
Abstract
This report describes the case of a male in his early 60s with coronary heart disease who developed recurrent urticaria following the initiation of antiplatelet and lipid-lowering therapy. Through sequential drug dechallenge and rechallenge, aspirin was identified as the probable cause. Despite initial treatment with cetirizine and reintroduction of aspirin, the patient’s symptoms recurred, necessitating readmission. A multidisciplinary team, including clinicians and clinical pharmacists, optimized the treatment strategy by replacing aspirin with ticagrelor and cilostazol for antiplatelet therapy, discontinuing and reintroducing atorvastatin to rule out drug allergy, and administering desloratadine citrate and methylprednisolone for antiallergic treatment. The patient’s urticaria resolved completely without recurrence, and aspirin was identified as the probable cause using the adverse drug reaction causality assessment scale. Although aspirin was reintroduced on Day 2, the concurrent use of multiple drugs, including corticosteroids and antihistamines, may have influenced the timing and severity of the subsequent urticaria recurrence. Postdischarge follow-up confirmed sustained remission, highlighting the importance of collaborative care in managing drug-induced urticaria and maintaining cardiovascular safety.
Introduction
Several drugs are reported to contribute to adverse drug reactions (ADRs), including urticaria. 1 Early screening for drug allergies aids in improving safety, compliance, and clinical effectiveness. Aspirin is commonly used for preventing plaque formation in coronary heart disease and has become a cornerstone in cardiovascular medicine. 2 However, it needs to be discontinued in some patients because of allergic skin reactions such as urticaria. According to epidemiological studies, the incidence of allergic reactions to aspirin ranges from 0.3% to 0.9%, among which, aspirin-associated urticaria accounts for 0.07%–0.2%.3,4 Furthermore, it has been reported that 1.5%–2.6% of patients with heart disease are allergic to aspirin. 5 Therefore, it is particularly important to determine effective measures to prevent allergic reactions to aspirin in clinical practice.
In this study, clinical pharmacists and clinicians worked together to analyze a case of recurrent aspirin-induced urticaria. The case illustrates the complexity of managing patients who require antiplatelet therapy but experience adverse allergic reactions, such as urticaria. Although aspirin discontinuation posed a thrombotic risk, the team prioritized the management of the patient’s allergic symptoms and maintained cardiovascular safety. Through systematic evaluation and a collaborative care model, the team confirmed aspirin as the likely cause of the urticaria and introduced an alternative antiplatelet regimen. This approach successfully resolved the patient’s allergic symptoms without compromising their cardiovascular health. The study emphasizes the critical role of multidisciplinary teams in optimizing treatment strategies for patients with suspected ADRs, highlighting the importance of balancing safety and therapeutic efficacy in clinical practice.
Case report
A male in his early 60s with a history of coronary heart disease underwent coronary stent implantation due to severe coronary stenosis in July 2021 at Zhejiang Provincial People’s Hospital, Affiliated People’s Hospital, Hangzhou Medical College (Hangzhou, China). Postoperatively, he was prescribed dual antiplatelet therapy with aspirin and clopidogrel, along with rosuvastatin for lipid-lowering and plaque stabilization. The patient had no known history of drug allergy. However, 1 day after starting these medicines, he developed urticaria (confirmed by a dermatologist), characterized by pruritus, erythema, and pain in the leg and foot (Figure 1). Cetirizine was administered, leading to significant symptom improvement. The patient was subsequently discharged and continued taking aspirin, clopidogrel, and rosuvastatin, as prescribed.
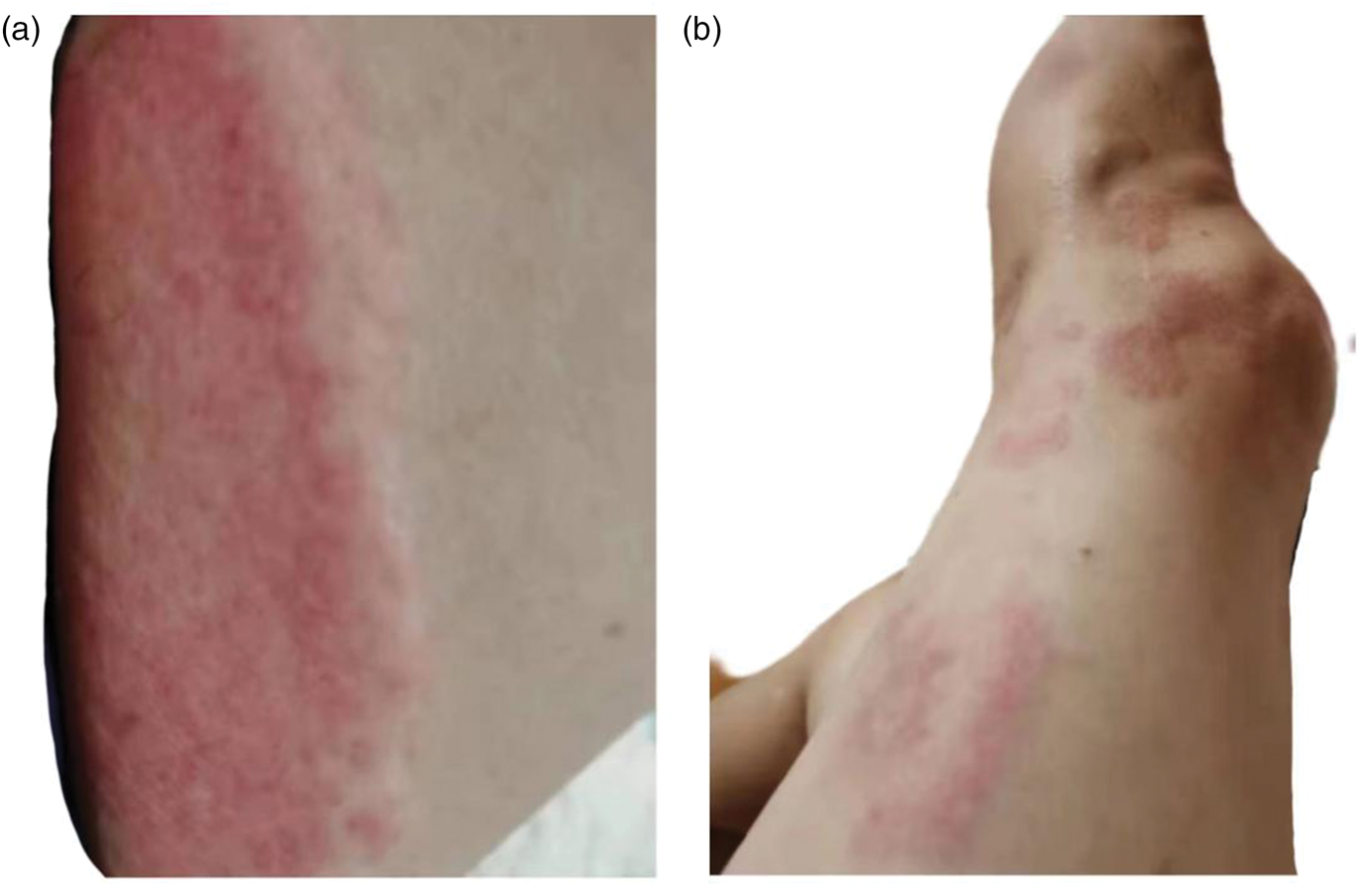
Clinical manifestations of urticaria in the (a) leg and (b) foot. These lesions appeared within aspirin administration and resolved gradually after antihistamine treatment and aspirin withdrawal. Photographs were taken after obtaining written informed consent from the patient.
However, the patient required readmission (second hospitalization) 2 days after discharge due to recurrent urticaria, which he found intolerable. Upon readmission (Day 1 of the second hospitalization), his antiplatelet regimen was switched to ticagrelor, replacing aspirin and clopidogrel, whereas atorvastatin was started in place of rosuvastatin for lipid-lowering and plaque stabilization (Table 1 and Figure 2). Concurrently, desloratadine citrate (qd for 12 days) was initiated for antiallergic treatment, and methylprednisolone (qd for 3 days) was administered for its antiallergic, anti-inflammatory, and immunosuppressive properties. By Day 2, urticaria symptoms had improved, prompting reintroduction of aspirin. Laboratory tests revealed a cardiac troponin I level of 0.007 μg/L and B-type natriuretic peptide level of 97.3 pg/mL, with no additional abnormalities detected. Atorvastatin was discontinued on Day 3 to evaluate its potential role in the recurrent urticaria, as statin-induced skin reactions had been rarely reported. However, on Day 4, severe urticaria recurred in the neck, limbs, and scalp. Methylprednisolone was resumed. Aspirin was withdrawn again on Day 4 to exclude its role in urticaria exacerbation. Subsequent symptom improvement with antiallergic therapy suggested a possible aspirin–allergy link. It is noteworthy that the initial recurrence of urticaria after discharge occurred while the patient was taking three concomitant drugs (aspirin, clopidogrel, and rosuvastatin), which precludes definitive attribution to aspirin alone at that time point. However, during the second hospitalization, aspirin was sequentially withdrawn and reintroduced and other medications were controlled, allowing a clearer causal inference.
Usage, dosage, and pharmacological action of the used drugs.
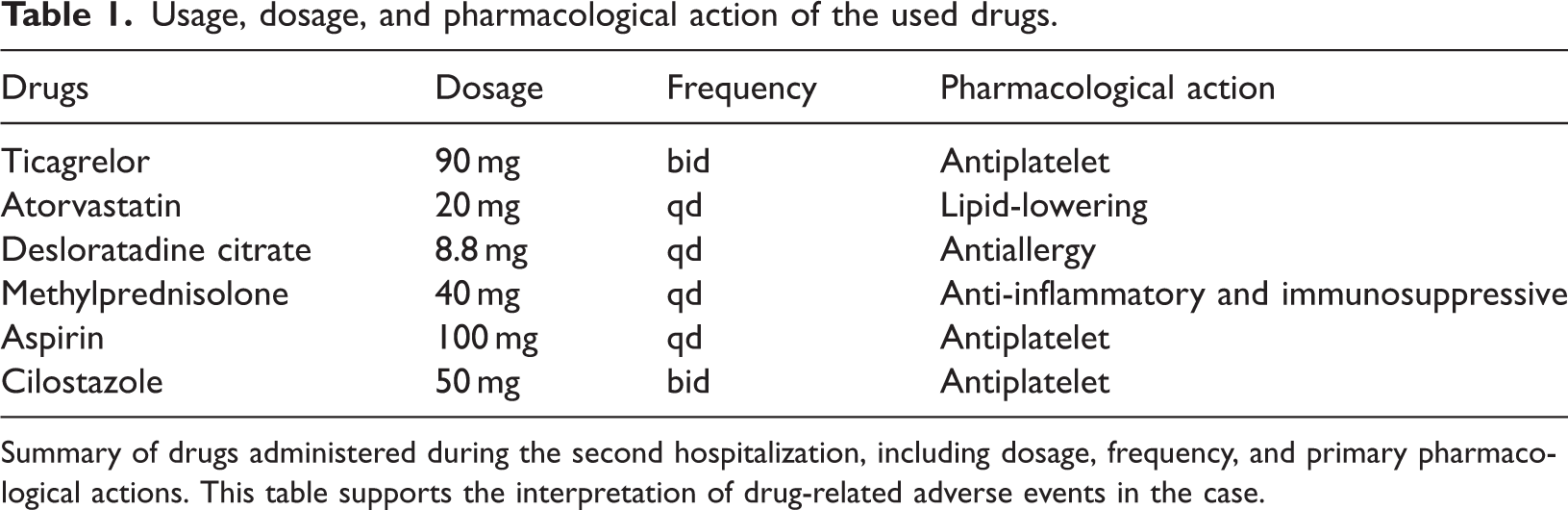
Summary of drugs administered during the second hospitalization, including dosage, frequency, and primary pharmacological actions. This table supports the interpretation of drug-related adverse events in the case.
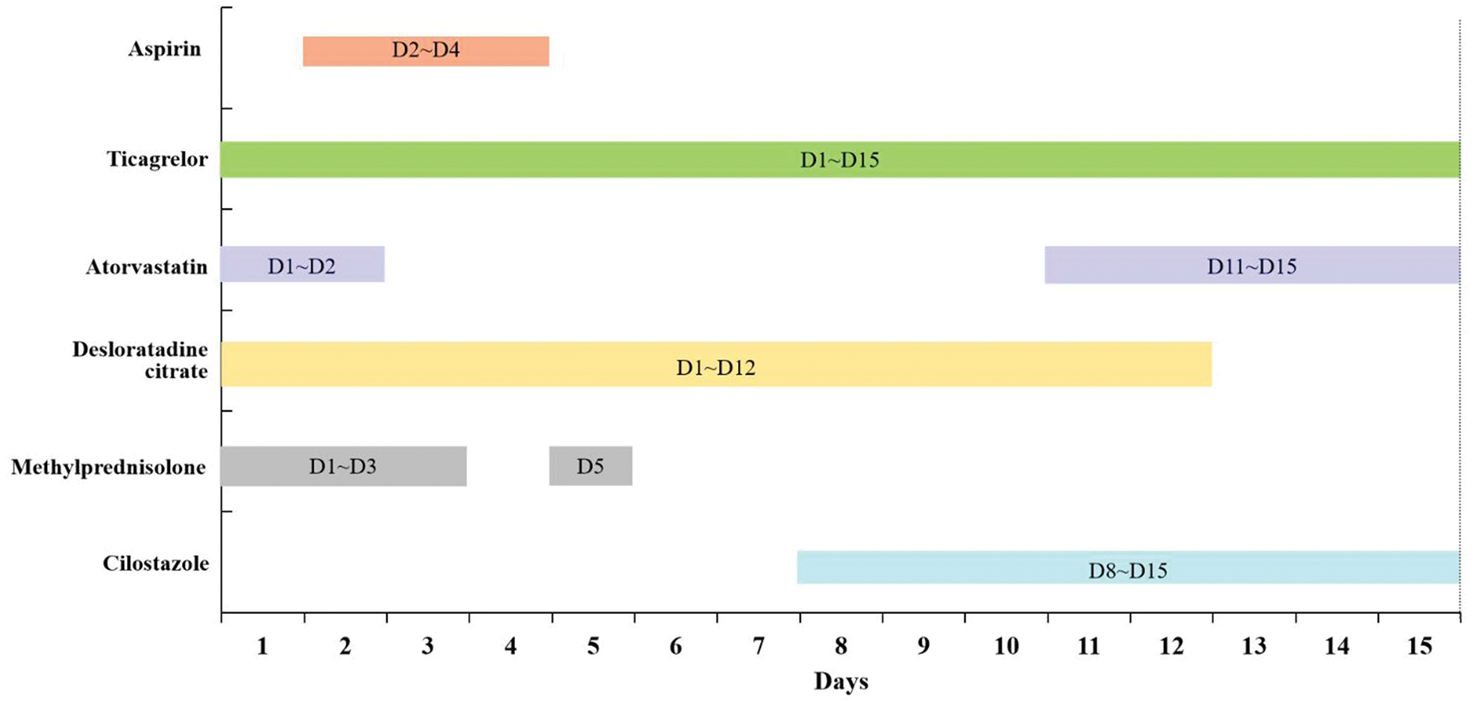
The timeline of drug use during the second hospitalization. The horizontal axis represents hospital days (Day 1–15). Each colored bar indicates the duration of use for a specific drug. Aspirin withdrawal on Day 4 was performed as a single-drug intervention, which helped clarify its role in urticaria recurrence. This timeline illustrates the sequential drug adjustments made to identify aspirin as the causative agent while maintaining antiplatelet therapy.
Given the thrombotic risk, cilostazol was introduced on Day 9 to replace aspirin for antiplatelet aggregation. Atorvastatin was reintroduced on Day 12 without urticaria recurrence, effectively excluding it as the causative allergen. By Day 15, his urticaria had resolved completely, and he was discharged. Postdischarge follow-up by clinical pharmacists confirmed no urticaria relapse, with the patient expressing satisfaction with the treatment and pharmacists’ role. Notably, the initial episode of urticaria occurred shortly after the concurrent initiation of aspirin, clopidogrel, and rosuvastatin, which precludes definitive identification of the causative drug based on the first episode alone. Therefore, causal attribution was primarily based on the subsequent dechallenge and rechallenge events during the second hospitalization. Aspirin was identified as the probable cause of urticaria, with a score of 5 on the ADR causality assessment scale, a validated tool widely used in clinical practice for ADR evaluation.6–8 The reporting of this study conforms to the Case Report (CARE) guidelines. 9
Discussion
Nonsteroidal anti-inflammatory drugs are the second leading cause of drug-induced hypersensitivity reactions, with aspirin hypersensitivity occurring in approximately 0.5%–1.9% of the general population. 10 Previous studies have primarily focused on the epidemiology and pathophysiology of aspirin hypersensitivity, but limited guidance exists regarding the management of such cases in the context of dual antiplatelet therapy, particularly during the critical post-stent period where aspirin is often indispensable. Pharmacists are indispensable in managing and safeguarding patient safety, particularly with regard to polypharmacy, adverse reactions, and prescribing practices.11–13 This case report addresses this gap by providing a detailed account of a multidisciplinary approach to resolve the conflict between thrombotic risk and allergic reactions, offering actionable insights for clinicians.
In this case, although the initial urticaria episode occurred following concurrent administration of three drugs (aspirin, clopidogrel, and rosuvastatin), the subsequent clinical course during the second hospitalization provided stronger evidence for causality. Specifically, reintroduction of aspirin on Day 2 led to severe urticaria recurrence on Day 4, whereas withdrawal of aspirin on Day 4 resulted in gradual symptom improvement. In contrast, atorvastatin was discontinued and reintroduced without any adverse effects, ruling it out as the allergen. These sequential dechallenge and rechallenge events strongly support aspirin as the probable cause of urticaria (ADR causality assessment scale score: 5). The reintroduction of aspirin leading to symptom recurrence further validated aspirin as the allergen, underscoring the necessity of prompt discontinuation of medication in such cases. The successful substitution of aspirin with cilostazol without compromise of antiplatelet efficacy highlights the importance of individualized therapy in high-risk populations.
Urticaria is a localized edematous reaction characterized by wheals and pruritus due to increased small blood vessel permeability. Although the exact mechanism behind aspirin-related urticaria is not fully understood, it is likely related to the diversion of arachidonic acid metabolism from the prostaglandin pathway to the cysteinyl leukotriene pathway, leading to histamine release. 14 Genetic factors, such as specific human leukocyte antigen (HLA) alleles DRB11302 and DQB10609, as well as promoter polymorphisms in the ALOX5 and FcepsilonRIalpha genes, may also play a role in the pathogenesis of aspirin-induced urticaria. 15 A recent study has shown that the combination of transcriptomic and metabolomics methods helps identify unique mRNA genetic markers and low salicylic acid levels in such patients. 16 However, the specificity of genetic and metabolomic differences between this patient and nonallergic patients has not been further investigated. Such analyses may help elucidate the patient’s allergy to aspirin and its potential genetic or metabolic mechanisms. This metabolic shift may result in direct effects on blood vessels and delayed mast cell degranulation, which leads to the release of histamine. Future research to identify these links could help clarify the underlying mechanisms and improve diagnostic accuracy.
Aspirin remains a cornerstone in the management of coronary heart disease; however, its use can pose significant challenges when severe adverse reactions such as urticaria occur. Aspirin desensitization, which modulates the immune response, has been shown as an effective method for controlling allergies. 17 Fortunately, replacing aspirin with alternative agents such as cilostazol and indobufen may be a viable strategy.18,19 Aspirin desensitization is a well-established therapeutic option for post-stent patients with aspirin-induced urticaria, particularly when alternative antiplatelet agents are not suitable or available. The protocol typically involves administering gradually increasing doses of aspirin over several hours to days, thereby inducing temporary tolerance. Although desensitization does not reverse the underlying hypersensitivity, it enables continued aspirin use, which remains the preferred antiplatelet agent according to several guidelines. Given the thrombotic risk associated with aspirin withdrawal early after stenting, desensitization should be considered when alternative agents such as cilostazol and indobufen are contraindicated or less preferred. Studies have demonstrated that cilostazol, when combined with clopidogrel, is associated with lower rates of restenosis and bleeding compared with aspirin. 18 Similarly, indobufen combined with clopidogrel has shown non-inferiority to aspirin and clopidogrel in certain patient populations. 19 These findings suggest that cilostazol or indobufen can serve as practical alternatives to traditional dual antiplatelet regimens. Cilostazol was introduced on Day 9 rather than earlier because the patient was already receiving ticagrelor monotherapy, which provided sufficient antiplatelet protection during the acute allergy workup. Earlier addition of cilostazol could have complicated the causality assessment of the urticaria. In patients requiring antiplatelet monotherapy who are unable to tolerate the adverse effects of aspirin, clopidogrel can be used as an alternative monotherapy. 20
Recent clinical guidelines have addressed the management of aspirin hypersensitivity in patients with acute coronary syndrome (ACS). The 2020 European Society of Cardiology (ESC) guideline for ACS management recommends that in patients with confirmed aspirin allergy, a P2Y12 inhibitor (e.g. clopidogrel or ticagrelor) monotherapy or dual antiplatelet therapy with alternative agents may be considered after specialist consultation. 21 Similarly, the 2021 American Heart Association(AHA)/American College of Cardiology (ACC) chest pain guideline emphasizes the role of aspirin desensitization in appropriate settings, particularly when no alternative antiplatelet agent is available. 22 For patients undergoing percutaneous coronary intervention, desensitization protocols may be safe and effective, enabling continued aspirin use without allergic recurrence. In our case, given the recurrent and severe urticaria, we opted for a desensitization-sparing strategy using cilostazol as an alternative, which aligns with the individualized approach recommended in recent guidelines.
Several clinical decisions in this case were made based on a balance between antithrombotic necessity and allergy control. First, aspirin was reintroduced on Day 2 of the second hospitalization to confirm causality, as its rapid withdrawal and rechallenge are standard in ADR evaluation. Second, the dose of methylprednisolone (40 mg qd for 3 days) was decided according to the institutional protocol for moderate-to-severe drug-induced urticaria without anaphylaxis, with the aim of achieving rapid symptom control and minimizing prolonged immunosuppression. Third, cilostazol (50 mg bid) was chosen over other antiplatelets based on published evidence showing its efficacy and safety as an aspirin alternative in aspirin-intolerant post-stent patients, and the dose was adjusted according to renal function and body weight. Fourth, atorvastatin was discontinued and reintroduced after a 9-day gap to exclude its allergenic potential, as delayed hypersensitivity to statins, though rare, has been reported. These timing and dosing strategies were determined collaboratively by the multidisciplinary team, integrating pharmacological principles and real-time clinical response. The intermittent use of methylprednisolone in this case reflected a stepwise approach, including an initial short course for acute symptom control followed by resumption upon symptom recurrence, which helped confirm the temporal relationship with aspirin exposure.
The main value of our report lies in the preliminary clinical observations and hypothesis generation. It provides a clear, step-by-step medication reconciliation and rechallenge protocol under pharmacist-led monitoring. It also validates the feasibility of replacing aspirin with cilostazol in dual antiplatelet therapy without increasing the thrombotic risk. These elements offer actionable insights for clinicians facing similar dilemmas. However, the single-case nature of this report limits the generalizability of its conclusions. Additionally, the absence of genetic or pharmacological testing (e.g. serum tryptase, leukotriene levels, and HLA typing) to confirm aspirin hypersensitivity represents a diagnostic gap. These tests were not performed due to lack of routine clinical availability and the need for timely management in our high-risk cardiovascular patient. The initial reaction occurred when multiple drugs were initiated simultaneously, complicating the determination of causality from this single event. Nevertheless, the positive rechallenge test using aspirin during the second hospitalization reinforced the causal link. It is noteworthy that the first rechallenge was confounded by the concurrent administration of clopidogrel and rosuvastatin. Although sequential drug manipulation during the second hospitalization ultimately identified aspirin as the probable culprit, the initial complexity underscores the difficulty of attributing adverse reactions in polypharmacy scenarios and supports the use of structured causality assessment tools. Despite the supportive temporal relationship, a multifactorial cause cannot be entirely dismissed. Additionally, a limitation of this case is that clopidogrel was discontinued alongside aspirin when switching to ticagrelor, which prevents the definitive exclusion of clopidogrel as a potential cause of the urticaria. To address this, future investigations should employ sequential withdrawal or drug provocation testing to pinpoint the responsible agent more accurately in similar cases. Future larger cohorts and standardized diagnostic protocols are needed to validate these findings and further investigate the long-term safety and efficacy of alternative antiplatelet agents.
Conclusion
This case highlights that a multidisciplinary approach, involving close collaboration between clinicians and clinical pharmacists, can help effectively manage aspirin-induced urticaria in a post-stent patient and maintaining cardiovascular safety. Replacing aspirin with cilostazol may be a viable alternative in similar hypersensitive patients. Further studies are warranted to validate these observations and explore the underlying mechanisms.
Footnotes
Acknowledgment
None.
Authors contribution
KLM conceived the drafting of the case and was responsible for the integrity of the work. LCL and YYX wrote the original draft. LCL, YF, YYX, and SZ analyzed the medication, reviewed the literature, and created the table and figures. All authors have read and approved the final manuscript.
Copyright and permissions
All figures and tables in this manuscript are original works created by the authors. No previously published or third-party copyrighted materials are used. The patient’s clinical images are published with written informed consent obtained from the patient as detailed in the “Ethics Statement and Informed Consent” section.
Data availability statement
Data are provided within the manuscript or supplementary information files.
Declaration of conflicting interests
The authors declare no conflicts of interest.
Ethics statement and informed consent
This report was approved by the Medical Ethics Committee of Zhejiang Provincial People’s Hospital (Hangzhou, China; Approval No. QT2023026; Date of approval: Feb 1, 2023). Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Funding
This work was supported by the Zhejiang Province Medical and Health Science and Technology Planning Project (No. 2025KY641), the Special Research Funding Project for High-Quality Development of Hospital Pharmacy and Pharmaceutical Affairs Management in Medical Communities of Zhejiang Pharmaceutical Association (No. 2025ZGYY17), and Zhejiang Provincial Natural Science Foundation of China (No. LYY19H280006).