
Abstract
Background
Ultrasound-guided radial artery cannulation is routinely performed; however, the optimal imaging approach remains debated. The short-axis out-of-plane approach facilitates vessel centering; however, it limits continuous needle-tip visualization, whereas the long-axis in-plane approach enables tip visualization but can be technically demanding. Dynamic needle tip positioning is a modified short-axis out-of-plane strategy designed to improve needle-tip tracking.
Methods
We conducted searches across PubMed, Embase, the Cochrane Library, Scopus, and Web of Science databases from inception through 1 January 2026. Randomized controlled trials involving adults that have compared the short-axis out-of-plane (dynamic needle tip positioning or traditional non–dynamic needle tip positioning) and long-axis in-plane approaches were included. The primary outcome was first-attempt success. Secondary outcomes included total success; time to cannulation; and hematoma, posterior wall puncture, and vasospasm incidences. Random-effects models were used, with prespecified subgroup analysis stratified by dynamic needle tip positioning. The protocol was registered in the International Prospective Register of Systematic Reviews (CRD420251276500). Small-study effects were assessed using Egger’s regression for outcomes reported in ≥10 studies.
Results
Thirteen trials (1482 participants) were included. Overall, first-attempt success rates did not differ between the short-axis out-of-plane and long-axis in-plane (relative risk = 0.99, 95% confidence interval: 0.85–1.15) approaches. Subgroup analysis showed higher first-attempt success rates with the dynamic needle tip positioning short-axis out-of-plane approach than with the long-axis in-plane approach (relative risk = 1.22, 95% confidence interval: 1.13–1.32), whereas the non–dynamic needle tip positioning short-axis out-of-plane approach demonstrated no advantage (relative risk = 0.88, 95% confidence interval: 0.72–1.09). Total success rates were similar (relative risk = 0.99, 95% confidence interval: 0.95–1.02), and time to cannulation did not differ (mean difference (short-axis out-of-plane–long-axis in-plane)) = −3.52 s, 95% confidence interval: −11.09 to 4.05). Hematoma incidence was comparable (relative risk = 1.79, 95% confidence interval: 0.89–3.58). Overall, posterior wall puncture incidence did not differ; however, the non–dynamic needle tip positioning short-axis out-of-plane approach increased the posterior wall puncture risk compared with the long-axis in-plane approach (relative risk = 3.29, 95% confidence interval: 1.33–8.11). Vasospasm incidence was similar overall using both approaches (relative risk = 0.74, 95% confidence interval: 0.38–1.43), with a lower incidence reported in the dynamic needle tip positioning trials (relative risk = 0.27, 95% confidence interval: 0.09–0.80).
Conclusions
The short-axis out-of-plane and long-axis in-plane approaches showed comparable overall efficacy. The dynamic needle tip positioning–based short-axis out-of-plane approach may improve first-attempt success rates and reduce the incidence of vasospasm without an apparent increase in posterior wall puncture risk, whereas the traditional short-axis out-of-plane approach may involve a higher posterior wall puncture risk. These findings suggest that needle-tip tracking is as important as the imaging plane itself; however, larger pragmatic trials are needed to confirm this finding.
Keywords
Introduction
Radial artery cannulation is routinely performed for continuous blood pressure monitoring and repeated arterial blood gas analysis in perioperative and critical care settings.1,2 Compared with the traditional palpation technique, ultrasound guidance improves cannulation success and reduces complications, particularly in patients with weak pulses, obesity, hypotension, or challenging vascular anatomy.3,4
Among ultrasound-guided approaches, short-axis out-of-plane (SA-OOP) and long-axis in-plane (LA-IP) are the two most commonly used techniques. SA-OOP facilitates vessel centering and visualization of surrounding structures; however, continuous visualization of the needle tip is limited, which may increase the risk of posterior wall puncture (PWP). In contrast, the LA-IP technique allows real-time visualization of the needle shaft and tip but requires stable alignment of the probe, needle, and artery within a single imaging plane and may therefore be technically more demanding.5–7 Dynamic needle tip positioning (DNTP) is a modified SA-OOP technique that uses stepwise probe advancement and repeated relocalization of the true needle tip, thereby preserving the geometric advantages of the short-axis view and improving tip control. 8 To facilitate understanding of this technique, a stepwise schematic illustration of DNTP is provided in Figure 1.
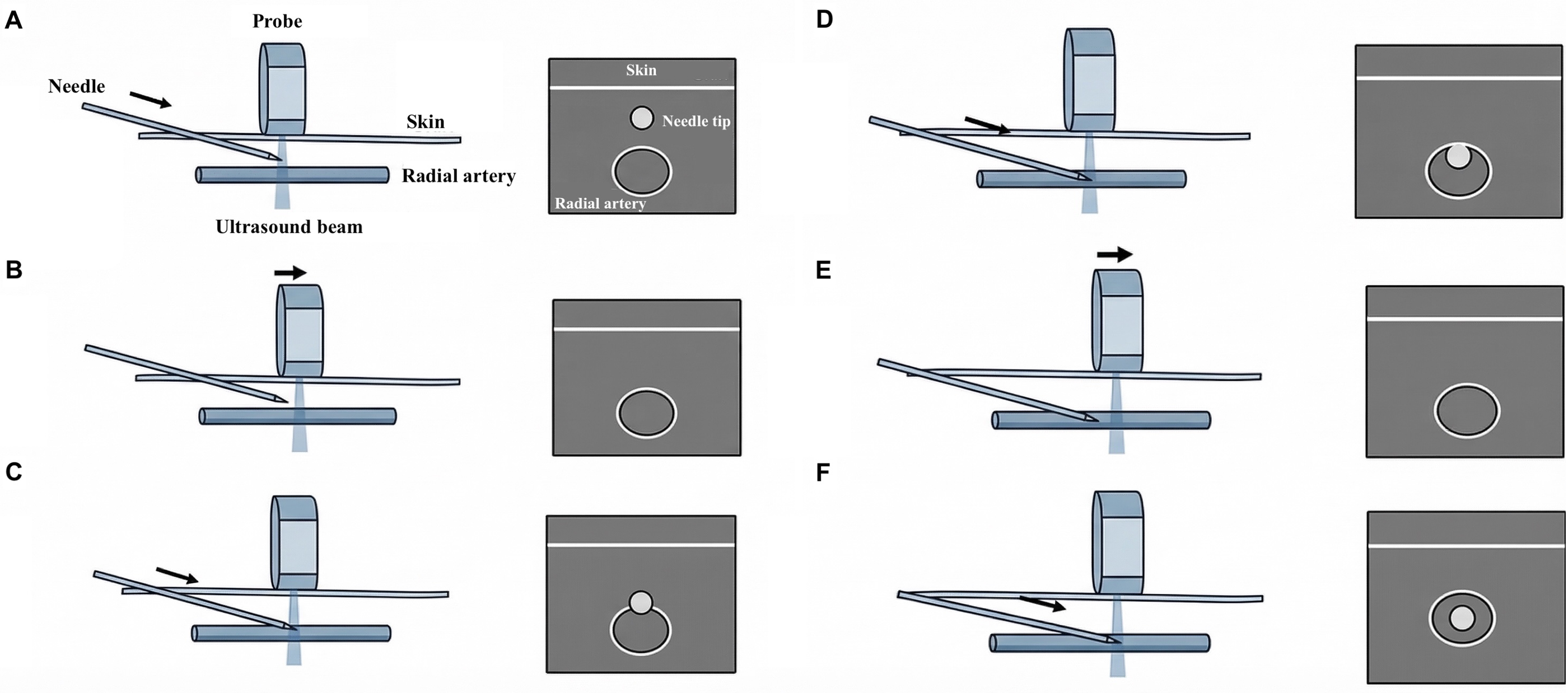
Stepwise schematic illustration of dynamic needle tip positioning (DNTP) during short-axis out-of-plane radial artery cannulation. (a to f) Illustration of sequential DNTP process. In each panel, the left image shows the spatial relationship between the needle, probe, ultrasound beam, skin, and radial artery, whereas the right image shows the corresponding short-axis ultrasound view. (a) The needle tip is identified as a hyperechoic dot superficial to the radial artery. (b) The transducer is slid slightly forward, causing the previously visualized needle tip to disappear from the ultrasound plane. (c) The needle is then advanced in small increments until the tip is redisplayed near the anterior wall of the radial artery. (d) Further needle advancement brings the tip to the anterior arterial wall, producing wall indentation. (e) The probe is again moved slightly forward to relocate the needle tip after it has advanced beyond the imaging plane. (f) Repetition of this “advance the needle–slide the probe–reidentify the tip” sequence enables continuous stepwise tracking of the needle tip into the arterial lumen, thereby facilitating controlled cannulation and reducing the risk of posterior wall puncture.
Previous meta-analyses comparing the SA-OOP and LA-IP approaches have reported inconsistent findings, partly because different short-axis variants were pooled together and because several newer randomized trials were not included.7,9 The aim of this systematic review and meta-analysis was to compare the SA-OOP and LA-IP approaches for ultrasound-guided radial artery cannulation in adults and determine whether DNTP modifies success and complication outcomes.
Methods
Protocol and registration
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; CRD420251276500) to prespecify the eligibility criteria, outcome definitions, and subgroup analyses.
Search strategy
Two investigators independently conducted searches across PubMed, Embase, the Cochrane Library, Scopus, and Web of Science databases from inception through 1 January 2026, with no language restrictions. The search strategy combined controlled vocabulary terms and free-text keywords related to ultrasound-guided radial artery cannulation and imaging approaches, including ultrasound/ultrasonography, radial artery, catheterization/cannulation, short-axis/transverse, long-axis/longitudinal, in-plane, and out-of-plane. We also manually screened the reference lists of eligible studies and relevant review articles to identify additional potentially eligible trials.
Eligibility criteria
Studies were considered eligible if they met the following the Population, Intervention, Comparison, Outcomes, and Study design (PICOS) criteria: (a) Population. Adults undergoing ultrasound-guided radial artery cannulation for perioperative care or hemodynamic monitoring; (b) Intervention. SA-OOP, including conventional non-DNTP SA-OOP and modified short-axis techniques such as DNTP; (c) Comparison. LA-IP; (d) Outcomes. The primary outcome was first-attempt success, and secondary outcomes included total cannulation success, time to cannulation (s), number of attempts, and complications, including hematoma, PWP, and vasospasm; (e) Study design. Randomized controlled trials (RCTs).
We excluded observational studies, case reports, editorials, conference abstracts without sufficient data, mannequin or phantom studies, and pediatric studies.
Study selection and data extraction
Two reviewers independently screened titles and abstracts, followed by full-texts assessment of potentially eligible studies. Data were extracted using a standardized form that recorded the first author, year, country, clinical setting, sample size, patient characteristics, operator experience, ultrasound equipment, and outcome data. Any disagreements were resolved by discussion, with adjudication by a third reviewer when necessary.
Risk of bias assessment
Risk of bias was assessed independently by two reviewers using the Cochrane Risk of Bias 2 (RoB 2) tool across five domains: (a) randomization process; (b) deviations from intended interventions; (c) missing outcome data; (d) measurement of the outcome; and (e) selection of the reported result. 10 Each study was judged as having low risk of bias, some concerns, or high risk of bias overall.
Statistical analyses
Statistical analyses were performed using Review Manager (RevMan) version 5.4 and Stata/SE version 16.0. For dichotomous outcomes, pooled effect sizes were expressed as risk ratios (RRs) with 95% confidence intervals (CIs). For continuous outcomes, mean differences (MDs) with 95% CIs were calculated. Statistical heterogeneity was assessed using Cochran’s Q test and quantified with the I 2 statistic; values of approximately 25%, 50%, and 75% were interpreted as low, moderate, and substantial heterogeneity, respectively.
Clinical and methodological heterogeneity was anticipated across studies, including variation in short-axis techniques such as DNTP; therefore, a random-effects model was applied for all meta-analyses. The Mantel–Haenszel method was used for dichotomous outcomes, and the inverse-variance method was used for continuous outcomes. Prespecified subgroup analyses were performed to compare DNTP trials with non-DNTP (traditional SA-OOP) trials to evaluate whether the pooled effects differed according to the short-axis technique used. Subgroup differences were assessed using the interaction test in RevMan where applicable.
Publication bias was assessed using funnel plots and Egger’s regression test for outcomes reported in at least 10 studies. All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant.
Results
Search results and study selection
The literature search identified 1847 records. After 969 duplicates were removed, 878 titles and abstracts were screened, and 19 articles were reviewed in full. Six reports were excluded because they were case reports, conference abstracts, or did not provide outcome data that could be extracted. The final dataset included 13 RCTs with 1482 patients. 6 11–22 The PRISMA flow diagram summarizes the selection process (Figure 2).
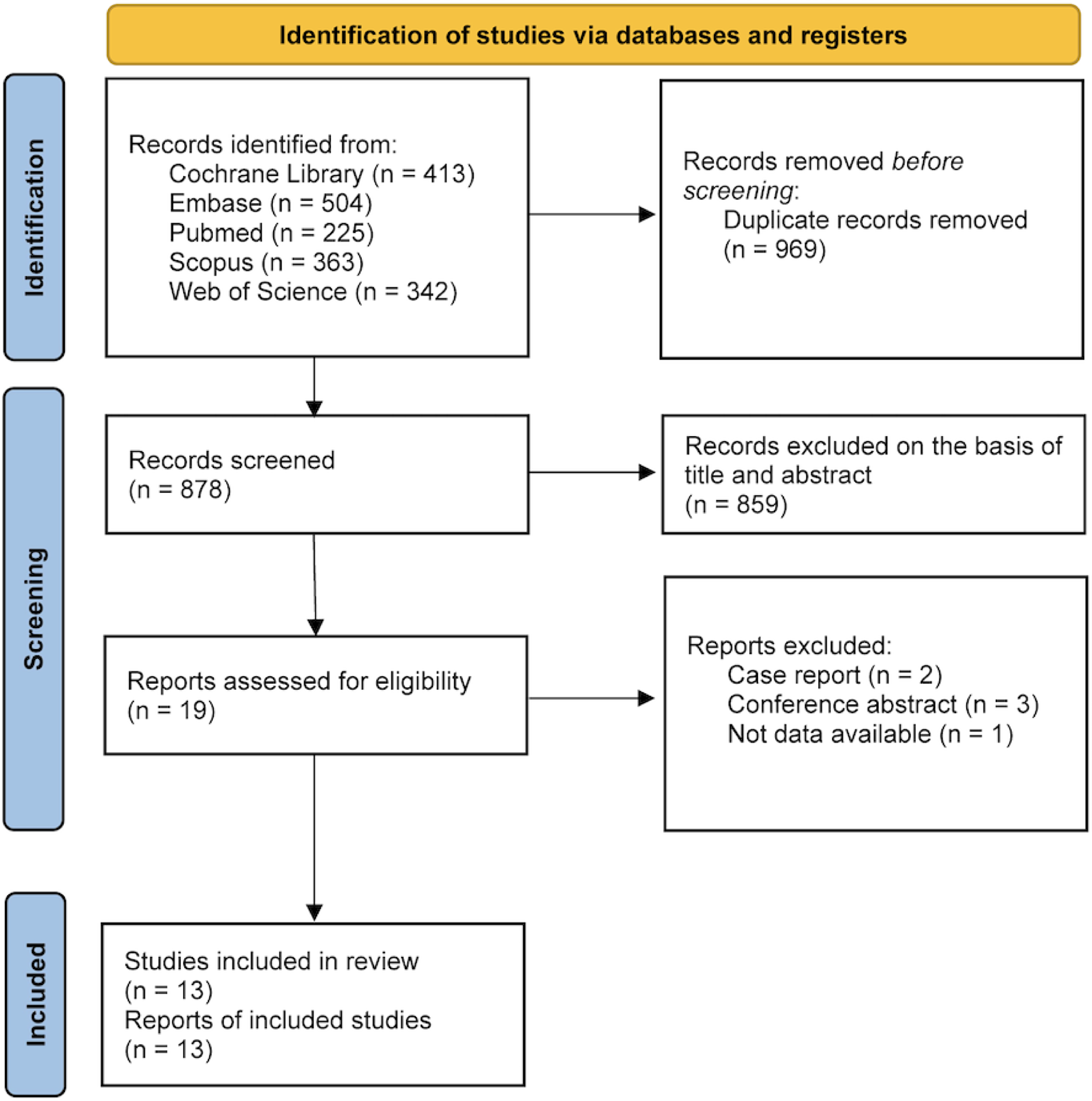
PRISMA flow diagram. Flow diagram showing study identification, screening, eligibility assessment, and inclusion, resulting in the inclusion of 13 randomized controlled trials.
Study characteristics and risk of bias
The main characteristics of the included trials are presented in Table 1. 6 11–22 The studies were conducted in Turkey, China, Egypt, India, South Korea, Oman, Pakistan, and Nepal. Most studies were performed in perioperative settings, with only limited representation from critical care environments. Sample sizes ranged from 60 to 163. Risk of bias was assessed using the RoB 2 tool and is summarized in Figure 3. Most trials were judged to be at low overall risk of bias, although some concerns regarding the accuracy of outcome measurements remained because operator blinding was not feasible in a procedure that depends on hand positioning and real-time image interpretation.
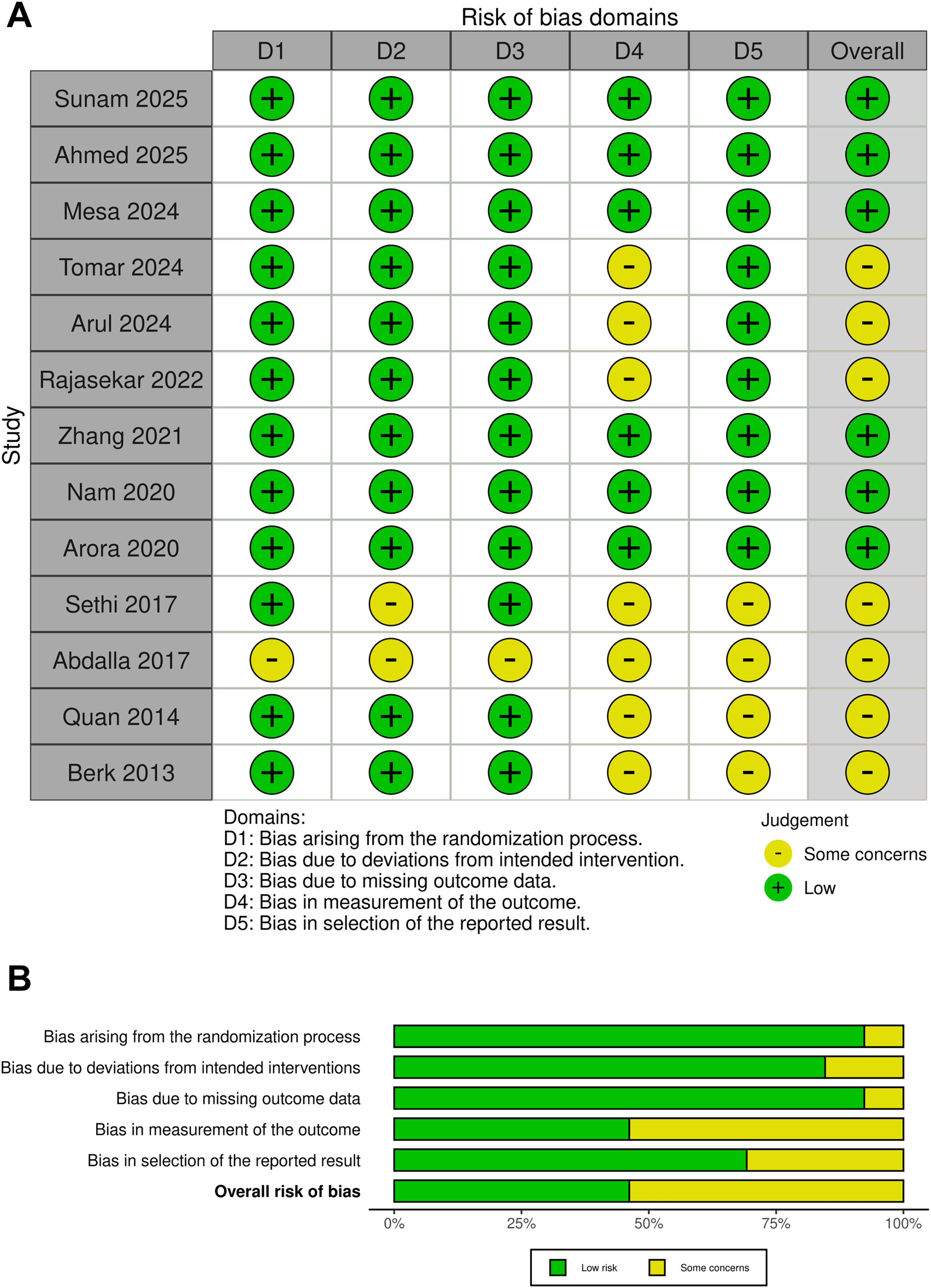
Risk of bias assessment (RoB 2). (a) Risk of bias graph. Reviewers’ judgments for each RoB 2 domain presented as percentages across included trials; (b) Risk of bias summary. Reviewers’ judgments for each RoB 2 domain for each trial.
Characteristics of included randomized controlled trials.

Data are presented as mean ± SD or n.
LA-IP: long-axis in-plane; DNTP: dynamic needle tip positioning; OR: operating room; ICU: intensive care unit; NR: not reported; BMI: body mass index; S: short-axis out-of-plane group; L: long-axis in-plane group; RA: radial artery.
Primary outcome
First-attempt success rate. All 13 trials reported first-attempt success. When the SA-OOP and LA-IP approaches were compared without separating short-axis variants, no significant difference was observed between the two approaches (RR = 0.99; 95% CI: 0.85–1.15; p = 0.860), and heterogeneity was substantial (I2 = 87%) (Figure 4).
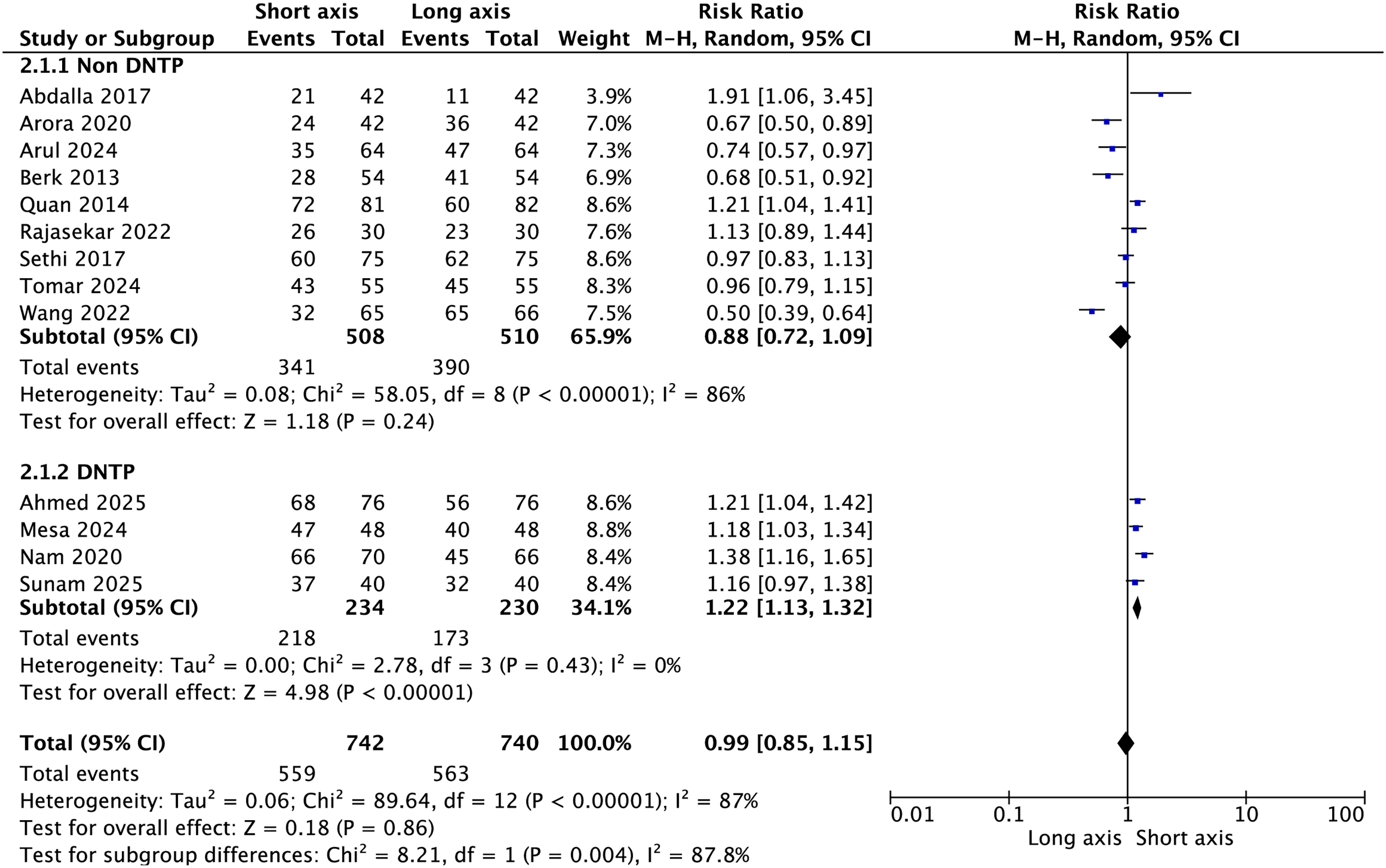
Forest plot of first-attempt success rates. Comparison of short-axis out-of-plane (SA-OOP) and long-axis in-plane (LA-IP) approaches. Prespecified subgroup analysis by dynamic needle tip positioning (DNTP) use (DNTP vs. non-DNTP (traditional SA-OOP)).
The prespecified subgroup analysis according to needle-tip tracking helped explain this heterogeneity. In trials using DNTP, the SA-OOP approach was associated with a higher first-attempt success rates than the LA-IP approach (RR = 1.22; 95% CI: 1.13–1.32; p < 0.001), with no evidence of heterogeneity (I2 = 0%). In contrast, in non-DNTP trials, the traditional SA-OOP approach did not show a significant advantage over the LA-IP approach (RR = 0.88; 95% CI: 0.72–1.09; p = 0.240), and heterogeneity remained substantial (I2 = 86%). The subgroup difference was statistically significant (p for interaction = 0.004), supporting DNTP as a clinically important effect modifier.
Secondary outcomes
Total cannulation success rate. Eleven trials reported total cannulation success. The pooled analysis showed no significant difference between the SA-OOP and LA-IP approaches (RR = 0.99; 95% CI: 0.95–1.02; p = 0.500), with substantial heterogeneity (I2 = 80%) (Figure 5). Subgroup analysis did not demonstrate a significant interaction according to the DNTP status (p for interaction = 0.420).
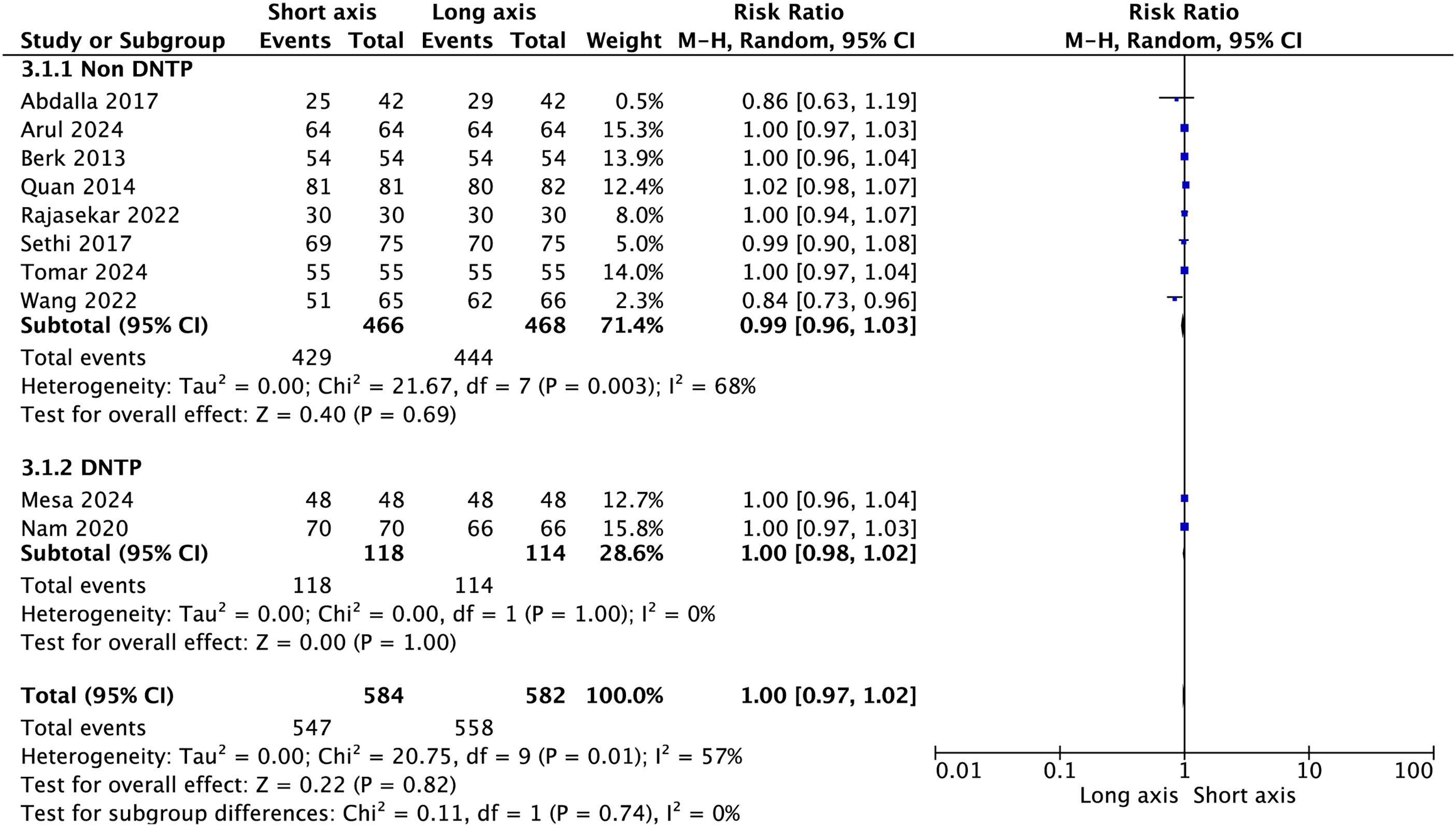
Forest plot of total cannulation success rates. Comparison of total cannulation success between the SA-OOP and LA-IP approaches.
Time to cannulation. Eight trials reported time to cannulation (SA-OOP: n = 441; LA-IP: n = 442). The pooled analysis showed no significant difference between the two approaches (MD (SA-OOP–LA-IP) = −3.52 s; 95% CI: −11.09 to 4.05; p = 0.360), but heterogeneity was extreme (τ2 = 107.33; χ2 = 224.69, df = 7, p < 0.001; I2 = 96.9%) (Figure 6). This marked variability likely reflects important between-study differences in the definition and measurement of procedural time. Some trials used relatively narrow intervals, such as needle puncture to flashback or arterial waveform, whereas others used broader workflow-based intervals, such as probe placement to successful cannulation. These definitional inconsistencies, together with variations in operator sequence and local procedural workflow, likely limited the interpretability of the pooled estimates for this outcome.
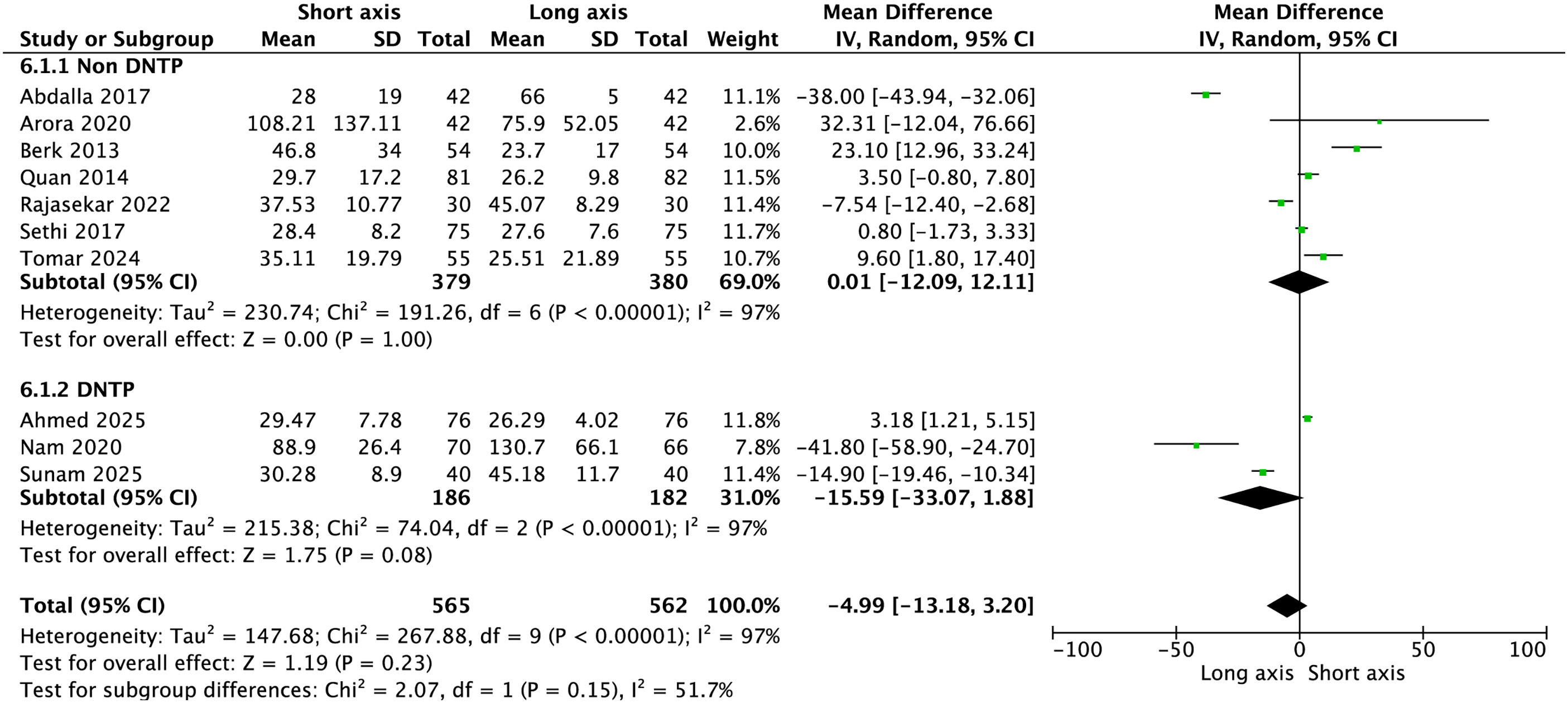
Forest plot of time to cannulation (s). Comparison of time to cannulation between the SA-OOP and LA-IP approaches. Mean difference is presented as MD (SA-OOP–LA-IP); negative values favor SA-OOP (shorter time), consistent with the “favors SA-OOP” direction shown in the plot.
Complications
Hematoma. Twelve trials reported hematoma. The pooled analysis did not show a statistically significant difference between the SA-OOP and LA-IP approaches (RR = 1.79; 95% CI: 0.89–3.58; p = 0.100), with moderate heterogeneity (I2 = 63%) (Figure 7). In subgroup analysis, the non-DNTP subgroup showed a greater hematoma risk (RR = 2.26; 95% CI: 0.94–5.42; p = 0.070), whereas no such rend was observed in the DNTP subgroup (RR = 1.01; 95% CI: 0.25–4.09; p = 0.990); however, the interaction test was not statistically significant (p for interaction = 0.340).
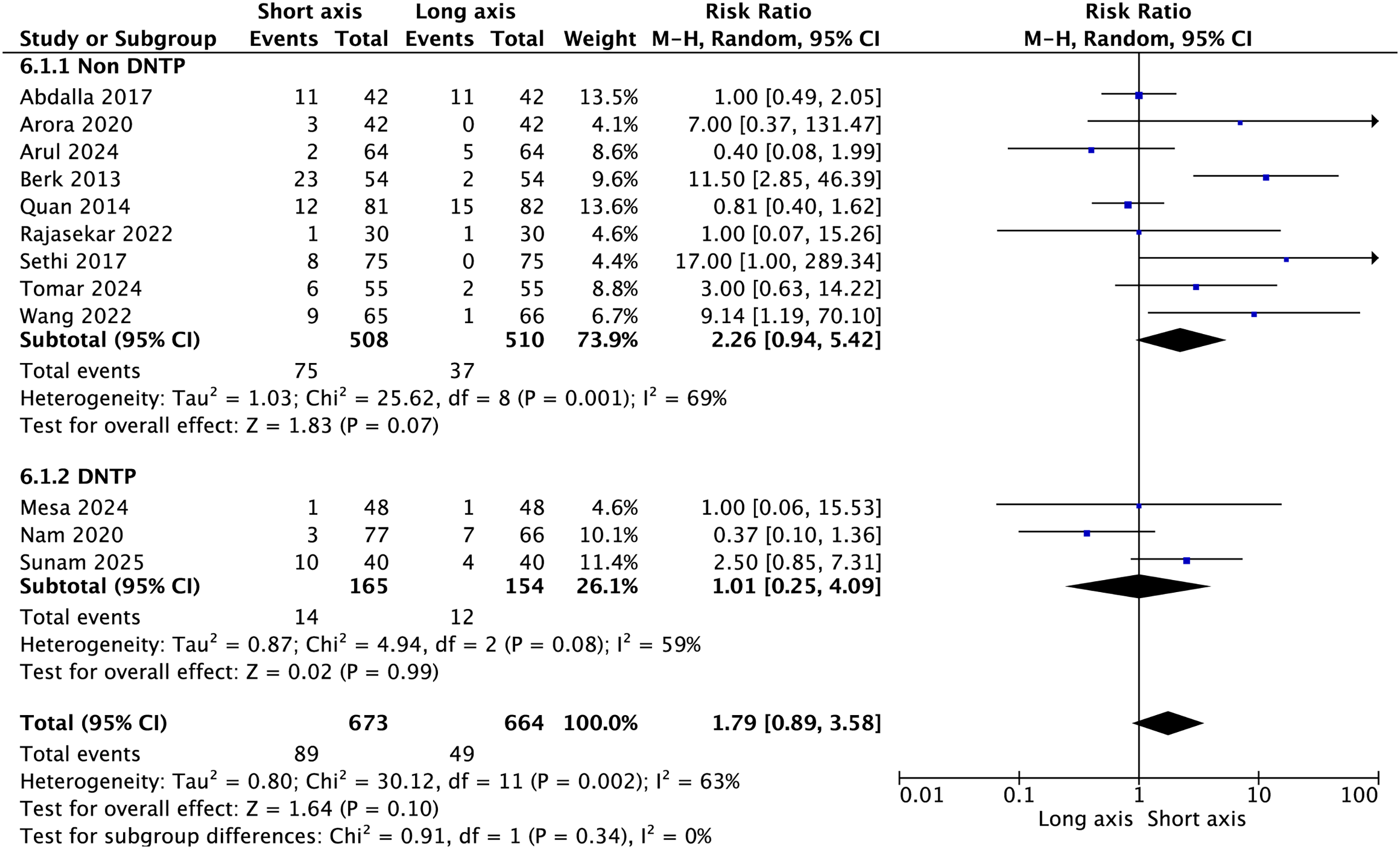
Forest plot of hematoma. Comparison of hematoma incidence between the SA-OOP and LA-IP approaches.
PWP. Five trials reported PWP. The overall pooled analysis did not show a significant difference between the SA-OOP and LA-IP approaches (RR = 2.02; 95% CI: 0.67–6.13; p = 0.210), and heterogeneity was substantial (I2 = 80%) (Figure 8). Subgroup analysis provided a more differentiated pattern. In non-DNTP trials, the traditional SA-OOP approach was associated with a higher risk of PWP than the LA-IP approach (RR = 3.29; 95% CI: 1.33–8.11; p = 0.010); however, the DNTP trials did not show a significant increase (RR = 0.42; 95% CI: 0.14–1.30; p = 0.130). The subgroup difference was statistically significant (p for interaction = 0.005).
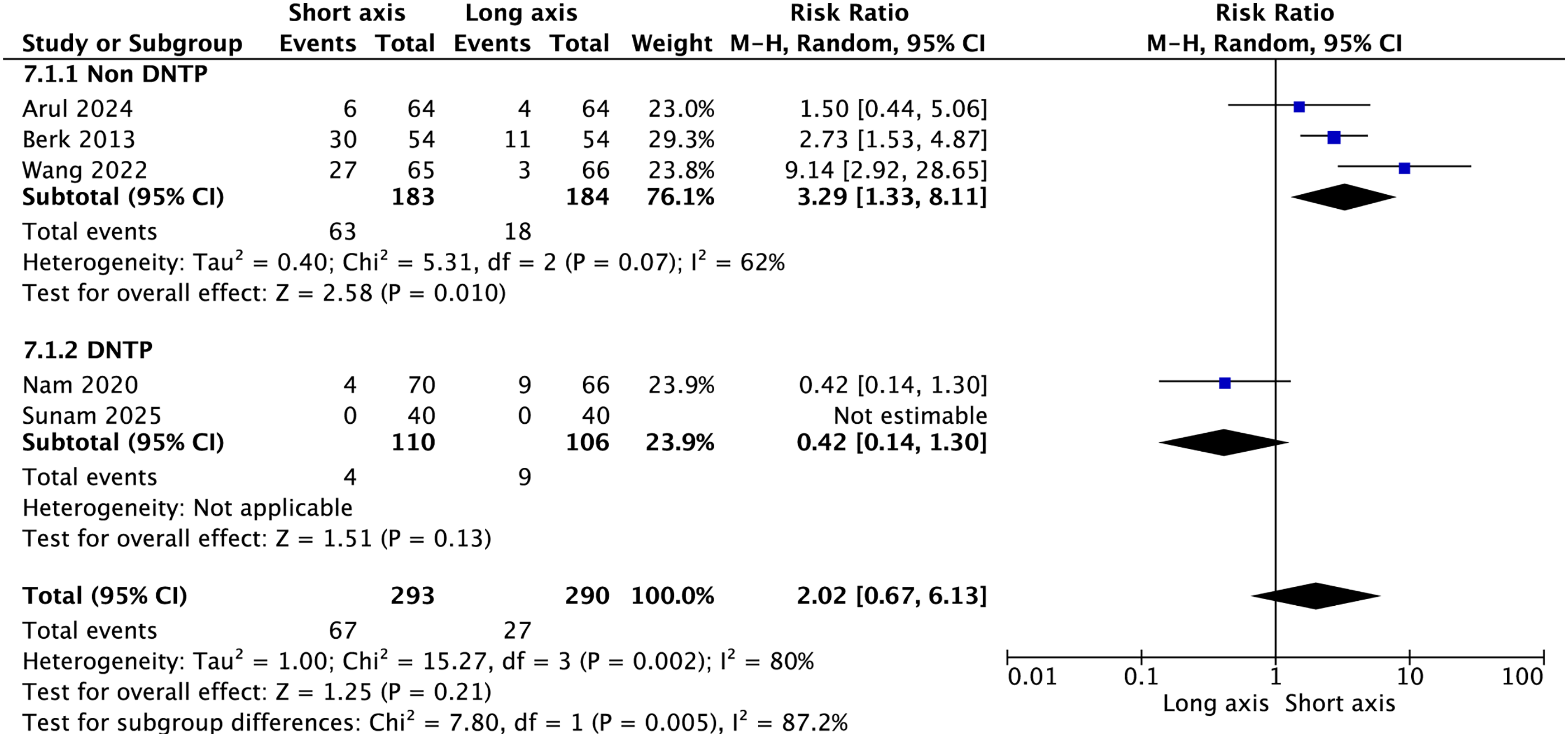
Forest plot of posterior wall puncture (PWP). Comparison of PWP incidence between the SA-OOP and LA-IP approaches with subgroup analysis by technique (DNTP vs. non-DNTP (traditional SA-OOP)).
Vasospasm. Nine trials reported vasospasm, whereas two trials had zero events in both groups and therefore could not contribute to RR pooling. The overall analysis showed no significant difference in the vasospasm incidence between the SA-OOP and LA-IP approaches (RR = 0.74; 95% CI 0.38–1.43; P = 0.360), with low heterogeneity (I2 = 24%) (Figure 9). However, subgroup analysis suggested technique-related variation. The DNTP trials showed a lower vasospasm rate than the LA-IP trials (RR = 0.27; 95% CI: 0.09–0.80; p = 0.020), whereas non-DNTP trials showed no significant difference (RR = 1.04; 95% CI: 0.55–1.95; p = 0.910). The subgroup difference was statistically significant (p for interaction = 0.040).
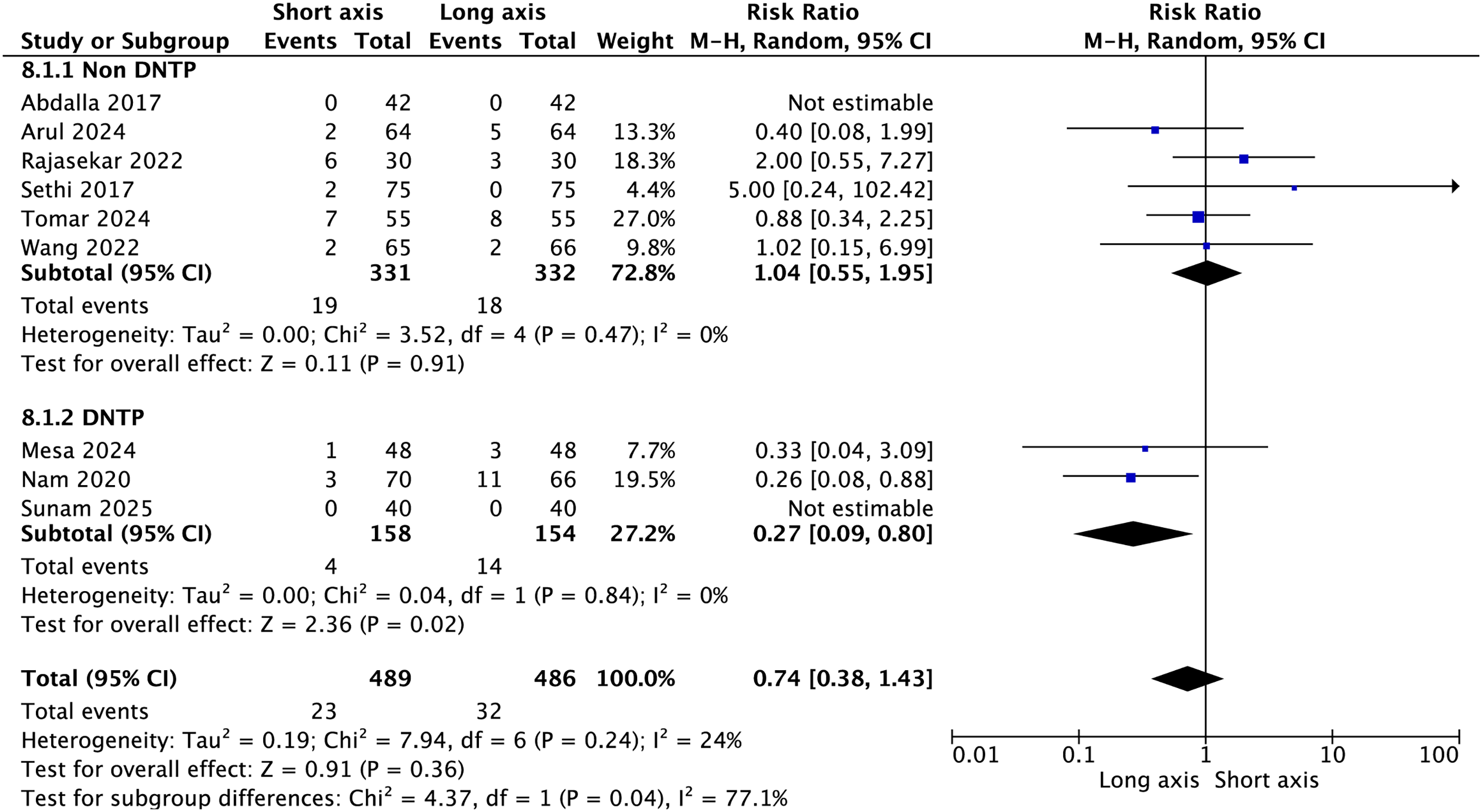
Forest plot of vasospasm incidence. Comparison of vasospasm incidence between the SA-OOP and LA-IP approaches.
Publication bias. Egger’s regression suggested small-study effects for first-attempt success (p = 0.030), indicating that publication bias or inflated effects in smaller studies cannot be excluded. No significant small-study effects were detected for total cannulation success (p = 0.745) or hematoma risk (p = 0.283) (Table 2). Egger’s regression was not performed for PWP or vasospasm because fewer than 10 studies reported these outcomes.
Egger’s regression test for small-study effects.

Egger’s regression was used to assess small-study effects (potential publication bias) for outcomes reported in ≥10 studies.
p <0.05 indicates statistical significance.
Coefficient: regression coefficient; SE: standard error; CI: confidence interval.
Discussion
Across 13 RCTs involving 1482 adults, the SA-OOP and LA-IP approaches showed a comparable pooled first-attempt success rate when all short-axis techniques were analyzed together, although substantial between-study heterogeneity was present. When the short-axis approach was stratified according to needle-tip tracking, a clearer pattern emerged. The SA-OOP approach with DNTP was associated with a higher first-attempt success rate than the LA-IP approach, whereas the traditional non-DNTP SA-OOP did not demonstrate a similarly higher rate. Total cannulation success and time to cannulation were also similar overall. Most complication outcomes were likewise comparable, although two technique-related signals were notable; the traditional SA-OOP approach was associated with a higher risk of PWP, whereas DNTP trials showed a lower incidence of vasospasm.
Previous reviews have reported inconsistent conclusions. A prior meta-analysis comparing the SA-OOP and LA-IP approaches have reported similar overall success rates together with substantial heterogeneity. 7 However, that review combined different arterial access sites and patient populations, including femoral access in neonates and infants, which may have increased between-study variability even when the same broad imaging-plane labels were used. 7 By contrast, our analysis was restricted to adult radial artery cannulation and prespecified DNTP as a subgroup of interest. This design provides a clinically plausible explanation for why earlier pooled estimates often appeared neutral despite meaningful differences between specific short-axis techniques.
From a procedural perspective, the practical distinction between these approaches lies in the balance between vessel visualization and needle-tip control. The SA-OOP approach facilitates centering of the artery in the cross-section; however, confirmation of the true needle tip may be limited, increasing the risk of advancing beyond the posterior wall before the tip is recognized. In contrast, the LA-IP approach enables continuous visualization of the needle shaft and tip, but requires stable alignment of the probe, needle, and artery within a single imaging plane, which may be technically challenging for less experienced operators or in patients with a small artery or wrist movement.23,24 DNTP addresses this trade-off by preserving the short-axis view and incorporating repeated confirmation of the true tip during stepwise needle advancement. 8 This mechanism is consistent with the higher first-attempt success observed in the DNTP subgroup and may also help explain why previous meta-analyses that pooled multiple short-axis variants often failed to identify a clear overall difference. 25
PWP is a clinically relevant failure mode in traditional SA-OOP because it may contribute to hematoma formation and make subsequent attempts more difficult. In our subgroup analysis, the non-DNTP SA-OOP approach was associated with a higher risk of PWP than the LA-IP approach, whereas the DNTP trials did not show a significant increase. This pattern is consistent with the procedural rationale of DNTP, in which repeated confirmation of the true needle tip may reduce overshoot beyond the posterior wall during needle advancement. 21 Although hematoma incidence did not differ significantly overall, the direction of effect observed in non-DNTP trials remains clinically plausible given the mechanistic link between PWP and hematoma during radial artery cannulation.
Vasospasm showed another technique-related signal. In DNTP trials, the risk of vasospasm was lower than that in LA-IP trials (RR = 0.27). This finding is biologically plausible because vasospasm is often triggered by repeated puncture attempts, vessel wall irritation, or periarterial bleeding.1,11 Improved needle-tip control and fewer unnecessary redirections may reduce vessel trauma and thereby decrease the likelihood of vasospasm. However, vasospasm events were infrequent, and several trials reported zero events; therefore, this finding should be interpreted as a preliminary signal that requires confirmation in larger pragmatic studies.
Time to cannulation was retained as a prespecified and clinically relevant secondary outcome because it reflects procedural efficiency and was reported in multiple randomized trials. However, given the substantial inconsistency in outcome definitions across studies, this endpoint was interpreted cautiously and considered exploratory rather than decisive. A likely explanation for the extreme heterogeneity is that time to cannulation was not standardized across studies. In practice, the difference between measuring “needle puncture to successful waveform” and “probe on skin to successful cannulation” may exceed the true procedural difference between the SA-OOP and LA-IP techniques themselves. Study-level differences in workflow, equipment setup, and operator sequence may also have contributed to this variability. In addition, DNTP involves small stepwise probe movements, which may prolong some components of the procedure, whereas fewer redirects or repeat punctures may offset that additional time. Taken together, these factors make pooled analyses of procedural time inherently less stable than pooled analyses of first-attempt success.
Limitations
Certain study limitations should be considered when interpreting these findings. First, operator blinding is not feasible in ultrasound-guided cannulation; therefore, performance bias cannot be excluded. Second, heterogeneity was substantial for several outcomes, particularly first-attempt success and time to cannulation. For procedural time, this heterogeneity was likely amplified by inconsistent outcome definitions across studies. Third, operator experience was variably reported and often reflected experienced anesthetists or expert operators, which may limit generalizability to less experienced clinicians. We did not perform meta-regression because study-level covariates such as operator experience, clinical setting, and ultrasound equipment were reported inconsistently across trials, and the number of available studies was limited, making such analyses potentially unstable. Fourth, ultrasound equipment and transducer specifications differed across studies, and these technical differences may have influenced image quality and procedural performance. Fifth, several safety outcomes were infrequent, resulting in wide CIs and reduced precision. Sixth, Egger’s regression suggested possible small-study effects for the primary outcome; therefore, the magnitude of benefit should be interpreted cautiously. Finally, baseline radial artery diameter was not systematically reported across most included trials, which prevented formal assessment of vessel caliber as an effect modifier, even though artery size may influence cannulation difficulty and success. In addition, most included trials were conducted in perioperative settings, and the findings may therefore not fully generalize to high-acuity intensive care unit (ICU) or emergency department practice.
Implications and future research
Taken together, these findings support a technique-based view rather than a simple short-axis versus long-axis comparison. If the SA-OOP approach is selected, incorporation of DNTP or another structured tip-tracking method may improve first-attempt success rates and reduce the incidence of selected complications, particularly PWP and vasospasm. Future randomized trials should use standardized and explicitly reported definitions of procedural time, report operator training and competency metrics in a reproducible manner, include pragmatic ICU and emergency department populations, and provide sufficient study-level detail to support future meta-regression or other covariate-based analyses. Additional clinically relevant outcomes, such as number of attempts, time to a usable arterial waveform, need for rescue techniques, and downstream access-related complications, should also be reported consistently.
Conclusion
The SA-OOP and LA-IP approaches showed similar overall performance when all short-axis techniques were pooled. However, the SA-OOP approach with DNTP was associated with higher first-attempt success rates and may be associated with a lower incidence of vasospasm, whereas the traditional non-DNTP SA-OOP approach was associated with a higher risk of PWP. Taken together, these findings suggest that needle-tip tracking technique is as important as the imaging plane itself in ultrasound-guided radial artery cannulation. Given the substantial heterogeneity, inconsistent outcome definitions, and limited generalizability to high-acuity settings, larger pragmatic trials are warranted.
Footnotes
Acknowledgments
This manuscript was polished for language clarity using Grammarly Premium and ChatGPT (OpenAI).
Informed consent statement
Not applicable.
Institutional review board statement
Not applicable.
Author contributions
Kui Mao: Conceptualization, Methodology, Investigation, Data curation, Formal analysis, and Writing–original draft.
Mengqi Cai: Investigation, Data curation, Formal analysis, Visualization, and Writing–review & editing.
Jialu Liang: Investigation, Data curation, Visualization, and Writing–review & editing.
Yangtian Ye: Formal analysis, Software, Visualization, and Writing–review & editing.
Jiuzhou Lin: Investigation, Data curation, and Writing–review & editing.
Min Tang: Investigation, Data curation, and Writing–review & editing.
Lihui Chen: Validation, Methodology, and Writing–review & editing.
Weiting Chen: Supervision, Conceptualization, Methodology, Project administration, and Writing–review & editing.
Jie Huang: Supervision, Conceptualization, Project administration, and Writing–review & editing.
All authors have read and approved the final manuscript.
Funding
This research received no external funding.
Conflicts of interest
The authors declare no conflicts of interest.
Data availability statement
All data pertaining to this study are contained within this manuscript.