
Abstract
Background
AngioJet rheolytic thrombectomy is associated with a higher risk of acute kidney injury due to its potential for inducing mechanical harm and intravascular hemolysis. However, previous studies have focused on a single disease entity.
Purpose
To identify predictors associated with acute kidney injury after AngioJet rheolytic thrombectomy across a range of disease entities.
Material and Methods
A total of 95 patients who underwent AngioJet rheolytic thrombectomy between October 2018 and April 2023 were retrospectively reviewed. In total, 11 patients were excluded due to the absence of a postprocedural serum creatinine test within 72 h; finally, 84 patients were included. Acute kidney injury was defined as a ≥1.5-fold increase or ≥0.3 mg/dL rise in serum creatinine within 72 h after the procedure. Univariate and multivariate analysis were performed to identify risk factors for acute kidney injury.
Results
Technical and clinical success were achieved in all patients (84/84, 100%). Of the 84 patients (40 men [47.6%], 44 women [52.4%]; mean age = 67.2 ± 15.9 years), 15 (17.8%) had developed acute kidney injury. Multivariate analysis showed concurrent malignancy (odds ratio [OR] = 42.231, 95% confidence interval [CI] = 2.332–764.693; P = 0.011) and AngioJet rheolytic thrombectomy in arterial system (OR = 24.109, 95% CI = 1.319–440.551; P = 0.032) as statistically significant predictors of acute kidney injury.
Conclusions
AngioJet rheolytic thrombectomy is a potential risk for acute kidney injury. Concurrent malignancy and AngioJet rheolytic thrombectomy in the arterial system are independent predictors of acute kidney injury.
Introduction
AngioJet rheolytic thrombectomy (ART) has been widely used in recent years as a treatment for thrombosed vessels. The ART system (Boston Scientific, Marlborough, MA, USA) is a pharmacomechanical peripheral thrombectomy device that incorporates mechanical fragmentation, pharmacologic lysis, and rheolytic aspiration of clots. Compared to catheter-directed thrombolysis, ART presents itself as a more efficacious approach for early thrombus removal. It offers several advantages, including reduced treatment duration, diminished total volume of fibrinolytic agents required, shorter stays in both the intensive care unit and hospital setting, decreased hospital costs, and potentially lowered risks of bleeding complications. Moreover, ART shows its adaptability in treating both arterial and venous acute thrombotic syndromes (1–3).
However, it is important to take into consideration an inevitable disadvantage of ART – it carries a higher risk of acute kidney injury (AKI). High-pressure shear stress at the treatment site can induce mechanical harm to circulating red blood cells, leading to intravascular hemolysis. The majority of patients treated by ART manifest some degree of hematuria, which ranges from microscopic in urinalysis to macroscopic hematuria. It is generally regarded as a benign side effect. However, close consideration might be needed after the procedure, as the condition might not be harmless. It can be associated with acute hemolysis, which is known to contribute to AKI. Several previous studies have documented cases of AKI after ART, such as volume and duration of aspiration thrombectomy. A study by Tian et al (4) compared AKI and non-AKI groups with acute lower extremity deep vein thrombosis (DVT) and reported that there were many significant differences in demographic data between the two groups. Escobar et al (5) compared patients who had thrombotic syndrome treated by AngioJet and those treated by conventional catheter-directed thrombectomy and suggested open surgery and >10% drop in hematocrit as risk factors for AKI. However, to our knowledge, most previous studies did not identify the ART site and malignancy as risk factors. Therefore, the aim of the present study was to identify predictors associated with AKI after ART across a range of disease entities.
Material and Methods
Study design and patient selection
This retrospective study at a single tertiary institution was approved by the institutional review board. The requirement for informed consent from patients was waived. Between October 2018 and April 2023, all consecutive patients who underwent ART at our institution were included. A total of 11 patients were excluded due to the absence of a postprocedural serum creatinine (sCr) test. Finally, 84 patients were included in the study.
Procedure
We conducted two types of procedures on our patients, encompassing pharmaco-rheolytic thrombectomy (n = 76) and rheolytic thrombectomy only (n = 8). Each pharmaco-rheolytic thrombectomy procedure was performed using the Power Pulse mode. The thrombolytic agents employed comprised tissue plasminogen activator (tPA) in 73 cases and urokinase (UK) in three cases. A 6-Fr Solent catheter (Boston Scientific, Marlborough, MA, USA) was used for arterial thrombosis, while an 8-Fr Zelante catheter (Boston Scientific, Marlborough, MA, USA) was used for venous thrombosis. Hypoosmolar, non-ionic iodinated contrast agent (Omnihexol; Korea United Pharm, Seoul, Republic of Korea) diluted with saline at approximately a half ratio was used in all cases.
Data analysis and definition
Clinical data were gathered with the objective of delineating the potential risk factors associated with AKI after ART intervention. Demographic variables were obtained from electronic medical records, including age, sex, hypertension (HTN), diabetes mellitus (DM), body mass index (BMI), cardiovascular disease, cerebrovascular disease, concurrent malignancy and type, and recent major surgery in 6 months. Laboratory data, such as pre- and post-procedural hematocrit, sCr, estimated glomerular filtration rate (eGFR), postprocedural creatinine kinase (CK), and myoglobin were investigated. Procedural records, such as ART site, usage and dose of pharmacologic thrombolytics, thrombectomy time, amount of used contrast media (CM), additional aspiration, and types of catheter, were also obtained from electronic medical records.
The outcome of interest was the occurrence of AKI after ART. AKI was defined as a ≥1.5-fold increase or ≥0.3 mg/dL rise in sCr within 72 h after ART. Technical success was defined as the successful use of ART. Clinical success was defined as symptom relief within 1 week after the procedure.
Statistical analysis
The statistical analysis was performed using MedCalc version 22.009. Numerical data were presented as mean ± SD. The 95% confidence intervals (CIs) for proportions were calculated. The t-test was used for continuous variables. Categorical variables were compared using the chi-square test or Fisher's exact test. Only variables with a P value < 0.1 in the univariate analysis were included in multivariate analyses using logistic regression. The results are presented as odds ratios (ORs) and P values. A P value < 0.05 was considered to be statistically significant.
Results
In total, we identified 84 patients (40 men [47.6%]; mean age = 67.2 ± 15.9 years) who underwent ART. Of the 84 patients, 15 (17.8%) had developed AKI. The average increase in sCr in the AKI group was approximately 1.74 times and 0.73 mg/dL.
A total of 59 patients underwent the procedure due to venous thrombosis, with causes being DVT of lower extremity (56/59, 94.9%), inferior vena cava thrombosis (1/59, 1.7%), and superior vena cava thrombosis (2/59, 3.4%). In total, 25 patients underwent the procedure due to arterial thrombosis, with causes being thrombosis in lower extremity arteries (21/24, 87.5%), superior mesenteric artery (SMA) thrombosis (2/24, 8.3%), and renal artery thrombosis (1/24, 4.2%). Comorbidities of patients are summarized in Table 1. Technical success was achieved in all patients. Clinical success was achieved in all patients except one who had recurrent thrombosis just after the procedure (83/84). During the procedure, a 6-Fr Solent catheter was used for every patient with arterial thrombosis and an 8-Fr Zelante catheter was used for every patient with venous thrombosis. Additional aspiration thrombectomy was performed, if needed. On average, CM usage amounted to 118.4 ± 9.8 mL (range = 24–288 mL). The mean thrombectomy time was 251.2 ± 15.7 s (range = 30–540 s). In total, 76 patients underwent pharmaco-rheolytic thrombectomy and eight patients underwent rheolytic thrombectomy only. In the pharmaco-rheolytic thrombectomy group, the power pulse mode was used in all cases and tPA (n = 73) and UK (n = 3) were used as thrombolytics. The mean use of tPA was 7.84 ± 0.81 mg and the usage of UK was 200,000 IU in all three patients.
Summary of patient comorbidities.
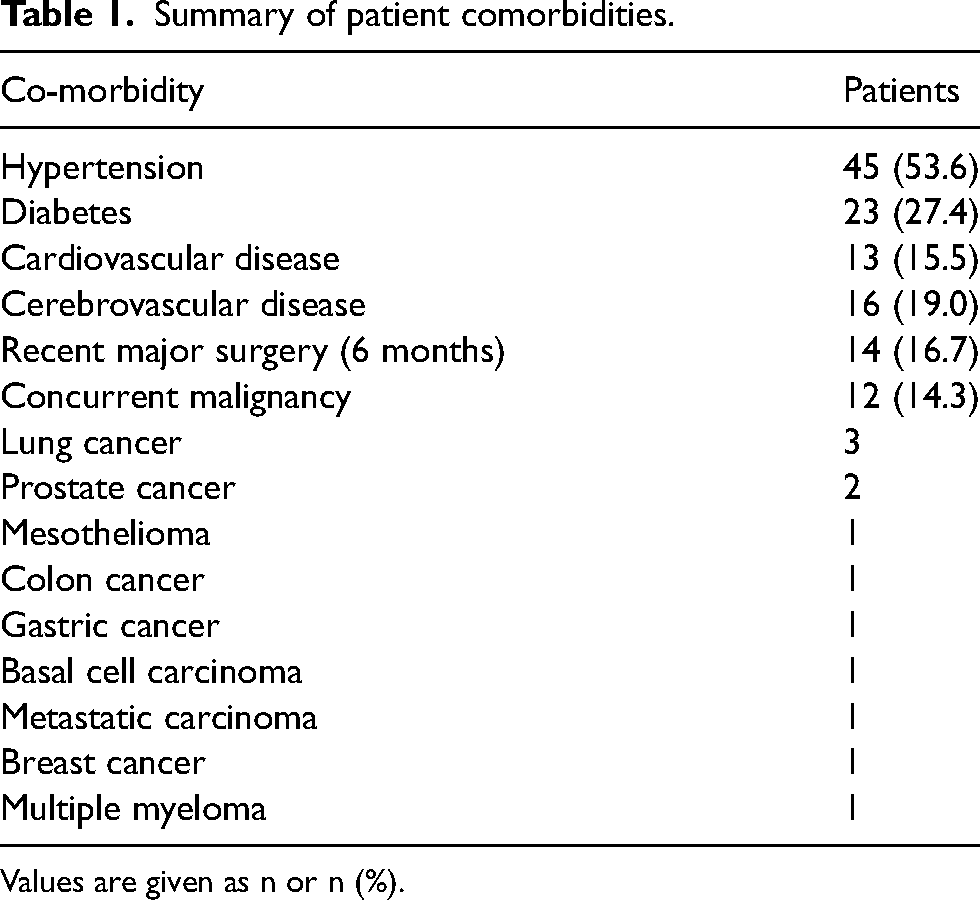
Values are given as n or n (%).
Univariate analysis is presented in Table 2. Upon conducting univariate analysis, age, sex, DM, cerebrovascular disease, recent major surgery, and thrombectomy time did not show a significant association with AKI. Hypertension, obesity, cardiovascular disease, concurrent malignancy, a decrease in hematocrit (≥15%), the use of CM ≥140 mL, and ART in arterial system showed statistical significance or a tendency in relation to AKI development (P < 0.1).
Univariate analysis comparing patients with and without risk factors.
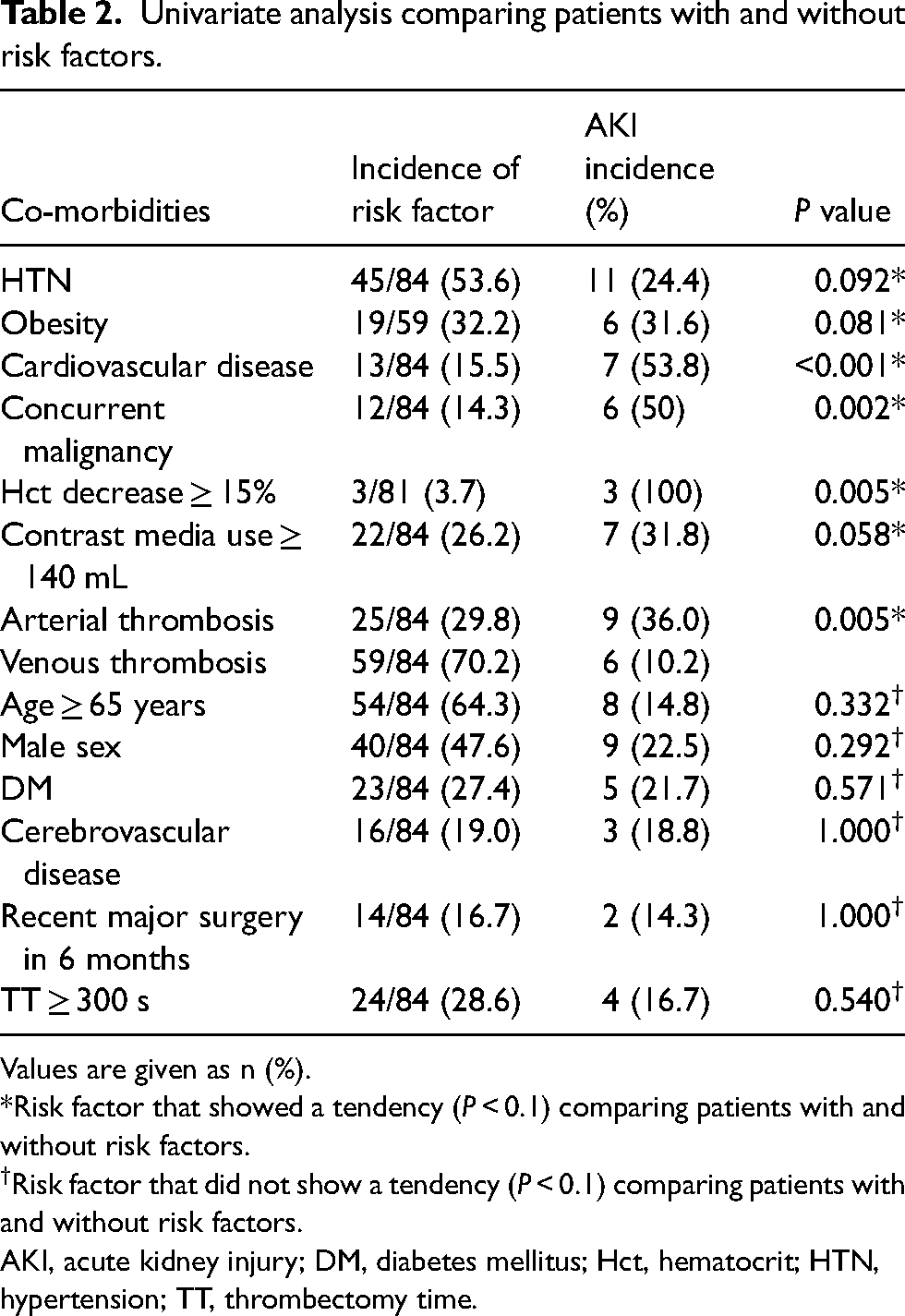
Values are given as n (%).
*Risk factor that showed a tendency (P < 0.1) comparing patients with and without risk factors.
Risk factor that did not show a tendency (P < 0.1) comparing patients with and without risk factors.
AKI, acute kidney injury; DM, diabetes mellitus; Hct, hematocrit; HTN, hypertension; TT, thrombectomy time.
We conducted multivariate analysis on the eight identified factors showing tendencies. The results of the logistic regression analysis for potential risk factors for AKI are summarized in Table 3 and Fig. 1. Logistic regression analysis identified concurrent malignancy (OR = 42.231, 95% CI = 2.332–764.693; P = 0.011) and ART in arterial system (OR = 24.109, 95% CI = 1.319–440.551; P = 0.032) as independent risk factors for developing AKI. In the arterial patient group and the venous patient group, significant differences were observed in terms of sex and baseline sCr. Data are summarized in Table 4.
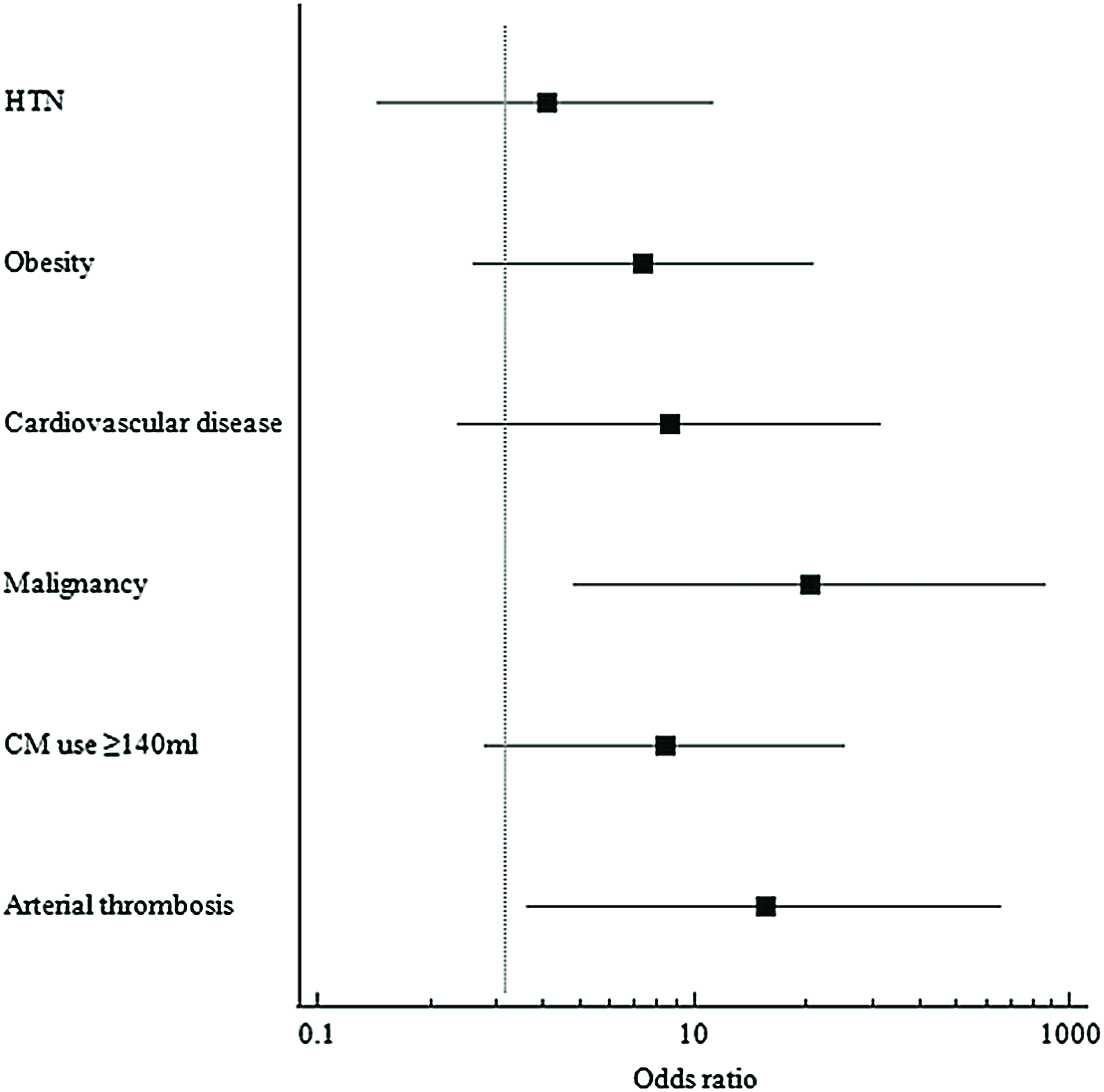
Forest plot of multivariate analysis.
Multivariate analysis comparing patients with and without risk factors.
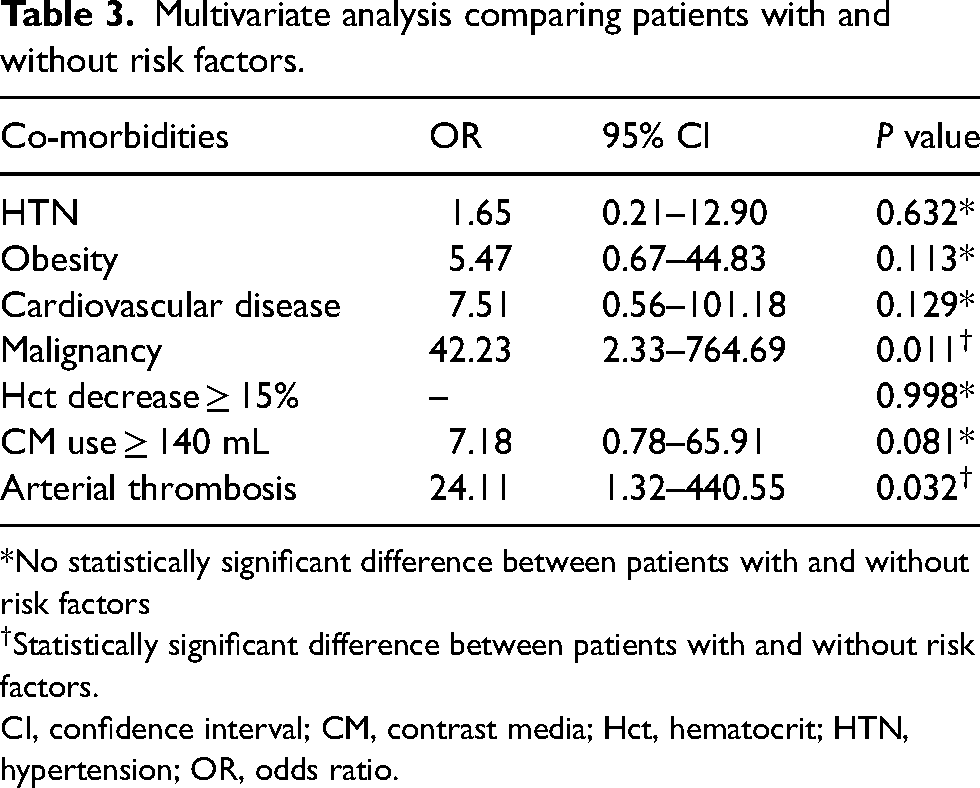
*No statistically significant difference between patients with and without risk factors
Statistically significant difference between patients with and without risk factors.
CI, confidence interval; CM, contrast media; Hct, hematocrit; HTN, hypertension; OR, odds ratio.
Comparison of patients with arterial thrombosis and patients with venous thrombosis.

Values are given as n (%) or mean ± SD.
*No statistically significant difference was found between patients with arterial thrombosis and patients with venous thrombosis.
Statistically significant differences were found between patients with arterial thrombosis and patients with venous thrombosis.
CM, contrast media; Hct, hematocrit; sCr, serum creatinine; TT, thrombectomy time.
Discussion
At our institution, we found that concurrent malignancy and ART in the arterial system were independent risk factors for AKI after ART. In the study, the AKI occurrence rate was 17.8% (15/84). The presence of concurrent malignancy and ART in the arterial system independently predicted the occurrence of AKI after ART. Furthermore, the quantity of CM used and the thrombectomy time were not significantly associated with AKI.
Several studies have shown that AKI was associated with ART. Escobar et al (2016) reported a 29% (15/52) occurrence rate of AKI after ART (5). Morrow et al (1) also reported a 21% occurrence rate of AKI after pharmacomechanical thrombectomy with the tPA pulse mode. Shen et al (6) reported that in iliofemoral DVT patients, ART was a statistically significant risk factor of AKI compared to catheter-directed thrombolysis. They also suggested that a history of major surgery within 3 months of endovascular intervention and an Hct drop were independent risk factors that raised the odds of postoperative AKI.
In this study, we included factors that may contribute to the development of AKI, which were used in previous studies. Addtionally, the dose of the CM and thrombectomy time were considered. We also included both arterial and venous thrombosis patients who underwent ART.
CM is generally considered a potential risk factor for AKI, which may produce contrast-induced nephropathy (CIN). There has been a debate over the relationship between CM and AKI in patients undergoing ART. Only a few papers suggest CM as a risk factor in the relationship between ART in systemic arteries and AKI. Tian et al (4) showed the volume of CM used in the procedure was higher in the AKI group than in the non-AKI group, but they did not suggest a threshold for CM used to prevent AKI, but rather limited it as a difference between the AKI and non-AKI groups. In our study, CM was not associated with AKI. The 2020 Radiologic Society of North America guidelines state that the risk of AKI from iodinated contrast media is overstated, and that a significant risk exists for patients with an eGFR < 30 mL/min/1.73 m2 who are not undergoing maintenance dialysis (2). In our study, three patients had an eGFR < 30 mL/min/1.73 m2 and one patient developed AKI after the procedure. Therefore, while contrast agent usage may not be a risk factor for AKI in the general patient population, caution is required in patients who already have impaired renal function.
The hemolytic effect of ART is considered a major mechanism. A decrease in Hct might be related to procedure time, and one can also consider its relationship with procedure duration. In previous studies, a decrease in Hct and thrombectomy time have been suggested as potential risk factors for AKI after ART (5,6). The rationale behind this consideration is that as thrombectomy time lengthens, the theoretical amount of hemolysis is expected to increase. However, the thrombectomy time did not demonstrate a notable association with AKI. The manufacturer of AngioJet, Boston Scientific, has provided guidelines (7) for thrombectomy time, and all of our procedures except one were conducted following those guidelines. Therefore, it can be considered that the risk of AKI does not increase due to the CM and thrombectomy time when the procedures are performed under the provided guidelines.
AKI is a common complication in patients with cancer. In a Danish population-based study (8), the 1-year risk of AKI in the cancer patient population was 17.5%, with a 27% risk over 5 years. Salahudeen et al (9) reported that 12% of patients admitted to the cancer center in the USA had AKI. It is known that there are various causes of AKI in cancer patients, such as prerenal causes, intrinsic causes, and postrenal causes (3). In our study, 6/12 (50%) patients developed AKI after the procedure. That is a higher figure compared to the incidence of renal failure in cancer patients without ART in previous studies. It can be assumed that ART accelerates several factors that increase the risk of renal failure in cancer patients. For example, ART-induced blood loss can accelerate prerenal AKI in cancer patients who are already depleted due to conditions such as vomiting, poor dietary intake, or anemia. In addition, hemolysis in cancer patients with pre-existing renal vulnerability can speed up the progression to AKI. However, our study had a very small sample size, and there is insufficient supporting evidence and medical records available. Therefore, additional research is needed.
As mentioned before, ART is an effective treatment for both arterial and venous thrombosis. To our knowledge, there has been no previous study comparing the arterial group and the venous group regarding AKI after ART. In our study, ART in the arterial system was an independent risk factor for AKI after ART. We can propose two reasons for this. First, thrombectomy in the arterial system may potentially influence the risk of AKI depending on the procedural location. In our study, all three patients (two with SMA thrombectomy and one with renal artery thrombectomy) who underwent procedures in the renal artery or suprarenal level developed AKI. This suggests the possibility that microthrombi formed during the ART procedure may be traveling towards the renal artery, leading to these occurrences. Second, there is a possibility that it might be due to rhabdomyolysis. In our study, among the six patients who underwent ART in the lower extremity and developed AKI, five had pre- and post-procedural CK or myoglobin level test results available. All patients had at least one of these values increase after the procedure. The occurrence of AKI due to rhabdomyolysis is a well-known phenomenon. However, in our study, the small number of patients and the insufficient medical record documentation make it necessary for further research to draw conclusions regarding these results.
The present study has some limitations. First, it was a retrospective and single-institution study. Second, due to the heterogeneity in the locations and causes of the procedures performed, it is challenging to explain AKI with a single mechanism. In addition, in our study, we did not investigate all possible causes of acute renal failure, including the use of nephrotoxic drugs like non-steroidal anti-inflammatory drugs.
In conclusion, ART is a potential risk for AKI. Concurrent malignancy and ART in the arterial system are independent predictors of AKI.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.