
Abstract
Objective
Chronic obstructive pulmonary disease is a progressive inflammatory lung disease characterized by chronic bronchitis and emphysema. This study aimed to evaluate the levels of composite inflammatory markers, including systemic immune-inflammation index, systemic inflammatory response index, pan-immune-inflammation value, neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, hemoglobin-to-red cell distribution width ratio, hemoglobin-to-monocyte ratio, and hemoglobin-to-white blood cell count ratio, in patients presenting with acute exacerbation of chronic obstructive pulmonary disease.
Methods
This retrospective observational study included patients aged ≥40 years who presented to a tertiary Chest Diseases clinic between 2022 and 2024 with acute exacerbation of chronic obstructive pulmonary disease. Patients were categorized into two groups (outpatient treatment and hospitalization groups) according to the management strategy used. Hematological parameters and composite inflammatory indices were calculated and compared between the groups.
Results
In total, 314 patients were included; 80.3% of them were male. Hospitalized patients were significantly older and had higher white blood cell counts, C-reactive protein levels, neutrophil-to-lymphocyte ratios, platelet-to-lymphocyte ratios, systemic immune-inflammation indices, systemic inflammatory response indices, and pan-immune-inflammation values than outpatients (all p < 0.001). In contrast, the hemoglobin-to-red cell distribution width, hemoglobin-to-monocyte, and hemoglobin-to-white blood cell count ratios were significantly lower in hospitalized patients (all p < 0.001).
Conclusions
Composite inflammatory indices derived from routine blood tests may reflect the systemic inflammatory burden during acute exacerbation of chronic obstructive pulmonary disease and may support the clinical assessment of hospitalization risk.
Keywords
Introduction
Chronic obstructive pulmonary disease (COPD) is a common chronic inflammatory lung disease characterized by progressive and irreversible airflow limitation, accompanied by symptoms such as dyspnea, cough, and sputum production. 1 COPD negatively affects the quality of life, imposes a substantial economic burden on healthcare systems, and is associated with increased morbidity and mortality worldwide. 2 Pathologically, COPD consists of two major components, chronic bronchitis, characterized by small airway disease and peribronchiolar fibrosis, and emphysema, which involves destruction of alveolar walls and is typically identified using computed tomography (CT). 3 Chronic inflammation, primarily triggered by environmental exposures, plays a central role in these pathological processes. Persistent inflammatory responses in the lung parenchyma and airways contribute to tissue destruction, impaired repair mechanisms, fibrosis, and progressive airflow limitation.4,5
There is growing interest in the identification of accessible biomarkers that reflect inflammatory activity during acute COPD exacerbation and may assist in clinical assessment. Composite inflammatory indices derived from complete blood count parameters—such as systemic immune-inflammation index (SII), systemic inflammatory response index (SIRI), pan-immune-inflammation value (PIV), and neutrophil-to-lymphocyte ratio (NLR)—have been investigated in various inflammatory and respiratory conditions.6,7 Recent studies have explored the role of these markers in lung diseases and COPD, particularly during exacerbation periods.8,9 However, data regarding their association with hospitalization status during acute exacerbation remain limited.
These indices are inexpensive, easily obtainable, and routinely available in clinical practice. Because they integrate multiple hematologic parameters, they may provide a broader reflection of systemic inflammatory burden compared with single laboratory markers. In this study, we evaluated SII, SIRI, platelet-to-lymphocyte ratio (PLR), PIV, NLR, hemoglobin-to-red cell distribution width ratio (Hb/RDW), hemoglobin-to-monocyte ratio (Hb/Mon), and hemoglobin-to-white blood cell count ratio (Hb/WBC) during acute exacerbation of COPD and investigated whether these indices differed between patients managed with hospitalization and those treated in the outpatient setting.
Materials and methods
This retrospective observational study was conducted by reviewing the medical records of patients diagnosed with acute exacerbation of COPD who presented to the Chest Diseases clinic between 2022 and 2024. The study was performed in accordance with the principles of the Declaration of Helsinki (1975, revised in 2024). Ethical approval was obtained from the Baskent University Institutional Review Board, Ankara, Turkey (Protocol No: KA:24/425). Due to the retrospective design of the study and the use of anonymized data, the requirement for written informed consent was waived by the ethics committee. All patient data were deidentified prior to analysis.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 10
Patient selection
The study included patients aged ≥40 years who were diagnosed with COPD and presented to the Chest Diseases clinic with acute exacerbation between 2022 and 2024. Medical records of patients who met the study criteria were retrospectively reviewed.
Acute exacerbation of COPD was defined as worsening of respiratory symptoms, including increased dyspnea, wheezing, increased sputum volume, and/or change in sputum color, lasting at least 2 consecutive days and requiring treatment with antibiotics and/or systemic corticosteroids.
Patients were categorized into two groups according to the management strategy. One group comprised those who required hospitalization, whereas the second included those treated in the outpatient setting without hospitalization.
Statistical analyses
All statistical analyses were performed using Python (pandas, scipy, and seaborn libraries). Descriptive statistics were presented as median (interquartile range (IQR)) values for continuous variables that did not follow a normal distribution. The normality of data was assessed using the Shapiro–Wilk test, and as most variables did not follow a normal distribution, non-parametric tests were applied.
To compare differences between outpatients and inpatients, the Mann–Whitney U test was performed for continuous variables. The test results were reported as Mann–Whitney U test values and p-values, where a p-value <0.05 was considered statistically significant. Additionally, the median and IQR values were calculated separately for the outpatient and inpatient groups to facilitate comparisons.
To visualize the distribution of key hematological and inflammatory markers, boxplots were generated for each variable, comparing outpatients and inpatients.
Results
This study included a total of 314 patients, of whom 252 (80.3%) were male, and 62 (19.7%) were female. Among the patients, 196 (62.4%) were treated as outpatients, whereas 118 (37.6%) required hospitalization. When evaluated according to sex and admission type, 36 female patients (58.1%) were treated as outpatients, and 26 (41.9%) were hospitalized. Similarly, 160 male patients (63.5%) received outpatient treatment, whereas 92 (36.5%) required hospitalization. The mean length of hospital stay for inpatients was 5.04 ± 2.98 days.
Table 1 presents a comparison of clinical and laboratory parameters between outpatient and inpatient groups. The median age of hospitalized patients was significantly higher (median = 74.00, IQR = 12.75) than that of outpatients (median = 65.00, IQR =18.00; p < 0.001). Similarly, the white blood cell (WBC) count, neutrophil count (Neu), and NLR were significantly higher in the inpatient group (p < 0.001). In addition, the C-reactive protein (CRP) levels of hospitalized patients were also markedly elevated (median = 45.85, IQR = 62.35) compared with those of outpatients (median = 17.40, IQR = 21.10; p < 0.001), indicating increased systemic inflammation.
Comparison of clinical and laboratory parameters between outpatients and inpatients.

IQR: interquartile range; WBC: white blood cell; Neu: neutrophil count; Lym: lymphocyte count; Mon: monocyte count; Eosin: eosinophil count; Plt: platelet count; HGB: hemoglobin; RDW: red cell distribution width; CRP: C-reactive protein; NLR: neutrophil-to-lymphocyte ratio; Hb/RDW: hemoglobin-to-red cell distribution width ratio; Hb/WBC: hemoglobin-to-white blood cell count ratio; Hb/Mon: hemoglobin-to-monocyte ratio; SII: systemic immune-inflammation index; SIRI: systemic inflammatory response index; PIV: pan-immune-inflammation value; PLR: platelet-to-lymphocyte ratio.
Conversely, lymphocyte counts (Lyms) were significantly lower in inpatients (p < 0.001). Hemoglobin (HGB) levels were also lower in hospitalized patients (median = 13.10, IQR = 2.10) than in outpatients (median = 14.60, IQR = 2.80; p < 0.001). In addition, composite inflammatory indices, including SII, SIRI, and PIV, were significantly higher in hospitalized patients (p < 0.001). These findings suggest that hospitalized patients exhibit greater inflammatory burden during acute COPD exacerbation.
Figure 1 illustrates the distribution of clinical and laboratory parameters between outpatient and inpatient groups. Inflammatory markers such as WBC, CRP, NLR, SII, SIRI, and PIV were generally higher among hospitalized patients, whereas Lyms and HGB levels tended to be lower. The boxplots confirm the results of the Mann–Whitney U test and visually demonstrated the differences between the two groups.
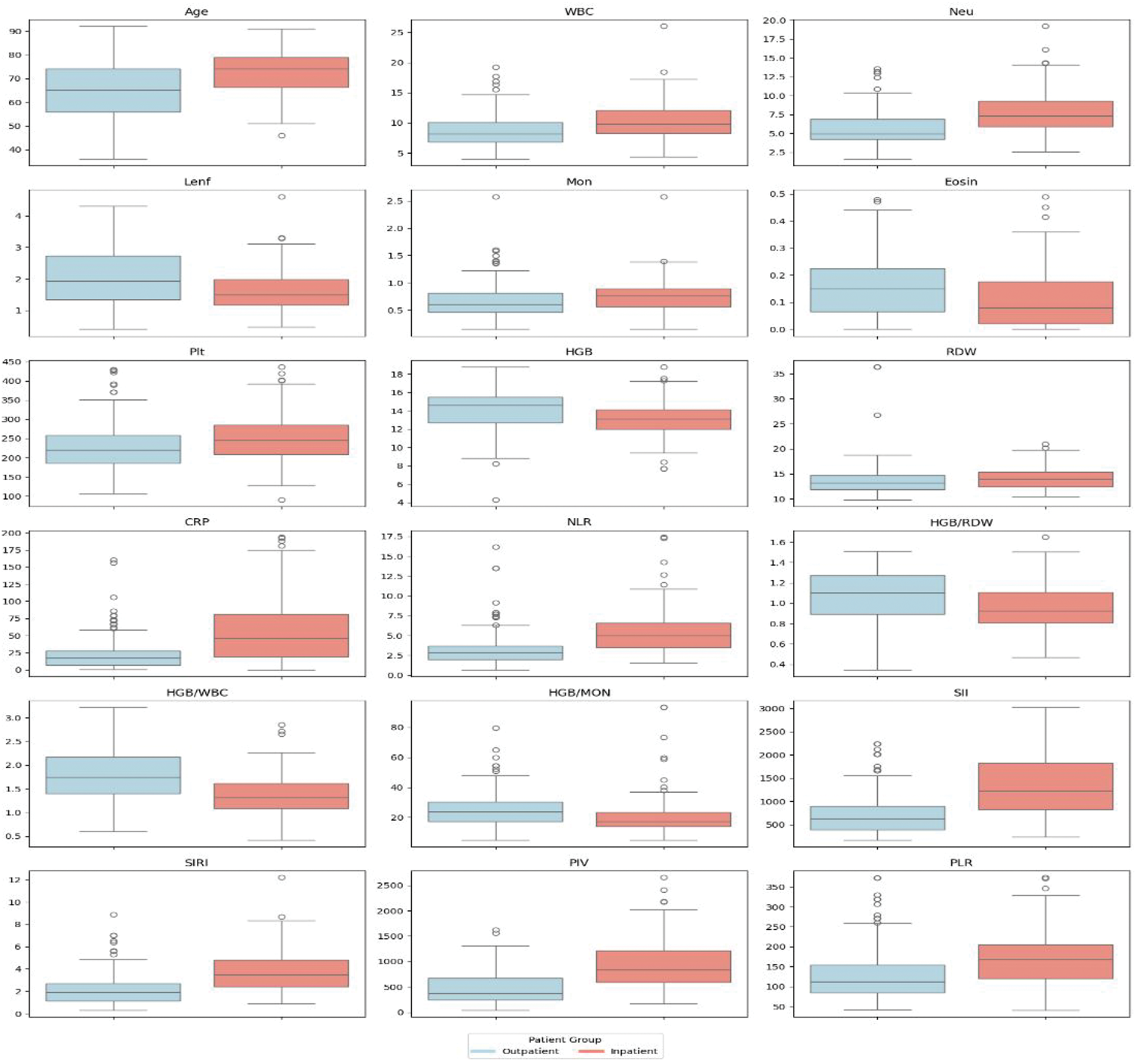
Comparison of clinical and laboratory parameters between outpatients and inpatients (boxplots).
Logistic regression and receiver operating characteristic (ROC) analyses for hospitalization
To evaluate the factors associated with hospitalization, age-adjusted logistic regression analyses were performed for each inflammatory marker. The results are presented in Table 2. Age was significantly associated with hospitalization in all models (odds ratio (OR) = 1.07, p < 0.001). In the age-adjusted models, the SII, SIRI, PIV, NLR, and CRP levels were significantly associated with hospitalization (p < 0.001). Among the evaluated markers, the SIRI (OR = 1.88, 95% confidence interval (CI): 1.56–2.25) and NLR (OR = 1.46, 95% CI: 1.28–1.66) demonstrated relatively stronger associations with hospitalization.
Age-adjusted and multivariable logistic regression analyses for predictors of hospitalization.
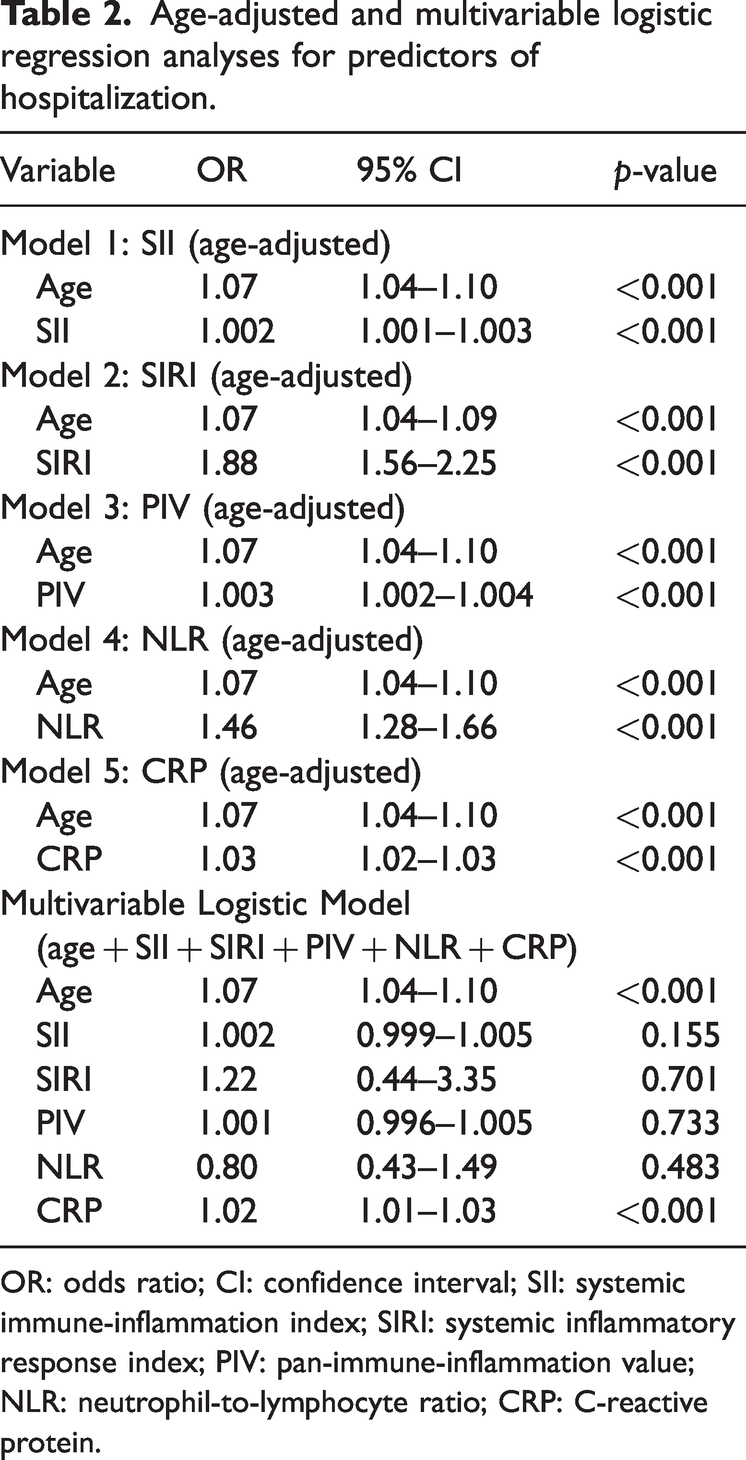
OR: odds ratio; CI: confidence interval; SII: systemic immune-inflammation index; SIRI: systemic inflammatory response index; PIV: pan-immune-inflammation value; NLR: neutrophil-to-lymphocyte ratio; CRP: C-reactive protein.
A multivariable logistic regression model including age, SII, SIRI, PIV, NLR, and CRP level was also constructed to evaluate their combined effects. In the multivariable model, age (OR = 1.07, 95% CI: 1.04–1.10, p < 0.001) and CRP level (OR = 1.02, 95% CI: 1.01–1.03, p < 0.001) remained independently associated with hospitalization, whereas SII, SIRI, PIV, and NLR did not remain statistically significant after adjustment.
To further assess the discriminative ability of the inflammatory markers, ROC curve analyses were performed (Table 3). Among the evaluated markers, PIV demonstrated the highest discriminative performance (area under the curve (AUC) = 0.802, 95% CI: 0.751–0.851), followed by the SII (AUC = 0.798, 95% CI: 0.745–0.848) and SIRI (AUC = 0.791, 95% CI: 0.739–0.841). The NLR also showed good discriminative performance (AUC = 0.781, 95% CI: 0.728–0.831), whereas CRP level showed moderate performance (AUC =0.729, 95% CI: 0.671–0.787).
ROC analysis and diagnostic performance of inflammatory markers and the multivariable model for predicting hospitalization.
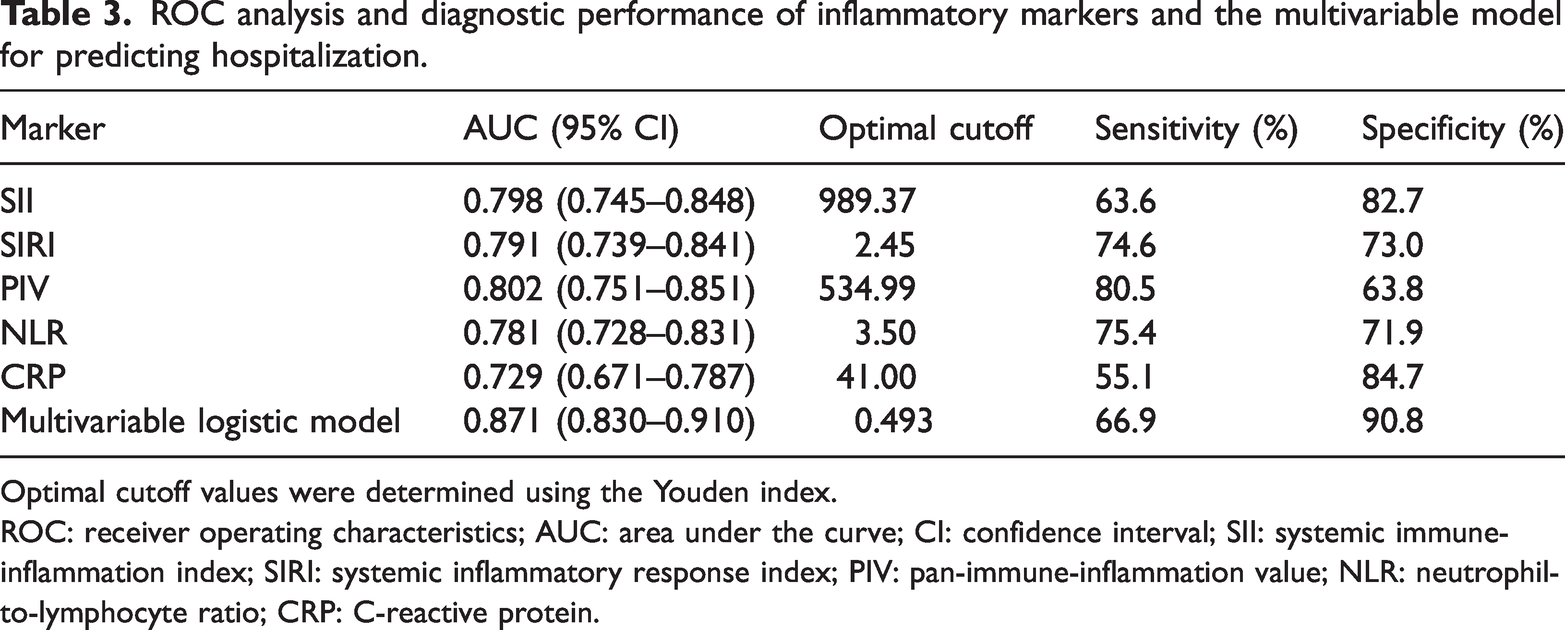
Optimal cutoff values were determined using the Youden index.
ROC: receiver operating characteristics; AUC: area under the curve; CI: confidence interval; SII: systemic immune-inflammation index; SIRI: systemic inflammatory response index; PIV: pan-immune-inflammation value; NLR: neutrophil-to-lymphocyte ratio; CRP: C-reactive protein.
The ROC curves of individual inflammatory markers and the multivariable logistic regression model are presented in Figure 2. The multivariable model demonstrated the highest predictive performance (AUC =0.871), indicating improved discrimination compared with individual inflammatory markers.
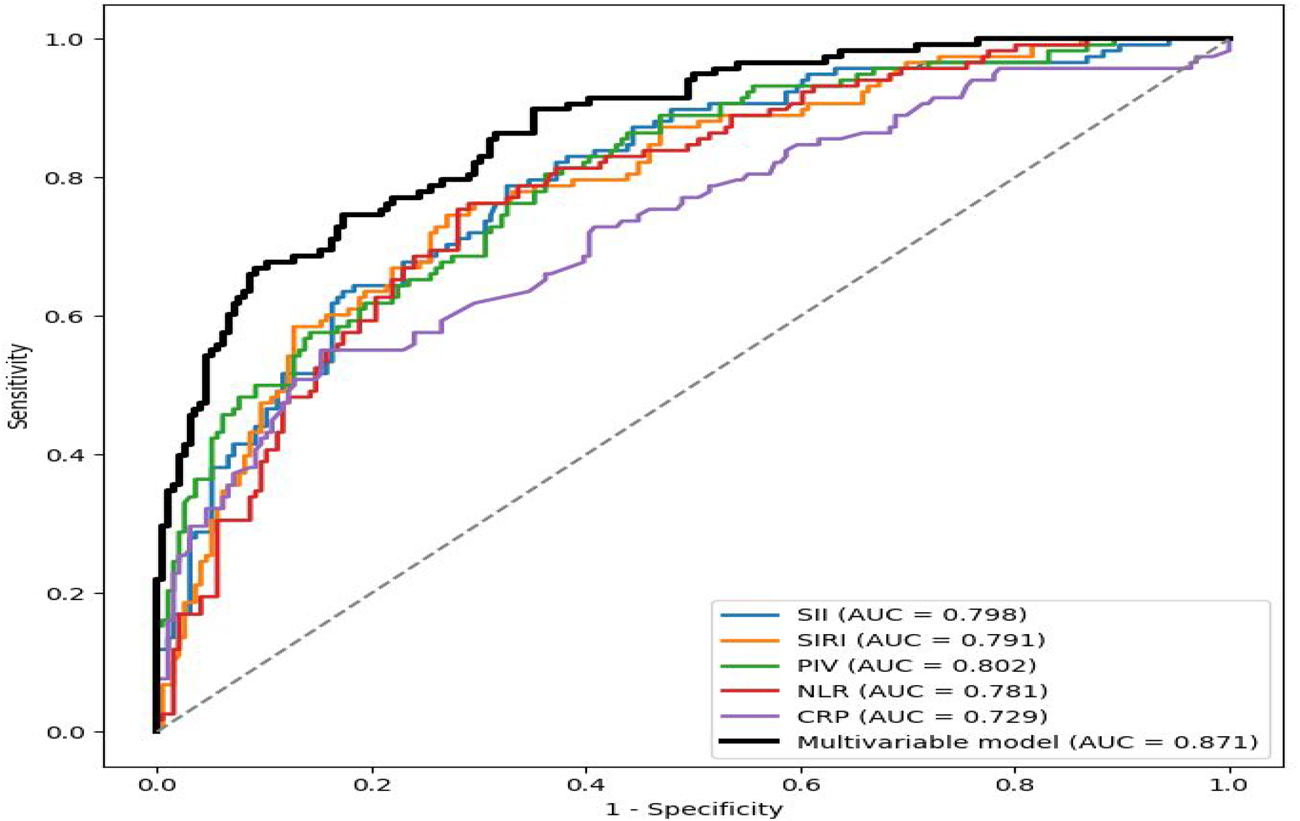
ROC curves of inflammatory markers and multivariable logistic regression model for predicting hospitalization. ROC: receiver operating characteristic.
Discussion
COPD is a common, irreversible, and progressive airflow limitation of the airways. The underlying cause of this airflow limitation is chronic airway inflammation. Persistent inflammation and airflow restriction ultimately result in dyspnea and other clinical manifestations. Pathologically, COPD includes emphysema and chronic bronchitis and is often referred to by these terms. 11
COPD has become a major global health problem and is one of the leading causes of morbidity and mortality worldwide. 2 It frequently progresses with acute exacerbations, during which airway and systemic inflammation increase. 12 In patients with COPD, inflammatory cell infiltration—particularly that of neutrophils and macrophages—is prominent. Activation of T cells and other inflammatory cells may contribute to structural damage in the airways and alveolar regions. The balance between Th1 and Th2 cells, along with macrophage and dendritic cell activity, may influence disease severity and clinical presentation.13–15
The NLR is a simple and objective marker for systemic inflammation. Neutrophils and lymphocytes play central roles in immune response, and NLR reflects the balance between these two cell types. 16 Previous studies have demonstrated that NLR increases during acute exacerbations of COPD and correlates with inflammatory activity, demonstrating performance comparable with that of CRP level in reflecting systemic inflammation.8,17 Another study has shown that the NLR is higher during acute exacerbations than during stable periods. 18 In our study, consistent with the literature, both NLR and CRP level were elevated during exacerbation, and NLRs were significantly higher in hospitalized patients than in outpatients. These findings suggest that the NLR reflects inflammatory burden during exacerbation and is associated with hospitalization status.
The PLR, similar to the NLR, is another indicator of systemic inflammation. Platelet activation has been associated with structural changes in the pulmonary vasculature and may occur during both stable COPD and exacerbation periods. 19 Inflammatory cytokines may contribute to thrombocytosis, and activated platelets can interact with endothelial cells and leukocytes, amplifying the inflammatory processes. Increased PLRs associated with lymphopenia have been reported in COPD. 20 Limited studies have shown that PLRs rise during acute exacerbations compared with that during the stable phase.21,22 In our study, PLRs were elevated during exacerbation and were significantly higher in hospitalized patients, supporting their association with increased inflammatory activity.
SII is a quantitative marker that reflects the balance between inflammatory and immune components. Elevated Neu and platelet counts combined with reduced Lyms contribute to higher SIIs. Previous studies have demonstrated its association with disease severity in various clinical conditions.23,24 In COPD populations, increased SIIs during exacerbation have been reported.25,26 In our study, SIIs were significantly higher in hospitalized patients, suggesting that this index reflects the intensity of systemic inflammation during exacerbation.
PIV is a relatively new composite marker that incorporates Neus, Lyms, as well as monocyte and platelet counts. Its clinical relevance has been demonstrated in several inflammatory conditions. 27 Elevated monocyte-related inflammatory pathways have also been described in COPD. 28 During exacerbations, Neu, platelet, and monocyte counts tend to increase, whereas Lyms decrease, resulting in elevated PIVs and SIRIs.8,29 In our study, PIVs were higher in hospitalized patients, indicating an association with greater inflammatory burden during acute exacerbation.
In addition to descriptive comparisons, logistic regression analyses were performed to evaluate the association between inflammatory markers and hospitalization. In the age-adjusted models, the SII, SIRI, PIV, NLR, and CRP levels were significantly associated with hospitalization status. Among these markers, SIRI and NLR demonstrated relatively stronger associations with hospitalization status. However, in the multivariable logistic regression model including all inflammatory indices, only age and CRP level remained independently associated with hospitalization status. This finding may be explained by the strong correlation between composite inflammatory indices derived from similar hematological parameters. Furthermore, ROC analysis demonstrated that PIV, SII, SIRI, and NLR showed good discriminative performance (AUC, approximately 0.78–0.80), whereas the multivariable model combining age and inflammatory markers achieved the highest predictive performance (AUC = 0.871). These findings suggest that combining inflammatory markers with clinical variables improves the assessment accuracy of hospitalization risk in patients with acute exacerbation of COPD.
The Hb/RDW has recently been investigated as an inflammation-related marker. A decreased Hb/RDW may reflect the combined effect of anemia and elevated red cell distribution width (RDW) in inflammatory states. Although limited data exist, previous studies have reported associations between the Hb/RDW and inflammatory conditions.30,31 In our study, Hb/RDWs were significantly lower in hospitalized patients, suggesting that this ratio also reflects systemic inflammatory intensity during COPD exacerbation.
Similarly, the Hb/WBC represents the relationship between HGB levels and leukocyte counts. Decreased HGB levels and increased WBC counts may occur in inflammatory states. In our cohort, Hb/WBCs were lower in hospitalized patients, indicating a possible association with higher inflammatory activity. However, further studies are required to clarify its clinical relevance in COPD.
Monocytes play a central role in inflammatory responses and can differentiate into macrophages and dendritic cells. 32 Their mobilization and migration during inflammatory processes have been well described.33,34 Increased peripheral monocyte counts during inflammation may contribute to lower Hb/Mons. In our study, Hb/Mons were significantly lower in hospitalized patients, which may reflect heightened inflammatory activation during COPD exacerbation.
Overall, our findings indicate that composite inflammatory indices derived from routine complete blood count parameters are associated with hospitalization status in patients with acute exacerbation of COPD. In particular, indices such as SII, SIRI, PIV, and NLR demonstrated significant associations with hospitalization in age-adjusted analyses and showed good discriminative performance in ROC analysis. These markers may reflect systemic inflammatory burden during exacerbation and could support clinical assessment when interpreted alongside established clinical parameters.
Limitations
This study has certain limitations that should be considered when interpreting the results. First, the retrospective design may have introduced selection bias and limits the ability to establish causal relationships between inflammatory markers and hospitalization status. Second, detailed clinical variables that may influence exacerbation severity—such as the Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage, baseline maintenance therapy, and comorbid conditions—were not available in our dataset. In addition, important clinical outcomes, including the need for noninvasive or invasive mechanical ventilation, intensive care unit admission, as well as mortality and readmission rates, were not systematically recorded. Therefore, hospitalization status was used as a pragmatic indicator of exacerbation severity in the present study.
Another limitation is that the study was conducted at a single center, which may limit the generalizability of the findings to other populations. Furthermore, although several inflammatory indices derived from complete blood count parameters were evaluated, these markers share common hematologic components and may therefore exhibit intercorrelations in multivariable analyses.
Despite these limitations, the study evaluated multiple composite inflammatory indices simultaneously in a relatively large sample. In addition, we performed multivariable logistic regression and ROC analyses, which strengthened the statistical power of the analyses examining the association between inflammatory markers and hospitalization status during acute exacerbation of COPD.
Conclusion
Composite inflammatory indices derived from routine complete blood count parameters were associated with hospitalization status in patients presenting with acute exacerbation of COPD in our study. In particular, indices such as SII, SIRI, PIV, and NLR showed significant associations with hospitalization in age-adjusted analyses and demonstrated good discriminative performance in the ROC analysis. However, in multivariable models, age and CRP levels remained independently associated with hospitalization, suggesting that these markers share overlapping inflammatory components.
Overall, these findings suggest that composite inflammatory indices reflect the systemic inflammatory burden during acute exacerbation of COPD and may provide additional information for clinical assessment when interpreted alongside established clinical parameters. Further prospective studies including detailed clinical severity measures are needed to confirm the potential clinical utility of these biomarkers.
Footnotes
Acknowledgments
The authors would like to thank the hospital administration and medical records department for their support in accessing the patient data used in this retrospective study.
Author contributions
Design: Yildiz Ucar
Data: Yildiz Ucar, Aynur Yonar, and Keziban Karabulut Ucar
Collection or Processing: Yildiz Ucar and Aynur Yonar
Analysis or Interpretation: Aynur Yonar
Literature Search: Yildiz Ucar, Keziban Karabulut Ucar
Writing: Yildiz Ucar
Data availability
All data generated or analyzed during this study are included in this published article and its supplementary information files.
Declaration of conflicting interests
The authors declare no competing interests.
Funding
The authors received no financial support for the research, authorship, and/or publication of this study.