
Abstract
Hyperperfusion is related to vessel recanalization, tissue reperfusion, and collateral circulation. To determine the prognostic impact of hyperperfusion after an acute ischemic stroke (AIS) identified by arterial spin labeling (ASL) cerebral blood flow. Studies published in PubMed, Embase, and Cochrane Library databases were searched. Studies assessing the diagnostic performance of ASL hyperperfusion after AIS were included. Functional prognosis, hemorrhagic transformation (HT), infarction volume, and penumbra salvage volume were evaluated. The standardized mean difference or risk ratio was pooled, implementing a random effect model. Multiple subgroup analyses were performed. Seven studies including 617 participants were included in this meta-analysis. ASL hyperperfusion in AIS was correlated well with symptom severity and outcome after 24 h National Institutes of Health Stroke Scale (NIHSS) and 90-day modified Rankin Scale (mRS). Earlier ASL hyperperfusion was associated with a smaller infarction volume and a larger penumbra salvage volume, while also indicating a higher risk of HT. In addition, in subgroup analysis, our results demonstrated that thrombolysis, mechanical thrombectomy treatment, early improvement of NIHSS, and involving infarction in cortical territory are associated with ASL hyperperfusion. ASL hyperperfusion was related to a favorable functional outcome but an increased risk of HT. Stroke patients with hyperperfusion showed smaller infarction volume and larger penumbra salvage volume than those with non-hyperperfusion.
Introduction
Stroke remains the second-leading cause of death and the third-leading cause of disability-adjusted life-years lost (DALYs) globally (1). The number of stroke events, incidence of stroke, mortality, and DALYs due to stroke all increase year upon year (2). Notably, ischemic stroke constitutes the majority, accounting for 62.4% of all strokes (2). There is no doubt that stroke has been a great burden for patients and their families, as well as society. Early detection, diagnosis, and intervention are important, and are strongly associated with prognosis.
Specific imaging profiles that are predictive of longer-term stroke recovery are important after effective treatment procedures. Recent research highlights the superior predictive value of reperfusion over recanalization, particularly concerning follow-up infarct volumes and clinical outcomes (3). The assessment of reperfusion after therapy in acute ischemic stroke (AIS) patients has received increased attention over the past few years. Computed tomography (CT)-based assessment of perfusion, dynamic susceptibility contrast magnetic resonance imaging (DSC-MRI), and diffusion-weighted imaging (DWI) have been widely implemented in numerous studies to quantify reperfusion (4–7). In addition, ASL, a non-invasive perfusion imaging technique, has emerged as a valuable tool for estimating cerebral blood flow (CBF) without radiation exposure or contrast-agent administration. This is particularly advantageous for patients with impaired renal function or those requiring repetitive perfusion imaging. ASL has demonstrated feasibility in qualitatively assessing reperfusion tissues. Previous research has established the reliability of ASL in detecting perfusion alterations in ischemic stroke, showing a moderate-to-good correlation with DSC perfusion-weighted imaging (PWI) (8,9). Notably, some studies suggest that ASL imaging exhibits greater sensitivity in visualizing hyperperfusion, a common phenomenon after ischemic stroke by thrombolysis (10). Lu et al. (11) also demonstrated that ASL hyperperfusion was significantly correlated with successful recanalization and might be an independent predictor of favorable outcomes at 90-day after mechanical thrombectomy. Furthermore, hyperperfusion, as evaluated by ASL, is associated with early clinical improvement (10). However, several other studies observed that hyperperfusion after reperfusion was related to hemorrhagic transformation (HT) and poor prognosis (12–14). Currently, the prognostic significance of hyperperfusion as evaluated by ASL remains controversial.
The aim of the present meta-analysis was to determine the prognostic impact of ASL hyperperfusion in AIS and to further analyze the relationship between the sign and infarction volume, penumbra salvage volume, and HT. Other factors, including age, sex, and underlying diseases, were also considered.
Material and Methods
This systematic review and meta-analysis was performed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (15). Our study was based on previously published literature; therefore, no informed consent or ethical committee approval was required.
Search strategy
We searched the PubMed, Embase, and Cochrane Library databases up to 20 May 2022 using the terms “hyperperfusion” AND [“infarction” OR “cerebrovascular disorder” OR “stroke”] AND [“arterial spin labeling” OR “ASL”] (see supplementary material). We also added language and human studies as constraints.
Eligibility criteria
The inclusion criteria were as follows: (i) AIS patients aged ≥ 18 years; (ii) ASL acquired after symptom onset or treatment; and (iii) functional outcomes were evaluated. The exclusion criteria were as follows: (i) contraindications of MRI; and (ii) studies that did not provide original data, such as reviews, meta-analysis, conference abstracts, and case reports.
Quality assessment and data extraction
Two reviewers carried out the data extraction independently by browsing the full text. All data were cross-checked by a second reviewer. The Newcastle-Ottawa Scale (NOS) was applied to assess the quality of the included studies, which consisted of three parts: selection, comparability, and outcome. If there was a disagreement about the results, the two reviewers would discuss until they were in consensus. From the studies that met the inclusion criteria, basic information was extracted, as follows: first author’s name; year of publication; duration of patient recruitment; sample size; sex; study design; treatment method; functional outcome assessments; and ASL examination time. Moreover, the baseline factors with the presence of ASL hyperperfusion were also extracted by the two reviewers independently, such as hypertension, atrial fibrillation, and diabetes mellitus. For longitudinal studies, we also listed follow-up durations and primary results extracted from the papers. The primary objective of this study was to analyze the functional prognosis evaluated with the modified Rankin Scale (mRS) or the National Institutes of Health Stroke Scale (NIHSS). The secondary objectives were to define the relationship between the sign with infarction volume, penumbra salvage volume and HT; and the influence of age, sex, smoking, cardiovascular risk factors, and large artery atherosclerosis.
Statistical analysis
STATA version 15.1 (STATACorp., College Station, TX, USA) was used for statistical analysis. Continuous variables and discontinuous variables were represented by standardized mean difference (SMD) and risk ratio (RR) with a 95% confidence interval (CI), respectively. The heterogeneity was estimated using the Cochran Q test and I2 statistics. If the I2 value was >40%, the random effect model was adopted, otherwise, the fixed effect model was adopted. Graphical representations were shown as forest plots. To evaluate the public bias and validate the robustness of our results, the funnel plot, subgroup analysis, and sensitivity analysis were performed, respectively. P <0.05 was considered statistically significant.
Results
Literature selection
A total of 350 studies were searched. By screening the title and abstract, 96 full-text studies were included. Due to incomplete information or data extraction, only seven studies were finally included (Fig. 1). One out of seven studies had a high risk of bias (see supplementary material; Fig. 2), but the overall results of the article were not significantly affected when this study was removed (see supplementary material; Fig. 3). The assessment of public bias is provided in the supplementary material (Fig. 1).
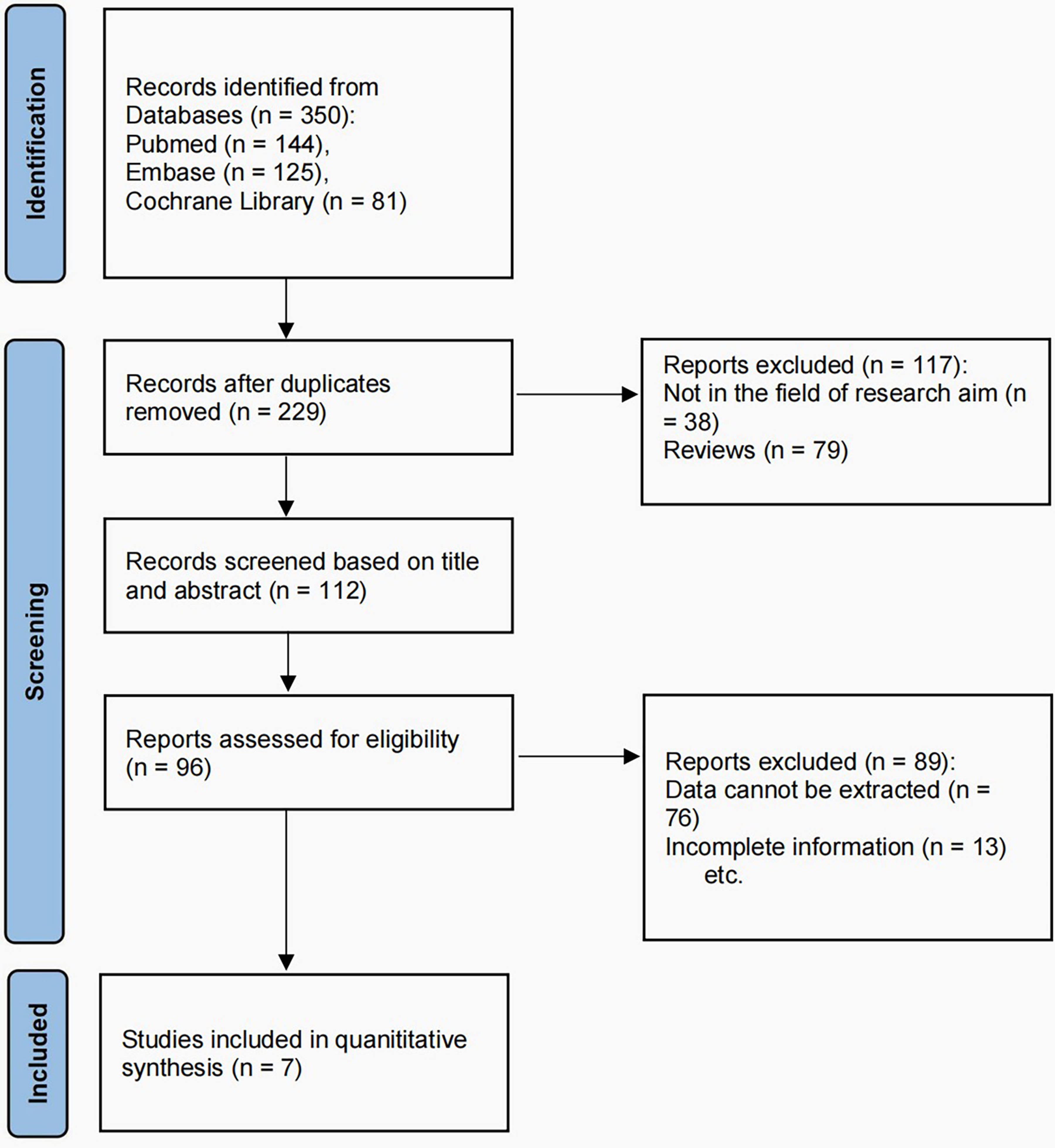
Selection process of the studies included in the meta-analysis.
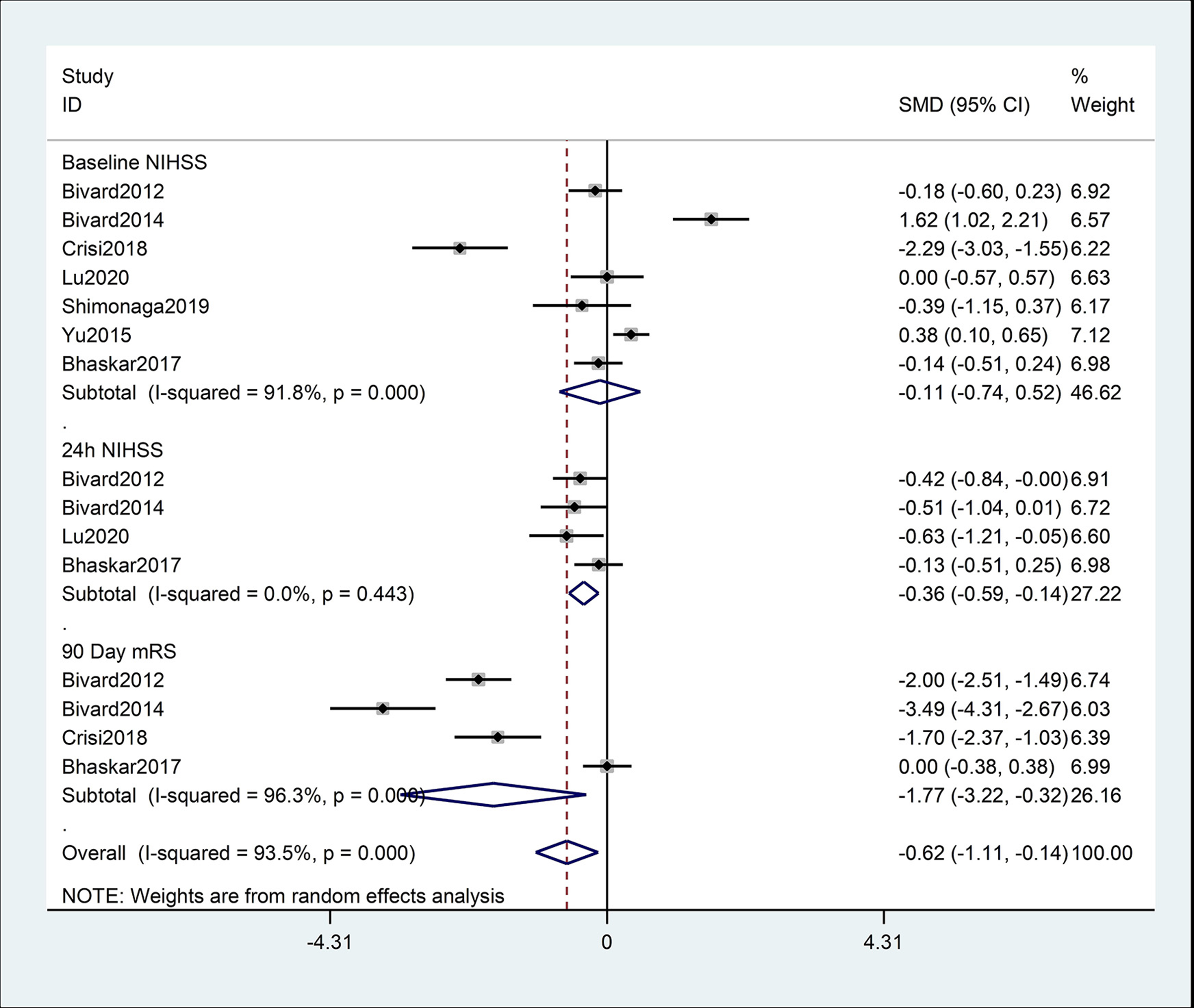
Meta-analysis of NIHSS and mRS score for ASL hyperperfusion and non-ASL hyperperfusion at different time points. ASL, arterial spin labeling.

Meta-analysis of associations between ASL hyperperfusion and DWI lesional volume and penumbral salvage volume. ASL, arterial spin labeling; DWI, diffusion-weighted imaging.
Characteristics of the included studies
Ultimately, four prospective studies and three retrospective studies were included. The definition of hyperperfusion in the included articles was determined by visual inspection in five studies and by comparison with the contralateral side in two studies. All of the included studies provided the baseline NIHSS scores at admission. There were four studies on 24-h NIHSS, four studies on 90-day mRS, and four studies on the risk of HT. Three studies reported penumbra salvage volume and six studies reported infarction volume. There were four studies that mentioned the following influence factors: present smoker; hypertension; atrial fibrillation; and intravenous tissue plasminogen activator. Diabetes mellitus and dyslipidemia were mentioned in three studies. Furthermore, two studies reported the factors of aspirin use, mechanical thrombectomy, large artery atherosclerosis, cardioembolic, infarction of cortical territory, and early improvement of NIHSS. The demographic characteristics and quality assessment are shown in Table 1 and Table 1 in the supplementary material.
Demographic characteristics of the included studies.

ASL, arterial spin labeling; IA, intra-arterial; IV, intravenous; MRI, magnetic resonance imaging; NA, not available; tPA, tissue plasminogen activator.
Association of hyperperfusion with functional prognosis
The ASL hyperperfusion was related to 24 h (SMD = −0.36, 95% CI = −0.59 to −0.14; P = 0.002; I2 = 0.0%) and 90-day (SMD = −1.77, 95% CI = −3.22 to −0.32; P = 0.016; I2 = 96.3%) functional outcome, suggesting that ASL hyperperfusion was related to a favorable prognosis (Fig. 2).
Association of hyperperfusion with infarction volume, penumbra salvage volume, and HT
Compared with the non-ASL hyperperfusion group, the ASL hyperperfusion group showed a smaller infarction volume (SMD = −0.46, 95% CI = −0.77 to −0.15; P = 0.003; I2 = 58.8%) and larger penumbra salvage volume (SMD = 1.38, 95% CI = 0.45–2.32; P = 0.004; I2 = 90.9%). In addition, the ASL hyperperfusion was associated with an increased risk of HT (RR = 2.38, 95% CI = 1.20–4.72; P = 0.013; I2 = 65.6%). The results of infarction volume and penumbra salvage volume are shown in Fig. 3, and the results of HT are shown in Fig. 4.

Meta-analysis of associations between ASL hyperperfusion and hemorrhagic transformation. ASL, arterial spin labeling.
Association of hyperperfusion with other influencing factors
Hyperperfusion was more frequently observed in patients who underwent intravenous thrombolysis (RR = 1.27, 95% CI = 1.08–1.48; P = 0.003; I2 = 65.4%) or mechanical thrombectomy (RR = 2.50, 95% CI = 1.63–3.82; P = 0.000; I2 = 0.0%) than in patients without these treatments. In the subgroup analysis, infarction in the cortical territory was correlated with ASL hyperperfusion (RR = 1.9, 95% CI = 1.46–2.48; P = 0.000; I2 = 7.8%). Moreover, a significant association between early improvement of NIHSS and ASL hyperperfusion was detected (SMD = 0.51, 95% CI = 0.17–0.85; P = 0.003; I2 = 0.0%) (Table 2).
Meta-analysis of the associations of baseline factors with the presence of ASL hyperperfusion.
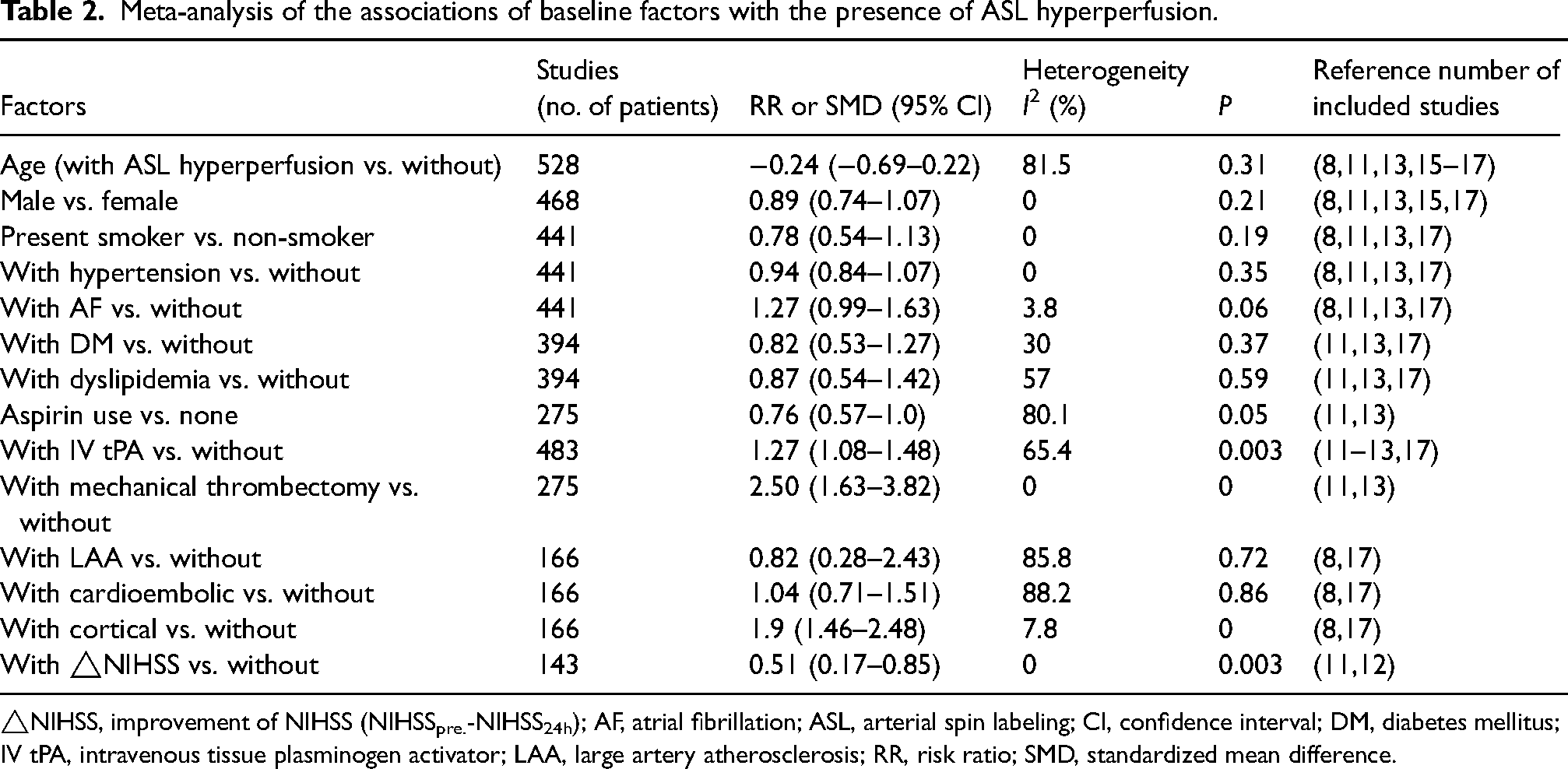
△NIHSS, improvement of NIHSS (NIHSSpre.-NIHSS24h); AF, atrial fibrillation; ASL, arterial spin labeling; CI, confidence interval; DM, diabetes mellitus; IV tPA, intravenous tissue plasminogen activator; LAA, large artery atherosclerosis; RR, risk ratio; SMD, standardized mean difference.
Discussion
The meta-analysis was designed to determine the prognostic impact of ASL hyperperfusion after AIS. Ultimately, we found that hyperperfusion was associated with a favorable functional prognosis. This correlation was particularly pronounced in patients who underwent intravenous thrombolysis, received mechanical thrombectomy treatment, exhibited cortical infarction, and demonstrated early improvement of NIHSS. Hyperperfusion was related to smaller infarction volume, larger penumbra salvage volume, and was associated with a greater frequency of HT.
A previous study using positron emission tomography (PET) to evaluate the relationship between CBF and neurological prognosis after the first stroke (5–18 h after stroke onset) found that patients in the hyperperfusion group had a good recovery (18). This is consistent with our finding that ASL hyperperfusion is associated with good clinical outcomes in AIS. The occurrence of hyperperfusion is due to vessel recanalization, tissue reperfusion, and collateral circulation (10,19,20). Tissues with hyperperfusion are more metabolically active and more capable of later neuroplasticity (16). Studies on animal models have shown that hyperperfusion is a sign of early effective recanalization (21–23). Reperfusion could predict follow-up infarction volume more accurately than recanalization (3). Kucinski et al. (24) found that patients with middle cerebral artery trunk occlusion had abundant collateral circulation and successful recanalization with thrombolytic therapy, which had better clinical results than other types of occlusions, but only collateral circulation was an independent radiological predictor of outcome after thrombolysis in AIS. The arterial collateral circulation, including the circle of Willis and leptomeningeal vessels, is distributed differently between patients (25,26). The richer the collateral circulation, the higher the signal on ASL, which shows hyperperfusion and vice versa. The presence of collaterals in ASL is closely related to better neurological outcomes in AIS (27). In line with a previous report, more robust leptomeningeal collateral perfusion scores on CBF were observed in better outcome patients in contrast to worse outcome patients, although the differences were not significant (28). A hypoperfusion volume ratio ≥ 50%, considered poor collateral circulation, was an independent risk factor for early neurological deterioration (29). In addition, it is worth noting that hyperperfusion is different from cerebral hyperperfusion syndrome, the latter refers to the increase of CBF exceeding the demand of brain tissue, and resulting in neurological impairment (14), which is rarer than hyperperfusion and mainly occurs in carotid endarterectomy or carotid artery stenting (13,30,31). Cerebral hyperperfusion syndrome often indicates a bad prognosis.
Both infarction volume and penumbra salvage volume are related to ASL hyperperfusion, possibly due to collateral circulation. The survival of penumbra mainly depends on the collateral circulation of the brain in AIS (32). The collateral circulation will act immediately to supply blood flow to the ischemic areas through anastomotic vessels when ischemia occurs, which can prevent further expansion of the infarction on the one hand and maintain perfusion of the penumbra on the other hand. If the collaterals are adequate to maintain the perfusion of the penumbra, a larger volume of penumbra will be saved and a smaller infarction volume will be found (27,33). Conversely, the infarction core expands outwards, thereby increasing the infarction volume and reducing the penumbra salvage volume. The prerequisite for reducing the infarction volume and saving the nerve cells around the infarct is a rapid and complete recanalization, but sufficient collaterals seem to be another potential prerequisite for the survival of the ischemic area to the success of recanalization (24,34). Dynamic changes of collateral flow were associated with infarction growth (35). Patients with robust collaterals had smaller final infarction volume and better clinical outcomes after AIS (36). One meta-analysis demonstrated that infarction volume had a significant relationship with unfavorable functional outcome in ischemic stroke patients (37). Given the above, it is very important to detect collaterals as soon as possible, which may be related to the prognosis of patients. We also found a significant correlation existed between hyperperfusion and HT, a bad complication that can be potentially life-threatening to stroke victims. This was similar to a previous study by Okazaki et al. (38), whose findings suggested that ASL hyperperfusion after reperfusion could be a marker of HT. The causes of this phenomenon may be related to the disruption of the blood–brain barrier and the damage of CBF autoregulation (12). HT can be divided into hemorrhagic infarction (HI) and parenchymal hemorrhage (PH) (39,40). PH is more severe than HI in classification. Yu et al. (12) have found that the time of hyperperfusion is related to the grade of HT: the later the hyperperfusion showed, the higher the grade of HT appeared. Effective dynamic cerebral autoregulation was related to smaller infarction volume and better neurological outcomes in AIS (41). In the case of poor baseline collaterals, effective recanalization treatment may induce HT and lead to deterioration of neurological function (17,42,43). Therefore, we speculated that non-hemorrhagic hyperperfusion may be a marker for favorable tissue outcomes. To reduce the risk of HT, clinical careful management, such as controlling blood pressure, is required.
According to the subgroup analysis of treatment methods, hyperperfusion is more likely to be observed after intravenous thrombolysis or mechanical thrombectomy. In accordance with a review of high recanalization rates, high favorable clinical outcome rates and low complication rates were associated with endovascular therapies for stroke. They also showed that the better the recanalization, the better the outcome (44). A study by Siegler et al. (33) reported that initial stroke severity was an independent risk factor for neurologic deterioration, which could be modifiable to reduce the clinical decline by achieving intravenous thrombolysis and intra-arterial therapy. To subdivide infarction location, we found that the cortical territory infarction was related to ASL hyperperfusion. As far as we know, the blood flow is more abundant in the cortex than in the subcortex. The leptomeningeal collaterals, which are densely distributed in the cortical vascular territory of superior middle cerebral, play an important role in providing blood flow to the distal brain tissue of infarction when the CBF changes (25,35,43). Furthermore, leptomeningeal and dural arterioles are anastomosed with cortical vessels to further strengthen collateral circulation (25). That may explain why hyperperfusion can be observed in cortical infarction. Moreover, a significant association between early improvement of NIHSS and ASL hyperperfusion was detected in the meta-analysis. Does it mean ASL hyperperfusion contributes to the early improvement of neurological function? Our results seem to form a closed-loop relationship and correspond to each other. However, due to the small number of articles included, the results need to be further explored.
Although ASL has shown promising results in stroke imaging, it has not been routinely applied in clinical scenarios. Challenges may arise from the available techniques, such as the influence of the post-labeling delay (PLD) during ASL acquisition, a key parameter in CBF quantification, and the difficulty of stroke patients’ access to MRI in the period required following treatment. Nevertheless, ASL is still a promising technique.
The present study has some limitations. First, the sample size included is too small, which may influence our conclusions. Second, there is considerable heterogeneity in our study, despite the use of a random effect model. Third, we performed a sensitivity analysis on the total risk of bias for all included studies. Using a “leave-one-out” approach by excluding the study by Yu et al. (12), the results showed that no individual study significantly influenced the results (see supplementary material Fig. 3). Further research is necessary to conduct more in-depth analyses in the future.
In conclusion, the results of the meta-analysis revealed that ASL hyperperfusion was associated with a good functional prognosis and was more frequently observed after intravenous thrombolysis or mechanical thrombectomy. In addition, ASL hyperperfusion was related to smaller infarction volume, larger penumbra salvage volume, and was correlated with an increased incidence of hemorrhagic transformation.
Supplemental Material
sj-docx-1-acr-10.1177_02841851241300328 - Supplemental material for The prognostic impact of arterial spin labeling hyperperfusion in acute ischemic stroke: a systematic review and meta-analysis
Supplemental material, sj-docx-1-acr-10.1177_02841851241300328 for The prognostic impact of arterial spin labeling hyperperfusion in acute ischemic stroke: a systematic review and meta-analysis by Yu Jin, Xi Bai, Da Guo and Zhiwei Guo in Acta Radiologica
Footnotes
Acknowledgments
The authors thank all the authors of the articles on ASL hyperperfusion.
Data availability
All data related to the article can be found in the original text and supplementary material.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.