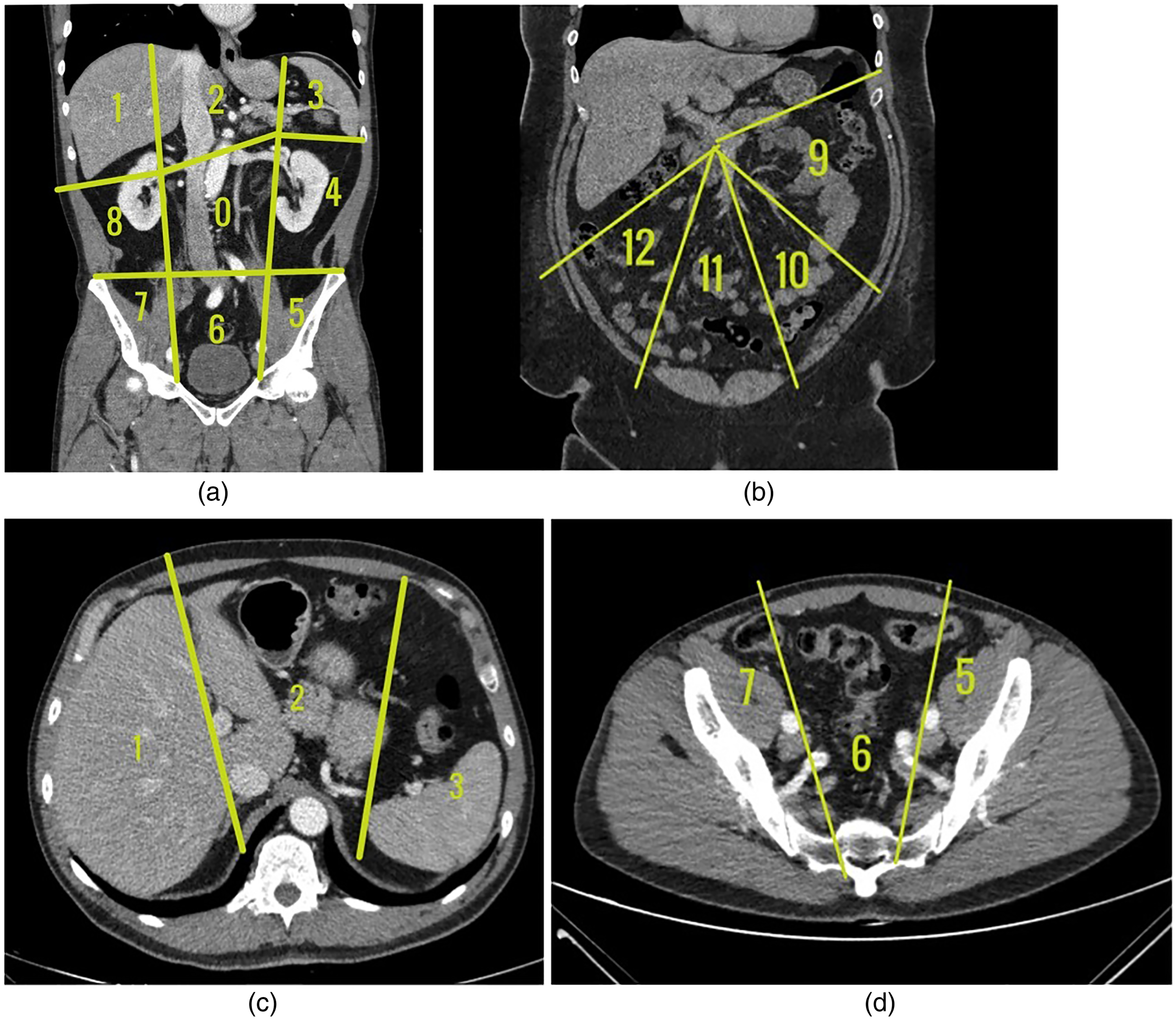
Anatomical landmarks for assessment of the radiological PCI. (a) Coronal view of regions 0–8. (b) Transverse view of PCI regions 1, 2, and 3. (c) Transverse view of PCI regions 5, 6, and 7. (d) Coronal view of regions 9–12. PCI, peritoneal cancer index.
The CT scans of patients from both groups were randomly presented to the radiologists who were blinded for the surgeons’ findings during DLS and for the final outcome (CRS-HIPEC or OC procedure). In case of disparities between the two radiologists’ findings, consensus was achieved.
Combining radiological findings with surgical findings (DLS)
Later, the radiological PCI and the report of the DLS in which all abdominal regions were also scored were combined and the findings were discussed by radiologists and surgeons. The combination of these findings led to a final MDT decision on the extent of the disease as described by the PCI and whether the patient was considered eligible for CRS-HIPEC. The surgeons and radiologists were blinded as to which treatment the patients had ultimately undergone. In Fig. 2, the work-up for CRS-HIPEC and the role of the MDT as described in this study is shown.
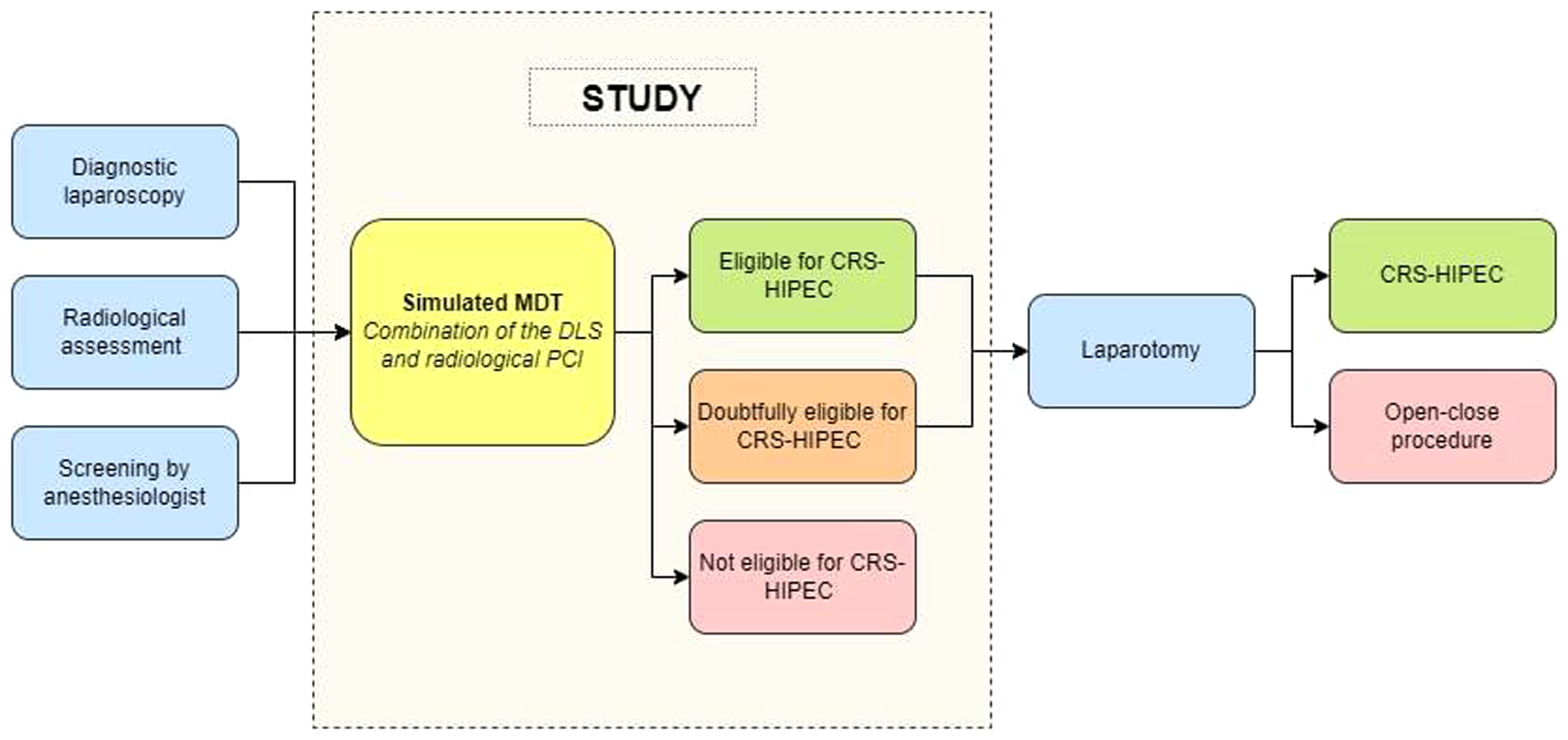
Flow chart of the study. CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; PCI, peritoneal cancer index.
Statistical analysis
Continuous variables were presented as median with interquartile range (IQR). Categorical variables were presented as absolute numbers and percentages. Baseline characteristics were compared using the chi-square test (for proportions) and Mann–Whitney U test (for continuous data). Two-sided P values <0.05 were considered statistically significant. Statistical analyses were performed using SPSS version 24.0.0 (IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
Between 2010 and 2018, a total of 35 patients underwent an OC procedure after complete preoperative work-up, including CT scan and DLS. These patients were compared with 26 randomly selected patients who underwent CRS-HIPEC in the same period.
Incomplete staging during preoperative DLS was more common in patients who underwent an OC procedure (P = 0.02). In 69% of patients who underwent an OC procedure, it was not feasible to inspect all PCI regions, or staging was not performed according to the PCI method. This was the case in only 35% of patients who underwent CRS-HIPEC.
The time between DLS and laparotomy was shorter in patients who did undergo CRS-HIPEC (P = 0.02). As expected, total PCI found during DLS, radiological PCI, and PCI found during laparotomy were higher in patients who underwent an OC procedure, when compared to the CRS-HIPEC group (all items P < 0.05). The length of hospital stay after laparotomy was longer in the CRS-HIPEC group (P <0.001) (Table 1).
Baseline characteristics and perioperative outcomes.

Boldvalues are given as n (%) or median (IQR).
CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; IQR, interquartile range; LOS, length of hospital stay; OC, open-close procedure; PCI, peritoneal cancer index.
Multidisciplinary team meeting
Tables 2 and 3 show the results of the DLS, the radiological assessment, the MDT consensus, and the OC/CRS-HIPEC procedure. In 24/35 (69%) patients having undergone an OC procedure, the MDT concluded that the patient was not eligible for CRS-HIPEC. In 21/24 (88%) patients, this conclusion was based on the combination of the radiological PCI and the surgical PCI. In 3/24 (13%) patients, the DLS was not performed according to the standard of care and the abdomen was not assessed systematically according to the PCI scoring method. If DLS had been performed according to local standards, an unnecessary laparotomy would have been prevented. In 11/35 (31%) patients who went on to undergo an OC procedure, the MDT still concluded that the patient was eligible for CRS-HIPEC. Possible explanations why the MDT could not predict PCI >20 are shown in Table 3.
PCI score and conclusions made during DLS, CT, MDT and OC (N = 35) / CRS-HIPEC (N = 26) procedure.
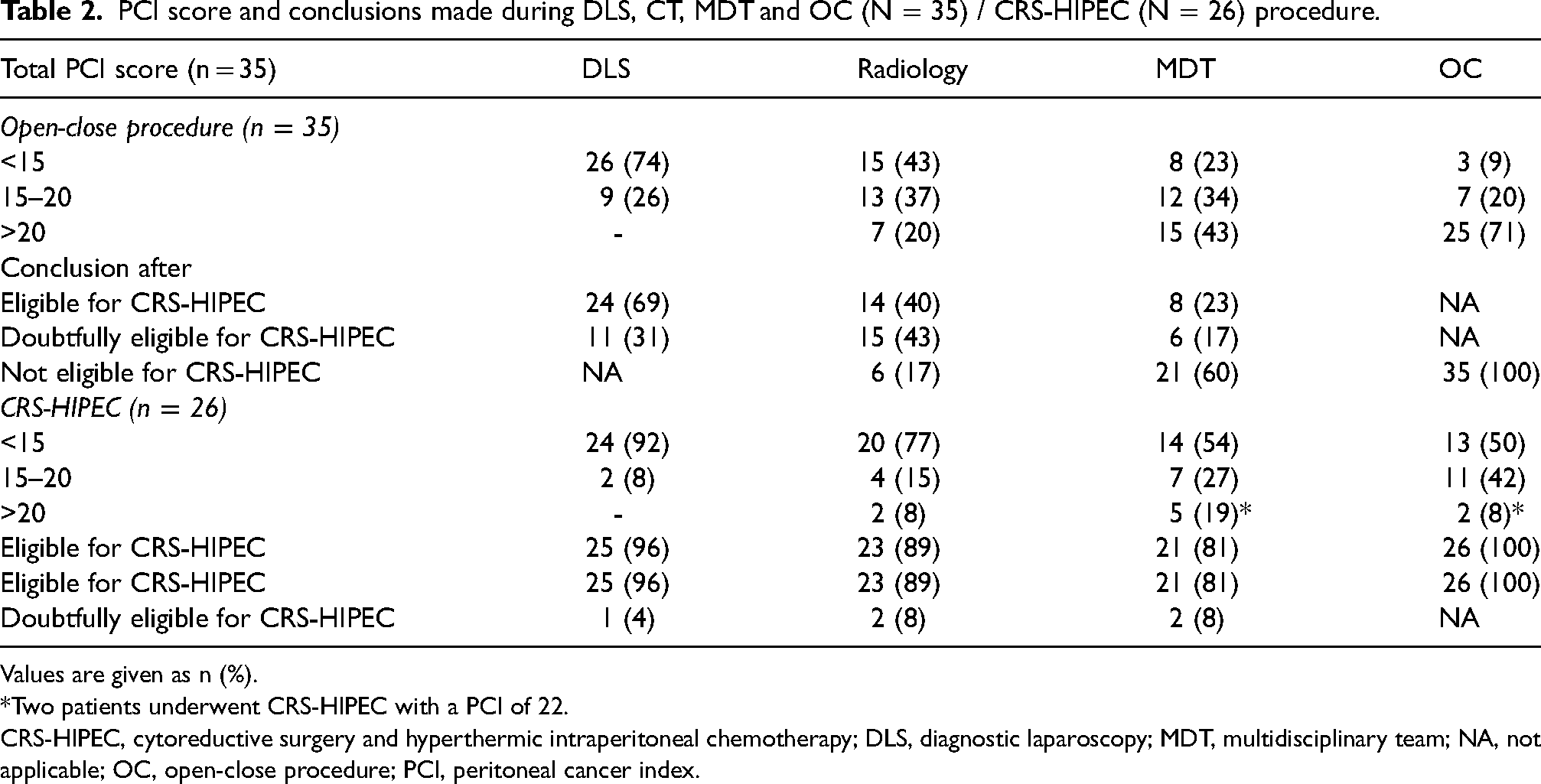
Values are given as n (%).
Two patients underwent CRS-HIPEC with a PCI of 22.
CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; MDT, multidisciplinary team; NA, not applicable; OC, open-close procedure; PCI, peritoneal cancer index.
Conclusions after the multidisciplinary team meeting (n = 35).
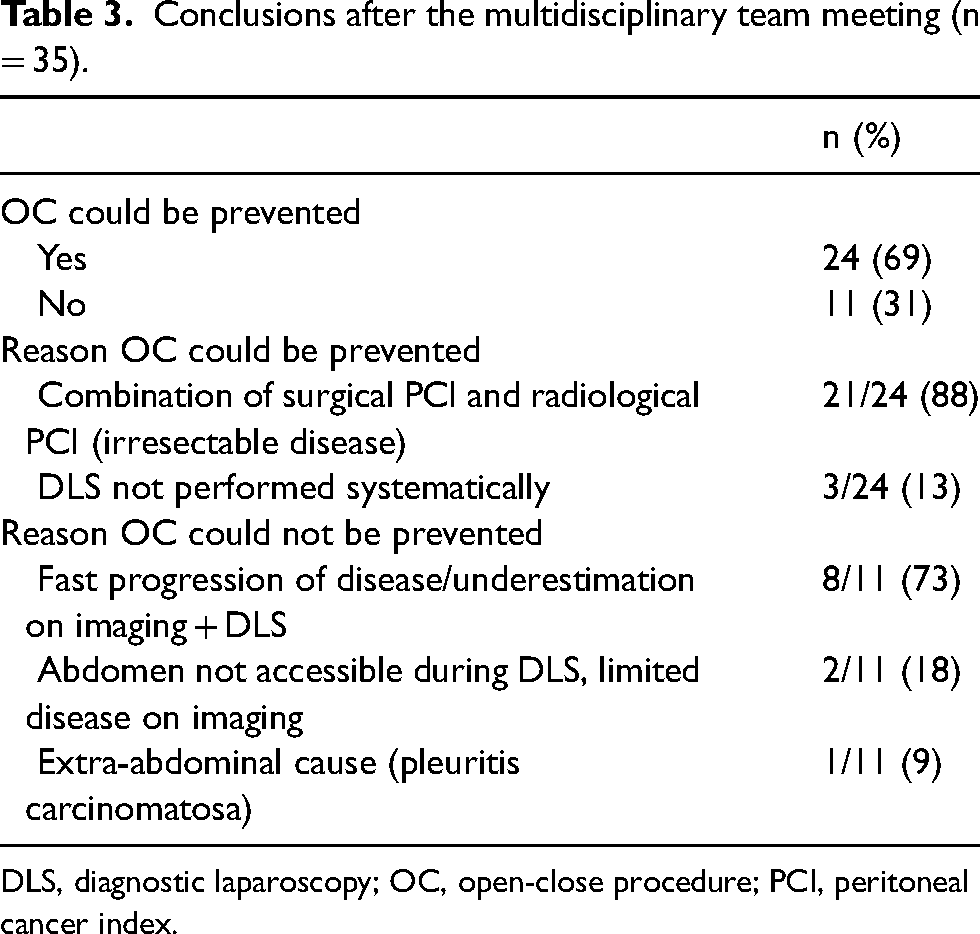
DLS, diagnostic laparoscopy; OC, open-close procedure; PCI, peritoneal cancer index.
In 3/26 (12%) patients who did undergo CRS-HIPEC, the MDT concluded that the patient was not eligible for CRS-HIPEC due to irresectable disease. Of those three patients, two did in fact have a PCI >20, but CRS-HIPEC was still performed because complete CRS was considered feasible by the operating surgeons and because the PCI was underestimated during the start of the procedure, after which the surgeons reached a point of no return. The third patient was found to have extensive peritoneal plaque formation after neoadjuvant chemotherapy. Perioperative frozen sections showed fibrotic tissue only, after which the patient underwent CRS-HIPEC.
Table 4 shows detailed information on how often a PCI region (regions 0–12) was judged to be involved during DLS, CT, MDT, and OC/HIPEC procedures.
Detailed information on regions scored during DLS, CT, MDT and OC (N = 35) / CRS-HIPEC (N = 26) procedure.
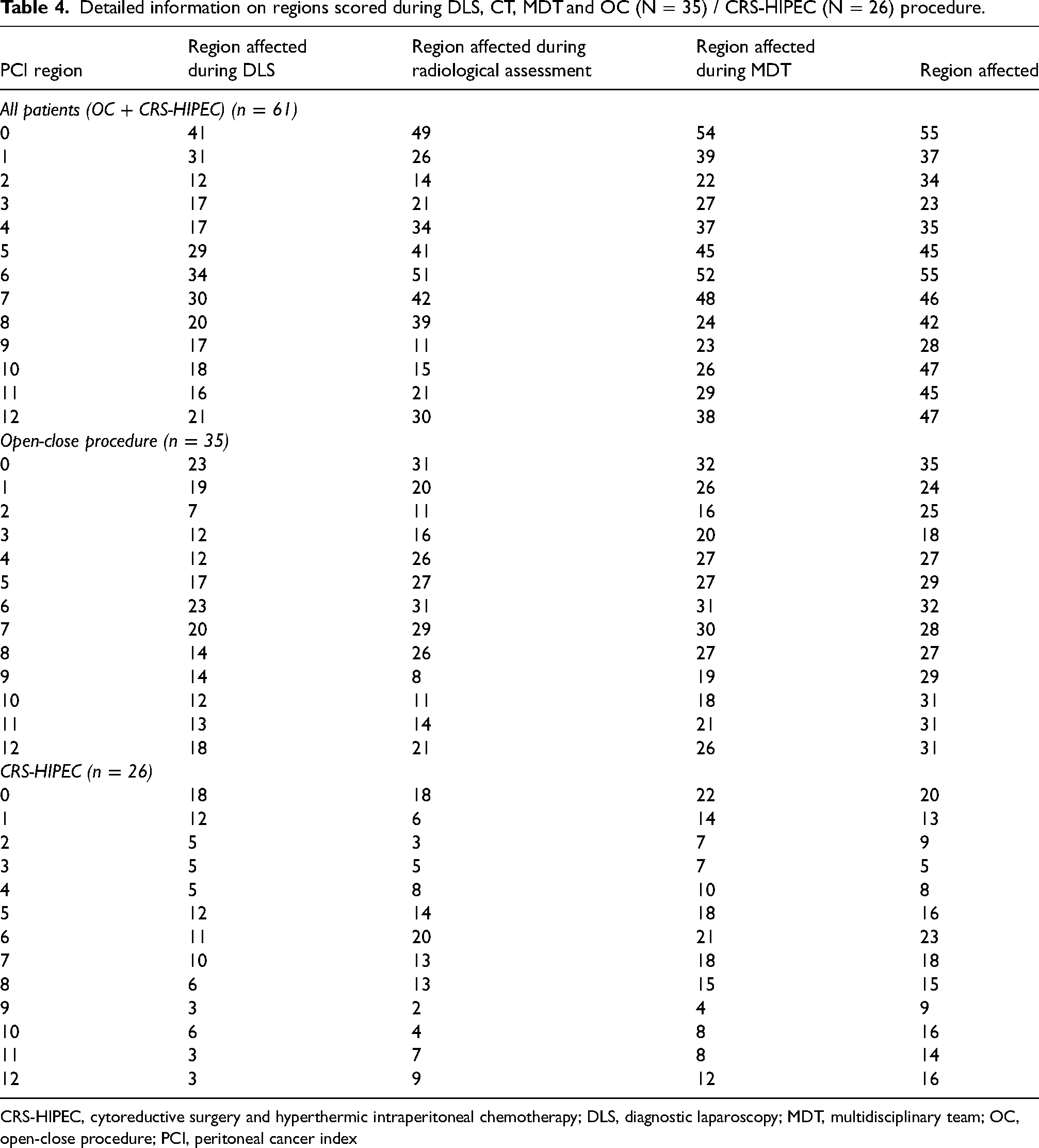
CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; MDT, multidisciplinary team; OC, open-close procedure; PCI, peritoneal cancer index
Lesions missed during radiological assessment
Table 5 presents discrepancies between the surgical PCI scored during DLS and the radiological PCI score based on imaging. Small lesions scored were often missed during radiological assessment (52%), followed by medium sized lesions scored 2 (21%) and large lesions scored 3 (13%).
Lesions missed during radiological assessment but scored during DLS.
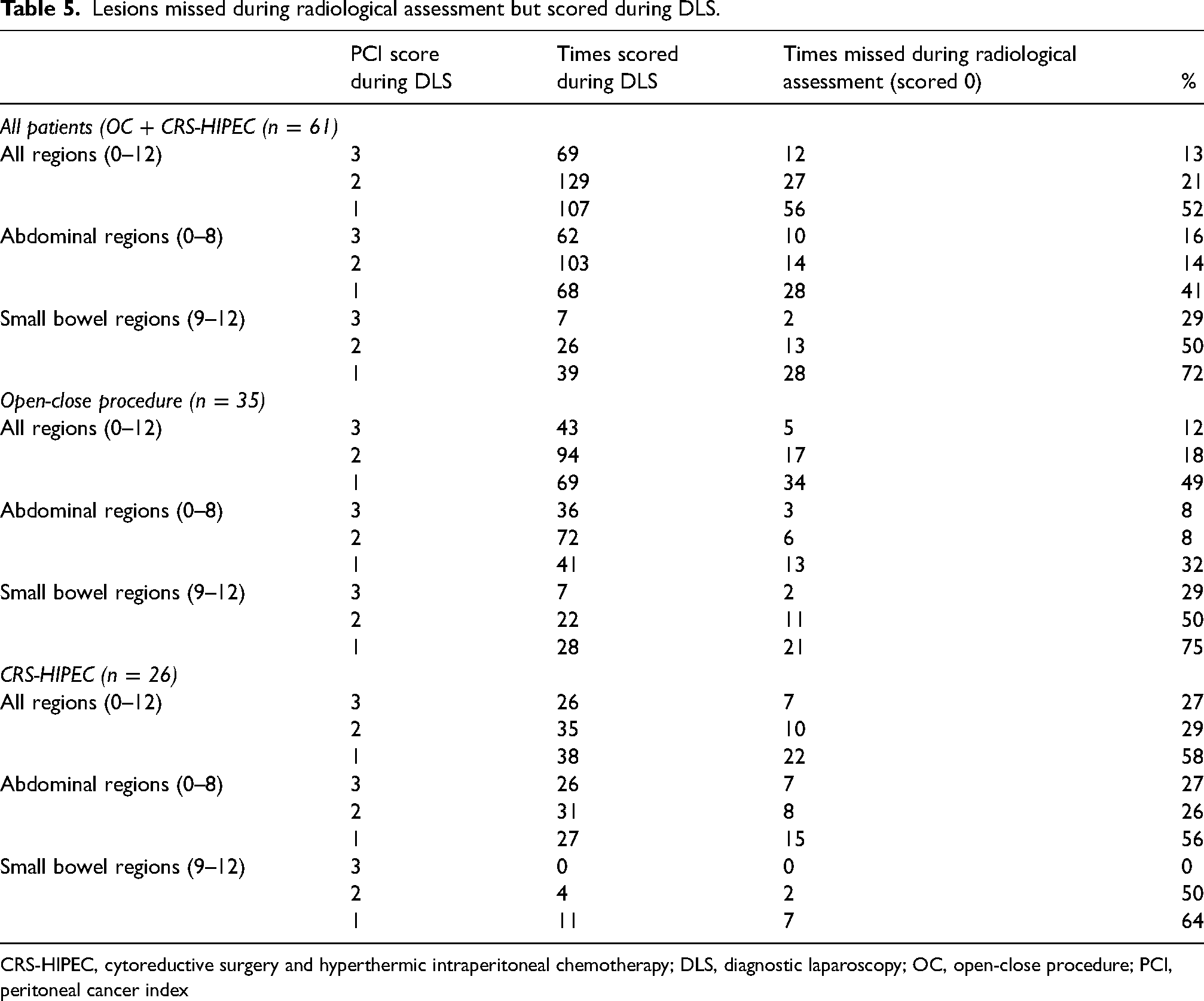
CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; OC, open-close procedure; PCI, peritoneal cancer index
Lesions scoring 1 or 2 involving the small bowel (regions 9–12) were more frequently missed during radiological assessment when compared to abdominal regions 0–8 (lesion size 1: 72% vs. 41%, P = 0.002; lesion size 2: 50% vs. 14%, P <0.001). The comparison of lesion size 3 between the small bowel and abdominal regions was not significant (29% vs. 16%, P = 0.392).
Lesions missed during surgical assessment
Table 6 shows the lesions missed during the surgical assessment but scored during the radiological assessment. The difference between small lesions (scored 1) missed during surgery (49%), lesions scored 2 (47%) and lesions scored 3 (41%) was not statistically significant. When we compared the abdominal regions with the small bowel regions there was no difference in the detection of lesions scored 1 (38% vs. 52%, P = 0812) or 2 (57% vs. 45%, P = 0080). Lesions scored 3 in the small bowel region during radiological assessment were more frequently missed when compared with the abdominal regions (76% vs. 35%, P < 0.001). A comparison of all regions separately was not significant (data not shown).
Lesions missed during surgical assessment (DLS), but scored during radiological assessment.
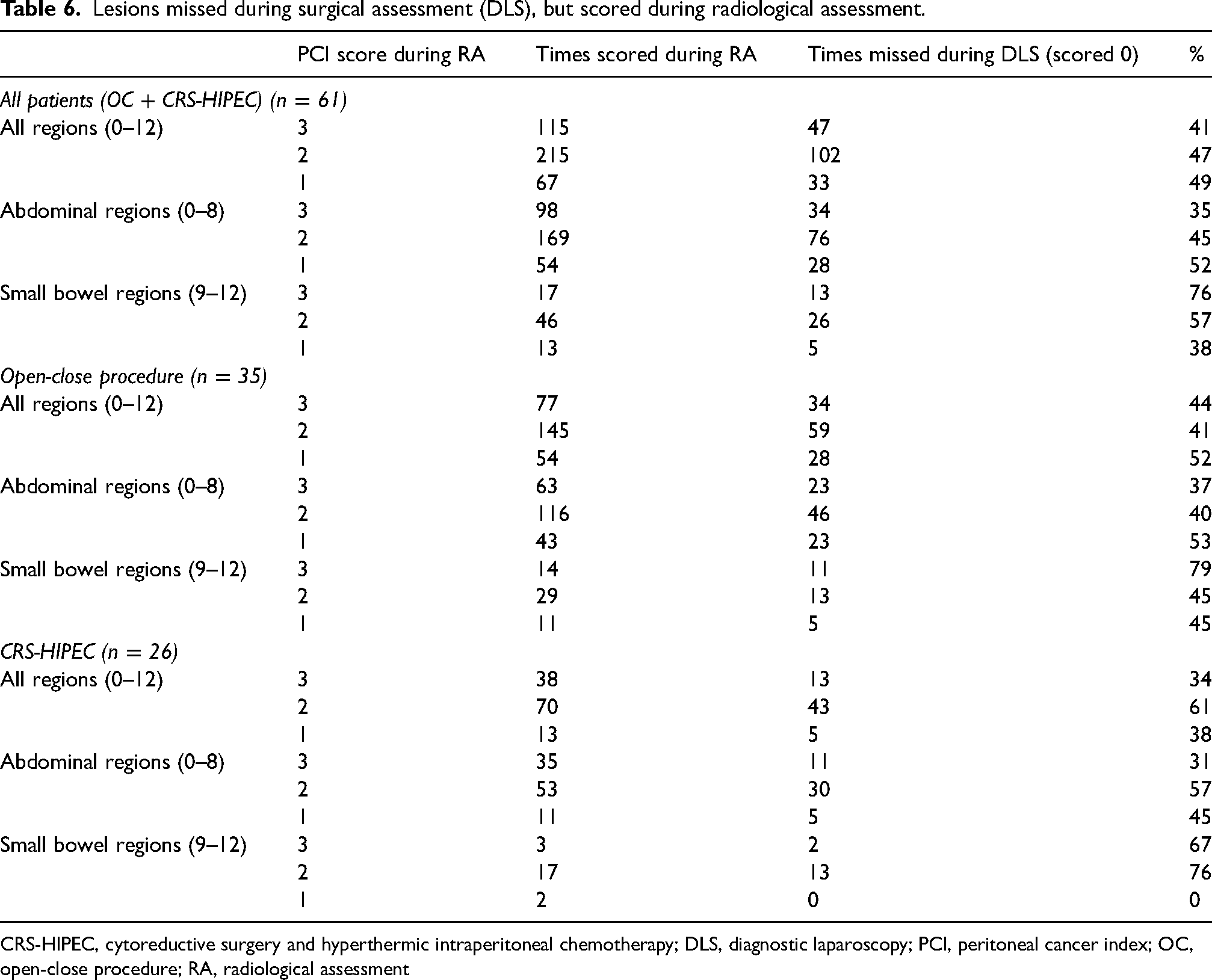
CRS-HIPEC, cytoreductive surgery and hyperthermic intraperitoneal chemotherapy; DLS, diagnostic laparoscopy; PCI, peritoneal cancer index; OC, open-close procedure; RA, radiological assessment
Discussion
The present study shows that patient selection for CRS-HIPEC can be improved by integrating the findings during DLS and CT during a MDT meeting. In 69% of OC cases, the MDT concluded that the PCI exceeded 20. This suggests that the visual PCI as scored by the surgeon during DLS is often inaccurate and misses peritoneal metastases that may have been identified on the preoperative CT scan. Patients may be spared unnecessary laparotomies, hospitalization, and potential morbidity; in addition, further treatment (e.g. systemic chemotherapy) would not have to be delayed. Besides a decrease in treatment burden, this will also result in cost reduction.
Although DLS is still considered to be the gold standard by most experts, the present study shows that discarding the results of other diagnostic modalities leads to the missing of critical peritoneal metastases. This can be explained by either the suboptimal execution of the DLS, or by limitation of the view by the patient's anatomy or hidden location of peritoneal metastases. In the present study, we also tried to identify specific regions that are more difficult to assess during DLS; unfortunately, the differences between regions were all not significant.
On the other hand, DLS is particularly valuable for the detection of miliary metastases on the mesentery, which are often missed by CT scan, given the typical small size of these lesions. Performing DLS systematically and reporting the PCI (per region) is of great importance. However, even when PCI is assessed according to standard of care, incomplete staging is common since it is not always feasible to assess all regions when performing laparoscopy (i.e. because of adhesions or tumor invasion) (12). In the present study, DLS was incomplete in 69% of patients who underwent an OC procedure. By specifically addressing regions on the CT scan that are difficult to visualize in a specific patient, a more accurate estimation of the PCI and thus eligibility for CRS-HIPEC might be achieved.
Currently, CT still is the most commonly used imaging tool during preoperative work-up in patients with colorectal cancer to detect liver and pulmonary metastases. Nevertheless, it is not commonly used to score the extent of intraperitoneal disease, as previous studies showed that CT generally underestimates the PCI (9,11). However, the sensitivity for larger nodules is adequate and these nodules that were clearly visible on CT were not always visualized during DLS.
This study showed that CT appears to be accurate for the detection of larger tumor deposits (size 2–3). CT is especially valuable in the abdominal regions 0–8, as 84%–86% of the lesions scored 2 or 3 were accurately detected. Small peritoneal lesions (scored 1) were detected in only half of the cases, and particularly small lesions in the small bowel regions are difficult to assess; 72% were missed.
This, together with the difficulties seen during DLS due to adhesions and tumor invasion, underlines that the combination of the two tools is of added value in the selection of patients for CRS-HIPEC.
The present study also showed that OC procedures were inevitable in some cases. The median time between DLS and OC was 38 days, which was significantly longer when compared to the time between DLS and HIPEC (26 days) (P = 0.020), which may have influenced our results. The median time between imaging and laparotomy was not significantly different (OC group: 46 days vs. HIPEC group: 57 days). During this time, PM may have increased. Keeping these intervals as short as possible might decrease the number of OC procedures.
This is the only study we are aware of that investigates the value of combining radiological and surgical PCI to assess the possibility of performing CRS and HIPEC. There are several limitations, of which most are inherent to the retrospective nature and small study population. An in-depth reassessment of the radiological findings was performed to assess the radiological PCI, but for the surgical PCI, only operation reports for DLS and OC procedures could be obtained.
To decrease the chance on bias, a control group of patients that did undergo CRS-HIPEC was added, and all members of the MDT were blinded for the outcome of the procedure (OC vs. successful CRS-HIPEC).
In the control group, the MDT concluded that in two patients, suitability for CRS-HIPEC was doubtful, and that in another three patients the PCI was >20. This was confirmed in two patients during surgery, and CRS-HIPEC was performed nonetheless. However, in one patient, the MDT appeared to have overestimated the PCI. The presence of extensive abdominal fibrosis on the mesentery caused this false-positive result for the radiological assessment. This patient had been treated with neoadjuvant chemotherapy and the pathology reports did not reveal malignant tissue. This further underlines our hypothesis that findings of preoperative imaging and DLS should be combined. In this patient, these plaques could have been evaluated specifically during the DLS and biopsies could have been taken. The integration of results from radiology and intraoperative findings is likely to be superior with a structured assessment of preoperative imaging, followed by a DLS that specifically addresses the findings on the CT. In the ideal scenario, the surgeon performing the DLS would use a radiological PCI, check each region, and change the score when visual assessment is adequate and different from the radiological assessment.
Although it is not considered standard of care yet, diffusion-weighted imaging (DWI) is another promising imaging modality for the evaluation of the abdominal tumor load and is potentially more reliable than CT (14–16). Currently, the accuracy and usefulness of DWI in the preoperative work-up for patients with colorectal PM is investigated in the Dutch multicenter randomized controlled DISCO trial (NCT04231175). In the future, DWI might be a valuable addition to the preoperative work-up for CRS-HIPEC. Whether DWI will be sensitive and specific enough to replace DLS is unsure, but in any case, the combination of MRI and DLS may further improve the results of integrated staging by preoperative imaging and DLS.
In conclusion, this study shows that combining the surgical PCI, as assessed during DLS, and the radiological PCI, assessed with CT by a MDT, could improve patient selection for CRS-HIPEC. By doing so, the majority of OC procedures may be prevented, thereby decreasing surgery-related morbidity and costs in patients with an incurable disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.