
Abstract
Background
High-risk factors of lung adenocarcinoma (LUAD), including poorly differentiated pattern, lymphovascular invasion, visceral pleural invasion, lymph node metastasis, and spread through air spaces, are associated with poor prognosis.
Purpose
To construct and validate a combined model based on dual-energy computed tomography (DECT) for predicting high-risk LUAD in nodules with solid components.
Material and Methods
A total of 539 pathologically confirmed LUADs were retrospectively enrolled and were randomly divided into training (n = 377) and testing cohorts (n = 162) (ratio = 7:3). DECT quantitative parameters, conventional quantitative-semantic features, and clinical characteristics were collected. Univariable and multivariable logistic regression was used to construct the conventional CT model, DECT model, and combined model. Area under the curve (AUC) was used to evaluate diagnostic performance of models.
Results
The combined model (features: sex, diameter, pleural indentation, electron density in venous phase [Rho_V], and NIC_A [normalized iodine concentration in arterial phase]) showed significantly higher AUC than the DECT model (features: Rho_V and NIC_A) (0.899 vs. 0.870; P = 0.005) and the conventional CT model (features: diameter and pleural indentation) (0.899 vs. 0.742; P <0.001) in the training cohort. In the testing cohort, the combined model showed significantly higher AUC than the conventional CT model (0.852 vs. 0.704; P <0.001), but no significant difference in AUC was found between the combined model and the DECT model (0.852 vs. 0.838; P = 0.354).
Conclusion
The combined model based on DECT has good diagnostic performance in predicting high-risk LUAD in nodules with solid components.
Keywords
Introduction
Lung adenocarcinoma (LUAD) is the most prevalent histological type of lung cancer (1). High-risk factors of LUAD, including poorly differentiated pattern (2,3), lymphovascular invasion (LVI) (4), visceral pleural invasion (VPI) (5,6), lymph node (LN) metastasis (7), and spread through air spaces (STAS) (8), are associated with poor prognosis. Huang et al. suggested that segmentectomy lead to no difference in short-term oncologic outcomes between clinical stage IA3 and IA1-2 non-small cell lung cancer (NSCLC) (9). However, lobectomy and complete LN dissection could improve long-term prognosis compared with sublobar resection and incomplete LN dissection in small-sized LUAD (diameter ≤30 mm) with high-risk factors (10–15). Besides, high-risk LUAD with VPI and LN metastasis (stage over IB) could benefit from neoadjuvant immunotherapy plus chemotherapy, resulting in longer event-free survival and a higher rate of pathological complete response (16). Therefore, preoperatively differentiating high-risk LUAD may be useful for nodule management and prognostic prediction.
Dual-energy computed tomography (DECT), which can obtain virtual non-contrast (VNC) image and multiple quantitative parameters, including iodine concentration (IC), electron density (Rho), slope of the spectral curve (λHU), and effective atomic number (Zeff), is commonly used for diagnosing pulmonary nodules. The VNC image may have the potential to replace the true non-contrast (TNC) image in chest imaging for reducing radiation dose (17,18). Among the DECT quantitative parameters, the normalized IC (NIC) could differentiate malignant solid nodules (19,20), predict LVI in NSCLC (21), and distinguish STAS in solid LUAD (22). The Rho could predict the LUAD invasiveness in ground-glass nodules (GGNs) (23,24). The λHU could predict high-grade NSCLC (25) and solid/micropapillary predominant LUAD (26). In addition, conventional CT quantitative-semantic features could predict high-risk LUAD in part-solid and solid nodules (27) and differentiate the invasiveness of LUAD in GGNs (28). However, to our knowledge, no previous studies predicted high-risk LUAD by integrating DECT quantitative parameters and conventional CT quantitative-semantic features.
Pure GGNs rarely have high-risk factors because of their indolent nature (29–33). Therefore, the aim of the present study was to construct and validate a combined model based on DECT integrating DECT quantitative parameters and conventional CT quantitative-semantic features in predicting high-risk LUAD in nodules with solid components.
Material and Methods
Patients
The Ethics Committee of Sichuan Cancer Hospital approved the retrospective study (ethical number: SCCHEC-02-2021-088, approval year: 2021) and the requirement for informed consent was waived. A total of 802 patients who underwent contrast-enhanced DECT between April 2021 and April 2025 were retrospectively enrolled. Inclusion criteria included the following: (i) pulmonary nodules (diameter ≤3 cm) with complete surgical resection; (ii) pathological diagnosis with LUAD; (iii) DECT examination within 14 days before surgery; and (iv) complete pathological data. The exclusion criteria were as follows: (i) pure GGNs; (ii) received anti-cancer treatment before DECT; (iii) poor image quality; and (iv) a history of other malignant tumors. The nodule with the largest diameter was selected for analysis when the patient had several resected nodules.
Finally, our study included 539 patients. All nodules were randomly divided into training (n = 377) and testing cohorts (n = 162) at a 7:3 ratio (Fig. 1).
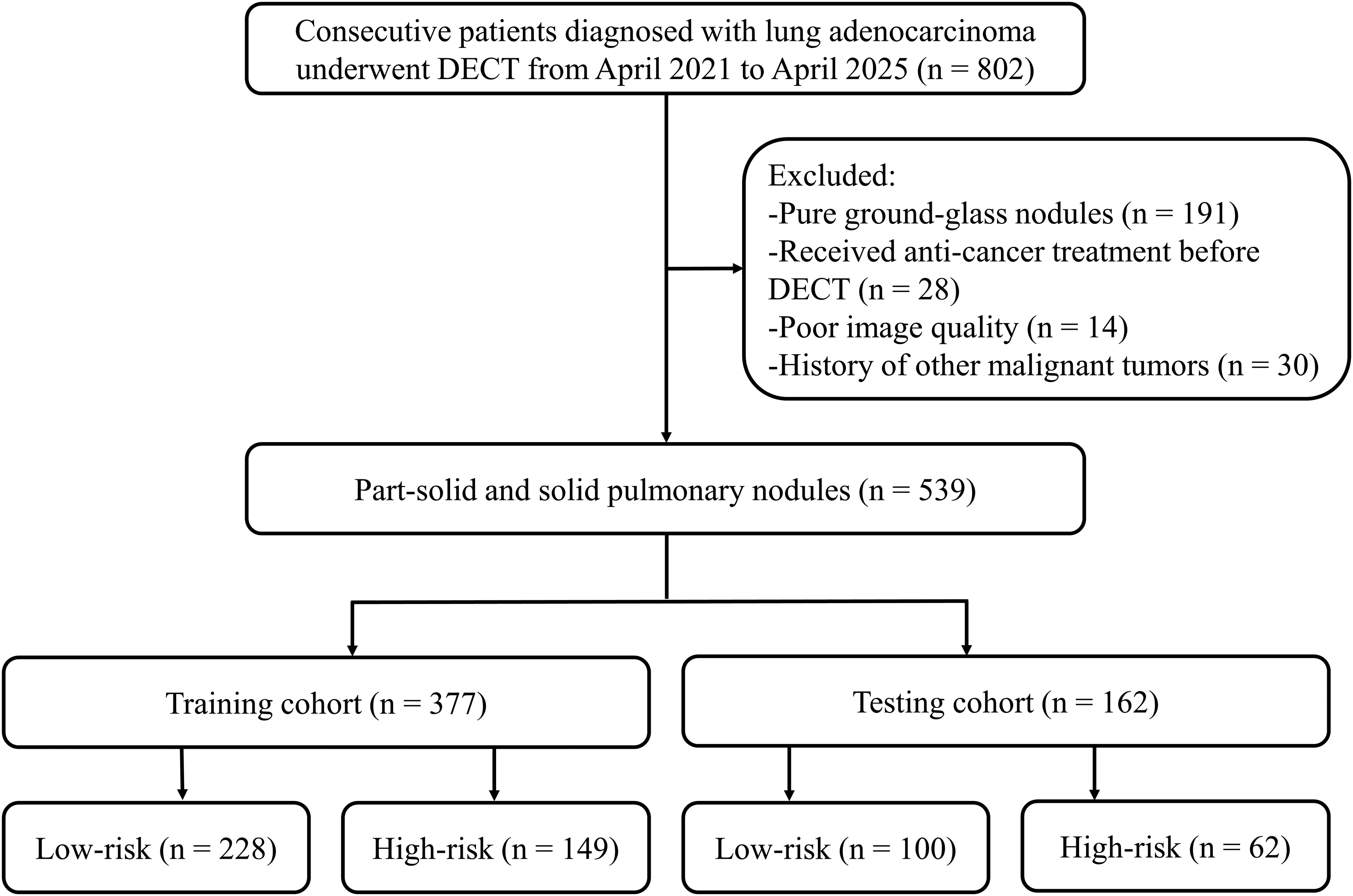
The flow chart of nodules selection. DECT, dual-energy computed tomography.
Image acquisition
All contrast-enhanced DECT examinations were carried out with dual-source CT (Somatom Definition Flash; Siemens Healthcare, Forchheim, Germany). A contrast agent of 80–90 mL (370 mg I/mL) was administered through the median cubital vein (2.5–3.0 mL/s), followed by 30–40 mL of saline (2.5–3.0 mL/s). All contrast-enhanced DECT of the chest was performed using the bolus-tracking method. When the threshold of the ascending aorta at the pulmonary trunk layer reached 100 HU, the arterial phase was initiated with a delay of 5 s. Then, the venous phase was initiated 30 s after the arterial phase.
The scanning parameters were as follows: reference current = 205/87 mAs; tube voltage = 80/Sn140 kV; pitch = 0.55; collimation = 64 × 0.6 mm; and rotation time = 0.28 s. The automated tube current modulation (CARE Dose 4D) was activated in this study.
Image reconstruction
The VNC image, which was used to assess the conventional CT quantitative-semantic features, was reconstructed using DECT data from the arterial phase, while the virtual monoenergetic image series (40 and 100 keV) were reconstructed using DECT data from the arterial and venous phases on a commercial workstation (SyngoVia VB40; Siemens Healthcare). The reconstruction parameters were as follows: iterative algorithm = SAFIRE (strength level 4); matrix = 512 × 512; reconstruction kernel = Q30f; field of view = 350 × 350 mm; slice thickness = 0.5 mm; and slice increment = 0.5 mm.
Conventional CT quantitative features
All nodules were automatically detected and segmented using an artificial intelligence (AI) platform (United Imaging Healthcare) based on deep learning algorithms (34). All segmentation results were also evaluated by two thoracic radiologists (JL and HQ, with 7 and 12 years of experience, respectively) in the lung window (level = −500 HU; width = 1500 HU). No manual adjustments were conducted due to the excellent segmentation results, even in the nodules with complex margins and adjacent vessels. The criteria for satisfaction were as follows: the segmentation included complete pulmonary nodules, while avoiding vessels and adjacent structures.
The AI-derived quantitative features of nodules, including axial maximal diameter, axial perpendicular diameter, mean attenuation, and volume, were recorded. The diameter was calculated with the formula: diameter = (axial maximal diameter + axial perpendicular diameter)/2. The axial maximal diameter of the solid component was manually measured by the aforementioned two radiologists. The consolidation:tumor ratio (CTR) was calculated with the formula: CTR = axial maximal diameter of the solid component/axial maximal diameter of the nodule.
To evaluate the performance of AI in automatically segmenting nodules, a senior thoracic radiologist (PZ, with 27 years of experience) selected 75 nodules for manual segmentation. Then, the inter-observer reproducibility of diameter, mean attenuation, and volume assessed by AI and the senior radiologist was evaluated.
Conventional CT semantic features
Two thoracic radiologists (JL and HQ, with 7 and 12 years of experience, respectively) who were blinded to histopathological results assessed the following semantic features: nodule type, spiculation, lobulation, air bronchogram, pleural indentation, pseudocavity, and vascular convergence sign (35). When the assessment results of the two radiologists were inconsistent, a senior thoracic radiologist (PZ, with 27 years of experience) resolved the disagreement.
DECT quantitative parameters
Two thoracic radiologists (JL and HQ, with 7 and 12 years of experience, respectively) placed circular regions of interest (ROIs) on the nodule and the aorta on the axial slice, which shows the maximum diameter of nodule. The circular ROIs were drawn as large as feasible while avoiding vessels, adjacent structures, and artifacts. The Zeff, Rho, IC (ICnodule), attenuation of 40 keV (Attenuation40keV), and attenuation of 100 keV (Attenuation100keV) of the nodule and IC of the aorta (ICaorta) were recorded. Then the λHU and NIC were respectively calculated with the formulas (25): λHU = (Attenuation40keV–Attenuation100keV)/60, NIC = ICnodule/ICaorta. Finally, a total of eight DECT quantitative parameters, including Zeff, Rho, NIC, and λHU in the arterial phase (Zeff_A, Rho_A, NIC_A, and λHU_A) and the venous phase (Zeff_V, Rho_V, NIC_V, and λHU_V), were recorded. The representative images were presented in Fig. 2.
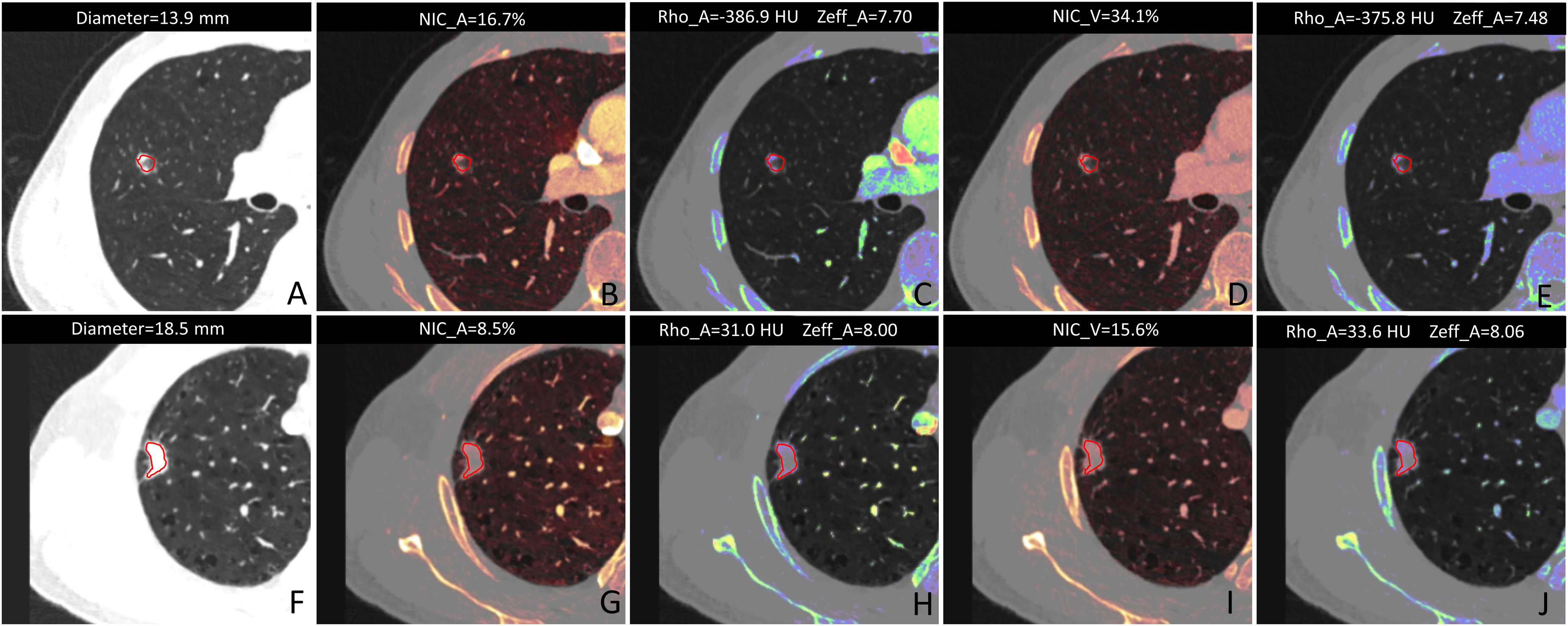
The representative DECT images of nodules. (a–e) A 55-year-old man with low-risk LUAD manifesting as part-solid nodule without pleural indentation. (f–j) A 44-year-old man with high-risk LUAD manifesting as solid nodule with pleural indentation. The high-risk LUAD showed higher diameter, Rho_A, Rho_V, Zeff_A, and Zeff_V, and lower NIC_A and NIC_V than the low-risk LUAD. A, arterial phase; DECT, dual-energy computed tomography; LUAD, lung adenocarcinoma; NIC, normalized iodine concentration; Rho, electron density; V, venous phase; Zeff, effective atomic number.
Reproducibility of manual quantitative parameters
A total of 75 nodules in this study were randomly selected for the reproducibility analysis. For inter-observer reproducibility, the CTR and DECT quantitative parameters were independently measured by two radiologists (JL and HQ, with 7 and 12 years of experience, respectively). For intra-observer reproducibility, the CTR and DECT quantitative parameters were measured again by a radiologist (JL) after 1 month.
Histopathological evaluation
All pathological diagnoses were obtained based on the classification of lung tumors (36). The high-risk factors in invasive adenocarcinomas were as follows: (i) poorly differentiated pattern (grade 3), which has ≥20% high-grade pattern, including micropapillary, solid, cribriform, and complex glandular patterns; (ii) LVI; (iii) VPI; (iv) LN metastasis; and (v) STAS. All LUADs were divided into a low-risk group (including invasive adenocarcinomas without high-risk factors and minimally invasive adenocarcinomas) and a high-risk group (including invasive adenocarcinomas with any of the high-risk factors) (Table 1).
Demographic and conventional CT features of nodules.
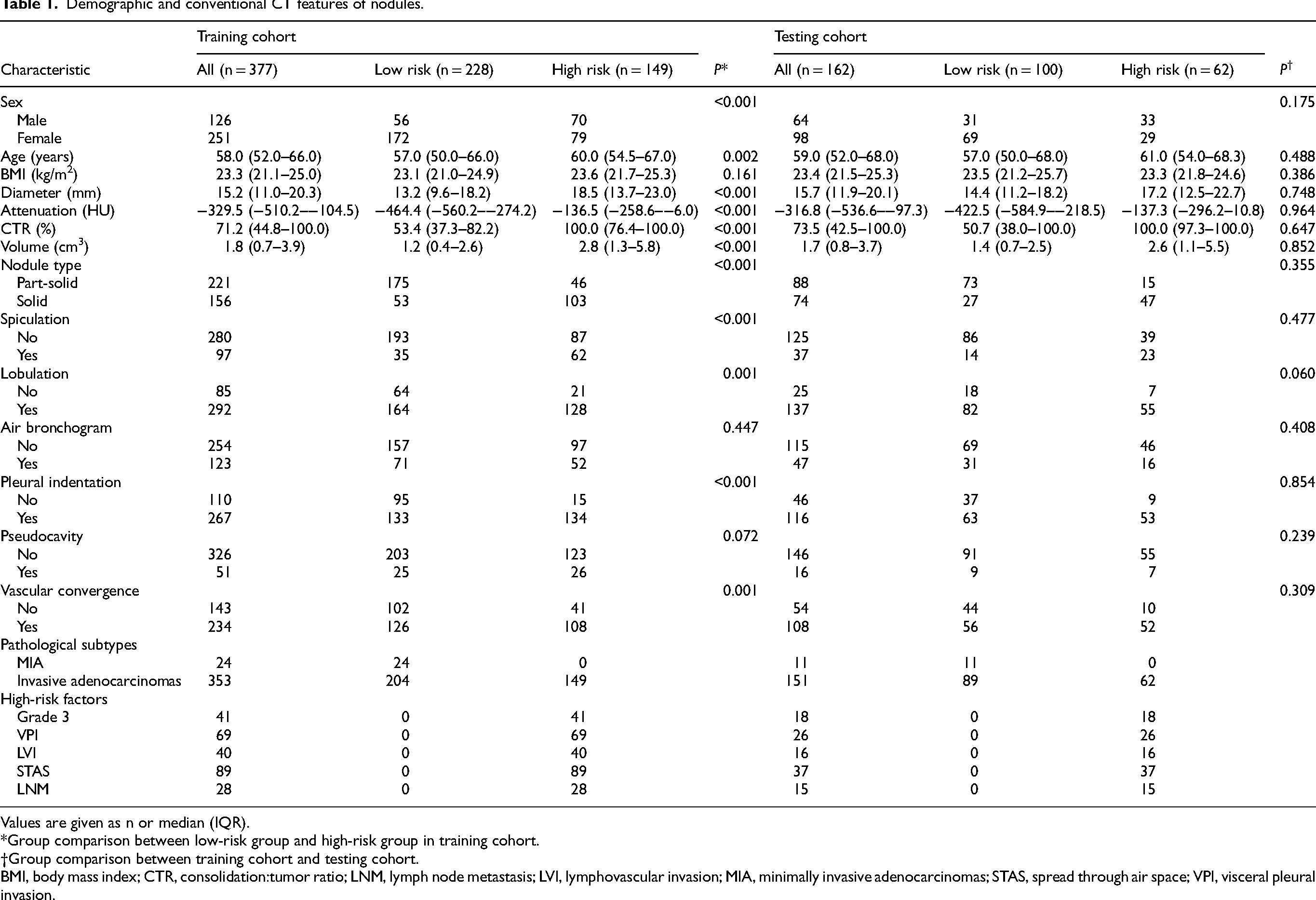
Values are given as n or median (IQR).
*Group comparison between low-risk group and high-risk group in training cohort.
Group comparison between training cohort and testing cohort.
BMI, body mass index; CTR, consolidation:tumor ratio; LNM, lymph node metastasis; LVI, lymphovascular invasion; MIA, minimally invasive adenocarcinomas; STAS, spread through air space; VPI, visceral pleural invasion.
Statistical analysis
This study used R (version 4.4.1) and MedCalc (version 18.2.1) for statistical analysis. The continuous and categorical variables were compared using the Mann–Whitney U-test and Fisher's exact test, respectively. The reproducibility of CTR and DECT quantitative parameters was assessed using the intraclass correlation coefficient (ICC) and Bland–Altman plot. The univariable and multivariable logistic regression (with the backward stepwise selection) was used to construct the conventional CT model, DECT model, and combined model in the training cohort. Then, the testing cohort was used to validate these models. The diagnostic performance was assessed with the area under the curve (AUC). The AUC of models was compared with the DeLong test (37). A two-tailed P <0.05 showed a statistical difference.
Results
Clinical and conventional CT quantitative-semantic features of nodules
In the training cohort, the high-risk group demonstrated significantly higher age, diameter, attenuation, CTR, and volume than the low-risk group (all P <0.05). There were significant differences in sex, nodule type, spiculation, lobulation, vascular convergence sign, and pleural indentation between the two groups (all P <0.05), except for body mass index (BMI) (P = 0.161), air bronchogram (P = 0.447), and pseudocavity (P = 0.072) (Table 1).
No significant differences in sex, BMI, age, diameter, attenuation, CTR, volume, nodule type, spiculation, lobulation, air bronchogram, pleural indentation, pseudocavity, and vascular convergence sign were found between the training and testing cohorts (all P >0.05) (Table 1).
The ICCs of diameter, attenuation, and volume assessed by AI and the senior radiologist were 0.916, 0.987, and 0.933, respectively, indicating a satisfactory reproducibility.
Reproducibility analysis of manual quantitative parameters
The CTR and quantitative parameters of DECT showed good inter-observer agreement (ICC = 0.809–0.935) and intra-observer agreement (ICC = 0.811–0.956) in this study (Table S1). The Bland–Altman plots were provided in Figures S1 and S2 in the supplementary material.
DECT quantitative parameters of nodules
In the training cohort, the high-risk group showed significantly higher Rho_A, Rho_V, Zeff_A, and Zeff_V and significantly lower NIC_A, λHU_A, and λHU_V than the low-risk group (all P <0.05). However, there was no significant difference in NIC_V between the two groups (P = 0.543) (Table 2).
DECT quantitative parameters of nodules.
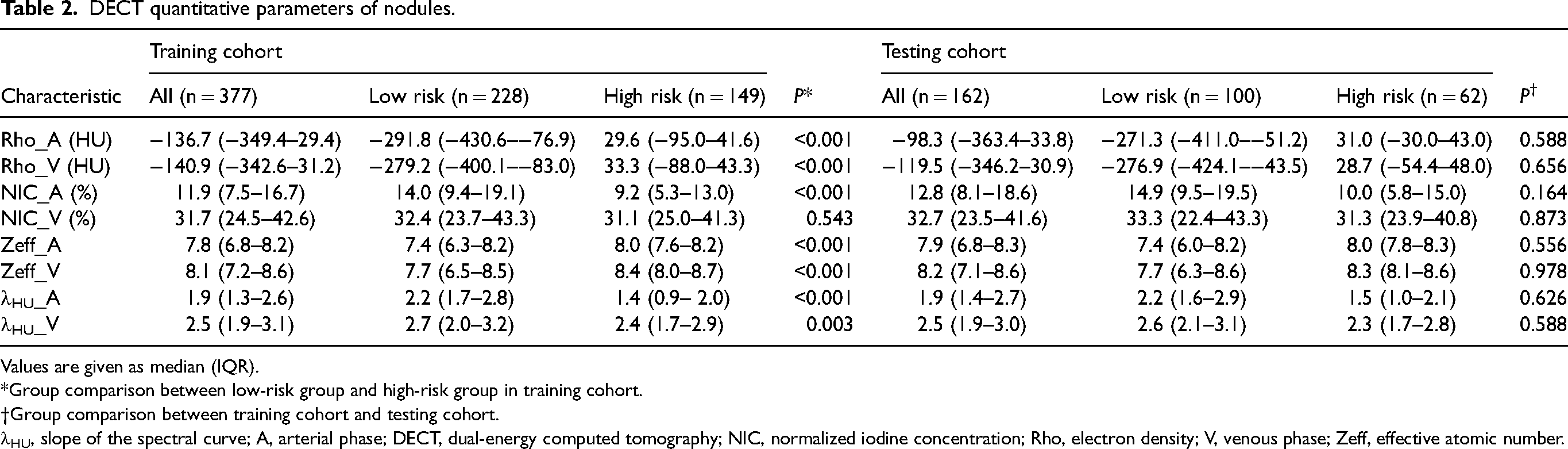
Values are given as median (IQR).
*Group comparison between low-risk group and high-risk group in training cohort.
Group comparison between training cohort and testing cohort.
λHU, slope of the spectral curve; A, arterial phase; DECT, dual-energy computed tomography; NIC, normalized iodine concentration; Rho, electron density; V, venous phase; Zeff, effective atomic number.
No significant differences in Rho_A, Rho_V, Zeff_A, Zeff_V, NIC_A, NIC_V, λHU_A, and λHU_V were found between the training cohort and testing cohort (all P >0.05) (Table 2).
Conventional CT model
Diameter, attenuation, CTR, volume, nodule type, spiculation, lobulation, pleural indentation, and vascular convergence sign were predictive factors for high-risk LUAD in the univariate logistic regression (all P <0.05). Multivariable logistic regression found that diameter and pleural indentation were the independent factors for high-risk LUAD (all P <0.05), which were used to construct the conventional CT model (Table 3). The calculation formula for the conventional CT model was shown in Table S2 in the supplementary material.
Univariable and multivariable logistic regression analysis for predicting high-risk lung adenocarcinomas in training cohort.
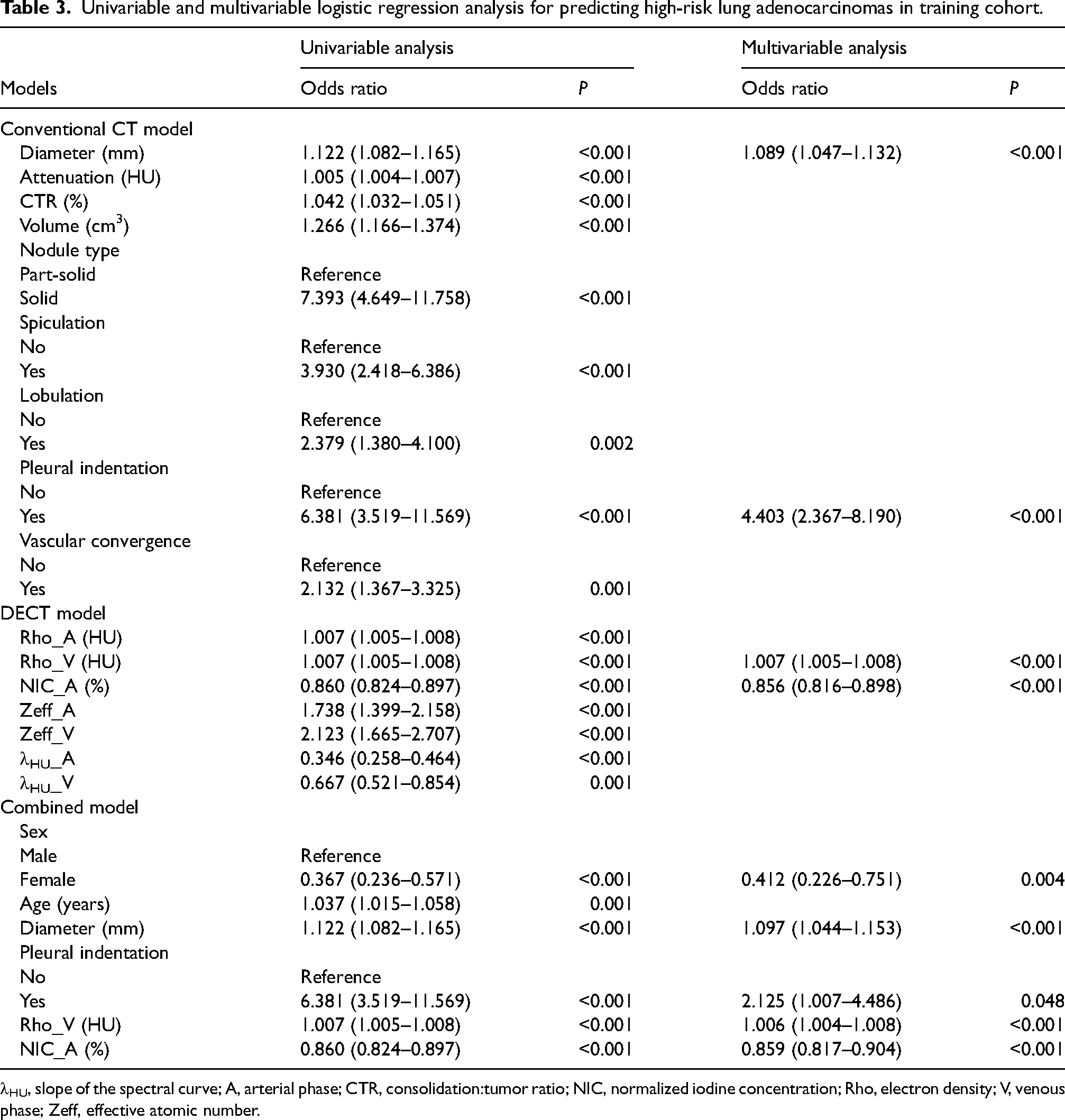
λHU, slope of the spectral curve; A, arterial phase; CTR, consolidation:tumor ratio; NIC, normalized iodine concentration; Rho, electron density; V, venous phase; Zeff, effective atomic number.
DECT model
Rho_A, Rho_V, NIC_A, Zeff_A, Zeff_V, λHU_A, and λHU_V were predictive factors for high-risk LUAD in the univariate logistic regression (all P <0.05). Multivariable logistic regression found that Rho_V and NIC_A were the independent factors for high-risk LUAD (all P <0.05), which were used to construct the DECT model (Table 3). The calculation formula for the DECT model was shown in Table S2 in the supplementary material.
Combined model
Furthermore, the combined model was constructed using multivariable logistic regression by integrating the clinical features with significant differences (sex and age) and all independent factors from the conventional CT model (diameter and pleural indentation) and DECT model (Rho_V and NIC_A). We found that sex, diameter, pleural indentation, Rho_V, and NIC_A were the independent factors for high-risk LUAD (all P <0.05), which were used to construct the combined model (Table 3). The calculation formula for the combined model was shown in Table S2 in the supplementary material.
Diagnostic performance
In the training cohort, the combined model showed significantly higher AUC than the DECT model (0.899 vs. 0.870, Z = 2.817; P = 0.005) and the conventional CT model (0.899 vs. 0.742, Z = 6.606; P <0.001). In the testing cohort, the combined model showed significantly higher AUC than the conventional CT model (0.852 vs. 0.704, Z = 3.598; P <0.001), but no significant difference in AUC was found between the combined model and the DECT model (0.852 vs. 0.838, Z = 0.927; P = 0.354).
In addition, the DECT model demonstrated significantly higher AUC than the conventional CT model in both the training (0.870 vs. 0.742, Z = 4.209; P <0.001) and testing cohorts (0.838 vs. 0.704, Z = 2.737; P = 0.006) (Table 4 and Fig. 3).

ROC curves of models in predicting high-risk lung adenocarcinoma in nodules with solid component in (a) the training cohort and (b) the testing cohort. AUC, area under the ROC curve; DECT, dual-energy computed tomography; ROC, receiver operating characteristic.
Diagnostic performance of models.
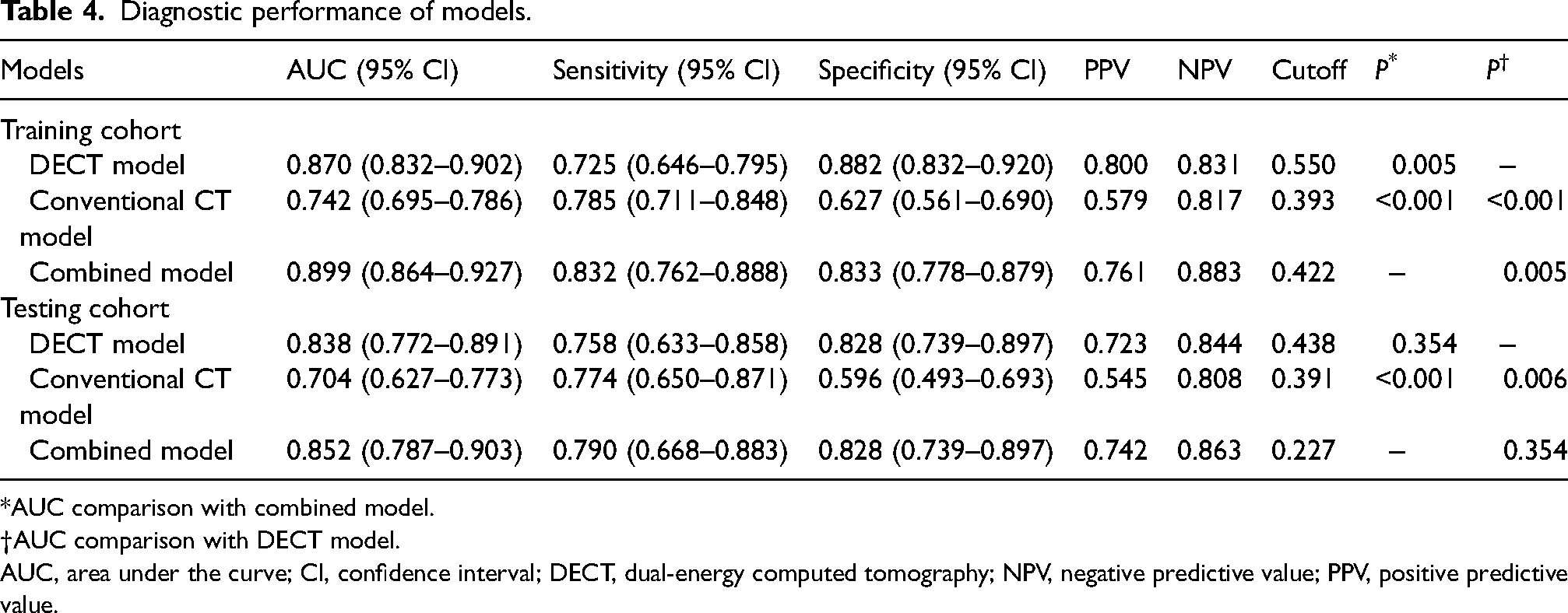
AUC comparison with combined model.
AUC comparison with DECT model.
AUC, area under the curve; CI, confidence interval; DECT, dual-energy computed tomography; NPV, negative predictive value; PPV, positive predictive value.
Discussion
Our study constructed the combined model (features: sex, diameter, pleural indentation, Rho_V, and NIC_A), the conventional CT model (features: diameter and pleural indentation), and the DECT model (features: Rho_V and NIC_A) to predict high-risk LUAD in nodules with solid components. We demonstrated that the combined model showed good performance in the training and testing cohorts, suggesting the potential of the combined model based on DECT in predicting high-risk LUAD as a non-invasive biomarker.
The high-risk factors of LUAD indicate the biological invasiveness. The VPI was identified as a non–size-dependent T2 identification and a prognostic predictor in TNM staging of LUAD, and the STAS has been identified as an invasion mode of lung cancer (36). The LUAD with high-risk factors has a poor prognosis (38–42). Therefore, accurately predicting high-risk LUAD during preoperative DECT could facilitate the nodule management. The high-risk factors can be diagnosed through preoperative and intraoperative pathology. However, preoperative biopsy and intraoperative frozen sections have inadequate accuracy in identifying high-risk factors because of sampling issues (43,44). The DECT quantitative parameters have an advantage in assessing the benign or malignant nature of solid nodules (19) and predicting the invasiveness of LUAD in GGNs (28). Therefore, they may have the potential to predict high-risk LUAD in nodules with solid component, and this study is intended to establish a DECT model as a decision-support tool to alert surgeons to high-risk features that might be missed by limited sampling.
Rho represents the likelihood of an electron occurring at a certain position (45) and is positively correlated with tissue density (46). The high-grade tumor may have higher tumor density due to the high degree of malignancy (47). IC reveals the actual enhancement value and reflects underlying microvessel density and tumor angiogenesis (48,49). The high-grade tumor may cause necrosis in the central region of the tumor due to faster growth speed (50), which may result in a decrease in NIC. Therefore, our study demonstrated that the higher Rho_A and lower NIC_V were associated with high-risk LUAD in the DECT model. Previous studies demonstrated that Rho could distinguish high-grade from low-grade cerebral gliomas (51) and differentiate invasive from minimally invasive adenocarcinoma in pure GGNs (24), and NIC could differentiate invasive from preinvasive adenocarcinomas (52), which was similar to our study.
λHU, offering attenuation changes of material at different energy levels (53) could differentiate high-grade from low-grade NSCLC in solid nodules (25). Zeff, reflecting the composite atom of a mixture of distinct materials (54), could differentiate invasive from non-invasive LUAD in part-solid nodules (55). However, λHU and Zeff were not the independent factors in differentiating high-risk LUAD in this study. This difference might be related to the different types of included pulmonary nodules. Previous research focused on solid nodules or part-solid nodules, whereas our study evaluated part-solid and solid nodules.
In quantitative-semantic features, a larger tumor diameter suggests a greater likelihood of high-grade pattern in LUAD (56). Pleural indentation presents scar contraction, which was caused by the fibrotic hyperplasia (57). In addition, active fibroblast proliferation indicates the invasive growth pattern of the tumor (58). Therefore, diameter and pleural indentation were the independent factors in differentiating high-risk LUAD in our conventional CT model. Previous studies demonstrated that diameter could predict poorly differentiated from well/moderately differentiated LUAD (59), and pleural indentation could differentiate acinar from lepidic predominant LUAD (56), which was similar to our study.
In terms of diagnostic performance, the combined model and the DECT model demonstrated higher AUC than the conventional CT model in the training cohort and testing cohort. The combined model showed significantly higher AUC than the DECT model in the training cohort, but no significant difference in AUC was found between the combined model and the DECT model in the testing cohort. Therefore, both the combined model and the DECT model may be helpful in predicting the high-risk LUAD in nodules with solid components. Although the AUC of the combined model and the DECT model (ranging = 0.838–0.899) is statistically significant in this study, it falls short of the clinical threshold (typically >0.90) required to alter high-stakes surgical management, such as deciding between a lobectomy and a segmentectomy.
In clinical practice, when a pulmonary nodule with solid component is detected, we may predict high-risk LUAD by integrating sex, diameter, pleural indentation, Rho_V, and NIC_A with the calculation formula of the combined model.
The present study has some limitations. First, this was a single-center study. Although we have validated the combined model using an internal testing cohort. However, further validation is needed using external testing cohort. Second, potential selection bias may not be avoided in this retrospective study. Third, the quantitative-semantic features were assessed on VNC images. A previous study demonstrated that the VNC image may replace the TNC image in the measurement of attenuation and volumetry in the lung tumor model (17). Finally, we only used the axial slice to measure the maximal and perpendicular diameter, which might lead to under-staging.
In conclusion, the combined model based on DECT integrating sex, diameter, pleural indentation, Rho_V, and NIC_A has good diagnostic performance in predicting high-risk LUAD in nodules with solid components, which may be useful for nodule management and prognostic prediction.
Supplemental Material
sj-docx-1-acr-10.1177_02841851261452150 - Supplemental material for A combined model based on dual-energy CT for predicting high-risk lung adenocarcinoma in nodules with solid component
Supplemental material, sj-docx-1-acr-10.1177_02841851261452150 for A combined model based on dual-energy CT for predicting high-risk lung adenocarcinoma in nodules with solid component by Changjiu He, Xianyu Cao, Haomiao Qing, Peng Zhou, Yi Zhang, Xiaolei Dong and Jieke Liu in Acta Radiologica
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Sichuan Provincial Natural Science Foundation, National Natural Science Foundation of China (grant nos. 2025ZNSFSC1765, 2023NSFSC1635, 82202141).
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.