
Abstract
Background
Voiding cystourethrography (VCUG) remains the best method to diagnose and to determine vesicoureteral reflux (VUR) grade.
Purpose
To determine necessity and indications of VCUG and to investigate high-grade VUR predictors.
Material and Methods
We retrospectively reviewed data. The patients were sorted into three age groups: 0–12 months; 13–24 months; and above 24 months. Student t-test, Mann–Whitney U test, ANOVA, and Kruskal Wallis test were used to compare the means between groups. Pearson’s correlation test was used for correlation analysis. Risk factors were determined by multivariate regression analysis.
Results
The most common indication for VCUG was recurrent urinary tract infections (UTIs). VCUG revealed VUR in 96 (18.4%) patients, posterior urethral valve (PUV) in 13 (2.5%) patients, and bladder anomalies in 14 (2.6%) patients. Neither sex nor age was statistically significantly associated with presence or grades of VUR. Multivariate analysis showed that a history of recurrent UTI (P = 0.008), a presence of high-grade hydronephrosis (HN) on renal-bladder ultrasound (RBUS) (P = 0.001), and a presence of scarring on dimercaptosuccinic acid renal cortical scintigraphy (DMSA) (P < 0.001) were strongly associated with high-grade VUR. In addition, female sex, renal dysfunction, high-grade VUR, history of recurrent UTIs, and older age at diagnosis were identified as risk factors for renal scarring.
Conclusion
We highlight that the most common indication for VCUG is recurrent UTIs, which is associated with higher renal damage and high-grade VUR. If a VCUG should be considered for children with recurrent UTIs, high-grade HN and renal scaring, which are the predictors of high-grade VUR.
Keywords
Introduction
Voiding cystourethrography (VCUG) remains the gold standard imaging technique for evaluating both the anatomical structure of the bladder and urethra, as well as diagnosing and grading vesicoureteral reflux (VUR) (1,2). The primary indication for performing VCUG is to determine the presence or absence of VUR in children with febrile urinary tract infections (UTIs) and abnormal renal ultrasound (US) findings. However, VCUG is an invasive procedure with potential complications, including catheterization, pain, radiation exposure, iatrogenic UTI, and trauma to the urethra or bladder (1,2).
VUR is the most common congenital anomalous development of the ureterovesical junction, which prevents the reflux of urine from the bladder, back up to the ureter, and into the collecting system of the kidney (1,3). VUR increases the risk of recurrent UTIs, leading to renal scarring and then worsening into renal hypertension and kidney failure (4,5). Primary VUR incidence in children is nearly 1% (1). The prevalence of VUR in infants diagnosed with prenatal hydronephrosis (HN) and screened for VUR was 16.2% (1,4). Although the risk of VUR in siblings of children with VUR was 27.4%, this rate was higher in children of parents with VUR (35.7%) (1,6). It is detected in one-third of the children with febrile UTI (4). Secondary VUR is caused by bladder neck or urethra obstruction or neurogenic bladder dysfunction (1). A dimercaptosuccinic acid (DMSA) scan is recommended as the best nuclear examination for the detection of parenchymal renal tissue and differential function between the two kidneys (1). DMSA, when performed at the right time, can detect whether there is renal scarring caused by UTI and the function, size, shape, and position of each kidney (1). The necessity of routine evaluation of UTI with VCUG is questioned because most diagnosed cases of VUR are low-grade. It is important to confirm the presence of a high-grade VUR in paediatric patients by selectively performing VCUG.
The aim of the present study was to determine the necessity and indications of VCUG and to investigate high-grade VUR predictors.
Material and Methods
In the present study, we evaluated the data of our pediatric patients who underwent VCUG to investigate predictors of high-grade VUR to reduce unnecessary VCUG applications.
This study was approved by the local ethics committee (reference no. 73799008; dated 28 July 2017). The requirement for informed consent was waived because of the retrospective observational nature of the study.
Patient population
This retrospective study included a total of 521 patients aged 0–17 years who underwent VCUG in a 1-year period. All VCUGs were performed at our hospital. Indications for VCUG include UTIs (febrile or recurrent), moderate or severe HN (antenatal or postnatal), urinary tract anomalies (double pelvis/ureter, multicystic dysplastic kidney [MCDK]), and bladder abnormalities (diverticulum, ureterocele, and neurogenic bladder). During a 1-year period, 532 children underwent VCUG. The inclusion criteria were patients aged 0–17 years who had undergone VCUG and whose medical charts were complete. Patients with ambiguous genitalia, anorectal malformation, second VCUG after VUR surgery, urine culture grew more than one organism, or missing data were excluded from the study (Fig. 1).

Flowchart of study population.

VUR and HN on (a) the right kidney and (b) the left kidney. HN, hydronephrosis; VUR, vesicoureteral reflux.
Data evaluation
The clinical and demographic data, history of UTIs, indication for VCUG, and results of VCUG, RBUS, and DMSA scans were recorded retrospectively. The patients were divided into three groups according to their ages: 0–12 months; 13–24 months; and above 24 months.
Ultrasound examinations of the urinary system were performed on all patients by experienced radiologists.
The evaluation of VCUG was performed at our academic children's hospital by pediatric radiologists. In addition, all VCUG images were specifically confirmed by the radiologist who participated in this study and has been practicing pediatric diagnostic imaging and interpretation for at least 15 years. The VUR was graded according to the recommendations of the International Reflux Study Committee (1). VCUG was conducted while the urine was sterile. All patients undergoing VCUG received antibiotic prophylaxis for 3 days after the procedure (4,5).
The DMSA scan was performed according to a standard protocol, at least 6 months after the febrile UTI.
Definitions
The diagnosis of febrile UTI was based on the presence of symptoms accompanied by a fever of ≥38 °C, a positive urine analysis (leukocyte esterase or nitrite positivity and/or bacteriuria or pyuria), and positive urine culture showing growth of a single uropathogen >100,000 CFU/mL (4,5).
Recurrent UTI was defined as two or more episodes of acute pyelonephritis/upper UTI, or one episode of acute pyelonephritis/upper UTI plus one or more episodes of cystitis/lower UTI, or three or more episodes of cystitis/lower UTIs within 1 year (4,5).
HN was defined as a dilation of the kidney collecting system. Antenatal HN was defined as a dilatation of the pelvis and calyces detected via prenatal ultrasound, and it was graded according to the maximal anteroposterior diameter of the renal pelvis and calyceal dilatation (6).
Chronic kidney disease was defined as a reduced glomerular filtration rate (<60 mL/min/1.73 m2) lasting for 3 months or longer (7).
Hypertension was defined as blood pressure higher than the 95th percentile for the child's age, sex, and height at three separate visits.
Continuous antibiotic prophylaxis (CAP) was administered to patients aged <1 year who had experienced a UTI or recurrent UTIs and had moderate or severe HN and/or hydroureteronephrosis (HUN) (8).
Statistical analysis
The statistical analysis was performed using SPSS version 17 (Chicago, IL, USA). The descriptive properties of the variables (mean, median, number, and percentage) were found. Numerical variables were checked for normal distribution. The comparisons of proportions were performed using chi-square tests. Student’s t-test was used for normally distributed numerical variables and the Mann–Whitney U test was used for non-normal distributed numerical variables when two groups were compared. When comparing the numerical values of multiple groups, ANOVA was used for normal dividing variables and the Kruskal–Wallis test was used for the comparison of non-normal dividing variables. Pearson’s correlation test was used for correlation analysis. Univariate logistic regression analysis was performed to determine high-grade VUR risk factors. Then, if a value was <0.25 in univariate analysis outcomes a multivariate regression analysis was performed and risk factors were determined. A P value <0.05 was considered statistically significant.
Results
Demographic and clinical findings
In total, 521 patients underwent VCUG (251 boys [48.2%], 270 girls [51.8%]; median age = 1.0 year for boys [range = 0–16 years] and 4.0 years for girls [range = 0–17 years]. Of the 96 (18.4%) patients in whom VUR was detected, 45.8% were boys and 54.2% were girls. There was a predominance of boys in the group aged <12 months and of girls in the group aged >24 months (Table 1).
Indications of VCUG according to sex and age groups.
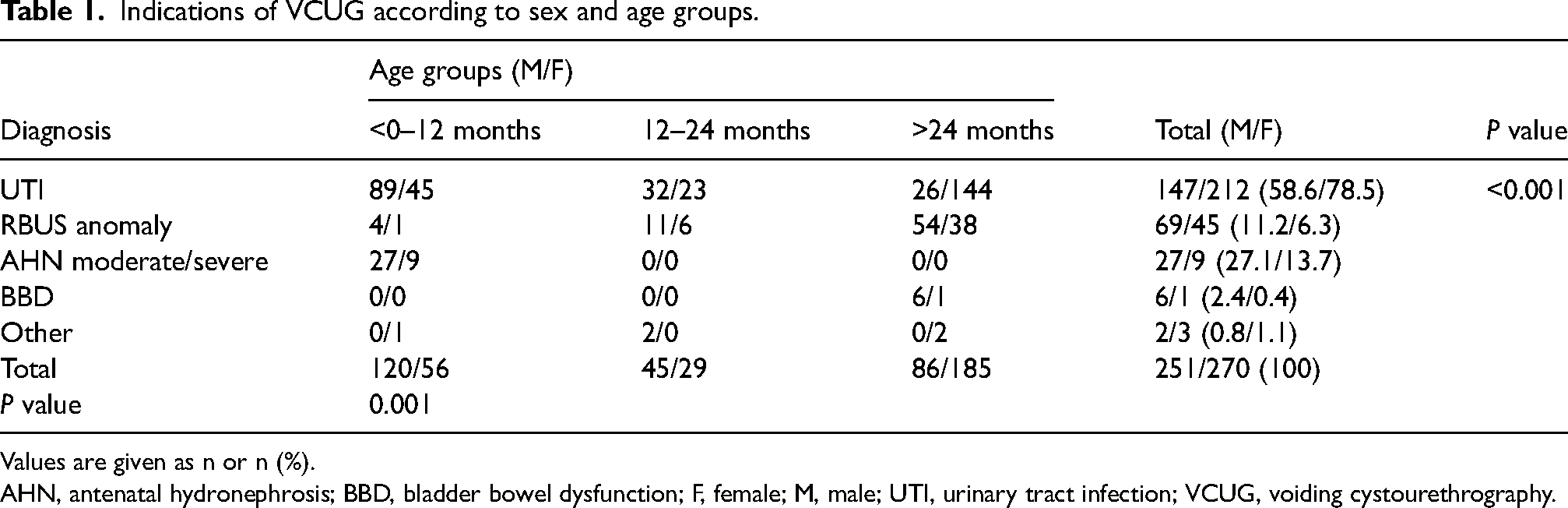
Values are given as n or n (%).
AHN, antenatal hydronephrosis; BBD, bladder bowel dysfunction; F, female; M, male; UTI, urinary tract infection; VCUG, voiding cystourethrography.
VCUG indications
The most common indication for VCUG was recurrent UTIs for all age groups (51.7%, 73%, and 62.7%, respectively; P <0.001) and sexes (47% for boys vs. 73% for girls; P <0.001). Other VCUG indications were the evaluation of moderate/severe antenatal HN and RBUS anomalies. The indications for VCUG are shown in Table 1.
Vesicoureteral reflux
Pathologic findings detected by VCUG were VUR in 96 (18.4%) patients, bladder anomalies (diverticulum, ureterocele, neurogenic bladder) in 14 (2.6%) patients, PUV in 13 (2.5%) patients, and vesicovaginal reflux in 1 (0.02%) patient. Vesicoureteral reflux was observed in 137 (26.3%) ureters (42.7% bilateral, 57.3% unilateral [52.6% left and 47.4% right ureter]) in 96 (18.4%) patients. Reflux was detected in 62 male ureters and 75 female ureters. In addition, there was no statistical difference between sex and either VUR detection rate or VUR grade, nor between age and either VUR detection rate or VUR grade (P = 0.710 and P = 0.246, respectively). VUR grades are presented in Table 2. Consanguineous marriage (P = 0.024), presence of UTI (P <0.001), history of recurrent UTIs (P <0.001), nitrite positivity (P <0.001), presence of HN (P <0.001) or HUN (P <0.001) with RBUS imaging, and detection of scarring (P <0.001) on DMSA were considered significant predictive risk factors for VUR.
Reflux grades according to VCUG indications.

Values are given as n or n (%).
AHN, antenatal hydronephrosis; BBD, bladder bowel dysfunction; RBUS, renal bladder ultrasonography; UTI, urinary tract infection; VCUG, voiding cystourethrography; VUR, vesicoureteral reflux.
Logistic regression analysis showed that a history of recurrent UTIs, high-grade HN on RBUS, and detection of scarring on DMSA were significantly predictive risk factors for high-grade VUR (Table 3).
Risk factors for high-grade VUR.
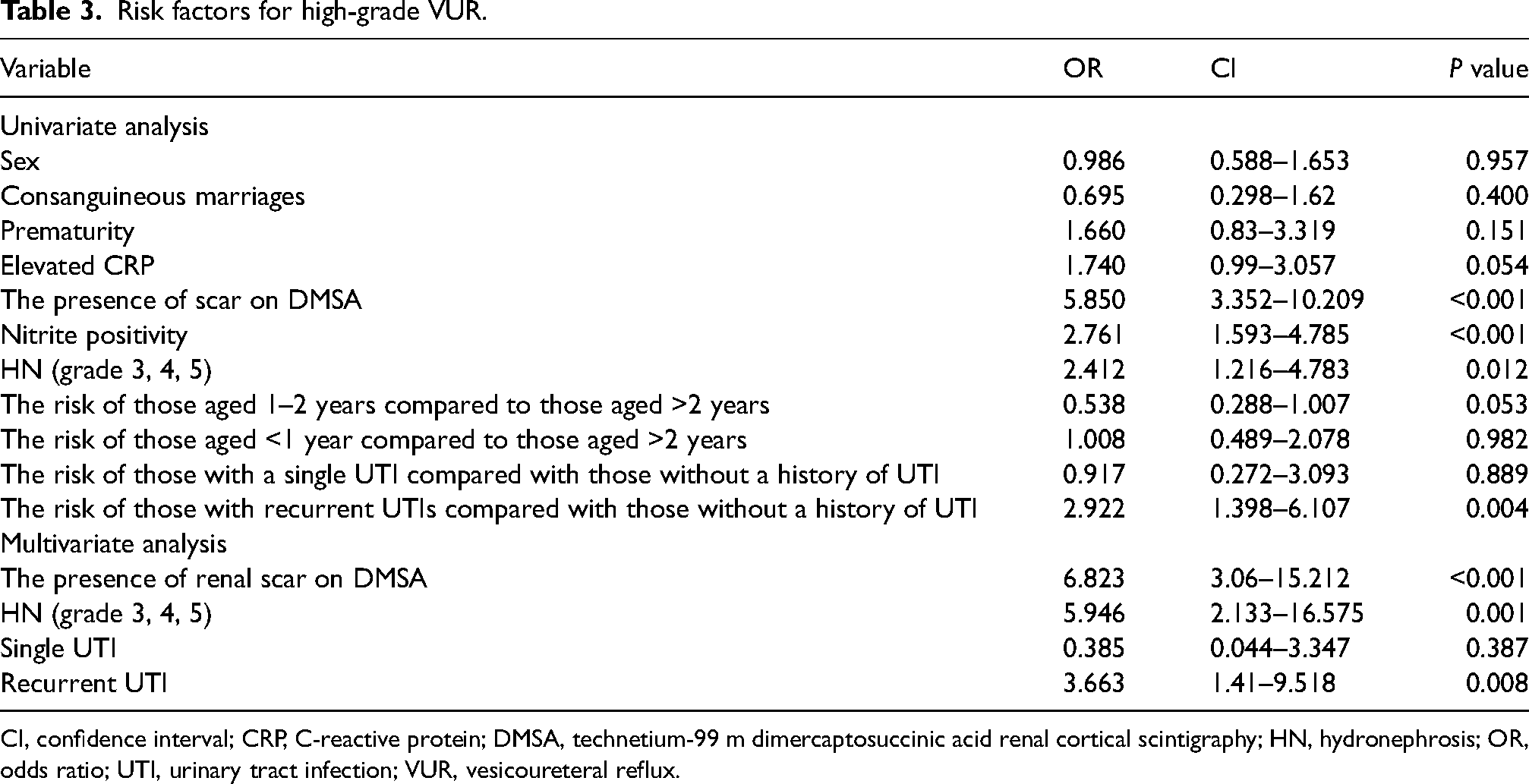
CI, confidence interval; CRP, C-reactive protein; DMSA, technetium-99 m dimercaptosuccinic acid renal cortical scintigraphy; HN, hydronephrosis; OR, odds ratio; UTI, urinary tract infection; VUR, vesicoureteral reflux.
VUR was detected in 77/316 (24.4%) patients (in 113 ureters) with recurrent UTIs, in contrast to 8/66 (12.1%) patients (in nine ureters) with single febrile UTI. There was statistical significance between recurrent UTI and age, sex, nitrite positivity, presence of HN in RBUS, presence of scarring on DMSA, and presence of VUR (P <0.001 for all).
The association of RBUS findings with VCUG abnormalities
Renal and bladder ultrasonography was performed in all patients before the application of VCUG and was evaluated as normal in 165/521 (31.7%) patients. Of the 376 ureters that were detected with HN on RBUS, 93 (24.7%) were found to be accompanied by VUR. Of the 35 patients with bladder abnormality on RBUS, 6 (31.4%) had VUR (in 13 ureters). Of the 35 patients with bladder abnormality on RBUS, 6 (1.2%) had VUR. VCUG revealed increased bladder wall trabeculation without PUV in 4 (11.4%) patients, ureterocele in 4 (11.4%) patients, and PUV in 3 (8.5%) patients.
A statistically significant correlation was found between HN grade and presence of VUR and between HN grade and VUR grade (VUR presence on the right kidney: P = 0.006; VUR presence on the left kidney: P = 0.033) (Fig. 2). The association of VUR and HN grades are shown in Table 4.
Incidence and grades of HN and grade of VUR.
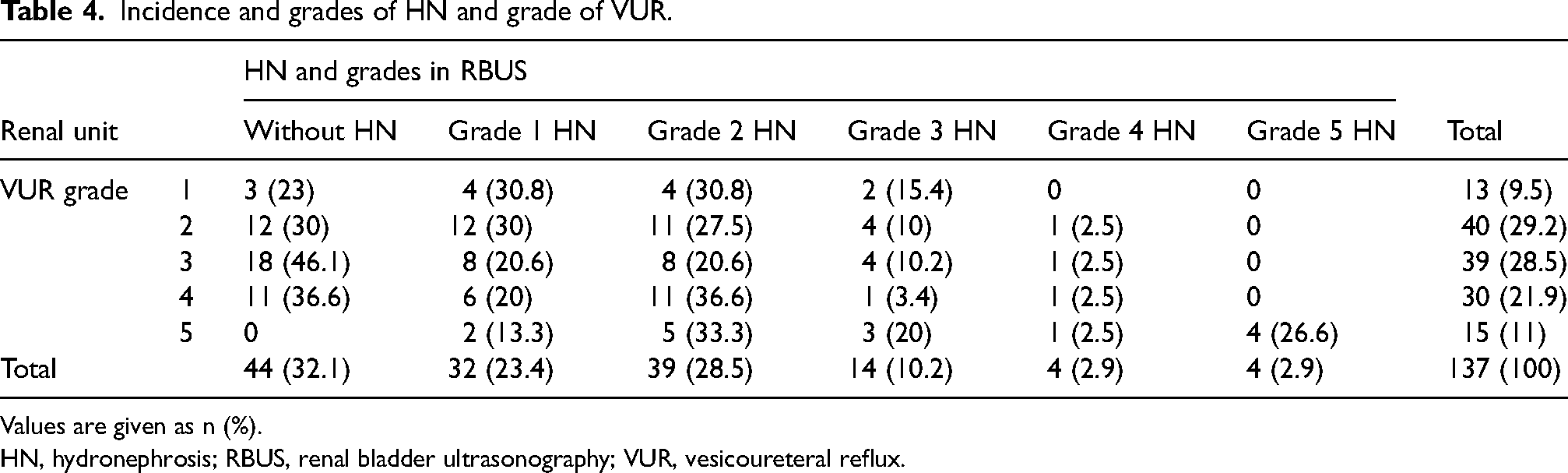
Values are given as n (%).
HN, hydronephrosis; RBUS, renal bladder ultrasonography; VUR, vesicoureteral reflux.
The correlation between UTI, VUR, and renal scarring
A DMSA scan was performed on 463 (88.9%) patients and renal parenchymal scarring was detected in 123 (26.5%) patients. Most of the patients with renal scarring (65.9%) were girls. The occurrence of renal scarring was statistically significantly higher in girls (P <0.001). Scarring on DMSA was observed in 20.8% of patients with low-grade VUR and 25.9% of patients with high-grade VUR. The risk of scarring on DMSA increased significantly with the progression of VUR grade in both boys and girls (P <0.001). Of the patients with renal scarring, 107 had a history of UTI (96 [78%] with recurrent UTIs). Scarring was detected by DMSA in the kidneys of 38 (12.3%) patients who had UTI but no VUR. Furthermore, 16 (13%) patients with scarring on DMSA had no UTI in their history or analysis.
Despite the presence of renal scarring on DMSA, nine cases of HN, three cases of ureteral dilations, two cases of possible renal scarring, one case of renal hypoplasia, and one case of ectopic kidney were revealed with RBUS in patients who had no experience of UTI. We detected VUR in 8 (50%) patients and PUV in 1 (6.3%) patient who did not have UTI using VCUG.
Moreover, VUR was found in 40 (11.7%) patients (grade 1, n = 2; grade 2, n = 13; grade 3, n = 12; grade 4, n = 9; grade 5, n = 4) whose DMSA was normal. DMSA scan showed that renal scarring was more commonly associated with high-grade VUR (P <0.001), female sex (P <0.001), older age (P <0.001), and history of recurrent UTIs (P <0.001). There was also a statistically significant correlation between renal scarring on DMSA and renal dysfunction (P = 0.007).
Discussion
In this study, the prevalence of reflux was 22.2% and was almost as high as suggested by Kopiczko (9). We demonstrated that high-grade HN on RBUS and detection of renal scarring on DMSA were significantly predictive risk factors for high-grade VUR, with the findings of the present study supporting previous research (10,11). We confirmed that recurrent UTI is associated with a greater prevalence of renal damage and more severe VUR (7,10–13). Furthermore, this study showed that children with renal scarring observed on DMSA were more likely to be older girls, have a history of UTI, have high-grade VUR, and have renal dysfunction.
The most common indication for the application of VCUG in our clinic is the investigation of recurrent UTIs in both sexes and all age groups, followed by congenital and/or acquired anomalies of the kidney and urinary tract. Our VCUG indications were similar to those reported in the literature (3,8–15). The incidence of VUR is significantly higher in children with UTIs and antenatal HN and patients with urinary tract anomalies compared with the general population (1,2,9).
In this study, VUR was detected in 21.1% of children with a history of UTI. In addition, the proportion of VUR was higher in children with recurrent UTIs (24.4%) than in children who had only one febrile UTI (12.1%). We found a significant relationship between both VUR presence and VUR grade with UTI. Our results showed a higher likelihood of detecting high-grade VUR in children evaluated for recurrent UTI, confirming that VCUG should be considered in children with recurrent UTIs (11–13,15–19). A study by Preda et al. detected VUR at a rate of 17.9% in infants aged <1 year who had UTI (16). Koçak et al. (17) reported detection rates of 18.3% in their studies of children who had recurrent UTIs. Similarly, a relationship between recurrent UTIs and VUR has been reported previously (10,11,16–19).
In the present study, VUR was also associated with abnormal RBUS. VUR was observed in 63.1% of children with ureteral dilatation, 33.8% of children with a duplex collecting system, 23% of children with renal scarring, 42.8% of children with a solitary kidney, and 31.4% of children with bladder anomalies. VCUG remains the modality of choice to obtain important information about the anatomical structure of children with abnormal RBUS findings (8,12,15,20). Symptomatic UTI presentation or abnormal RBUS results may lead to early diagnosis of the possibility of higher-grade VUR.
We observed a statistically significant relationship between the HN grade and both the presence and grade of VUR. We also found that 29/84 (34.5%) ureters with high-grade VUR did not have HN. VCUG is recommended for patients with obstructive uropathy who have experienced UTIs in follow-up (8,12,15,21,22). We found VUR in 11.1% of cases with antenatal HN, which is consistent with the range of 10%–20% reported in the literature (8,12,21,22). The application of VCUG should be more selective in cases of antenatal HN because of very low VUR detection even if there are UTIs, co-morbid additional findings, or severe obstructive uropathy findings. Voiding cystography may be recommended if there is a bilateral or persistent moderate or severe HN and/or ureteral dilation. The guidelines of the American Academy of Pediatrics (AAP) and National Institute for Health and Clinical Excellence (NICE) and recent studies recommend the application of VCUG in selected cases at risk of both VUR and progressive renal damage. In addition, NICE and The European Society of Pediatric Radiology guidelines recommend a hybrid of bottom-up and top-down approaches utilizing both DMSA and MCUG in selected cases (3,8,23).
One study reported that if NICE guidelines had been applied, then a significant number of children aged <3 years with a high degree of VUR, which may require surgical intervention, would have been missed (24). Tse et al. (25) reported that 25 ureteral refluxes and 22 renal scars would have been missed when NICE guidelines were used in 6-month-old infants with UTIs. Furthermore, the implementation of AAP guidelines will cause significant missed diagnoses and diagnostic delays (26,27).
This study identified varying degrees of reflux to 22 ureters that had normal findings on RBUS. Although routine VCUG is not recommended when RBUS findings are normal after a first febrile UTI (13), a normal RBUS is not sufficient to exclude a significant proportion of patients at risk for VUR. As a result, the NICE and AAP guidelines have faced considerable criticism (27–29).
Renal scarring was detected by DMSA in 29 (11.7%) children who had normal RBUS in our study. We also observed that presence of severe HN on RBUS and renal scarring on DMSA were statistically significant predictive risk factors for high-grade VUR in children with UTIs. Similar results were reported by Kopiczko and Hoberman (10,11). VUR is remarkably significantly associated with renal damage (7,18). However, 13% of our patients with renal scarring on DMSA did not have a history of UTI. This study found eight children with scarring on DMSA but no associated VUR. This finding can be explained by the presence of VUR, which had a spontaneous resolution. We showed that the normal RBUS findings did not exclude scarring presence on DMSA and also that the absence of scarring is not sufficient to exclude the diagnosis of VUR, consistent with the literature (13). The diagnosis of VUR may be missed in 5%–27% of cases when VCUG is not performed on patients who have a normal DMSA scan after UTI (30). A study reported that renal scarring was seen in 15/23 children without VUR (7). This study confirmed that RBUS alone may not be sufficient in determining the description of a renal scarring and VUR. We found children with scarring on DMSA showed a statistically significant association with high-grade VUR, female sex, older age, recurrent UTI, and renal dysfunction. Abnormal RBUS findings, fever, some uropathogens, older age, female sex, presence of VUR, and grade of VUR have a high risk for the development of renal scarring (31). Therefore, it is rational to consider performing a VCUG if a UTI is present in patients with a presence of severe abnormal findings on RBUS and scarring on DMSA.
We found VUR in 5/11 (45.5%) children with a diagnosis of MCDK. Although VCUG is recommended for patients with MCDK because of the 10%–30% probability of VUR in the contralateral kidney, some studies suggest VCUG only in the presence of concomitant UTIs (8,32). Our increased VUR rates can be explained by our VCUG application to MCDK patients accompanying UTI.
This study determined that consanguineous marriage was a risk factor for high-grade VUR. Primary VUR, which has a familial predisposition, is particularly low-grade and usually improves over time. Based on the available evidence, screening of asymptomatic siblings and offspring is not recommended unless there is an abnormal RBUS findings or a history of UTI. Families with VUR must be adequately informed about the increased risk of UTIs and VUR in siblings and future offspring compared to the general population (1,6).
None of our patients developed VCUG-related complications. Iatrogenic complications associated with VCUG, a relatively invasive procedure, are rare events. After VCUG, some complications have been reported in the literature, including urinary discomfort, contact dermatitis, allergic reaction, dysuria, hematuria, and bladder rupture (1,2,20). Most complications associated with VCUG are not critical. Antimicrobial prophylaxis and aseptic technique are recommended to prevent VCUG-related UTI (4,5).
The present study has some limitations. First, it was conducted retrospectively at a single hospital. Interpretation of diagnostic imaging tests was subjective, even if performed by experienced physicians. Second, the lack of experience with the sonographic diagnosis of VUR with contrast-enhanced VUS is another limitation of this study. However, it is known that reflux grading is more limited in VUS. The most commonly used grading system for reflux is the “International system of radiographic grading” (1). The reflux grading system is based solely on VCUG.
In conclusion, in this study, high-grade VUR was strongly associated with recurrent UTIs, scarring on DMSA, and high-grade HN findings on RBUS; our VCUG indications changed statistically significantly with increasing age. This study showed that there was a statistically significant correlation between the presence of scarring on DMSA, VUR grade, sex, age, history of UTI, and renal dysfunction. Our results suggest that VCUG should be recommended in cases of recurrent UTIs, abnormal findings on RBUS, or scarring on DMSA. The clinical indications for performing VCUG should focus on detecting high-grade VUR. However, recommendations for voiding cystography in children remain controversial. There is a need for prospective controlled clinical trials that assess a broad range of factors, including geographic characteristics, age, sex, individual susceptibility, innate immune response, causative pathogens, nitrite positivity, acute phase reactants, presence of fever, lower urinary tract symptoms, and the impact of imaging studies. Such trials should involve large, representative populations to guide evidence-based recommendations.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.