
Abstract
Background
Percutaneous cholecystostomy (PC) is a therapeutic intervention for acute cholecystitis. The benefits of cholecystostomy have been demonstrated in the medical literature, with up to 90% of acute cholecystitis cases shown to resolve postoperatively, and only 40% of patients subsequently undergoing an interval cholecystectomy.
Purpose
To compare the survival outcomes between acute complicated and uncomplicated cholecystitis in patients undergoing PC as an initial intervention, as there is a paucity of evidence in the literature on this perspective.
Material and Methods
A retrospective search was conducted of all patients who underwent PC for acute cholecystitis between August 2016 and December 2020 at a tertiary institution. A total of 100 patients were included in this study.
Results
The outcome, in the form of 30-day mortality, 90-day mortality, being alive after six months, and reintervention, was compared between complicated and uncomplicated cases using the chi-square test or Fisher's exact test. There was no statistically significant difference in any of the compared outcomes. The only variable that showed a statistically significant association with the risk of mortality was acute kidney injury (AKI) at admission. Patients who had stage 1, 2, or 3 AKI had a higher hazard for mortality as compared to patients with no kidney disease.
Conclusion
Our results demonstrate that PC is a safe and effective procedure. Mortality is not affected by the presence of complications. The results have, however, highlighted the importance of recognizing and treating AKI, an independent risk factor affecting mortality.
Introduction
Acute cholecystitis is a common condition accounting for 3%–10% of all patients presenting with acute abdominal pain (1). Of these cases, 90%–95% are secondary to cholecystolithiasis and are therefore termed acute calculus cholecystitis (2). Complications from acute cholecystitis are not uncommon, and are estimated to occur in 7%–26% of cases with varying severity, morbidity, and mortality. Complications include gallbladder gangrene, perforation and subsequent biliary peritonitis or biloma, abscess formation, and the formation of a biliary fistula or cystic artery pseudoaneurysm (1). The updated Tokyo guidelines in 2018 (TG18) provide a framework in which to categorize the severity of acute cholecystitis as mild, moderate, or severe, based on the presence of some of these complications in addition to other physical and biochemical findings (3).
Early laparoscopic cholecystectomy is the gold standard for managing acute calculus cholecystitis according to the 2020 World Society of Emergency Surgery most recent guidelines (4). Percutaneous cholecystostomy (PC) is an alternative therapeutic intervention that involves the image-guided insertion of a drain for the purpose of decompressing the gallbladder under local anesthesia. This has the benefit of being minimally invasive, which is particularly advantageous in those deemed unfit for surgery under TG18 guidelines (5) and can serve either as a definitive treatment or as a bridge to an elective cholecystectomy when the patient is convalescent.
The benefits of cholecystostomy have been demonstrated in the medical literature, with up to 90% of acute cholecystitis cases shown to resolve postoperatively (6), and only 40% of patients subsequently undergo an interval cholecystectomy (7). Severe cases based on the TG18 severity grading treated with PC have been reported to be associated with lower rates of definitive cholecystectomy; however, this appears to come at a cost of higher mortality and higher hospital readmission rates (8).
The aim of the present study was to compare the outcomes between acute complicated and uncomplicated cholecystitis in patients undergoing PC as an initial intervention, as there is a paucity of evidence in the literature on this perspective. This study aims to refine the patient selection criteria by comparing parameters that affect the outcome of cholecystostomy in these two patient groups to optimize the patient's status before this intervention.
For this study, we categorized cases with imaging evidence of gangrene, perforation, or biloma, or those with concurrent emphysematous change as acute complicated cholecystitis and those without these features as uncomplicated cholecystitis.
Material and Methods
A retrospective search was conducted of all patients who underwent PC for non-malignant causes of acute cholecystitis between August 2016 and December 2020 at a single-center, tertiary institution. In view of ensuring the baselines of co-morbidities were comparable, all patients included in the study were not suitable for surgical intervention. Ethical approval is not applicable to this study, as this study is based upon a service improvement project using pseudo-anonymized patient data.
In total, 100 patients who underwent PC were included in this study. The procedure was performed under ultrasound guidance using an 8-Fr drain by either a transhepatic or transperitoneal route, at the discretion of the performing radiologist.
Primary outcomes
The primary outcomes included a comparison of procedure-related mortality (at 30 days and 90 days) between patients presenting with complicated and uncomplicated cholecystitis, as we hypothesized that performing PC in the latter would be considered higher risk.
Secondary outcomes
This included a review of other variables which may be associated with increased mortality in patients presenting with acute cholecystitis. These included:
Demographics (age, sex) Presence of gallstones Biochemical factors, such as C-reactive protein (CRP), white cell count (WCC), bilirubin, and acute kidney injury (AKI) Reintervention rates Duration of drain in situ
Data collection
The following patient information was collated for analysis: general demographics (age, sex, admission hospital, American Society of Anesthesiologists [ASA] score); relevant clinical details (date of admission, admission to intensive care, date of discharge, length of stay); preoperative biochemistry profile (CRP, WCC, highest lipase, highest amylase, bilirubin, diagnosis of AKI during admission, most recent estimated glomerular filtration rate [eGFR] before the procedure); details of radiological diagnosis (days from admission to imaging diagnosis, imaging modality, features of complicated cholecystitis); details of PC (indication, days from admission to cholecystostomy, access route, cholecystostomy tube size, technical success rate, procedure-related morbidity, duration of PC placement); readmissions (indication, length of stay, days from prior discharge to readmission, frequency); PC overall outcome (total number of PC procedures per patient, cholecystectomy, days from admission to cholecystectomy); and overall survival (30-day mortality, 90-day mortality, 180-day mortality, days lived after PC, date and cause of death).
Descriptive statistics are presented in the form of frequencies and percentages. A comparison of the outcome in the complicated and uncomplicated groups was carried out using the chi-square test or Fisher's exact test while a comparison of the survival in the two groups was done using the Log-rank test. Survival data are presented using Kaplan–Meier curves (Figs. 1–4), and the Cox proportional hazards model was used for the factors affecting survival. Unadjusted and adjusted hazard ratio (HR) is presented with the 95% confidence interval (CI). SPSS version 28 for windows software (IBM Corp., Armonk, NY, USA) was used for the analysis, and a P value <0.05 was considered statistically significant.
In total, 100 patients (47 men, 53 women; 47 patients were aged ≥80 years) with acute cholecystitis who underwent PC were included in this study. Of them, 34 cases were uncomplicated and 66 were complicated.
Results
Data statistics were presented in the form of frequencies and percentages (Tables 1–5). The technical success rate was 100% and there were no major procedure-related complications. A total of 12 patients had reintervention. The 30-day mortality rate was 9%, and the 90-day mortality rate was 11%. After six months, 84 patients were alive of a total of 97 patients whose data were available.
Characteristics of the study sample (n = 100).
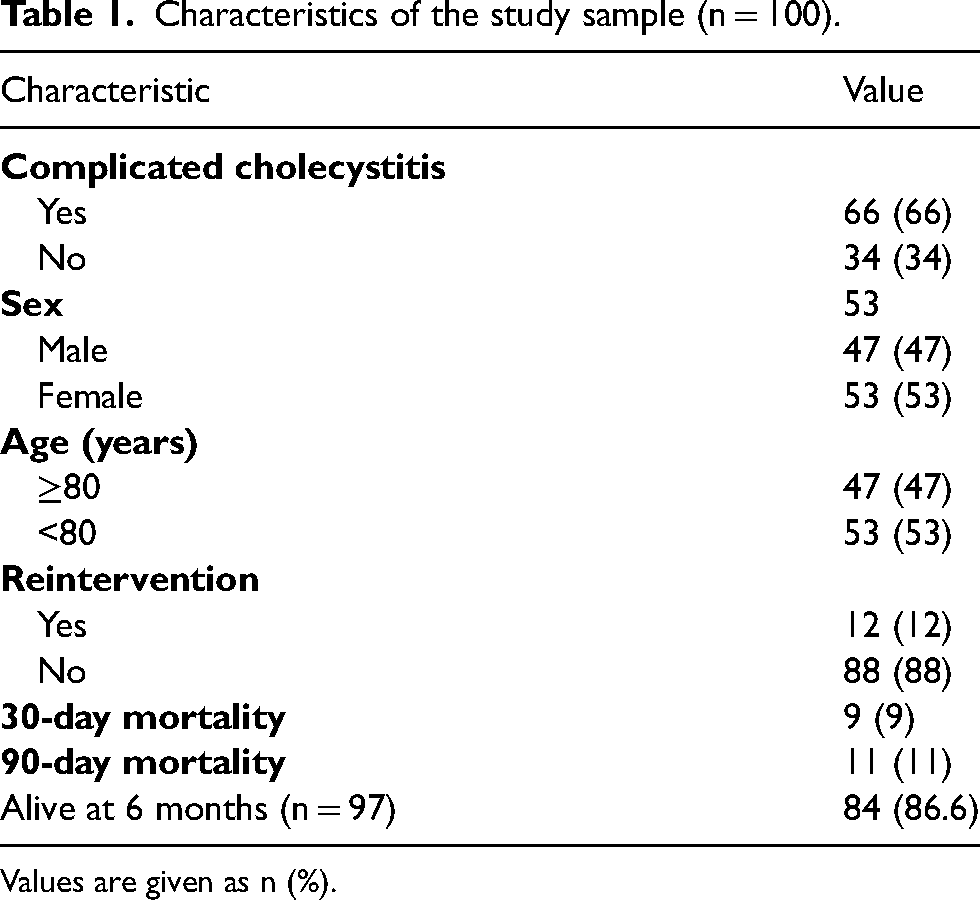
Values are given as n (%).
Comparison of the outcome between complicated and uncomplicated cases of cholecystitis.

Values are given as n (%).
Comparison of the survival time between complicated and uncomplicated cases (based on 30 days of follow-up).
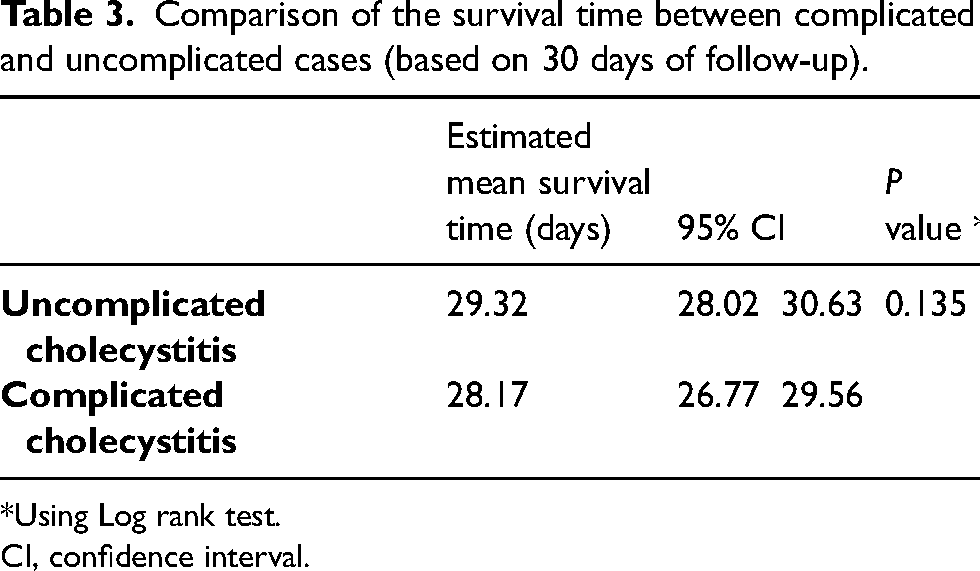
*Using Log rank test.
CI, confidence interval.
Cox proportional hazards model for the factors affecting survival (30 days of follow-up).
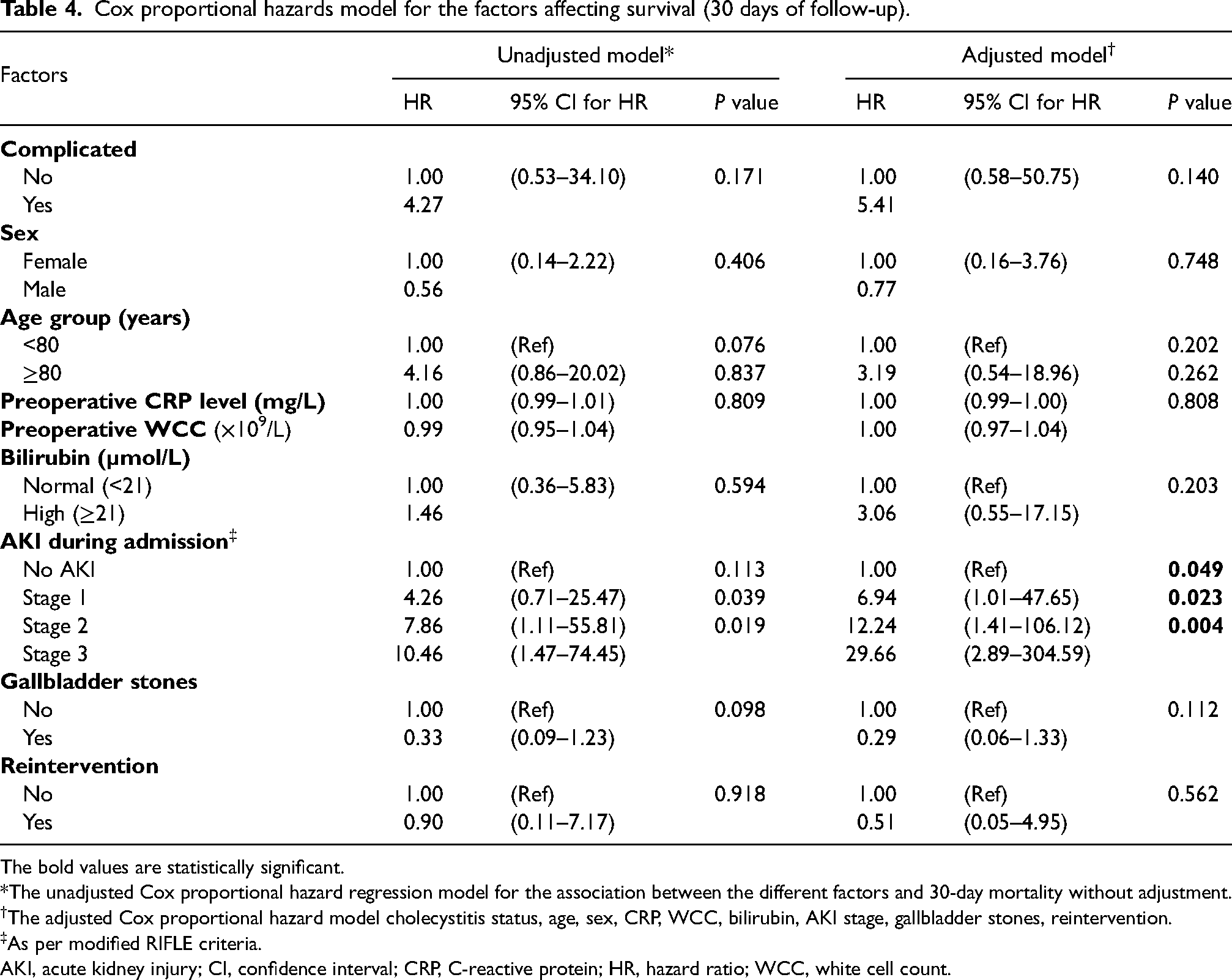
The bold values are statistically significant.
*The unadjusted Cox proportional hazard regression model for the association between the different factors and 30-day mortality without adjustment.
The adjusted Cox proportional hazard model cholecystitis status, age, sex, CRP, WCC, bilirubin, AKI stage, gallbladder stones, reintervention.
As per modified RIFLE criteria.
AKI, acute kidney injury; CI, confidence interval; CRP, C-reactive protein; HR, hazard ratio; WCC, white cell count.
Logistic regression model of predictors of six-month survival.
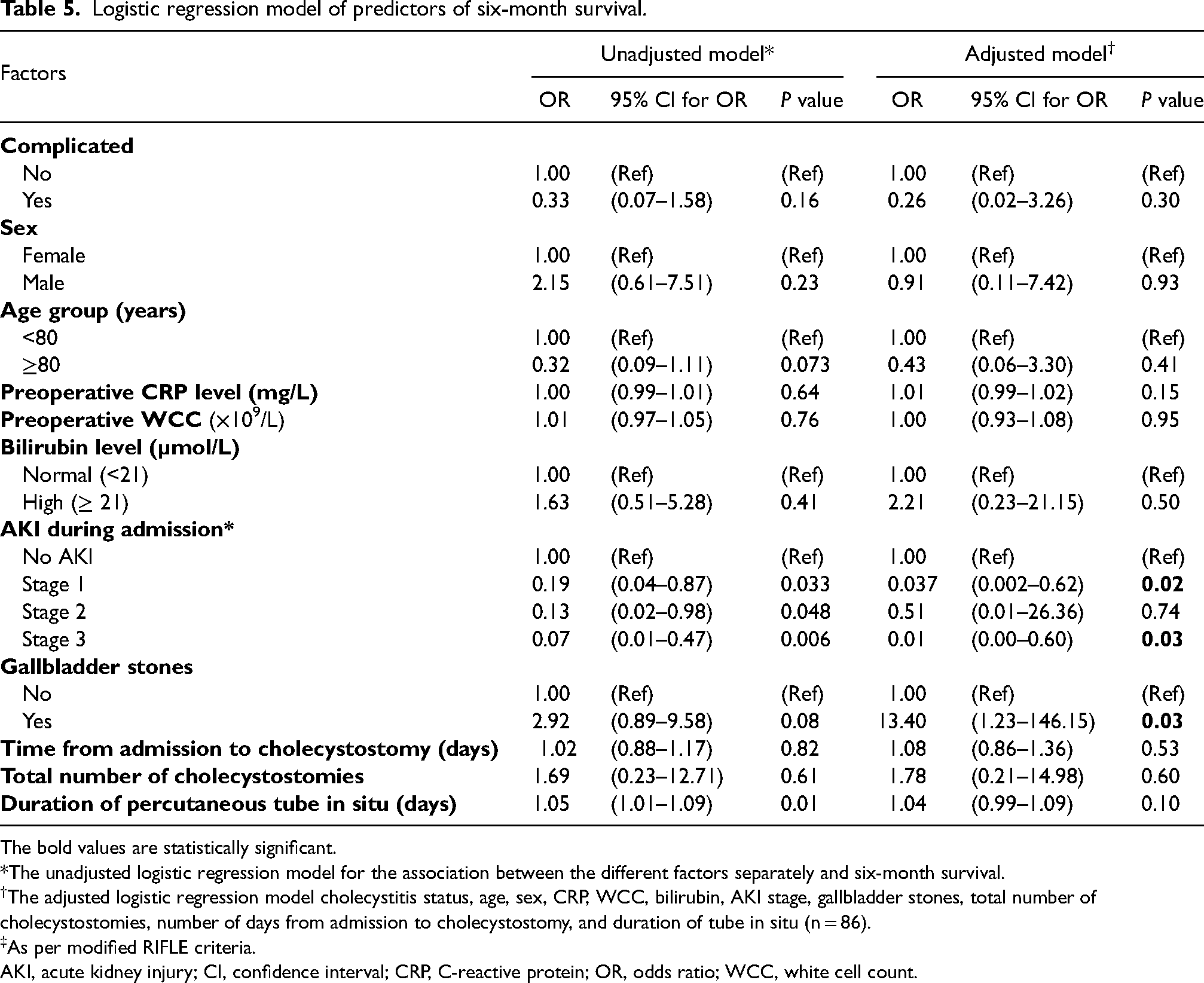
The bold values are statistically significant.
*The unadjusted logistic regression model for the association between the different factors separately and six-month survival.
The adjusted logistic regression model cholecystitis status, age, sex, CRP, WCC, bilirubin, AKI stage, gallbladder stones, total number of cholecystostomies, number of days from admission to cholecystostomy, and duration of tube in situ (n = 86).
As per modified RIFLE criteria.
AKI, acute kidney injury; CI, confidence interval; CRP, C-reactive protein; OR, odds ratio; WCC, white cell count.
The outcome, in the form of 30-day mortality, 90-day mortality, being alive after six months, and reintervention, was compared between the complicated and uncomplicated cases using the chi-square test or Fisher's exact test. There was no statistically significant difference in any of the compared outcomes.
A comparison of the survival time between complicated and uncomplicated cases (based on 30 days of follow-up) was carried out using a log-rank test and the survival data are presented using the Kaplan–Meier curve, as presented in Fig. 1. There was no statistically significant difference in survival between the complicated and uncomplicated groups.
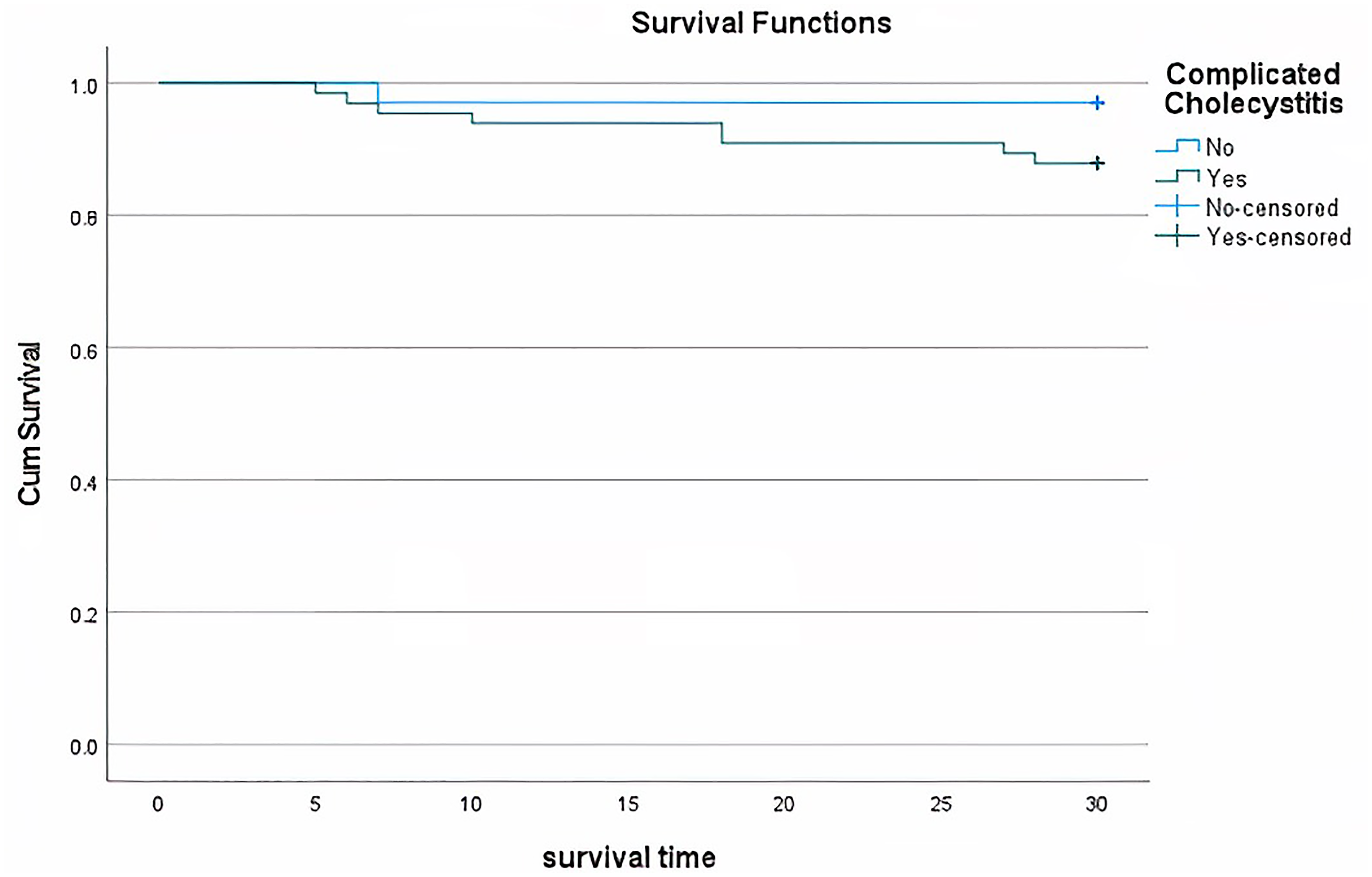
Kaplan–Meier curve for survival in the complicated and uncomplicated cases (based on 30 days of follow up).
The Cox proportional hazards model was used to study the factors affecting survival (30-day follow-up). Univariate and multivariable models are presented using the HR with a 95% CI (Table 4).
The only variable that showed a statistically significant association with the risk of mortality was AKI at admission (as per modified RIFLE criteria). Patients who had stage 1, 2, or 3 AKI had a higher hazard for mortality compared to patients with no kidney disease. For patients with stage 1, HR was 6.94 (95% CI = 1.01–47.65, P = 0.049); for stage 2, HR was 12.24 (95% CI = 1.41–106.12, P = 0.023; and for patients with stage 3, HR was 29.66 (95% CI = 2.89–304.59, P = 0.004) (Fig. 2).
There was no statistically significant difference in hazard of 30-day mortality between complicated and uncomplicated cases (P = 0.094), between patients who required and did not require reintervention (Fig. 3), or between patients aged <80 years and those aged ≥80 years (P = 0.117) (Fig. 4).
The presence of gallbladder stones showed no statistically significant association in hazard of 30-day mortality (P = 0.112).
A binary logistic regression model was conducted. An unadjusted model was used to assess each possible factor separately without adjustments and the effect on six-month survival.
The unadjusted model (Table 5) showed that most factors were insignificant in predicting survival at six months, apart from AKI stage 1 (P = 0.033), stage 2 (P = 0.048), stage 3 (P = 0.006), and duration of the tube in situ (P = 0.01).
Furthermore, a multiple regression model adjusting for age, sex, CRP, WCC, bilirubin, AKI stage, gallbladder stones, the total number of cholecystostomies, number of days from admission to cholecystostomy, and duration of tube in situ with different possible predictors was performed.
The fit of the model was assessed using the Hosmer and Lemeshow test (P = 0.94) and receiver operating characteristic (ROC) curve analysis (area under the ROC curve [AUC] = 0.93). The adjusted model shows that having AKI before having a cholecystostomy, specifically stage 1 (P = 0.02) and stage 3 (P = 0.03), is statistically different from not having any AKI in six-month survival after cholecystostomy. In addition, there is another statistically significant difference in six-month survival between calculus and calculus cholecystitis (P = 0.03). Furthermore, the statistically significant association of the duration of the drain in situ is mitigated when an adjusted model is used to assess the effect on six-month survival.
Patients with AKI stage 1 are nearly 97% less likely to survive after six months in comparison to patients without AKI (odds ratio [OR] = 0.037, 95% CI = 0.002–0.62), adjusted for the mentioned variables. Patients with AKI stage 3 are 99% less likely to survive after six months in comparison to patients without AKI (OR = 0.01, 95% CI = <0.001–0.60), adjusted for the mentioned variables.
Patients with calculus cholecystitis are 13-fold more likely to survive after six months in comparison to patients with acalculous cholecystitis (OR = 13.40, 95% CI = 1.23–146.15), adjusted for the mentioned variables. The 95% CI for these ORs comparing stage 1 and 3 AKI versus no AKI in patients with acute cholecystitis, and patients with calculus versus those with acalculous cholecystitis is very wide (Table 5). This is explained by the small sample size. Thus, this association should be interpreted with caution.
While the OR is statistically significant, the 95% CI suggests that the magnitude of the effect could be anywhere between very large intervals. A larger study is needed to generate a more precise estimate of the effect.
Discussion
Acute cholecystitis is a common condition and can be complicated by perforation, gangrene of the gallbladder, hepatic abscess, and bilomas. PC is an effective procedure for temporizing patients who are acutely unwell and can provide a more permanent therapeutic option for those who remain unfit for surgery. The concern is whether performing PC in patients with complicated features is associated with higher mortality in comparison with uncomplicated cases. Our study demonstrates that there is no significance in mortality between the two groups, an important statistic to appreciate when decision-making for treatment. This is important given that many patients are unstable when presenting on admission and performing emergency surgery can be associated with higher mortality (9).
We have also demonstrated that there are no significant differences in survival outcomes when considering demographic (age, sex) and biochemical factors (CRP, WCC, bilirubin).
The study has, however, highlighted the significance of appreciating and correcting AKI on admission, as this has been demonstrated to be a significant independent predictor for mortality in patients presenting with acute cholecystitis. Most of these patients are unwell and dehydrated on admission due to sepsis, which is a risk factor for developing AKI. The association of AKI with high mortality in patients with acute cholangitis has been recently published as an independent predictor for mortality, highlighting the importance of early recognition and treatment (10). However, there is a paucity of data demonstrating this in patients with acute cholecystitis undergoing PC. This would be of critical value to interventional radiologists and treating teams since this highlighted that AKI is a single predictor of mortality, and therefore appropriately treating these patients with intravenous fluids and antibiotics before being intervened on is crucial.
The presence of gallstones, although associated with statistically significant results, demonstrates a very wide CI, and therefore needs to be interpreted with caution. This would be in line consistent with the Tokyo guidelines suggesting lower mortality in patients with calculous cholecystitis as opposed to acalculous cholecystitis. A recent paper comparing the mortality in patients with calculous cholecystitis in patients who underwent operative treatment versus non-operative treatment (antibiotic therapy and PC) demonstrated the contrary. Interestingly, when the two groups were pair-matched for identical severity, there was no statistically significant difference between the two groups (11).
The duration of the tube being in situ has shown to be associated with poorer outcomes; however, this effect is mitigated when adjusted for other variables. It is not surprising that patients with prolonged drains in situ experience recurrent episodes of gallstone-related symptoms, tube dislodgement, tube blockade, or bile leakage. However, this has not been associated with high mortality in patients who are not suitable for surgery and require long-term indwelling drains (12). Emphasis should therefore be placed on appropriate tube management in this cohort as most of these patients are not even suitable for surgical management even after stabilization with percutaneous drainage. Cholecystolithotomy has also been described as an effective long-term alternative in patients with gallstone disease in whom surgery is not appropriate (13).
The present study has some limitations. These include its small sample size and its retrospective nature. The results have, however, provided us with better insights into the risk stratification and management of these patients. We did not compare the differences between PC and surgical cholecystectomy in acutely unwell and high-risk patients as this has been reported, commented on, and was not the objective of our study (14,15). Hung et al. described the interval management of drains until the subsequent and more definitive management with surgery (12). Their paper highlights practices that have not yet been standardized and may form the basis of future studies. Hatzidakis et al. describes interventional techniques (such as stenting and lithotripsy) through the cystic duct via existing percutaneous gallbladder drains as a safe and effective option with low complication rates (16). Long-term data or even larger pooled data is, however, lacking; from our perspective, we feel that larger studies comparing drains that have been internalized versus those that remain external would be of clinical interest to interventional radiologists. Internalization may also prove to be a better long-term option for cost mitigation as the management of recurrent biliary events in patients with long-term drains in situ has been described to be associated with higher costs (17).
In conclusion, our results demonstrate that PC is a safe and effective procedure, particularly in patients who are too unwell to receive definitive surgical treatment. Mortality is not affected by the presence of complications, contrary to what we thought when conducting this study. The results have, however, highlighted the importance of recognizing and treating AKI, an independent risk factor affecting mortality. Further, larger studies would be recommended to better assess the long-term outcomes of these two cohorts.

Kaplan–Meier curve for survival in patients with different stages of AKI (based on 30 days of follow-up).

Kaplan–Meier curve for survival in cases with reintervention and without reintervention (based on 30 days of follow-up).
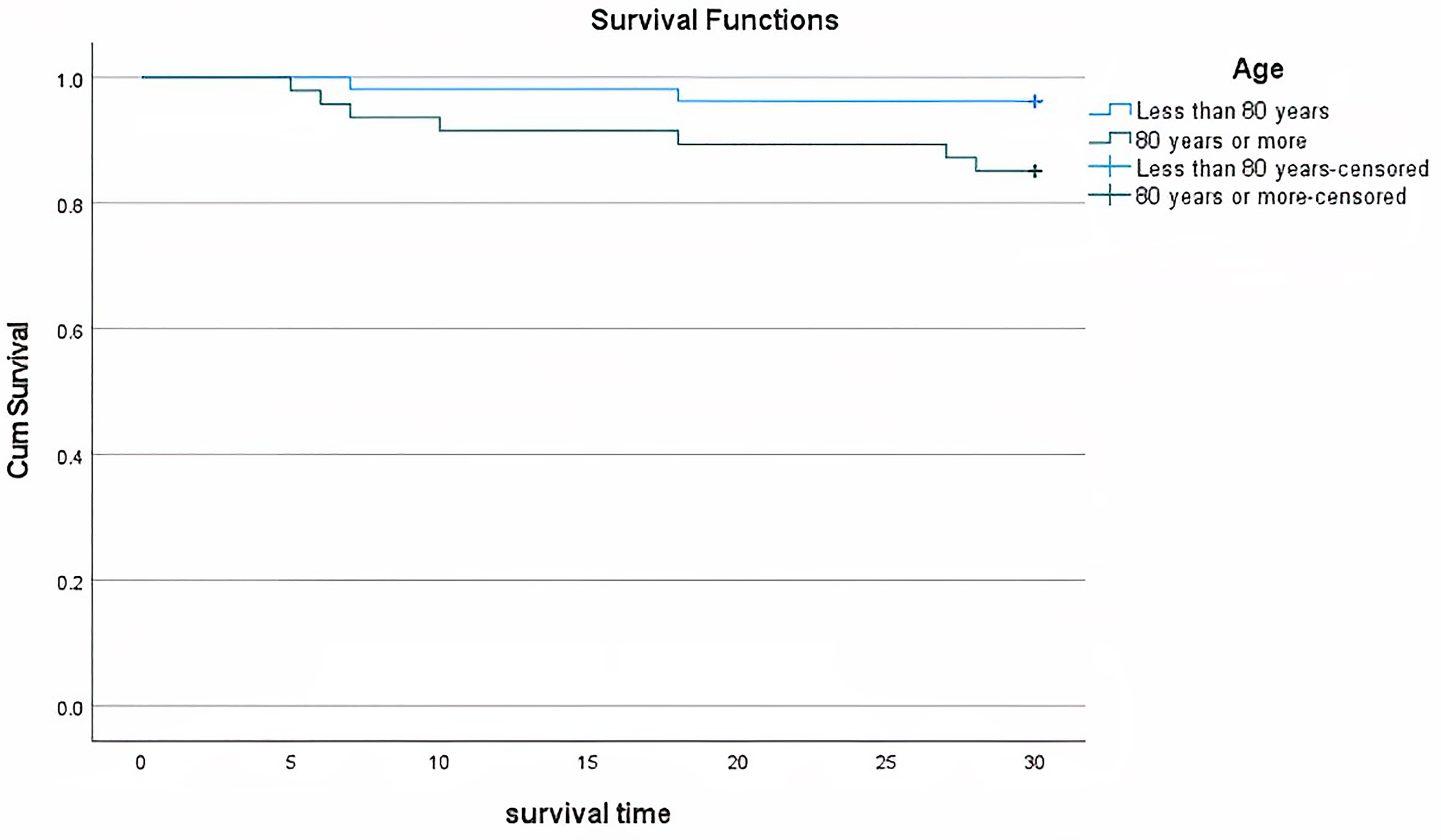
Kaplan–Meier curve for survival in the cases of different age groups (based on 30 days of follow-up).
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.