
Abstract
Background
Fracture healing complications remain a major problem in trauma monitoring. An open wedge osteotomy of the distal radius provides a unique way of evaluating fracture healing. Since the introduction of cone-beam computed tomography (CBCT) at our institution, it has become the method of choice for assessing hand and wrist bones. To date, CT volumetry has been validated for multidetector CT (MDCT) but not for CBCT.
Purpose
To assess osteotomy healing using CBCT volumetry and to evaluate two different segmentation techniques.
Material and Methods
A total of 36 patients were surgically treated for malunited distal radius fractures with open-wedge osteotomy either leaving the void empty (open wedge empty [OWE]) or filled with bone graft substitutes (BGS). They were scanned using CBCT and MDCT postoperatively and after 3, 6, and 12 months. Segmentation was performed both manually and semi-automatically for volumetric measurement. Inter- and intra-observer reliability were assessed using intraclass correlation (ICC).
Results
The median osteotomy volume in the OWE group postoperatively was 0.87 cm3 (range=0.42–2.72). At 3 months, all but one of the OWE volumes had diminished to half or less of their initial volume. In the BGS group, the median postoperative volume was 1.30 cm3 (range=0.73–1.81) and at 12 months, 76% of the initial volume remained. Reliability between CBCT and MDCT volumetry expressed as ICC was ≥0.96. ICC for the two segmentation techniques was ≥0.99 and ICC for inter-observer reliability ≥0.97.
Conclusion
CBCT volumetry is a reliable tool and comparable to MDCT to quantify bone healing of an osteotomy.
Keywords
Introduction
Common complications after a fracture include delayed or impaired healing, which are seen in approximately 10% of all fractures (1). To enable early detection of healing complications, it is important to establish non-invasive ways to evaluate bone healing, so patients who need intervention might be identified (2,3).
A combination of conventional radiography (CR) and clinical assessment of function and stability remain standard practice (4) for the assessment of fracture healing, even though new imaging tools have been developed in recent decades. Other methods, such as measuring bone mineralization, computational techniques measuring bridging callus in conventional CR, quantification of optical density (OD) dual X-ray absorptiometry, and ultrasonography, have been proposed (2,3,5,6). High-resolution peripheral quantitative computed tomography (HR-pQCT) giving ultrathin tomographic CT slices was recently used to analyze the fracture healing process in patients with distal radius fracture (7). Multidisciplinary CT (MDCT) volumetry has been shown to be a promising tool monitoring bone healing in a pig model study (1,8,9); however, to the best of our knowledge, there is no clinical study using this technique.
Cone-beam CT (CBCT) is a CT technique comprising a cone-shaped X-ray beam and a digital flat panel detector, collecting all data for image reconstruction in one single gantry rotation (10). CBCT has been shown to be useful for the imaging of extremities (11–13). The benefits of CBCT compared to MDCT include higher patient comfort, shorter imaging procedure, higher spatial resolution, and lower radiation doses (14,15).
Since the introduction of CBCT at our institution in 2013, it has become the imaging modality of choice for the visualization of the skeleton of wrists, hands, ankles, and feet, concerning the upper extremity – especially intra-articular wrist fractures, scaphoid fractures, or other complex hand or wrist trauma. This was an important background to why we wanted to investigate the possibility of evaluating the process of wrist osteotomy healing in the distal radius using this method. Most studies that useMDCT to assess callus formation rely on the fact that tissue density might be measured in calibrated HU values. This was not possible with the CBCT technique as the images are not being calibrated, nor is there any way to obtain a calibration due to the different tomographic technique in CBCT. Instead, all images produced were interpreted using Syngovia software (Siemens, Erlangen, Germany). The software provided us with artificial HU values according to the relative grayscale in the image, which is related to the X-ray attenuation of the tissue concerned (16,17). In addition, we have chosen CT volumetry as it has been used in an in-vivo MDCT pig-model study. It was shown to be a promising tool for monitoring bone healing (1); however, to the best of our knowledge, there has been no clinical study using this technique on humans.
The use of a controlled osteotomy in an otherwise uninjured patient and utilization of a radiolucent PolyEther Ether ketone (PEEK) plate offers a unique method of quantitating bone healing in vivo on CBCT or MDCT scans, by measuring osteotomy volumes over time using imaging software for 3D reading.
The main aim of the present study was to assess the possibility of using CBCT for evaluating volume reduction of the osteotomy gap as a tool for assessing osteotomy healing and investigate the reliability of volumetry of CBCT by comparing it to MDCT, which is regarded as the reference method in our study (8,9). Another purpose was to evaluate two different segmentation techniques for volumetry – manual and semi-automatic – using threshold values of density.
Material and Methods
Patient characteristics
This study of osteotomy healing was carried out on 36 consecutive patients, all included between December 2014 and May 2018 in a randomized controlled study (RCT) designed to compare the functional outcomes of patients undergoing corrective osteotomy for malunited distal radius fractures with two different surgical techniques (18). From this cohort, 25 patients are also included in two qualitative studies of wrist disability after distal radius fracture and one patient is included in a cross-sectional long-term follow-up study (18–20).
An open wedge correction osteotomy was performed through a dorsal approach and fixation of the wrist was made through a conventional volar approach by attaching a radiolucent plate DiphosR, made of carbon fibers and PEEK (Lima Corp., Udine, Italy). The patient was randomized during surgery to either have the dorsal void filled with a bone graft substitute (BGS) (HydroSet; Stryker Leibinger GmbH& Co. KG, Freiburg, Germany) or leaving the open wedge empty (OWE) (18).
Imaging of all included patients was performed using both CR, radio stereoscopic assessment (RSA), and CBCT at four time points during the trial: immediately postoperatively and after 3, 6, and 12 months.
A subgroup of 19 patients (16 women, 3 men) also had MDCT at the same day as CBCT. In this group, there were 10 individuals from the BGS group and nine from the OWE group.
CR was the standard follow-up procedure during the study and was undertaken to assess the overall osteotomy healing process, the positioning of screws and the carbon-fiber plate, and to check for possible complications. Results from the RSA are to be published separately.
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee in Gothenburg, Sweden (no. 472-14) and registered in a local register at Sahlgrenska Hospital (no. 29934). All participants gave informed, written consent.
Data collection
CBCT was conducted with an extremity CBCT unit (Planmed Verity; Planmed Oy, Helsinki, Finland) with the following exposure parameters: 90 kV; tube current = 6 mAs; tube load = 36 mAs; pixel size = 0.25 mm; slice thickness = 0.25 mm; and field of view (FOV) = 13 cm in the proximal-distal direction. One series consists of 300 exposures, each taking 20 ms. Reconstructions were made in three planes relative to the radius (axial, coronal, and sagittal) with a slice thickness of 0.25 mm.
The MDCT was conducted with a Discovery CT 750 (GE Healthcare, Milwaukee WI, USA) with the following exposure parameters: tube voltage = 100 kV; tube current = 80 mA; pitch = 0.53; rotation time = 0.8 s; ASIR VS 40% head filter; kernel HD Boneplus2 HiRes; matrix = 512 × 512; and slice thickness = 0.625 mm. Reconstructions were made in three orthogonal planes with a slice thickness of 1.0 mm.
Volume measurements
The MDCT and CBCT images were analyzed using Syngovia (Siemens, Erlangen, Germany) image processing software, which allowed multiplanar reformation (MPR) to obtain orthogonal projections of the postoperative deformity, such as axial, sagittal, and transversal planes of the operated wrist (Figs. 1 and 2). The acquired data consisted of a stack of approximately 200 axial images and the sagittal plane used for segmentation with a skeletal windowing of 450–1500 Hounsfield units (HU).
Two methods for volume estimation of the osteotomy were investigated, i.e. manual segmentation and semi-automatic segmentation. All images were analyzed blindly regarding clinical outcome by three observers, all being senior radiology residents (observers 1, 2, and 3). Intra-observer observations were made after an interval of at least 2 weeks.
In the manual segmentation, the radiologist outlined the area of interest on every single slice based upon visual inspection on the sagittal plane. When the segmentation was completed, the slices were summarized, which made the lines editable and gave them a green color (Fig. 3). Refinements of the segmentation were carried out using the axial and coronal planes.

Cone-beam computed tomography images of the same patient after open wedge corrective osteotomy was performed, leaving the void empty (arrow): (a) immediate postoperatively and (b) 3 months, (c) 6 months, and (d) 12 months postoperatively.

Cone-beam computed tomography images of the same patient after open wedge corrective osteotomy was performed, filled with bone graft substitute (arrow): (a) immediate postoperatively and (b) 3 months, (c) 6 months, and (d) 12 months postoperatively.
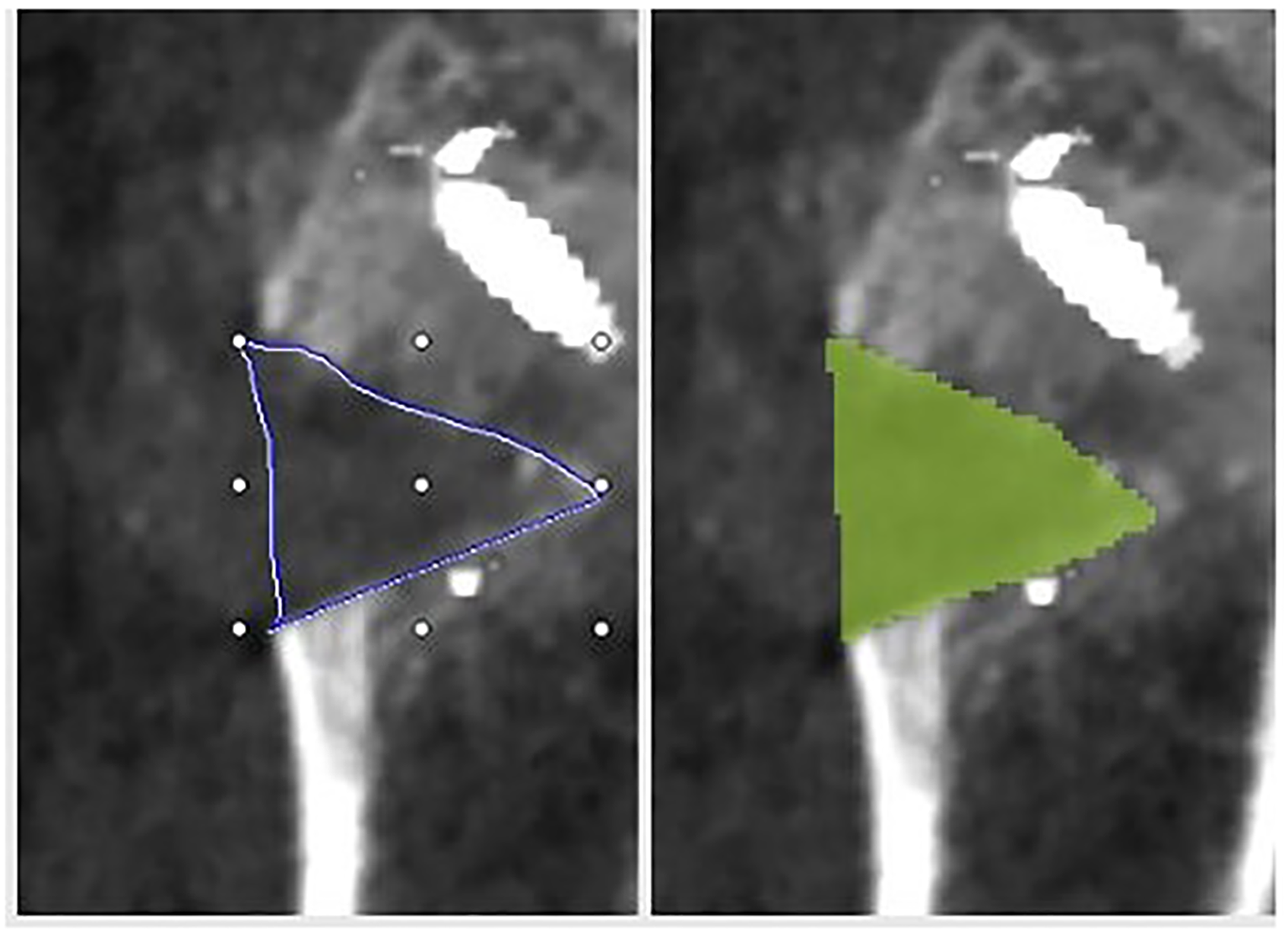
Manual segmentation of wedge-shaped osteotomy using “FreeHand MPR”: (a) manual outlining of the section area; (b) automatic calculation of the slice area.
The semi-automatic segmentation was performed using threshold values of density. The software allowed setting an upper and lower threshold of the HU values within the marked area to decrease error calculations from artefacts or unwanted objects, such as screws or fat. In CBCT, the HU values were artificial based on the relative grayscale in the image. In patients with empty void osteotomies, the highest threshold was set to 400 HU to prevent native bone and bone formation being calculated into the segmentation. In patients who had BGS osteotomy, the lowest threshold was set to 1000 HU because that would ensure only the bone graft being included and not native bone. No upper or lower HU value were defined. With the semi-automatic method, the section area was outlined and accepted by the observer on every 3rd– 5th slice and the in-between slices were interpolated by the software (Fig. 4). The segmentation time was considerably faster in the semi-automatic method. However, each slice was still assessed by the observer to detect various errors and reduce artefacts. Once segmentation was complete using either of the two methods, data were recorded and manually inserted into Excel (365) for Windows (Microsoft Corp., Redmond, WA, USA).
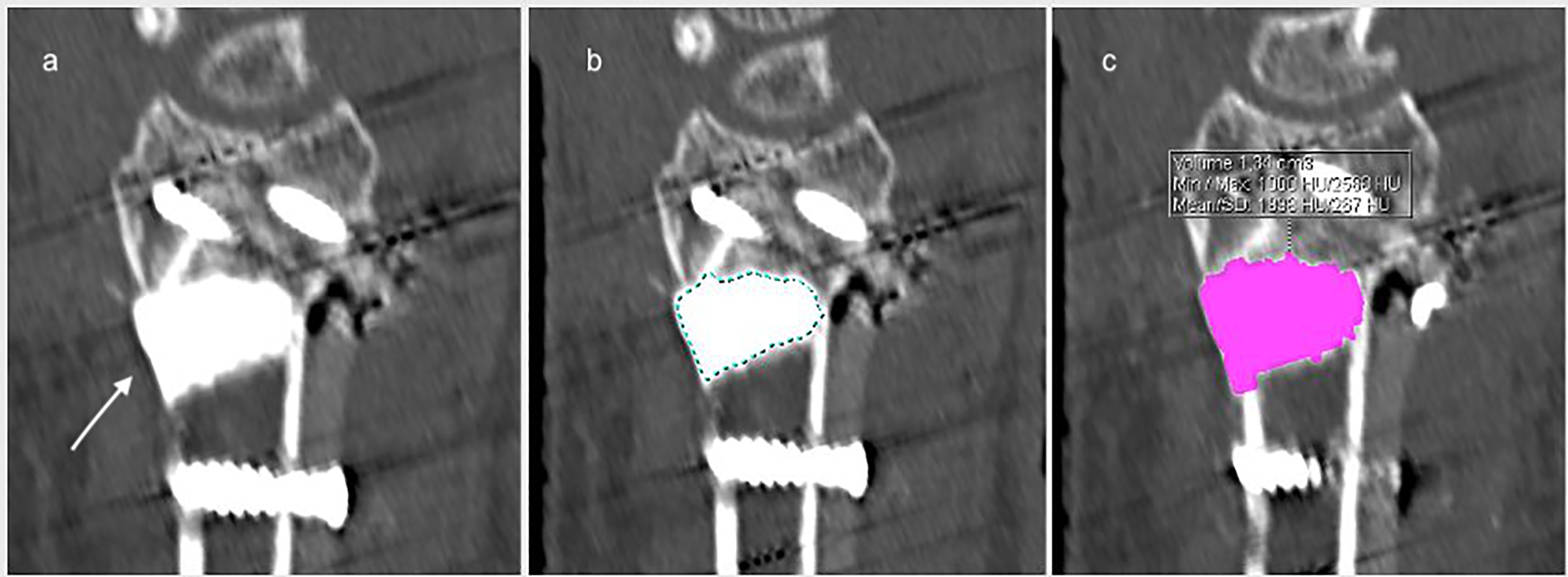
Semi-automatic segmentation of a wedge-shaped osteotomy filled with bone graft substitute (arrow) (a) before drawing, (b) threshold outlining of the section area, (c) automatic calculated area.
Estimated radiation doses
The effective dose for one investigation was calculated to be 2 µSv for MDCT and 0.2 µSv for CBCT.
Reliability measurements
All CBCT investigations were assessed using both the manual and semi-automatic methods, by two different observers (observers 1 and 2), one of whom also assessed MDCT using the semi-automatic method. To evaluate inter-observer reliability for CBCT, five patients in each subgroup were assessed twice using the semi-automatic method (observers 2 and 3) (Table 1).
Patients investigated using CBCT and MDCT and measuring performed by three observers (observers 1, 2, and 3).

Values are given as n.
BGS, bone graft substitute; CBCT, cone-beam computed tomography; MDCT, multidetector computed tomography; OWE, open wedge empty.
Statistics
All statistical analyses were performed using commercially available software (SPSS version 25.0; IBM Corp., Armonk, NY, USA). Shapiro–Wilk's test for normal distribution was used to determine whether the variables were normally distributed, and results are presented as mean ± SD for normally distributed variables and median (range) for those with a non-parametric distribution. Due to small subgroups, non-parametric tests were used for tests of hypothesis. The Mann–Whitney U-test was used for comparisons between groups. Correlations were assessed using Spearman's rank order test. The intraclass correlation coefficient (ICC) was used to assess intra-and inter-rater reliability using ICC Model 3, type 1, in which each subject is assessed by each rater and reliability is calculated from one single measurement (two-way mixed effects, consistency, single measurements). All significance tests were two-tailed and P < 0.05 was considered statistically significant.
Results
Of the original 38 patients, two study participants, both from the BGS group, declined participating in the postoperative follow-up imaging scheme. Thus, patient data were assessed for 19 patients (4 men, 15 women; median age = 65 years; age range = 24–68 years) for the OWE group and 17 patients (5 men, 12 women; median age = 60 years; age range = 22–80 years) for the BGS group.
CBCT images were obtained from all 36 patients (9 men, 27 women; median age = 64 years; age range = 22–80 years). The median age of the 19 patients (3 men, 16 women) undergoing both CBCT and MDCT was 65 years (age range = 49–80 years). There were 10 patients in the OWE subgroup (1 man, 9 women; median age = 66 years; age range = 49–67 years) and nine patients in the BGS subgroup (2 men, 7 women; median age = 64 years; age range = 52–80 years) undergoing both CBCT and MDCT.
CR showed no complications in any of the included patients.
Reliability
The reliability, expressed as ICC, for the two different segmentation techniques, the two modalities used for imaging (MDCT and CBCT), and for the repeatability of the CBCT volumetry using threshold technique are presented in Table 2.
Reliability for the two segmentation techniques, the two modalities (MDCT and CBCT), and for repeatability of the threshold segmentations, expressed as ICC.
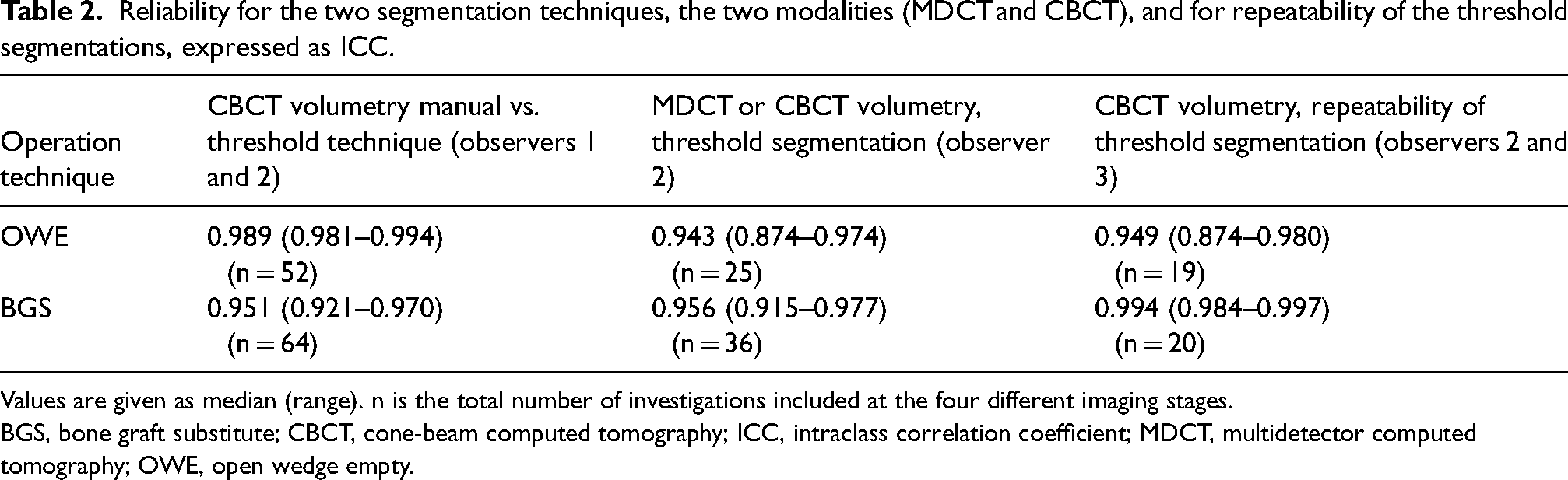
Values are given as median (range). n is the total number of investigations included at the four different imaging stages.
BGS, bone graft substitute; CBCT, cone-beam computed tomography; ICC, intraclass correlation coefficient; MDCT, multidetector computed tomography; OWE, open wedge empty.
Volumes
The CBCT osteotomy volumes at the first postoperative measurement were significantly larger in the BGS group compared to the OWE group. For each time interval, there was a significant decrease of volume in both treatment groups.
In the OWE group, the median osteotomy volume was 0.87 cm3 (range = 0.42–2.72 cm3) immediately postoperatively and 0.23 cm3 (range = 0.23–0.75 cm3) at 3 months. At 3 months, all but one of the OWE volumes had diminished to half or less than half of the initial void volume. At 6 months, four of the OWE voids were totally filled with new bone, and at 12 months, 12 of 19 osteotomy voids were fully consolidated.
In the BGS group, the median postoperative volume was 1.30 cm3 (range = 0.73–1.81 cm3). The decline in volume was small throughout the follow-up period and had at 12 months reached 76% of the initial volume (Table 3). All volume measurements assessed with CBCT and MDCT using manual as well as semi-automatic segmentation for OWE osteotomy at four occasions during the first postoperative year are presented in Supplementary Table 4.
Volume assessed by CBCT for OWE osteotomy and BSG at four occasions during the first postoperative year.
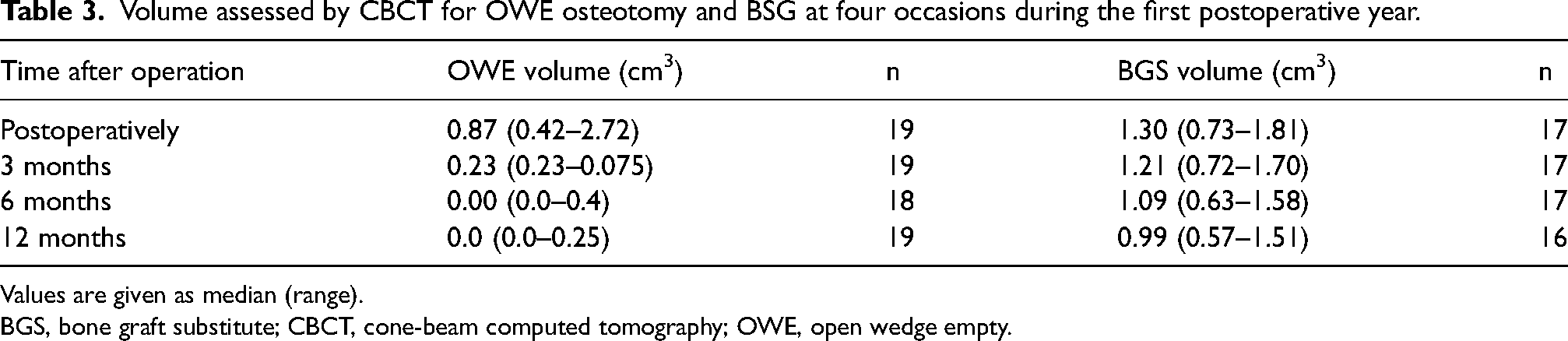
Values are given as median (range).
BGS, bone graft substitute; CBCT, cone-beam computed tomography; OWE, open wedge empty.
Discussion
Our results show that quantitative volume assessment of bone defect healing of an osteotomy can be measured with excellent repeatability using both MDCT and CBCT with the segmentation technique relying on the difference in tissue density between mineralized bone and non-osseous tissue in the osteotomy void. To the best of our knowledge, MDCT volumetry for measuring bone healing has to date only been applied in a pig model (1). This showed an excellent correlation for MDCT volumetry in bone defect healing and histomorphometry, using the same commercially available software program (Syngo Volume; Siemens, Germany) as in our study. We wanted to investigate if the segmentation technique was applicable both when the void was left empty and when bone graft substitute was used, as this represents entirely different spectra of densities. The defect was measured directly postoperatively, and the decrease in volume after 3, 6 and 12 months later was regarded as the actual volume of consolidated osseous tissue. This allowed us to use only one threshold in each group, i.e. ≤400 HU was set as the highest threshold for OWE and ≥1000 HU as the lowest for BGS patients, in contrast to Rigger et al., who measured the new bone formation using a lower and an upper threshold (1).
Our results show that the semi-automatic tool for the segmentation of volumes in MDCT was as reliable as the manual method. This has been shown for lung nodules (21) and bone cysts (8,9), but not, as far as we know, for bone healing volumes. Manual segmentation is time-consuming, laborious, and requires skilled users as it depends on manually drawing the complex boundaries of the structures. The semi-automatic method was much quicker, taking about a few minutes per volume compared to approximately 10–15 min for the manual technique. Precise time measurement was not included in this study.
The non-calibrated artificial densities, provided by the Syngovia software, for CBCT were shown to be as reliable as MDCT in defining callus from non-osseous tissue or bone graft substitute. Using this volumetry technique, there was no need to match the subsequent scanning as is necessary if a chosen ROI is to be analyzed and compared over time (7,22).
The radius PEEK plate is radiolucent, and thus the only metal artefacts encountered were from the titanium screws of the plate, which in no case disturbed the volume measurements. The scanning time for both MDCT and CBCT were relatively short, about 30–36 s, and no motion artifacts were seen. This makes it possible to include the whole volume of the osteotomy void in contrast to HRpQCT, which is a method restricted to a short scan length and has a considerably longer scanning time (7).
One advantage of using CBCT instead of MDCT while monitoring extremity fracture healing is the lower radiation dose. The advent of new low-dose protocols for MDCT reduces the difference in irradiation between the two methods; however, in a recently published paper (15), the effective dose of CBCT of the wrist is estimated to be 0.7–2-4-fold compared to one exposure with a CR device while MDCT showed an 8.6-fold effective dose. CBCT is more practical for the patients owing to its ability to examine an extremity in a sitting position. In addition, CBCT is performed with a smaller, cheaper machine than MDCT and can therefore be more efficient in terms of price and storage.
The present study has some limitations. First, there were no cases with delayed healing or non-union in the study group, indicating that the method of osteosynthesis outweighed any difference in fracture healing time between the two treatment groups. Further on, the callus formation in the BGS group could not be radiologically evaluated as the bone graft substitute resorbed slowly, thus obscuring the osseous filling of the void. However, this group was included to assure the segmentation technique could be applied even with densities in the higher field. In addition, the HU values measuring volumetry in the CBCT group were artificial by using the software program Syngovia. Finally, the sample size was small and the measurement time between the two methods of measuring was not recorded.
In conclusion, CBCT volumetry of bone defect healing is a new method for monitoring osteotomy healing in vivo with high repeatability. CBCT is cheaper, smaller, and uses less radiation compared to conventional MDCT. The method is easy to apply in a regular clinical setting and might be a tool for monitoring bone healing in osteotomies and, in future, bone lengthening and other conditions where there is a bone defect.
Supplemental Material
sj-docx-1-acr-10.1177_02841851241287903 - Supplemental material for Cone-beam CT volumetry: a new method for evaluating osteotomy healing – a clinical evaluation and MDCT comparison
Supplemental material, sj-docx-1-acr-10.1177_02841851241287903 for Cone-beam CT volumetry: a new method for evaluating osteotomy healing – a clinical evaluation and MDCT comparison by Ivan Cetinic, Michael Ullman, Linn Hellman and Ylva Aurell in Acta Radiologica
Footnotes
Acknowledgments
We thank Ayad Abbas for performing the manual segmentations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Local Research and Development Board of Gothenburg and Södra Bohuslän (no: VGFOUGSB-512721) and by Sahlgrenska University Hospital and the University of Gothenburg, Sweden.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.