
Abstract
Background
Differentiating benign from malignant thyroid nodules is essential for effective patient management.
Purpose
To evaluate the diagnostic performance of contrast-enhanced ultrasound (CEUS) for thyroid nodule characterization based on currently available evidence.
Material and Methods
We conducted a systematic review and meta-analysis of studies evaluating the diagnostic accuracy of CEUS for thyroid nodules. PubMed, Scopus, and Web of Science were searched through 31 March 2025. Studies using histopathologic or cytologic reference standards were included. Pooled estimates of sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy were calculated using random-effects models. Subgroup analyses and meta-regression were performed to explore potential effect modifiers. Studies evaluating contrast-enhanced computed tomography were included in the qualitative synthesis but were not incorporated into the quantitative meta-analysis.
Results
A total of 59 studies were included in the systematic review. Among these, 54 CEUS studies provided sufficient data for quantitative synthesis. CEUS demonstrated pooled sensitivity of 78.6% and specificity of 82.6%, with an overall diagnostic accuracy of 81.6%. Subgroup analyses indicated that examiner experience significantly influenced diagnostic performance, with higher sensitivity observed in studies involving more experienced operators. Meta-regression did not identify statistically significant independent associations between examined covariates and diagnostic outcomes.
Conclusion
The available literature indicates that CEUS demonstrates favorable diagnostic performance for differentiating benign from malignant thyroid nodules. Further prospective studies using standardized imaging protocols and reporting frameworks are needed to better define the role of CEUS in thyroid nodule evaluation.
Introduction
Thyroid nodules are a common clinical finding, with a prevalence exceeding 60% in the general population when assessed by high-resolution ultrasonography (1). Although the majority of these nodules are benign, approximately 5%–15% are malignant, necessitating reliable diagnostic strategies to distinguish between benign and malignant lesions to guide appropriate clinical management (2). Conventional ultrasound (US) remains the first-line imaging modality due to its accessibility and real-time evaluation of nodule morphology and vascularity (3). However, its diagnostic performance is limited by operator dependency and variability in image interpretation, particularly in nodules with indeterminate cytology (4).
To improve diagnostic characterization, advanced imaging techniques have been explored. Contrast-enhanced ultrasound (CEUS) utilizes microbubble contrast agents to dynamically evaluate the microvascular architecture of thyroid nodules in real time, allowing detailed assessment of lesion perfusion patterns (5–8). Previous studies have suggested that CEUS may aid in differentiating benign from malignant nodules by identifying irregular, heterogeneous, or hypoenhancing perfusion patterns associated with malignancy (9). As a result, CEUS has attracted increasing interest as a potential adjunct imaging modality in the evaluation of thyroid nodules.
In contrast, contrast-enhanced computed tomography (CECT) is primarily used for staging of thyroid malignancy rather than for primary characterization of thyroid nodules. CECT provides cross-sectional anatomical information that may assist in assessing extrathyroidal extension, mediastinal involvement, and cervical lymph node metastasis (5,6). Although some studies have explored CT-based features for differentiating benign from malignant nodules, its role in primary nodule characterization remains limited and heterogeneous.
Several previous meta-analyses have evaluated the diagnostic performance of CEUS in thyroid nodule assessment (9–11). However, variability across studies in imaging protocols, examiner experience, and methodological characteristics has resulted in heterogeneous findings. In addition, potential modifiers of diagnostic performance—such as examiner expertise, blinding procedures, and examination timing—remain insufficiently explored.
Therefore, the aim of the present study was to conduct a comprehensive systematic review and meta-analysis to evaluate the diagnostic performance of CEUS for differentiating benign from malignant thyroid nodules. In addition to estimating pooled diagnostic accuracy measures, we explored potential sources of heterogeneity through subgroup analyses and meta-regression. Evidence from studies evaluating CECT was summarized descriptively to provide contextual background within the broader imaging literature.
Material and Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines (12).
Eligibility criteria
Studies were eligible for inclusion if they met the following criteria: (i) enrolled patients with thyroid nodules confirmed by cytopathology or histopathology; (ii) evaluated CEUS or CECT for the assessment of thyroid nodules; (iii) reported diagnostic performance metrics or provided sufficient data to calculate sensitivity and specificity; and (iv) were observational studies (cohort, cross-sectional, or case–control), non-randomized interventional studies, or randomized controlled trials. Studies with fewer than 20 nodules, reviews, editorials, letters, conference abstracts, animal studies, and studies without sufficient data for analysis were excluded.
Information sources and search strategy
A comprehensive literature search was conducted on 31 March 2025, across three major databases: PubMed, Scopus, and Web of Science. Manual search of references through Google Scholar, citations, and journals was performed (13). The search strategy included combinations of keywords and MeSH terms related to “thyroid,” “contrast-enhanced,” “CT,” “ultrasound,” “sensitivity,” and “specificity.” The full search strategies for each database are provided in Table S1. No restrictions were applied with respect to language or publication year.
Study selection
All retrieved records were imported into EndNote (Clarivate Analytics) for de-duplication. Independent reviewers screened titles and abstracts for relevance. Full texts of potentially eligible studies were retrieved and assessed against the inclusion and exclusion criteria. Disagreements were resolved by consulting the senior researcher.
Data extraction
Data extraction was performed independently by two reviewers using a pre-piloted data extraction form. Extracted data included study characteristics (first author, year, country), study design, number of patients and nodules, imaging modality (CECT or CEUS), reference standard (histopathology or cytology), diagnostic performance metrics (true positives, false positives, true negatives, false negatives, sensitivity, specificity, positive predictive value [PPV], negative predictive value [NPV], and accuracy), as well as covariates such as examiner type (radiologist vs. non-radiologist), examiner experience (in years), and whether the examiner was blinded to the reference outcome, clinical information, or results of other imaging modalities where reported. Where reported, information on risk stratification frameworks (e.g. Thyroid Imaging Reporting and Data System [TI-RADS]) and diagnostic thresholds used to define malignancy were also extracted. Discrepancies were resolved by consensus.
Quality assessment
Methodological quality of included studies was assessed independently by two reviewers. Observational studies were evaluated using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (14). Non-randomized interventional studies were assessed using the ROBINS-I tool (15), while the included randomized controlled trial was evaluated using the Cochrane Risk of Bias 2 (RoB 2.0) tool (16). Each study was rated as good, fair, or poor quality based on predefined scoring criteria.
Data synthesis and statistical analysis
The primary objective of the quantitative synthesis was to estimate the diagnostic performance of CEUS for differentiating benign from malignant thyroid nodules. Therefore, pooled analyses were restricted to studies evaluating CEUS that provided sufficient data for quantitative synthesis. Studies evaluating CECT were retained within the systematic review and summarized qualitatively but were not included in the quantitative meta-analysis because of their limited number and heterogeneity in study objectives.
Pooled estimates of sensitivity, specificity, PPV, NPV, and diagnostic accuracy were calculated using random-effects models with restricted maximum likelihood (REML) estimation. Between-study heterogeneity was assessed using τ2, I2, and H2 statistics. Forest plots were generated to visualize pooled diagnostic estimates.
For each individual study, 95% confidence intervals (CIs) for sensitivity, specificity, PPV, NPV, and accuracy were computed using the normal approximation (Wald method) for proportions, based on binomial distribution. The standard error (SE) of each proportion was calculated as √[p(1−p)/n], where p is the proportion and n is the number of cases relevant to that metric. In studies with small sample sizes or proportions close to 0 or 1, resulting intervals were interpreted cautiously due to potential instability. All proportion estimates were expressed as percentages with corresponding 95% CIs.
Subgroup analyses were conducted to explore potential sources of heterogeneity, including examination timing (same-day vs. different-day imaging), examiner type, examiner experience (in years), and blinding status. Meta-regression analyses were performed using both univariate and multivariate models to evaluate the influence of these covariates on diagnostic performance. Regression coefficients and p-values were reported for each variable. A two-sided P value <0.05 was considered statistically significant.
All analyses were performed using STATA version 18.0 software (StataCorp LLC, College Station, TX, USA), employing the metan, metareg, and midas packages for diagnostic accuracy meta-analysis.
Results
Literature search results
A total of 1558 records were identified through database searches, including 369 from PubMed, 854 from Scopus, and 335 from Web of Science (Fig. S1). After removal of 585 duplicate records, 973 titles and abstracts were screened, of which 801 were excluded. A total of 172 reports were sought for retrieval and 153 full-text articles were assessed for eligibility. Of these, 93 reports were excluded due to lack of original data (n = 51), absence of CEUS or CECT evaluation (n = 6), or failure to report diagnostic performance data (n = 37).
Ultimately, 59 studies met the inclusion criteria and were included in the qualitative synthesis (5,17–74). Among these, 57 studies evaluated CEUS, of which 54 provided sufficient data for quantitative meta-analysis. Two studies evaluated CECT, and these were included in the qualitative synthesis but were not entered into the quantitative meta-analysis because the primary objective of the quantitative synthesis was to estimate the diagnostic performance of CEUS.
Baseline characteristics of included studies
The baseline characteristics of included studies are summarized in Table 1. Most evidence came from China (47 studies) with very few studies from Romania (n = 1), Germany (n = 1), and Italy (n = 1). In terms of design, 54 studies were retrospective cohort in nature, four were non-randomized studies, and one was a randomized trial. A total of 8855 patients (9720 nodules) were assessed, with 4482 benign and 4729 malignant nodules being investigated. The mean age of patients was 46.28 years. The examiners were radiologists in 36 studies and non-radiologists in 16 studies. However, detailed information regarding examiner subspecialty or expertise was inconsistently reported, particularly among CECT studies, precluding subgroup analysis based on observer characteristics. Six studies reported diagnostic performance using TI-RADS-based classification, with most defining malignancy as TI-RADS category ≥4. However, reporting was heterogeneous and insufficient for quantitative subgroup analysis. Reporting of image interpretation procedures, including independence of modality readings and blinding to results of other imaging modalities, was inconsistent across studies.
The baseline characteristics of included studies assessing the diagnostic accuracy measures of CECT and CEUS in thyroid nodules (benign vs. malignant)
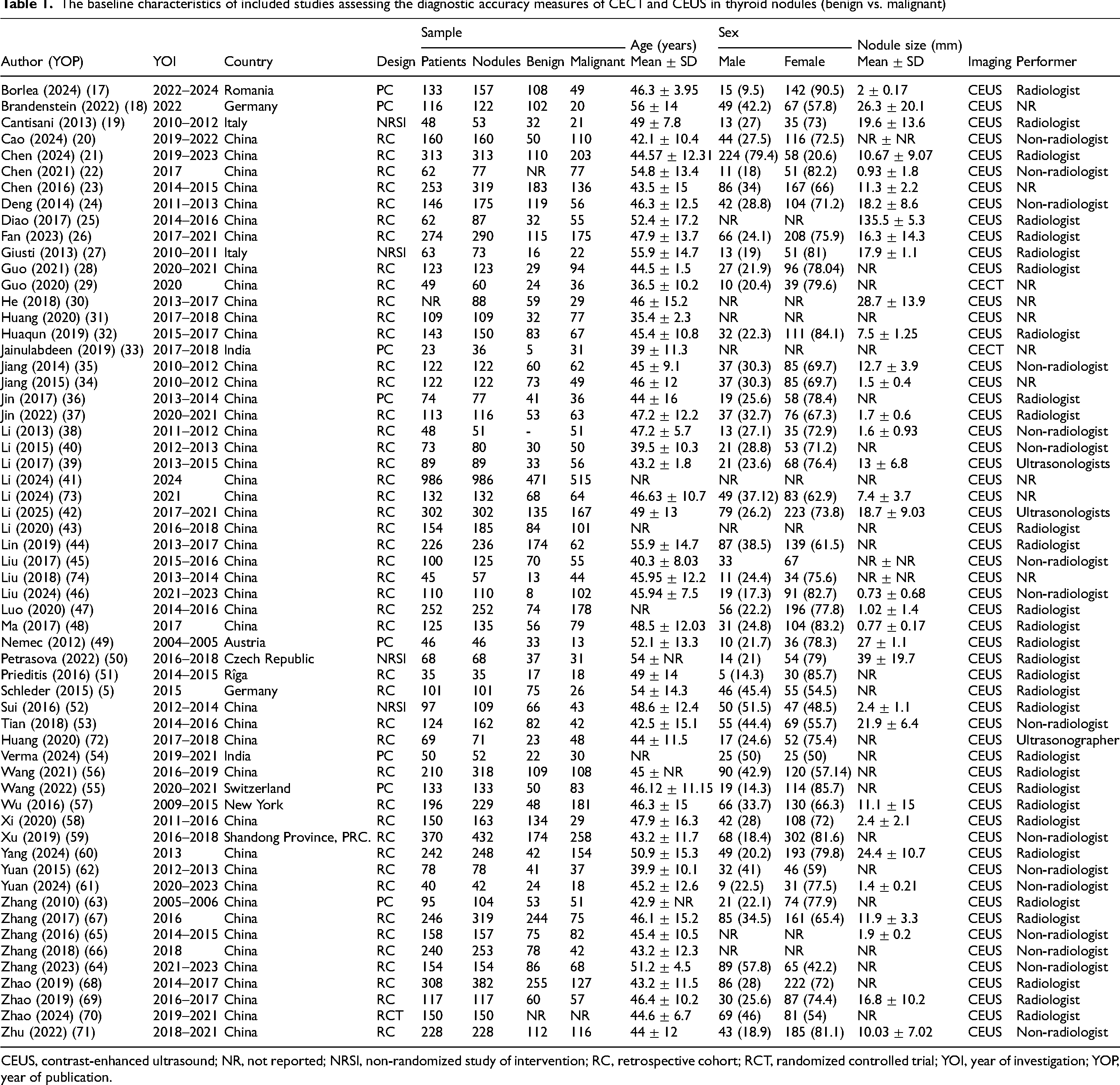
CEUS, contrast-enhanced ultrasound; NR, not reported; NRSI, non-randomized study of intervention; RC, retrospective cohort; RCT, randomized controlled trial; YOI, year of investigation; YOP, year of publication.
Methodological quality of included studies
Of the 54 included observational studies, 20 studies had fair quality and 34 studies had good quality based on the NIH quality assessment tool (Table S2). As for the four included non-randomized studies, they had overall moderate risk of bias. As for the sole randomized controlled trial included in this review, it had overall some concerns with its methodology.
Sensitivity of CEUS
Pooled results
The meta-analysis of 54 studies resulted in a pooled sensitivity of 78.60% (95% CI = 74.52–82.69, I2 = 95.58%) (Fig. 1). Although heterogeneity was considerable, the leave-one-out sensitivity analysis was unremarkable (Fig. S2). The funnel plot showed asymmetry, and Egger's coefficient showed significant publication bias (P <0.001) (Fig. S3).
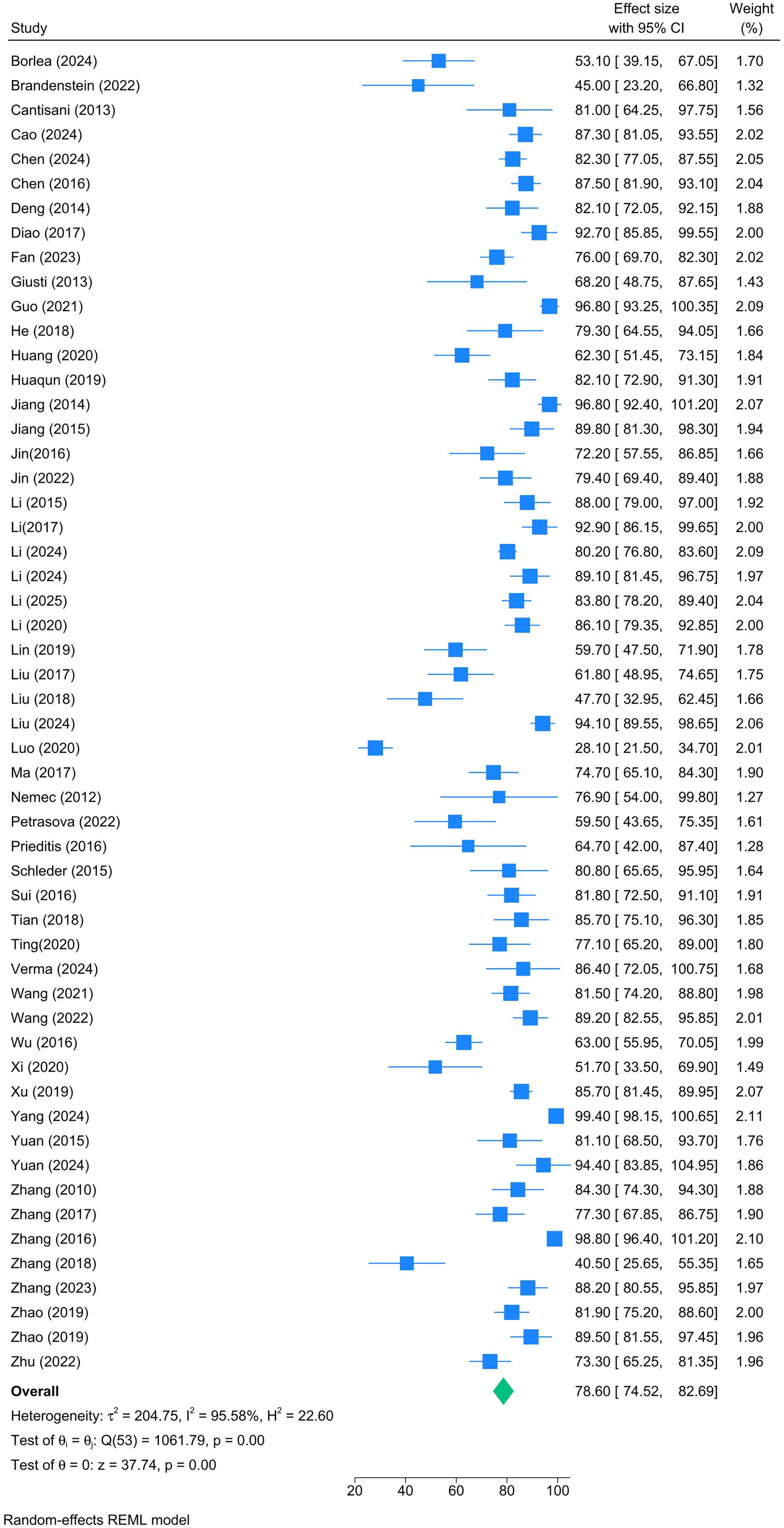
Forest plot showing the pooled sensitivity of contrast-enhanced ultrasound in differentiating benign and malignant thyroid nodules.
Subgroup analysis
A total of 31 studies contributed to the subgroup analysis (Fig. S4). Examiner's expertise was a significant effect moderator (P <0.001). Meanwhile, examination date (P = 0.90), examiner type (P = 0.88), and blinding of examiners (P = 0.23) revealed no significant effect modification. Radiologists with 20 years of experience showed the greatest sensitivity (two studies, 95.95%) while those with 10 years of experience had the lowest sensitivity (seven studies, 66.83%).
Meta-regression
In the adjusted model (Table 2), none of the examined covariates—including mean patient age, nodule size, number of nodules, timing of examination, examiner specialty, experience, or blinding—were significantly associated with sensitivity (P >0.05 for all).
Multivariate adjusted meta-regression analysis of the determinants of diagnostic accuracy measures
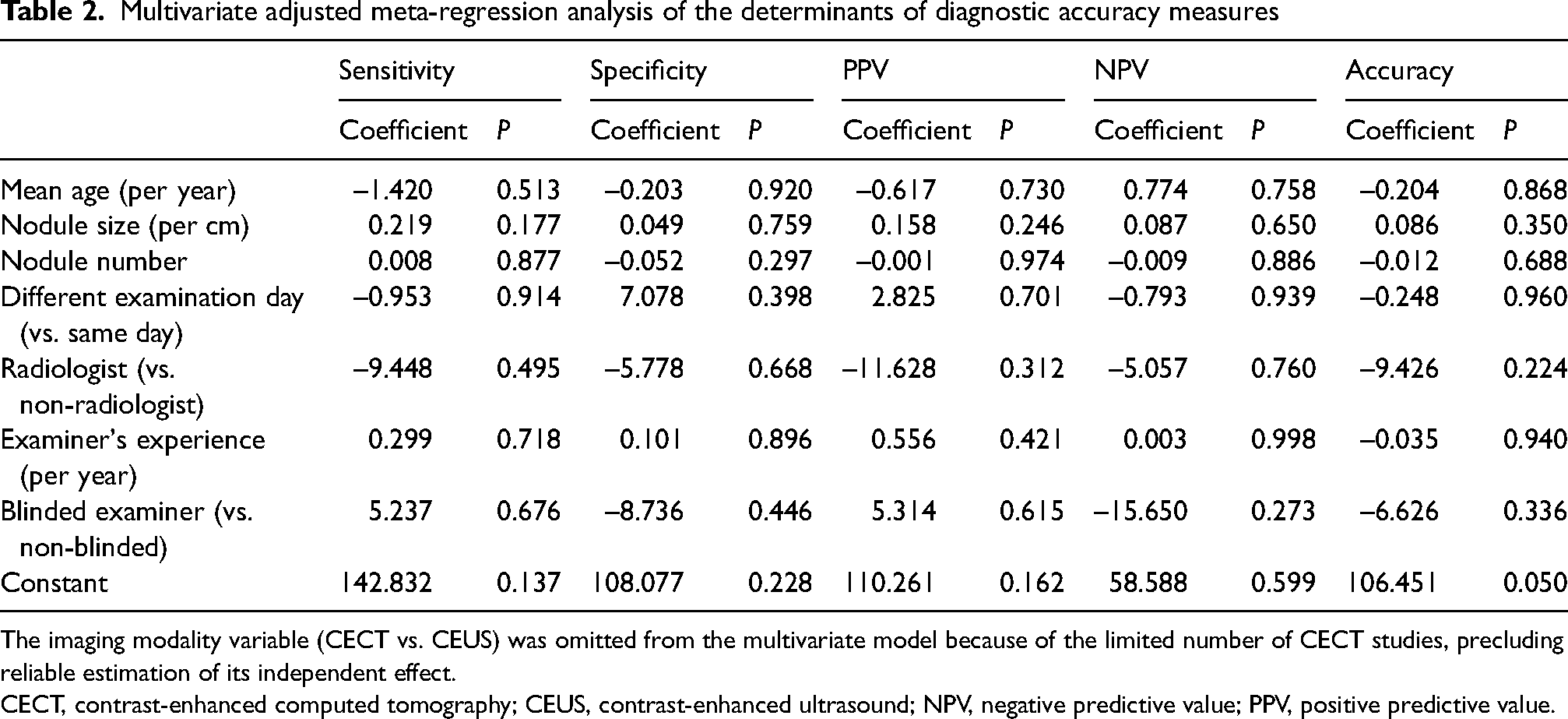
The imaging modality variable (CECT vs. CEUS) was omitted from the multivariate model because of the limited number of CECT studies, precluding reliable estimation of its independent effect.
CECT, contrast-enhanced computed tomography; CEUS, contrast-enhanced ultrasound; NPV, negative predictive value; PPV, positive predictive value.
Specificity of CEUS
Pooled results
The meta-analysis of 54 studies revealed a pooled specificity of 82.63% (95% CI = 79.09–86.17, I2 = 92.49%) (Fig. 2). Although heterogeneity was considerable, the leave-one-out sensitivity analysis was unremarkable (Fig. S5). The funnel plot showed asymmetry, and Egger's coefficient showed significant publication bias (P <0.001) (Fig. S6).
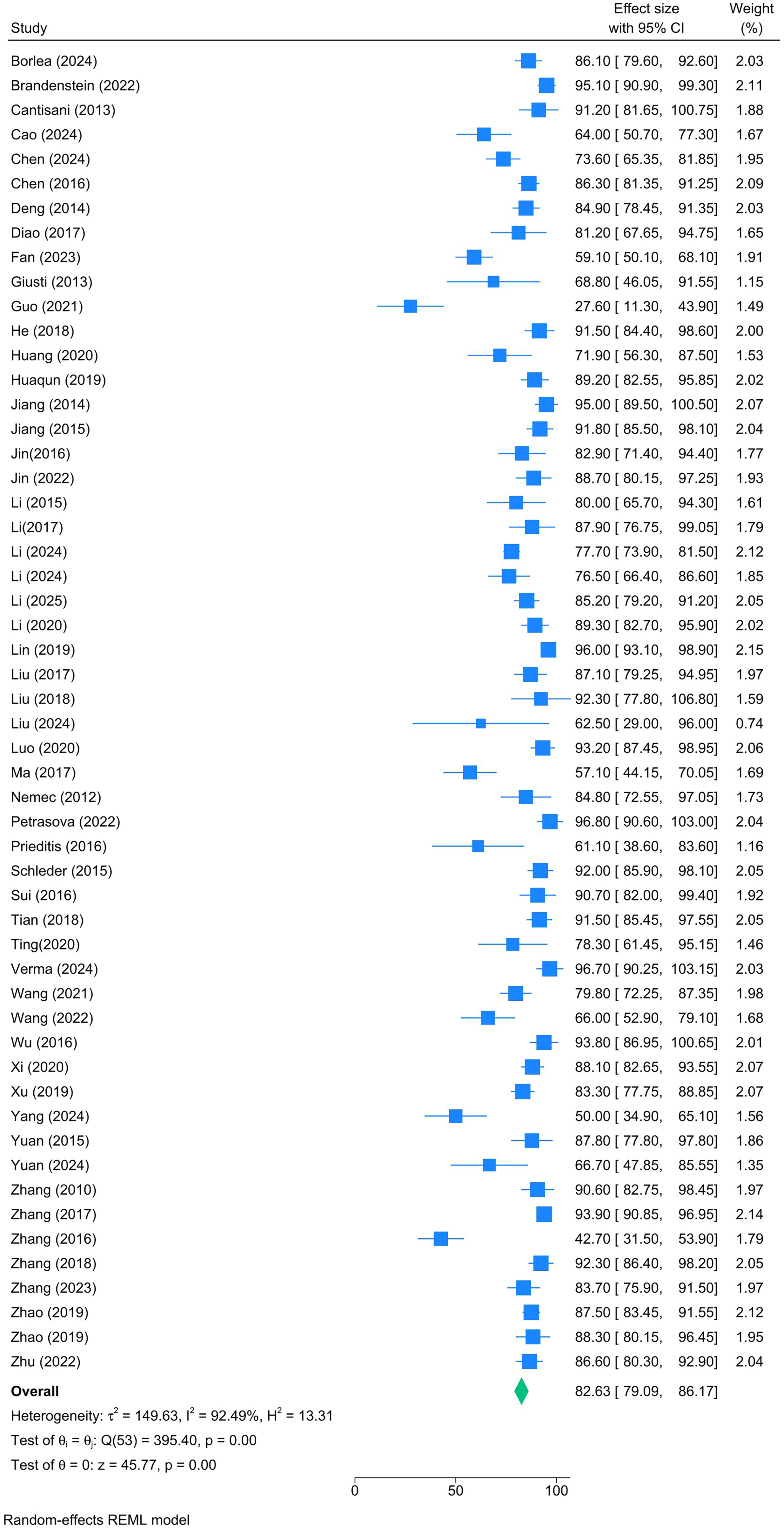
Forest plot showing the pooled specificity of contrast-enhanced ultrasound in differentiating benign and malignant thyroid nodules.
Subgroup analysis
In total, 31 studies contributed to the subgroup analysis (Fig. S7). Examiner's expertise was a significant effect moderator (P <0.001). Meanwhile, examination date (P = 0.85), examiner type (P = 0.68), and blinding of examiners (P = 0.46) revealed no significant effect modification. Radiologists with 9 years of experience showed the greatest specificity (one study, 96.70%) while those with 20 years of experience had the lowest specificity (two studies, 58.06%).
Meta-regression
In the multivariate-adjusted model, no significant associations were observed for any of the included covariates (Table 2). The directionality of effects for examiner blinding (coefficient = −8.736; P = 0.446) and radiologist status (coefficient = −5.778; P = 0.668) suggested lower specificity, but these did not attain statistical significance.
PPV of CEUS
Pooled results
The meta-analysis of 54 studies revealed a pooled PPV of 83.90% (95% CI = 81.58–86.23; I2 = 79.35%) (Fig. 3). Although heterogeneity was considerable, the leave-one-out sensitivity analysis was unremarkable (Fig. S8). The funnel plot showed asymmetry, and Egger's coefficient showed significant publication bias (P <0.001) (Fig. S9).
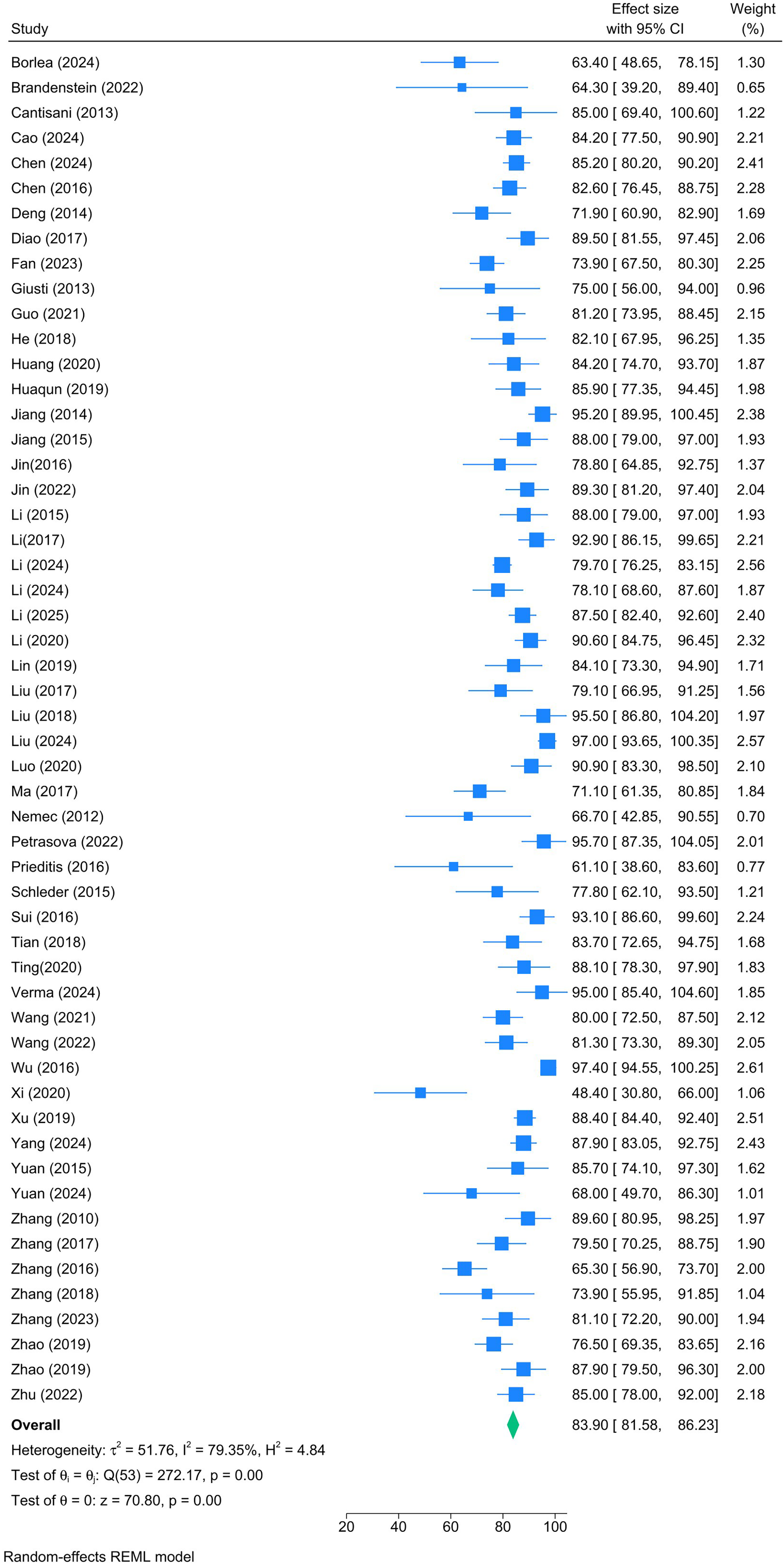
Forest plot showing the pooled positive predictive value of contrast-enhanced ultrasound in differentiating benign and malignant thyroid nodules.
Subgroup analysis
A total of 31 studies contributed to the subgroup analysis (Fig. S10). Examiner's expertise was a significant effect moderator (P <0.001). Meanwhile, examination date (P = 0.45), examiner type (P = 0.19), and blinding of examiners (P = 0.30) revealed no significant effect modification. Radiologists with 9 years of experience showed the greatest PPV (one study, 95.00%), while those with 12 years of experience had the lowest PPV (two studies, 69.52%). Notably, radiologists had insignificantly lower PPV compared to non-radiologists (83.85% vs. 89.13%).
Meta-regression
In the adjusted model (Table 2), none of the examined covariates—including examiner experience (coefficient = 0.556; P = 0.421) and blinding (coefficient = 5.314; P = 0.615)—were independently associated with PPV.
NPV of CEUS
Pooled results
The meta-analysis of 54 studies revealed a pooled NPV of 79.55% (95% CI = 75.49–83.61; I2 = 93.82%) (Fig. 4). Although heterogeneity was considerable, the leave-one-out sensitivity analysis was unremarkable (Fig. S11). The funnel plot showed asymmetry, and Egger's coefficient showed significant publication bias (P <0.001) (Fig. S12).
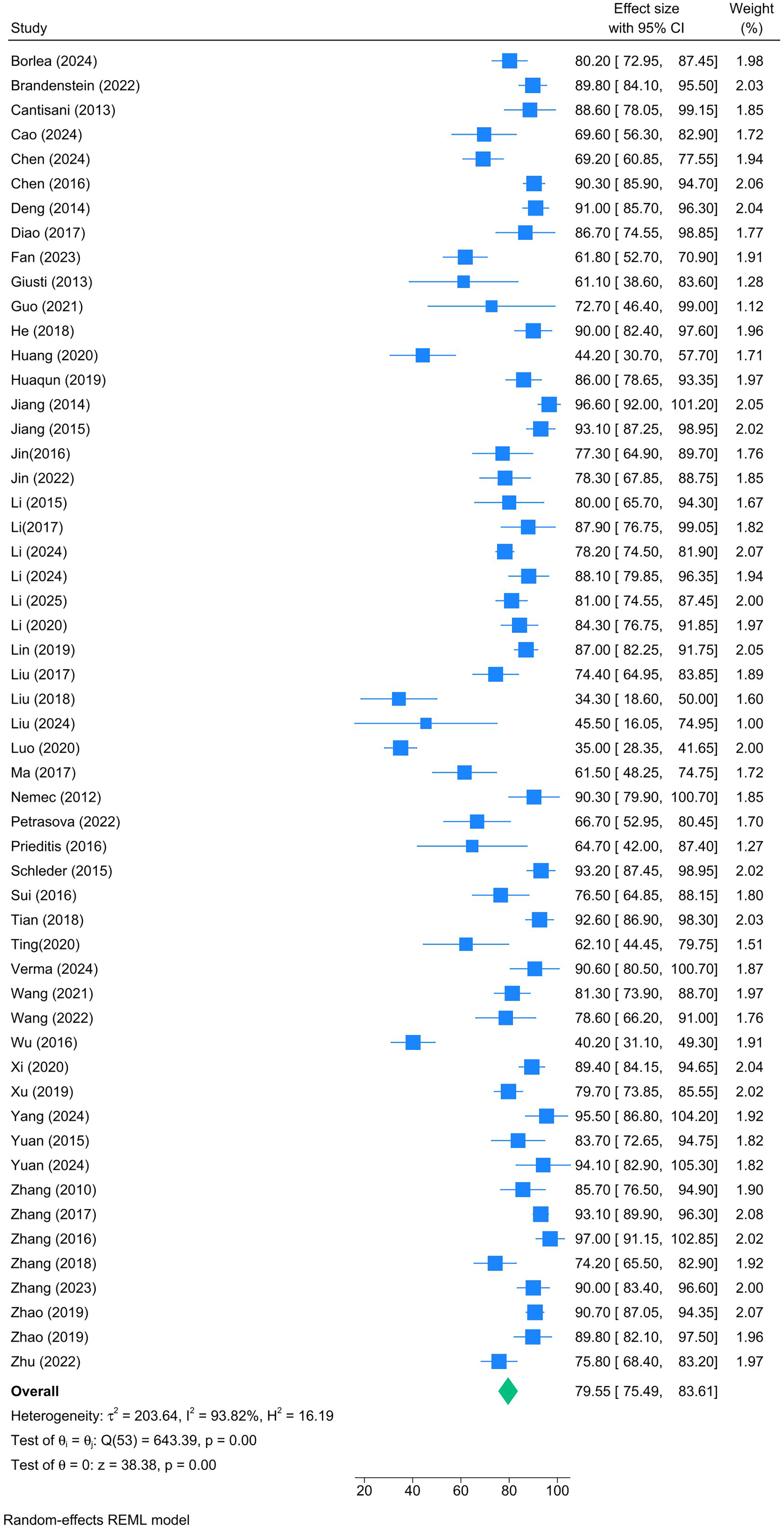
Forest plot showing the pooled negative predictive value of contrast-enhanced ultrasound in differentiating benign and malignant thyroid nodules.
Subgroup analysis
In total, 31 studies contributed to the subgroup analysis (Fig. S13). Both examiner's experience (P <0.001) and blinding of examiner (P = 0.04) were significant moderators of NPV. Specifically, radiologists with 1 year of experience showed the greatest NPV (one study, 93.10%) while those with 12 years of experience had the lowest NPV (two studies, 62.31%). Blinded examiners (20 studies, NPV = 74.09%, 95% CI = 66.26–81.92) had significantly lower NPV than non-blinded peers (11 studies, NPV = 83.83%, 95% CI = 78.89–88.76). Meanwhile, examination date (P = 0.83) and examiner type (P = 0.85) revealed no significant effect modification.
Meta-regression
Across the multivariate model, no covariate demonstrated a significant effect on NPV (Table 2). Notably, examiner blinding was associated with a large negative coefficient (–15.650; P = 0.273), suggesting a possible—but statistically non-significant—reduction in NPV with blinded assessments.
Diagnostic accuracy of CEUS
Pooled results
The meta-analysis of 54 studies revealed a pooled accuracy of 81.64% (95% CI = 79.26–84.02; I2 = 89.36%) (Fig. 5). Although heterogeneity was considerable, the leave-one-out sensitivity analysis was unremarkable (Fig. S14). The funnel plot showed asymmetry, and Egger's coefficient showed significant publication bias (P <0.001) (Fig. S15).
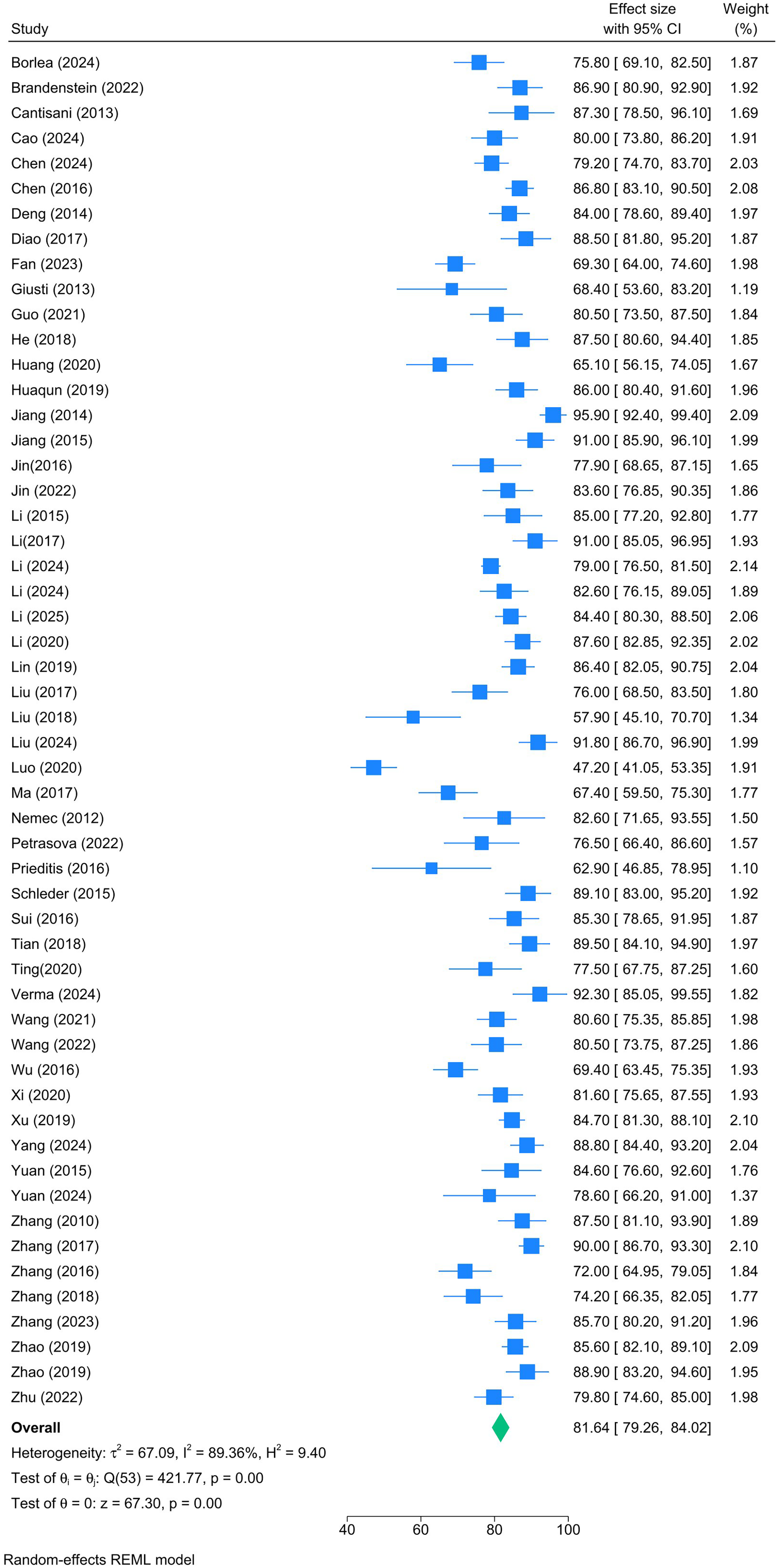
Forest plot showing the pooled accuracy of contrast-enhanced ultrasound in differentiating benign and malignant thyroid nodules.
Subgroup analysis
In total, 31 studies contributed to the subgroup analysis (Fig. S16). Examiner's experience was a significant determinant of CEUS accuracy (P <0.001). Radiologists with 9 years of experience showed the greatest accuracy (one study, 92.30%) while those with 12 years of experience had the lowest accuracy (two studies, 66.52%). Meanwhile, examination date (P = 0.74), examiner type (P = 0.33), and blinding of examiners (P = 0.23) revealed no significant effect modification.
Meta-regression
In the adjusted multivariate model (Table 2), none of the examined covariates reached statistical significance. The largest independent effect estimate was observed for blinding (coefficient = −6.626; P = 0.336), though again, this did not reach the threshold for statistical significance.
Narrative synthesis of studies reporting CECT
Two studies evaluating CECT were identified and included in the qualitative synthesis but were not incorporated into the quantitative meta-analysis due to the limited number of studies and the conceptual focus of the meta-analysis on CEUS.
Guo et al. (29) evaluated the diagnostic value of CECT texture and histogram analysis for differentiating benign from malignant thyroid nodules in a retrospective study of 49 patients with 60 nodules. The study reported that malignant nodules exhibited significantly higher entropy values compared with benign nodules (P = 0.005). Using an entropy cutoff value of 6.55, the reported diagnostic performance showed an area under the receiver operating characteristic curve of 0.716, with a sensitivity of 75.0% and specificity of 62.5% for distinguishing malignant from benign nodules.
Another prospective observational study evaluated the role of CECT in the preoperative assessment of differentiated thyroid carcinoma in comparison with ultrasonography and histopathology. In this cohort of 23 patients, CECT demonstrated a sensitivity of 52.4% and specificity of 66.7% for identifying malignant thyroid nodules (33). The study further emphasized that CECT was primarily useful for evaluating locoregional disease extent and cervical lymph node metastasis rather than primary nodule characterization.
Taken together, the available evidence suggests that although CECT may provide complementary information—particularly regarding tumor extent and nodal involvement—the current literature evaluating its role in primary thyroid nodule characterization remains limited.
Discussion
This systematic review and meta-analysis evaluated the diagnostic performance of CEUS for differentiating benign from malignant thyroid nodules based on currently available evidence. Across 54 studies included in the quantitative synthesis, CEUS demonstrated pooled sensitivity of 78.6% and specificity of 82.6%, with an overall diagnostic accuracy of 81.6%. These findings indicate that CEUS provides consistently favorable diagnostic performance for thyroid nodule characterization in the published literature.
The pooled diagnostic estimates observed in this analysis are broadly consistent with previous meta-analyses. For example, Yu et al. (75) reported pooled sensitivity and specificity of 85.3% and 87.6%, respectively, while Zhang et al. (6) documented sensitivity of approximately 87% and specificity of 83% with an area under the receiver operating characteristic curve of 0.926. Similarly, Sun et al. (76) reported pooled sensitivity and specificity of 88% and 90%, respectively. Taken together, these findings suggest that CEUS can provide reliable characterization of thyroid nodules, particularly through the evaluation of microvascular perfusion patterns that may differ between benign and malignant lesions.
One of the novel contributions of our study is the meta-regression analysis, which revealed that examiner experience significantly modulated sensitivity, specificity, PPV, and accuracy, particularly in CEUS studies. Notably, radiologists with ≥20 years of experience achieved markedly higher sensitivity levels (up to 95.95%), whereas mid-level experience (e.g. 10–12 years) was associated with lower sensitivity and specificity. These findings mirror the observations of Li et al. (11) and Nemec et al. (77), both of whom underscored the operator dependency of CEUS and the potential for variability in diagnostic accuracy based on user proficiency.
Blinding status also emerged as a significant moderator in subgroup analyses of NPV, with blinded examiners reporting significantly lower NPV. Although blinding is crucial to minimize bias, it may inadvertently limit contextual interpretation, particularly in CEUS where perfusion dynamics are subjectively assessed. This paradox echoes observations by Trimboli et al. (9), who suggested that clinical integration and anatomical familiarity may complement CEUS interpretation, despite theoretical blinding advantages.
Although a small number of studies evaluating CECT were identified during the systematic search, the available evidence was limited and heterogeneous. Consequently, CECT studies were included only in the qualitative synthesis and were not incorporated into the quantitative meta-analysis. Existing studies suggest that CECT may provide complementary information, particularly in the assessment of locoregional tumor extension and cervical lymph node involvement. For example, one study evaluating CECT texture analysis reported moderate diagnostic performance for distinguishing malignant from benign nodules, while another prospective study primarily examined the role of CECT in preoperative staging rather than primary lesion characterization (29,33). Taken together, these observations support the view that CT-based imaging is typically used as an adjunct modality in the evaluation of thyroid malignancy rather than as a primary tool for nodule characterization.
From a clinical perspective, CEUS may provide additional functional information beyond conventional US by allowing real-time visualization of microvascular perfusion patterns. Ding et al. (10) emphasized CEUS's value in identifying microcarcinomas and small nodules where conventional ultrasound and cytology often yield inconclusive results. This capability may be particularly useful in nodules with indeterminate morphological features on conventional US, where further characterization of vascular behavior could contribute to diagnostic assessment. Nevertheless, CEUS should be considered as a complementary imaging technique within the broader diagnostic pathway, which continues to rely on established approaches such as US risk stratification systems and cytological evaluation.
The present study has some limitations. First, although a large number of CEUS studies were included, only a small number of studies evaluated CECT, limiting the ability to examine CT-based diagnostic performance systematically. As a result, the present meta-analysis focuses primarily on CEUS evidence, and no direct statistical comparison between imaging modalities was performed. Second, the majority of included studies were conducted in China, which may limit the generalizability of the findings to other regions such as Europe and North America. Clinical practice patterns, imaging protocols, availability of CEUS, and guideline recommendations for thyroid nodule evaluation vary across healthcare systems. Differences in operator training, experience, and patient selection criteria may also influence diagnostic performance. Consequently, the pooled estimates reported in this meta-analysis may not fully reflect real-world practice in settings with different clinical workflows or regulatory environments. Third, despite subgroup analyses, substantial heterogeneity remained for several outcomes. This residual heterogeneity may reflect variability in imaging protocols, CEUS techniques, contrast agents, diagnostic thresholds, and study populations across included studies. Fourth, the availability of data reported according to standardized risk stratification systems such as the TI-RADS was limited. Only a small number of included studies evaluated diagnostic performance using TI-RADS-based thresholds, most commonly defining malignancy as category ≥4, and the heterogeneity of reporting precluded subgroup analysis. In addition, reporting of image interpretation procedures was inconsistent across studies, and the independence of readings between imaging modalities could not be consistently verified. Lack of standardized blinding or independent assessment may introduce diagnostic or observer bias. Finally, reporting of methodological characteristics such as examiner expertise, subspecialty training, and blinding procedures was inconsistent across studies. Limited reporting of these factors restricted the ability to fully evaluate their influence on diagnostic performance and highlights the need for more standardized reporting in future CEUS research.
In conclusion, the available literature indicates that CEUS demonstrates favorable diagnostic performance for the characterization of thyroid nodules. The pooled evidence suggests that CEUS can provide useful information for distinguishing benign from malignant lesions, although diagnostic performance may be influenced by operator experience and methodological variability across studies. Further prospective studies using standardized imaging protocols and reporting frameworks are needed to clarify the role of CEUS within the diagnostic pathway for thyroid nodules and to better define its integration with existing imaging and cytological evaluation strategies.
Supplemental Material
sj-docx-1-acr-10.1177_02841851261437491 - Supplemental material for Diagnostic performance of contrast-enhanced ultrasound for thyroid nodule characterization: a systematic review and meta-analysis
Supplemental material, sj-docx-1-acr-10.1177_02841851261437491 for Diagnostic performance of contrast-enhanced ultrasound for thyroid nodule characterization: a systematic review and meta-analysis by Xiang Huo, Jianlin He, Yijun Sun and Yanhong Ren in Acta Radiologica
Supplemental Material
sj-docx-2-acr-10.1177_02841851261437491 - Supplemental material for Diagnostic performance of contrast-enhanced ultrasound for thyroid nodule characterization: a systematic review and meta-analysis
Supplemental material, sj-docx-2-acr-10.1177_02841851261437491 for Diagnostic performance of contrast-enhanced ultrasound for thyroid nodule characterization: a systematic review and meta-analysis by Xiang Huo, Jianlin He, Yijun Sun and Yanhong Ren in Acta Radiologica
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.