
Abstract
Background
Embolization plays a significant role in interventional radiology and modern medicine, intersecting with several specialties. The technological advancement of embolic agents has contributed to successful outcomes in the treatment of a wide range of diseases.
Purpose
To compare the histomorphological effects of Embosoft microspheres and Embosphere microspheres in uterine artery embolization (UAE) in sheep.
Material and Methods
Superselective and bilateral UAE was performed with Embosoft and Embosphere microspheres in 10 adult non-pregnant sheep. Embosoft microspheres with a diameter of 500–700 μm were compared with Embosphere microspheres of a similar diameter in two groups of five sheep each. One sheep was embolized only with non-ionic iodinated contrast solution and saline (SF0.9%). The evaluation was based on histopathological examination of the uterus, performed 7 days after embolization. Necrosis scores, the diameter of occluded arteries, and the number of particles were assessed. ANOVA test and Student's t-test were used to determine the differences between the study groups.
Results
The mean volume of embolic agents was 18.35 mL in the Embosphere group and 19.1 mL in the Embosoft group, with no statistically significant difference (P = 0.62). No significant difference was observed between the corresponding sides in the two groups. In addition, there were no significant differences in the thickness of the surface epithelium (Embosphere 21.26 μm vs. 19.72 μm Embosoft; P = 0.56) and glandular area between the groups (Embosphere 12.20% vs. 17.77% Embosoft; P = 0.18).
Conclusion
Embosoft micropheres were associated with a greater inflammatory response and a smaller area of degeneration compared to Embosphere microspheres.
Introduction
Uterine fibroids, or myomas, are the most common benign tumors in women of reproductive age. The main symptoms include heavy menstrual bleeding, abdominal pain, dyspareunia, and pelvic pressure, all of which impact the quality of life in approximately half of affected women (1,2). Conventional surgical approaches, such as hysterectomy or myomectomy, remain the treatment of choice for symptomatic cases, as they offer definitive management and eliminate the risk of recurrence. Embolization was first introduced in 1995 as a technique to reduce intraoperative bleeding during hysterectomy and has since gained recognition as a minimally invasive alternative to conventional surgery (3,4). Since the first published study on uterine fibroid embolization, various embolic agents have been employed, demonstrating clinical success and significant tumor size reduction (5).
Several studies have provided strong evidence supporting uterine artery embolization (UAE) as an effective alternative to hysterectomy or myomectomy. Notable trials include the Fibroids of the Uterus: Myomectomy versus Embolisation (FUME) study (6), the UK Randomised Study of Embolisation and Surgical Treatment for Uterine Fibroids (REST) (7), and the EMbolisation versus hysterectoMY (EMMY) trial (8), all of which established robust evidence for UAE as a viable alternative to surgery (1,3).
A variety of embolic agents are now available to interventional radiologists for use in UAE, reflecting advances in technology that have contributed to high technical and clinical success rates, along with favorable safety profiles. However, there is limited clinical evidence to determine the most effective embolic agent. Polyvinyl alcohol (PVA) and gelatin sponge remain the most commonly used agents, although newer calibrated particles have gained widespread use in fibroid embolization. These include PVA acrylamide microspheres (Beadblock; Biocompatibles UK Ltd., part of Boston Scientific Corp.); tris-acrylic gelatin microspheres (Embosphere; Biosphere Medical, Roissy, France); Polyzene F-coated hydrogel microspheres (Embozene; CeloNova Biosciences, Georgia, USA), and HydroPearl Microspheres (Terumo Interventional Systems, Tokyo, Japan) (5,9). Clinical outcomes across studies using these embolic agents have been largely comparable, with no single agent demonstrating clear superiority (5).
The aim of the present study was to compare the distribution of Embosoft microspheres (Scitech Produtos Médicos Ltd.) and Embosphere tris-acrylic gelatin microspheres (Biosphere Medical, Roissy, France) in the uterine arterial vasculature of sheep following uterine embolization. The comparison was based on histomorphological evaluation of different zones of the uterus. It was hypothesized that embolization with Embosoft micropheres would yield similar results to Embosphere, given that both are spherical particles of comparable caliber, despite being composed of different materials.
Material and Methods
Microspheres
The study was conducted at the University of São Paulo School of Medicine (FM-USP), São Paulo, SP, Brazil. This project was approved by the Animal Use Ethics Committee of the University of São Paulo School of Medicine on 10 October 2016, with approval of the document for research protocol no. 482/13.
Microspheres calibrated to 500–700 μm—specifically, tris-acrylic gelatin microspheres Embosphere microspheres (Biosphere Medical, Roissy, France)—were compared with 500–700-μm Embosoft microspheres (Scitech; Produtos Médicos Ltda). For both types, each vial contained 2 mL of microsphere sediment. To prepare the sediment, 10 mL of iodinated contrast medium and 10 mL of saline were added to each 2-mL syringe of microspheres, resulting in a total volume of 22 mL, composed of 50% contrast and 50% normal saline solution.
Animals
A total of 11 bilateral UAEs were performed on 11 Santa Inês sheep (Ovis aries) at the Animal Research and Experimentation Support Service, Heart Institute (InCor), São Paulo. In total, 22 uterine arteries were embolized. Each sheep received an intravaginal administration of 40 mg of progesterone 14 days before the UAE. One day before the procedure, all animals were administered 500 IU of equine serum gonadotropin (Folligon, MSD) intramuscularly to induce ovulation.
Ten sheep were randomly assigned to two treatment groups: five received Embosoft microspheres and five received Embosphere microspheres (Biosphere Medical, Roissy, France), both with a particle size of 500–700 µm. The 11th sheep underwent bilateral uterine artery catheterization but was embolized only with a non-ionic iodinated contrast solution and 0.9% saline.
The inclusion criteria were female, adult, nulliparous, and healthy sheep. The exclusion criterion was pregnancy.
Uterine artery embolization
The sheep were fasted for 24 h before UAE. Premedication consisted of intramuscular administration of midazolam (0.5 mg/kg) and ketamine (3 mg/kg). Anesthesia was induced with intravenous thionembutal (10–15 mL) and fentanyl, followed by orotracheal intubation and mechanical ventilation. Anesthetic maintenance was achieved with 2% inhaled isoflurane. In addition, all animals received prophylactic benzylpenicillin.
The common femoral artery was accessed via surgical dissection of the right inguinal region, and a 5-Fr valved introducer was inserted using the Seldinger technique. Using fluoroscopy and digital image acquisition (Pulsera; Philips BV, Eindhoven, the Netherlands), an initial pelvic arteriographic study was performed with a 5-Fr pigtail catheter positioned at the distal aorta, just above the aortoiliac bifurcation, to visualize the vascular anatomy.
Under fluoroscopic guidance, the left internal iliac artery was catheterized using a 5-Fr cobra-type catheter (Scitech Produtos Médicos Ltda, Goiânia, Goiás, Brazil). After arteriographic evaluation in posteroanterior and left oblique views, superselective catheterization of the left uterine artery was performed with a Vasco 21MP microcatheter (Balt Extrusion, Montmorency, France) and a 0.14-inch Choice PT2 guidewire (Boston Scientific, MA, USA). Immediate embolization of the left uterine artery was then carried out using Embosphere or Embosoft microspheres (500–700 μm). The same procedure was subsequently performed on the right side.
Embolizations were performed according to the predetermined randomization until stasis of the targeted vessels was achieved, marking the endpoint of the procedure, while carefully avoiding reflux into adjacent vascular structures. After UAE, the animals remained intubated and on mechanical ventilation until they had fully recovered from anesthesia. They were then extubated and transferred to individual pens.
All animals received water and food ad libitum and received appropriate veterinary care. Later, they were transferred to a commercial farm, where they remained for 6 days. Veterinary monitoring continued throughout the protocol, in compliance with Brazilian regulations governing the ethical use of animals in research.
Euthanasia
On day 7 after embolization, the animals were returned to the laboratory. After deep sedation, euthanasia was performed by intravenous injection of potassium chloride. Subsequently, total hysterectomies with bilateral adnexectomies were carried out.
Tissue specimens were collected from four distinct regions of the uterus: the myometrium adjacent to the insertion of the uterine artery, the fundic myometrium, the endometrium, and the ovarian hilum. Three tissue samples, each approximately 0.5 mm in size, were taken from each of these regions.
The collected specimens were sent to the Laboratory of Structural and Molecular Gynecology (LIM 58) in the Department of Gynecology, where they underwent histomorphological evaluation.
Histomorphological evaluation
The tissue samples were fixed in 10% buffered formalin for 48 h, followed by the standard histological processing steps: dehydration in ethyl alcohol, clearing with xylene, impregnation with liquid histological paraffin in an oven at 60°C, and embedding in paraffin at room temperature. The paraffin blocks containing the biological material were sectioned with a Microm HM315 R microtome set to produce 4-µm-thick sections. The sections were then placed in an oven at 60°C for 24 h to dry.
Subsequently, the slides were stained with hematoxylin and eosin (H&E) for histomorphological evaluation. Histological analysis was performed in a blind manner, i.e. the pathologist was unaware of the group assignment for each sample.
Statistical analysis
Statistical analysis was performed using SPSS version 18.0 (SPSS Inc., Chicago, IL, USA). ANOVA and Student's t-test were used for data analysis. All tests were two-tailed, and P <0.05 was considered statistically significant.
Results
A total of 22 vessels were catheterized: 10 were occluded with Embosphere microspheres (500–700 μm; Biosphere Medical, Roissy, France), 10 vessels were occluded with Embosoft microspheres (500–700 μm; Scitech Produtos Médicos Ltda), and two vessels were embolized with non-ionic iodinated contrast solution and 0.9% saline only.
Superselective and bilateral catheterization with flow-directed embolization of the uterine arteries was successfully achieved in all animals. No differences in arterial diameter were observed between the groups undergoing embolization with microspheres and the sham group. In addition, no catheter occlusion occurred with the use of calibrated microspheres.
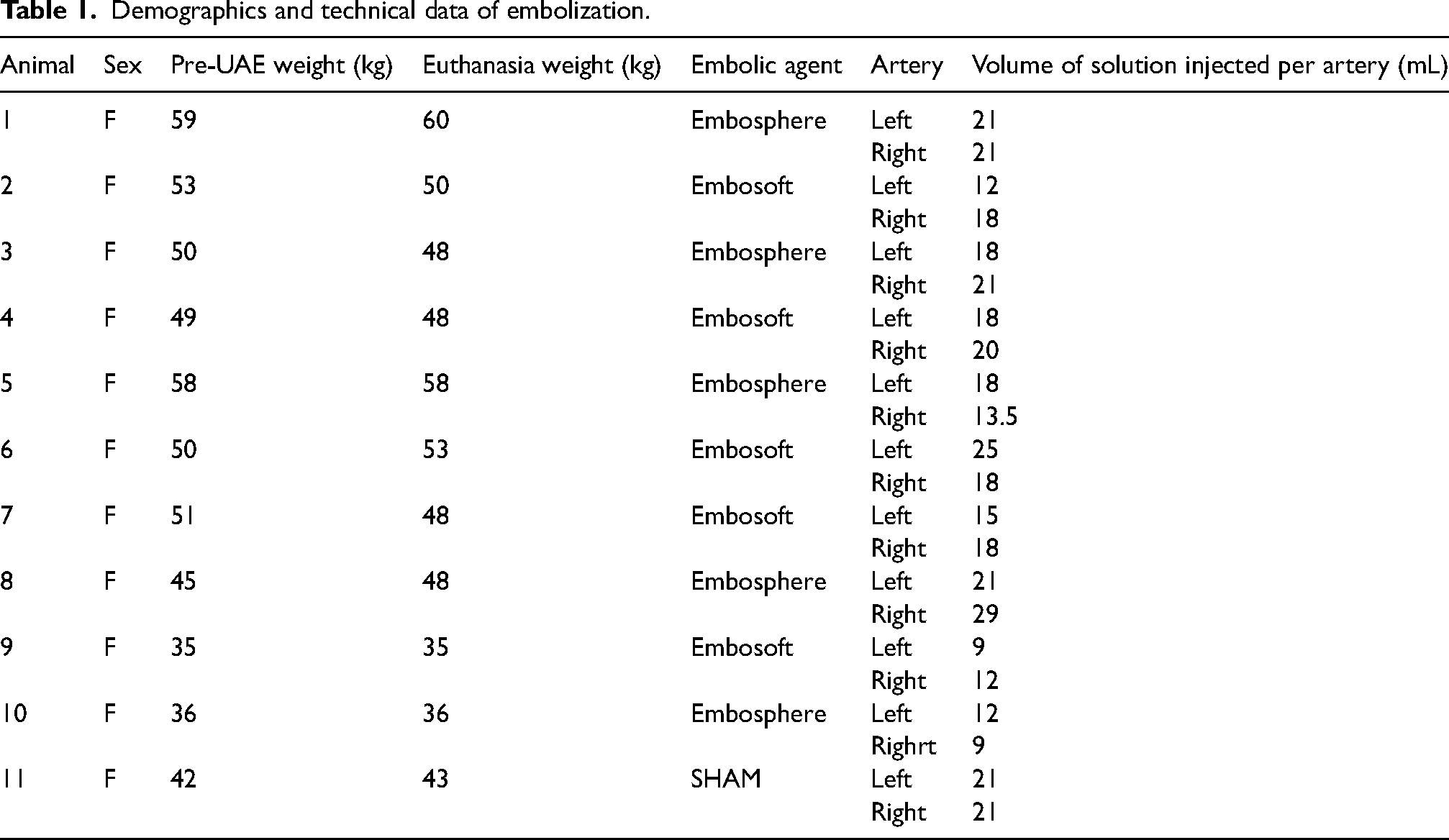
The mean volume of embolic agent in the Embosphere group was 18.35 ± 5.41 mL, while in the Embosoft group it was 19.1 ± 6.41 mL. A Student's t-test for two independent samples yielded a t-value of 0.39, with a P value of 0.62 and 18 degrees of freedom. As the P value (0.62) is greater than the significance level of 0.05, there was no statistically significant difference between the mean injected volumes of the two groups. Similarly, no statistical difference was observed when comparing the independent sides between groups. In the sham group, 21 mL of non-ionic iodinated contrast solution and 0.9% saline was injected on each side (Table 1).
Demographics and technical data of embolization.
Results of histological analysis
Morphological analysis of the endometrium between the groups
In all groups, the endometrial surface epithelium remained intact. There were no statistically significant differences in epithelial thickness between the groups (Embosphere 21.26 μm vs. 19.72 μm Embosoft; P = 0.56) or in glandular area (Embosphere 12.20% vs. 17.77% Embosoft; P = 0.18) (Figs. 1 and 2).
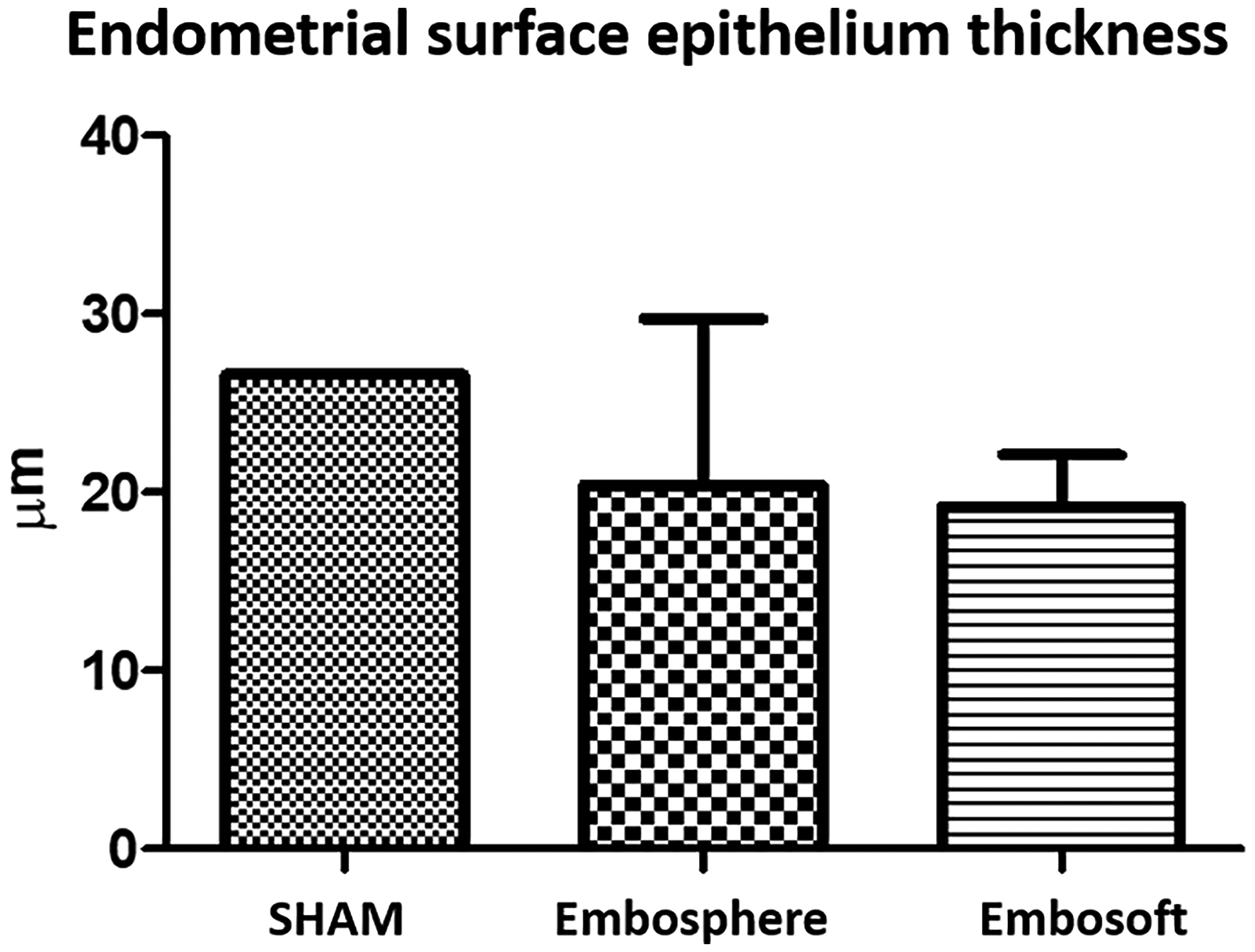
The graph represents the thickness of the endometrial surface epithelium and demonstrates the normal thickness found in the sham sheep (27.38 μm), and the thickness found in the two groups studied (Embosphere 21.26 μm vs. 19.72 μm Embosoft). It is noted that, although the thicknesses in the Embosphere and Embosoft groups were slightly reduced, there were no significant differences.
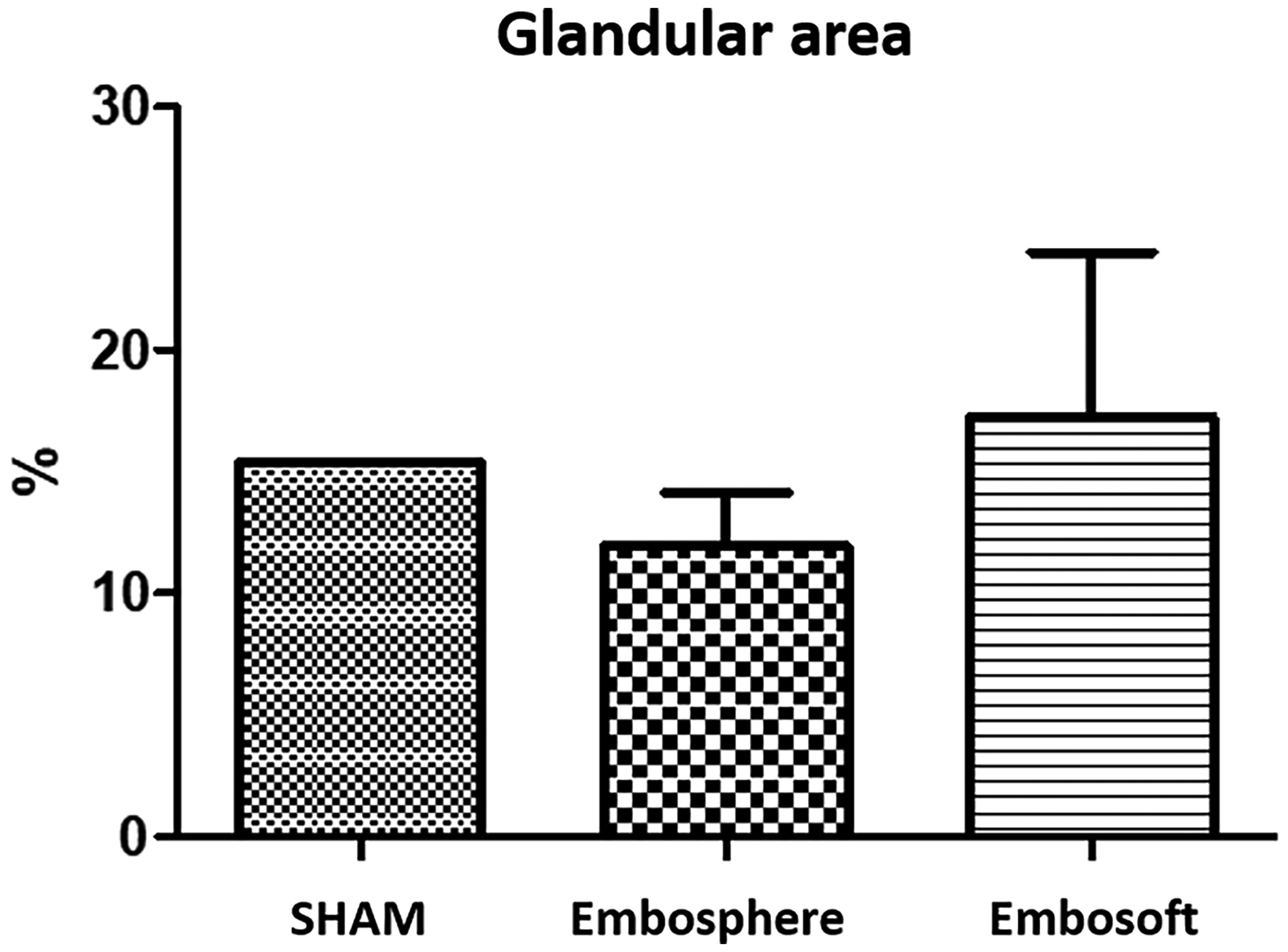
This graph shows that Embosoft preserved a larger area of glandular tissue; in other words, the embolization was less aggressive to the endometrial tissue. However, there were no significant differences between the groups (sham 15.92% vs. Embosphere 12.20% vs. 17.77% Embosoft).
In the sham group, the endometrial stroma appeared intact. In contrast, both the Embosphere and Embosoft groups showed poorly cellularized and faintly stained stromal regions near the myometrium. However, in the Embosoft group, more cellularized and intensely stained stromal areas were observed compared to the Embosphere group, suggesting a more advanced stage of tissue renewal. In addition, the Embosoft group exhibited a greater presence of leukocyte infiltrates and macrophages compared to the control group (Fig. 3). Despite myometrial injury, the endometrium across all groups showed features of recovery, with varying thicknesses in the superficial epithelium, glandular epithelium, and lamina propria.
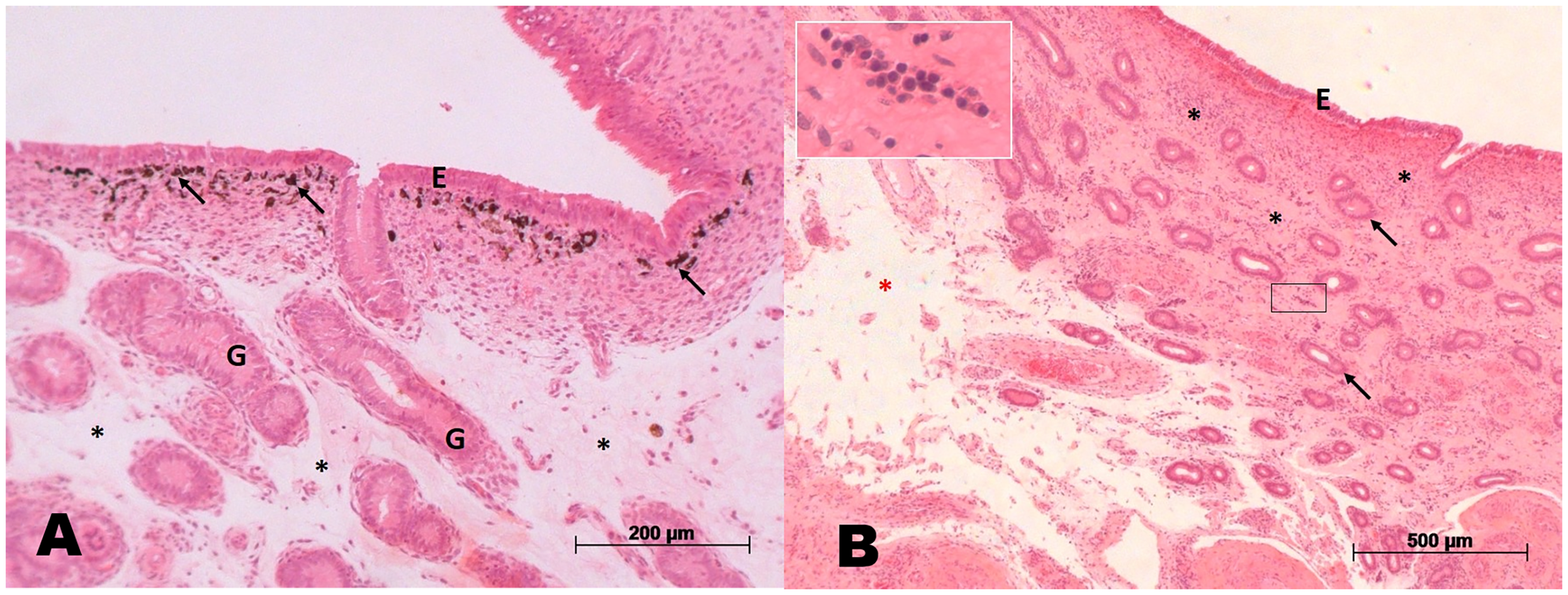
(A) Animal embolized with Embosoft. Note the presence of endometrium with a specific quantity of glands (G), amid a slightly stained and poorly cellularized stroma (asterisks). Presence of preserved superficial epithelium (E) and a large quantity of macrophages containing a pigment inside them just below the epithelium (arrows). (B) Animal embolized with Embosphere. Endometrium with signs of remodeling; intact surface epithelium (E); presence of glands (arrows) amid a more cellularized and stained stroma (asterisks). Some regions with poorly cellularized stroma (red asterisk). Also note the presence of a leukocyte infiltrate (arrows in the enlarged image), which represents the region demarcated with a rectangle). Magnification of the enlarged image: 400×.
Morphological analysis of the myometrium between the groups
The sham group showed preserved fundic and adjacent myometrium, with many smooth muscle fibers oriented in multiple directions. In the Embosphere group, areas of normal myometrium were observed alongside regions of hyalinization and degeneration in both the fundic and adjacent myometrium (Fig. 4). On the other hand, the Embosoft group also displayed some regions of normal myometrium but exhibited a greater extent of hyalinized and degenerated tissue in both the fundic and adjacent myometrium compared to the Embosphere group. In addition, macrophages and blood vessels were more frequently observed in the fundic and adjacent myometrial regions of the Embosoft group than in the other groups.
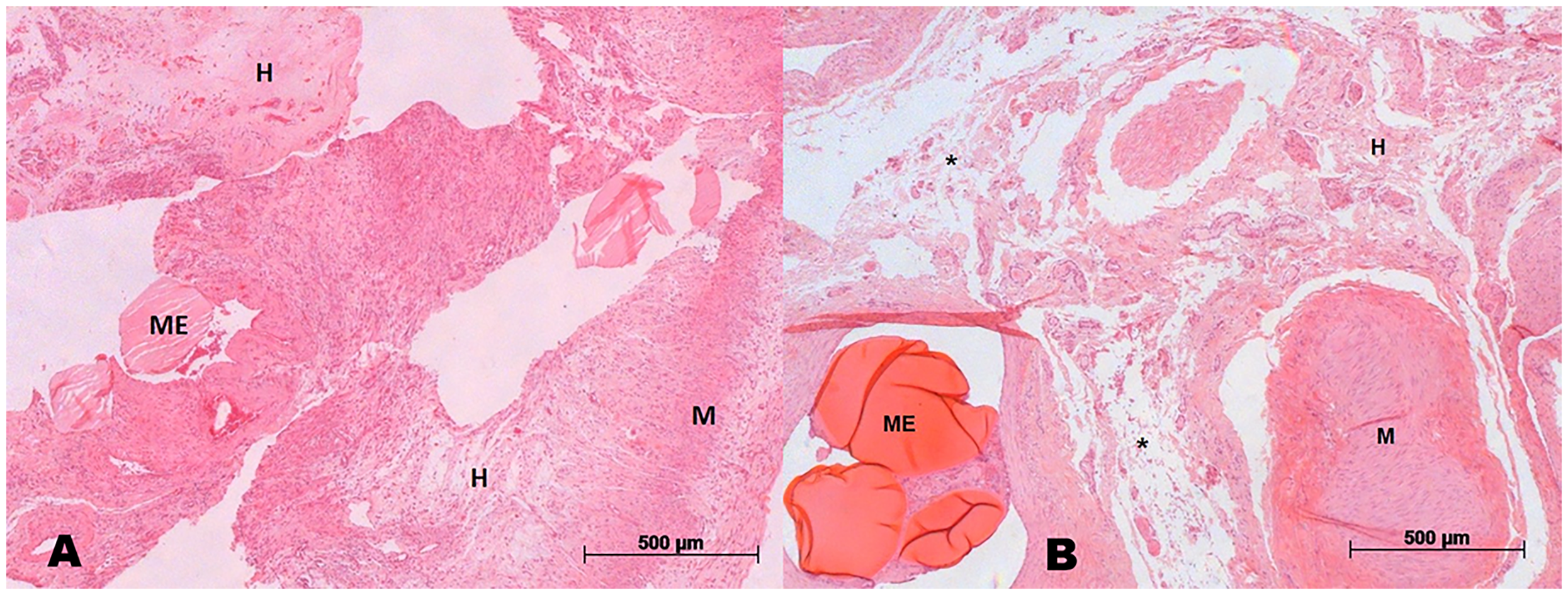
(A) Animal embolized with Embosoft. Fundic myometrium with few preserved regions (M) and large regions of hyalinized myometrium (H). Probable presence of microsphere (ME). (B) Animal embolized with Embosphere. Adjacent myometrium degenerated (asterisks) and hyalinized (H) for the most part, with very few preserved regions (M). Presence of microspheres (ME).
Morphological analysis of the ovarian hilum between the groups
No morphological differences were observed in the ovarian hilum among the evaluated groups. In all groups, ovarian follicles at different stages of development—primordial, primary, antral, and mature—were identified within a well-cellularized stroma. The presence of oocytes in mature follicles was likely due to the cutting plane. Atretic follicles, corpora albicans, and helicine arteries and veins were also present in the ovarian hilum across all groups.
Discussion
Uterine fibroids are the most common tumors affecting women of reproductive age, with prevalence increasing with age. Approximately half of affected women experience bothersome symptoms, such as heavy menstrual bleeding, abdominal pain, and pelvic pressure, which significantly impact quality of life (6). Although surgical interventions, namely myomectomy or hysterectomy, have long been the standard treatment for symptomatic fibroids, UAE emerged in the 1990s as a minimally invasive and effective alternative. UAE is now well-supported by a strong evidence base. Although PVA particles and spherical calibrated microspheres are frequently used embolic agents, no prior studies have directly compared Embosphere microspheres (Biosphere Medical, Roissy, France) and Embosoft microspheres (Scitech Produtos Médicos Ltda.) in uterine embolization. Despite advances in the development of spherical and calibrated particles, there remains a risk of unintended embolization, excessive tissue necrosis, or catheter blockage during the procedure.
In this study, no differences were observed in the degree of vascular penetration between Embosphere microspheres and Embosoft microspheres. In addition, Embosoft microspheres did not exhibit aggregation within the catheters, indicating better suspension homogeneity compared to Embosphere microspheres.
Although no differences were observed in the degree of particle penetration into the endometrium, the Embosoft group showed more stromal regions with increased cellularity and a greater presence of leukocyte infiltrate and macrophages compared to the control group. This suggests a more advanced stage of tissue regeneration and a more pronounced local inflammatory response. On the other hand, despite the heightened inflammatory reaction associated with Embosoft particles in both endometrial and myometrial regions, greater hyalinization and tissue degeneration were noted in the Embosphere group. These findings indicate that while both microspheres achieved similar levels of vascular occlusion, they elicited different degrees of local tissue response.
During UAE, awareness of potential utero-ovarian anastomoses is crucial. The choice of particle size is important to avoid complications such as ovarian failure or amenorrhea, as particles smaller than 500 µm may traverse these anastomoses and lead to non-target embolization. In this study, both Embosoft and Embosphere microspheres were within the same calibrated size range (500–700 µm), and no morphological alterations were observed in the ovaries. This supports the suitability and safe calibration of Embosoft microspheres for UAE procedures.
A variety of particulate embolic agents are available for UAE. In a systematic review and meta-analysis evaluating these agents, Embosphere demonstrated a higher percentage of fibroid devascularization compared to spherical PVA particles. No significant differences in clinical outcomes were observed among the other embolic agents, which may be attributed to the limited number of studies and the lack of standardization in UAE procedures (5). In addition, spherical particles have been shown to achieve deeper penetration into the vascular bed than PVA; however, this has not translated into statistically significant differences in clinical or technical outcomes (10). Therefore, standardization of UAE techniques should be encouraged to generate more consistent and comparable data, ultimately supporting evidence-based decision-making in the selection of embolic agents.
The present study has some limitations. One notable limitation is the lack of comparison with pathological uterine conditions, such as fibroids or adenomyosis, which would allow for assessment of uterine volumetric reduction and associated clinical outcomes. In addition, the small sample size may limit the generalizability of the findings.
In conclusion, this experimental model demonstrates a pathophysiological evaluation of UAE. Embosoft microspheres are associated with a greater inflammatory response and a smaller area of degeneration compared to Embosphere microspheres. Further clinical studies are warranted to compare Embosoft with other embolic particles.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.