
Abstract
Objective
To identify risk factors for futile recanalization after mechanical thrombectomy in patients with acute ischemic stroke and develop an interpretable nomogram for risk stratification.
Methods
This multicenter retrospective study included 350 patients with acute ischemic stroke who underwent mechanical thrombectomy. A development cohort consisting of 260 patients was derived from two centers, and an external validation cohort comprising 90 patients was obtained from an independent center. Futile recanalization was defined as a 90-day modified Rankin Scale score >2 despite successful recanalization. Clinical, imaging, and perioperative variables were collected. The development cohort was randomly divided into training and test cohorts in a 7:3 ratio. Least absolute shrinkage and selection operator regression and multivariable logistic regression were used to identify independent predictors, and a nomogram was developed. Model performance was evaluated using receiver operating characteristic analysis, calibration assessment including calibration curve, calibration slope, calibration intercept, and Brier score, and decision curve analysis. External validation was performed to evaluate model generalizability.
Results
Of 350 included patients, 152 (43.43%) experienced futile recanalization. Higher baseline National Institutes of Health Stroke Scale score, lower Alberta Stroke Program Early CT Score, elevated admission blood glucose levels, poor collateral circulation, and longer onset-to-recanalization time were identified as independent predictors of futile recanalization. The nomogram demonstrated acceptable discriminative ability, with area under the receiver operating characteristic curve values of 0.84 (95% confidence interval: 0.78–0.84), 0.86 (95% confidence interval: 0.78–0.86), and 0.8 (95% confidence interval: 0.7–0.8) in the training, test, and external validation cohorts, respectively. Calibration was satisfactory, and decision curve analysis indicated potential clinical utility.
Conclusions
This multicenter retrospective study developed a nomogram with acceptable discriminative ability, satisfactory calibration, and potential clinical utility for predicting futile recanalization after mechanical thrombectomy in acute ischemic stroke. The model may support perioperative risk stratification and individualized management; however, further validation in larger prospective cohorts is warranted.
Keywords
Introduction
Acute ischemic stroke (AIS) is a leading cause of mortality and long-term disability worldwide, with its incidence and disability burden continuing to rise, thereby imposing substantial socioeconomic and healthcare burdens on patients, families, and healthcare systems. 1 For patients with AIS caused by large vessel occlusion (LVO), mechanical thrombectomy (MT) is the most effective strategy for achieving vascular recanalization. 2 Following the publication of multiple landmark randomized controlled trials in 2015, including MR CLEAN, ESCAPE, and SWIFT PRIME, which demonstrated significant clinical efficacy, MT has been incorporated into national and international stroke treatment guidelines and has substantially improved recanalization rates and long-term functional outcomes in selected patients.3–5
However, with the widespread adoption of MT in clinical practice, an important and increasingly recognized phenomenon has emerged. Despite successful angiographic recanalization, a substantial proportion of patients fail to achieve favorable neurological outcomes. Previous studies have reported that approximately 30%–50% of patients with AIS continue to experience poor functional outcomes at 90 days, even after technically successful recanalization, a phenomenon commonly known as futile recanalization (FR).6,7 Futile recanalization is generally defined as the absence of meaningful neurological recovery following successful vascular recanalization, typically reflected by a modified Rankin Scale (mRS) score >2 at 90 days after treatment. 8 This phenomenon indicates that evaluating treatment success solely on the basis of vessel recanalization is insufficient, as multiple factors, including cerebral tissue perfusion, reperfusion-related injury, and individual physiological heterogeneity, collectively influence clinical outcomes.
At present, a growing body of evidence has investigated risk factors associated with FR following MT. Previous studies have suggested that higher baseline National Institutes of Health Stroke Scale (NIHSS) score, lower Alberta Stroke Program Early CT Score (ASPECTS), prolonged onset-to-recanalization time (OTR), poor collateral circulation, and postoperative hemorrhage may be closely associated with the occurrence of FR.9,10 However, heterogeneity in study design, patient populations, and outcome definitions across studies has resulted in limited consistency and robustness of these findings. Moreover, most existing investigations have focused on isolated risk factor analyses, and an intuitive predictive tool that integrates multiple key variables to enable individualized risk assessment remains lacking in routine clinical practice.
Nomograms, visual prediction tools derived from regression-based models, integrate multiple independent risk factors into a concise and intuitive scoring system and have been widely used in clinical risk assessment in oncology, cardiovascular diseases, and cerebrovascular diseases.11,12 Compared with reliance on single indicators, nomogram-based models offer improved interpretability and clinical utility, providing quantitative support for decision-making in treatment planning. Nevertheless, studies developing nomogram-based prediction models for FR after MT in patients with AIS remain limited, particularly those incorporating multicenter data and external validation.
Based on these considerations, this multicenter retrospective study systematically analyzed patients with AIS who underwent MT to identify independent risk factors associated with FR. On this basis, an interpretable nomogram prediction model was developed and validated to enable early identification and individualized assessment of the risk of FR after treatment. This model was developed with an aim to support precise clinical decision making, optimize reperfusion strategies, and ultimately improve patient outcomes.
Materials and methods
Study population
This study was conducted as a multicenter retrospective cohort study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 13 A total of 260 patients with AIS who underwent MT between January 2023 and November 2025 were retrospectively enrolled to form the development cohort. Patients were treated at the Department of Neurosurgery, Ji’an Central People’s Hospital, and the Department of Neurology, The Affiliated Hospital of Xuzhou Medical University. Particularly, 170 patients were enrolled from Ji’an Central People’s Hospital and 90 from The Affiliated Hospital of Xuzhou Medical University. The development cohort was randomly divided into training and test cohorts in a 7:3 ratio.
In addition, patients with AIS who underwent MT at the Department of Neurology, The Affiliated Changshu Hospital of Soochow University, between January 2025 and November 2025 were retrospectively screened, and 90 eligible patients were included as an external validation cohort to assess the generalizability of the prediction model. The admission diagnosis, treatment procedures, and outcome assessments were performed in accordance with the Chinese Expert Consensus on Mechanical Thrombectomy for Acute Ischemic Stroke (2023 edition). Inclusion criteria were as follows: (a) age 18–85 years; (b) time from symptom onset to hospital admission ≤24 h and eligibility for MT; (c) imaging-confirmed LVO in the anterior or posterior circulation by computed tomography angiography (CTA), magnetic resonance angiography (MRA), or digital subtraction angiography (DSA) involving the internal carotid artery, middle cerebral artery (M1/M2 segments), vertebral artery, or basilar artery; (d) preoperative mRS score ≤1; and (e) complete clinical and imaging data with 90-day follow-up available. Exclusion criteria were as follows: (a) preoperative imaging findings suggestive of intracranial hemorrhage or large territorial cerebral infarction accompanied by marked cerebral edema; (b) severe cardiac, hepatic, or renal dysfunction or the presence of malignant tumors; (c) severe infection, coagulation disorders, or a history of major surgery shortly before the procedure; and (d) failure to undergo MT at participating centers or absence of postoperative follow-up data. This multicenter retrospective study was approved by the Ethics Committee of Ji’an Central People’s Hospital, Ji’an, Jiangxi, China (Approval Number: 2025-L00003; Date of Approval: 20 January 2025). Ethical approval was also obtained from the corresponding ethics committees of the participating external centers, including The Affiliated Hospital of Xuzhou Medical University, Xuzhou, Jiangsu, China (Approval Number: XYFY2024-KL237-01; Date of Approval: 17 May 2024) and The Affiliated Changshu Hospital of Soochow University, Changshu, Jiangsu, China (Approval Number: 2025-L-061; Date of Approval: 3 December 2025). All patient details were deidentified prior to analysis to ensure that no individual patient could be identified. All procedures were conducted in accordance with the ethical principles of the Declaration of Helsinki, as revised in 2024. Because of the retrospective nature of this study, the requirement for written informed consent was waived by the ethics committees of the participating centers.
Clinical data collection
Clinical data were collected in the following categories: (a) Demographic characteristics. age, sex, body mass index (BMI), smoking history, alcohol consumption, and medical comorbidities, including hypertension, diabetes mellitus, coronary artery disease, atrial fibrillation, and hyperlipidemia; (b) Clinical parameters. NIHSS score on admission, blood pressure, blood glucose levels, blood lipid levels, hemoglobin levels, platelet count, and C-reactive protein (CRP) levels; and (c) Imaging and procedural characteristics. infarct location and extent, ASPECTS, collateral circulation status assessed using the American Society of Interventional and Therapeutic Neuroradiology/Society of Interventional Radiology (ASITN/SIR) grading system, occluded vessel location, OTR, number of thrombectomy passes, degree of recanalization evaluated using the modified Thrombolysis in Cerebral Infarction (mTICI) scale, and reperfusion injury. Postoperative symptomatic intracranial hemorrhage (sICH) was also recorded; however, it was not included in the primary model and was evaluated only in sensitivity analyses.
Functional outcomes were assessed at 90 days after the procedure through outpatient visit or telephone follow-up using mRS. Patients were categorized into the non-FR group (mRS ≤ 2) and the FR group (mRS > 2).
Data partitioning
The development cohort consisted of 260 patients with AIS who underwent MT at Ji’an Central People’s Hospital and The Affiliated Hospital of Xuzhou Medical University. Using random sampling, this cohort was divided into a training cohort (n = 182) and a test cohort (n = 78) in a 7:3 ratio for model development and internal validation.
The external validation cohort comprised 90 patients with AIS who underwent MT at The Affiliated Changshu Hospital of Soochow University and was used independently to assess the generalizability and robustness of the model across different clinical centers.
The patient enrollment and data partitioning process is shown in Figure 1.

Flowchart of patient selection.
Statistical analysis
Continuous variables were summarized as median (interquartile range (IQR)), and categorical variables were presented as counts and percentages (n (%)). Between-group comparisons of continuous variables were performed using the Mann–Whitney U test, whereas categorical variables were compared using the chi-square test or Fisher’s exact test, as appropriate.
To improve the robustness of predictor selection, least absolute shrinkage and selection operator (LASSO) regression was first used to screen candidate variables. Variables selected by LASSO were then entered into multivariable logistic regression to identify independent predictors of FR. In the multivariable model, OTR was analyzed per 30-min increase. A nomogram prediction model was subsequently constructed based on the final regression results. Model discrimination was evaluated using the area under the receiver operating characteristic (ROC) curve (AUC) with 95% confidence intervals (CIs). Calibration was assessed using calibration curves, calibration slope, calibration intercept, and Brier score. Decision curve analysis (DCA) was performed to evaluate the clinical net benefit of the model. Model performance was assessed in the training cohort, test cohort, and external validation cohort. In addition, a sensitivity analysis was performed by reintroducing sICH into the model to assess the robustness of the primary findings. All statistical analyses were performed using R software (version 4.3.2), and a two-sided p value <0.05 was considered statistically significant.
Results
Baseline characteristics of patients in the non-FR and FR groups
A total of 350 patients with AIS who underwent MT were included in this study, comprising 170 patients from Ji’an Central People’s Hospital, 90 from The Affiliated Hospital of Xuzhou Medical University, and 90 from The Affiliated Changshu Hospital of Soochow University. Based on 90-day functional outcomes, 152 patients (43.43%) were classified into the non-FR group and 198 (56.57%) into the FR group. The baseline characteristics of patients in the two groups are summarized in Table 1, whereas baseline characteristics across the three participating centers are presented in Supplementary Table 1.
Baseline characteristics of patients in the non-FR and FR groups.

ASPECTS: Alberta Stroke Program Early CT Score; BMI: body mass index; FR: futile recanalization; Glu: glucose; L: lymphocyte count; mTICI: modified Thrombolysis in Cerebral Infarction; N: neutrophil count; NIHSS: National Institutes of Health Stroke Scale; NLR: neutrophil-to-lymphocyte ratio; OTR: onset-to-recanalization time; sICH: symptomatic intracranial hemorrhage; CRP: C-reactive protein; SBP: systolic blood pressure; DBP: diastolic blood pressure; RBC: red blood cells; INR: International normalized ratio; APTT: activated partial thromboplastin time; TC: total cholesterol; LDL: low density lipoprotein; HDL: high density lipoprotein; HbA1c: glycated hemoglobin; TOAST: Trial of Org 10172 in Acute Stroke Treatment; PLT: platelet count; PT: prothrombin time; TT: thrombin time; FIB: fibrinogen; TG: triglycerides.
As shown in Table 1, significant differences were observed between the non-FR and FR groups in baseline NIHSS score, ASPECTS, collateral status, OTR, admission glucose level, CRP levels, neutrophil count, neutrophil-to-lymphocyte ratio (NLR), and total cholesterol (TC). Patients in the FR group had higher NIHSS scores, glucose levels, CRP levels, neutrophil count, and NLR levels; longer OTR; lower ASPECTS and TC; and poorer collateral status. In contrast, the remaining baseline characteristics did not differ significantly between the two groups. Detailed distributions of these clinical, laboratory, imaging, and procedural variables are provided in Table 1.
Variable selection using LASSO regression
To improve the robustness of predictor selection, LASSO regression was performed. The coefficient profiles of candidate predictors are shown in Figure 2(a), and the optimal penalty parameter was determined using 10-fold cross-validation (Figure 2(b)). Both lambda.min and lambda.1se were identified, and variables selected according to the lambda.min criterion were entered into subsequent multivariable logistic regression analysis. A total of five candidate predictors were retained, including baseline NIHSS score, ASPECTS, collateral status, OTR, and admission glucose level.

LASSO regression for predictor selection. (a) LASSO coefficient profiles of candidate predictors; (b) cross-validation plot for tuning parameter selection with lambda.min and lambda.1se. LASSO: Least absolute shrinkage and selection operator.
Multivariable logistic regression analysis of predictors for FR
Variables selected by LASSO were subsequently entered into the multivariable logistic regression model. As shown in Table 2, baseline NIHSS score (odds ratio (OR) =1.09, 95% CI: 1.04–1.14, p ≤ 0.001), ASPECTS (OR = 0.8, 95% CI: 0.67–0.95, p = 0.012), collateral status (OR = 3.56, 95% CI: 1.62–7.79, p = 0.002), OTR per 30-min increase (OR = 1.12, 95% CI: 1.01–1.25, p = 0.037), and admission blood glucose levels (OR = 1.23, 95% CI: 1.1–1.38, p ≤ 0.001) were independently associated with FR. Because sICH was excluded from the primary model, it was not included in the final multivariable analysis.
Multivariable logistic regression analysis of predictors of futile recanalization.
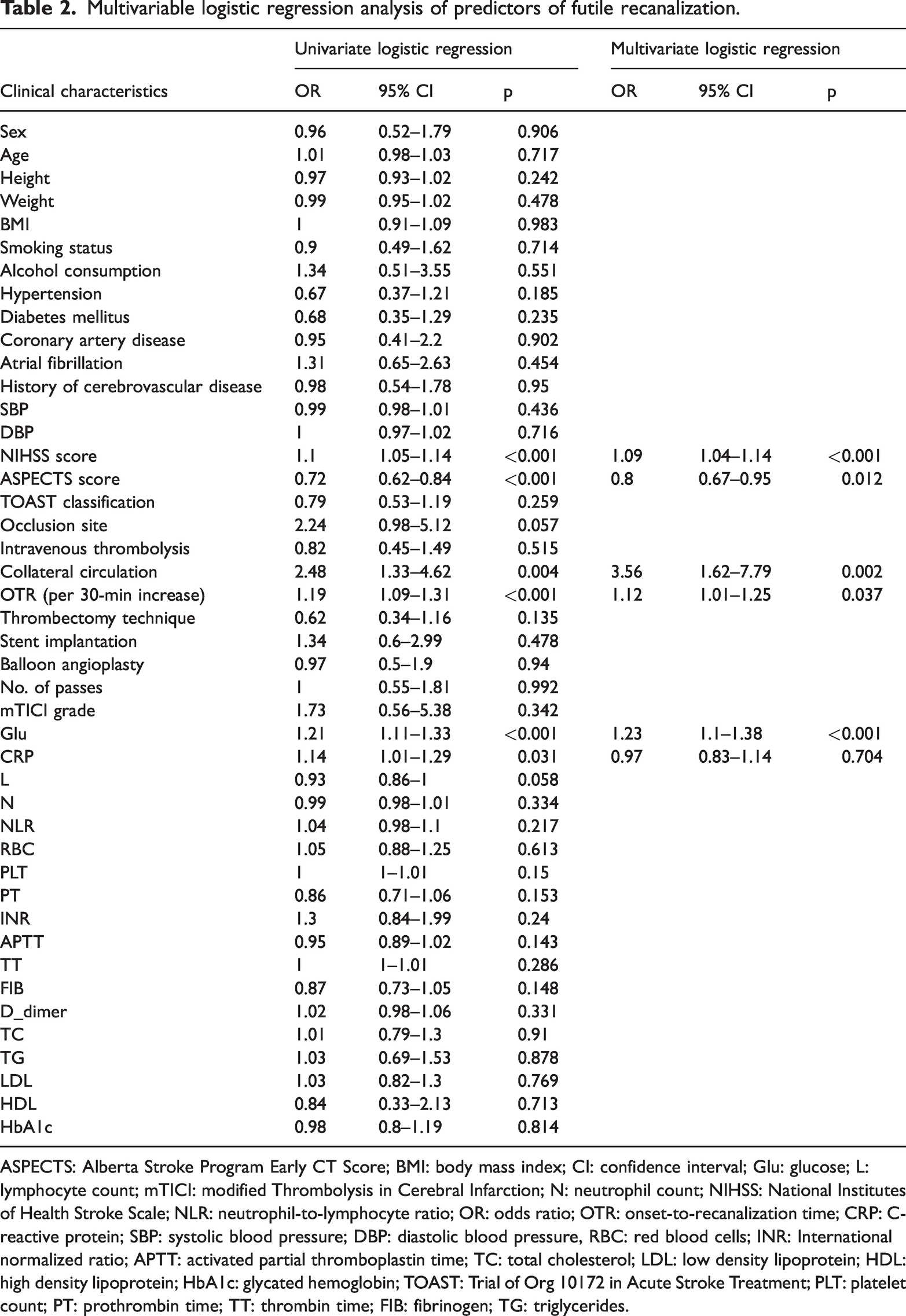
ASPECTS: Alberta Stroke Program Early CT Score; BMI: body mass index; CI: confidence interval; Glu: glucose; L: lymphocyte count; mTICI: modified Thrombolysis in Cerebral Infarction; N: neutrophil count; NIHSS: National Institutes of Health Stroke Scale; NLR: neutrophil-to-lymphocyte ratio; OR: odds ratio; OTR: onset-to-recanalization time; CRP: C-reactive protein; SBP: systolic blood pressure; DBP: diastolic blood pressure, RBC: red blood cells; INR: International normalized ratio; APTT: activated partial thromboplastin time; TC: total cholesterol; LDL: low density lipoprotein; HDL: high density lipoprotein; HbA1c: glycated hemoglobin; TOAST: Trial of Org 10172 in Acute Stroke Treatment; PLT: platelet count; PT: prothrombin time; TT: thrombin time; FIB: fibrinogen; TG: triglycerides.
Nomogram construction
Based on the final multivariable logistic regression model, a nomogram was constructed to provide individualized prediction of FR after MT (Figure 3). The nomogram incorporated NIHSS, ASPECTS, collateral status, OTR per 30-min increase, and admission blood glucose levels.

Nomogram for predicting futile recanalization after mechanical thrombectomy.
Discriminative performance of the prediction model
The discriminative ability of the model was evaluated using ROC analysis. As shown in Figure 4(a) to (c), the model achieved an AUC of 0.84 (95% CI: 0.78–0.84) in the training cohort, 0.86 (95% CI: 0.78–0.86) in the test cohort, and 0.80 (95% CI: 0.70–0.80) in the external validation cohort, indicating acceptable to good discriminative performance.
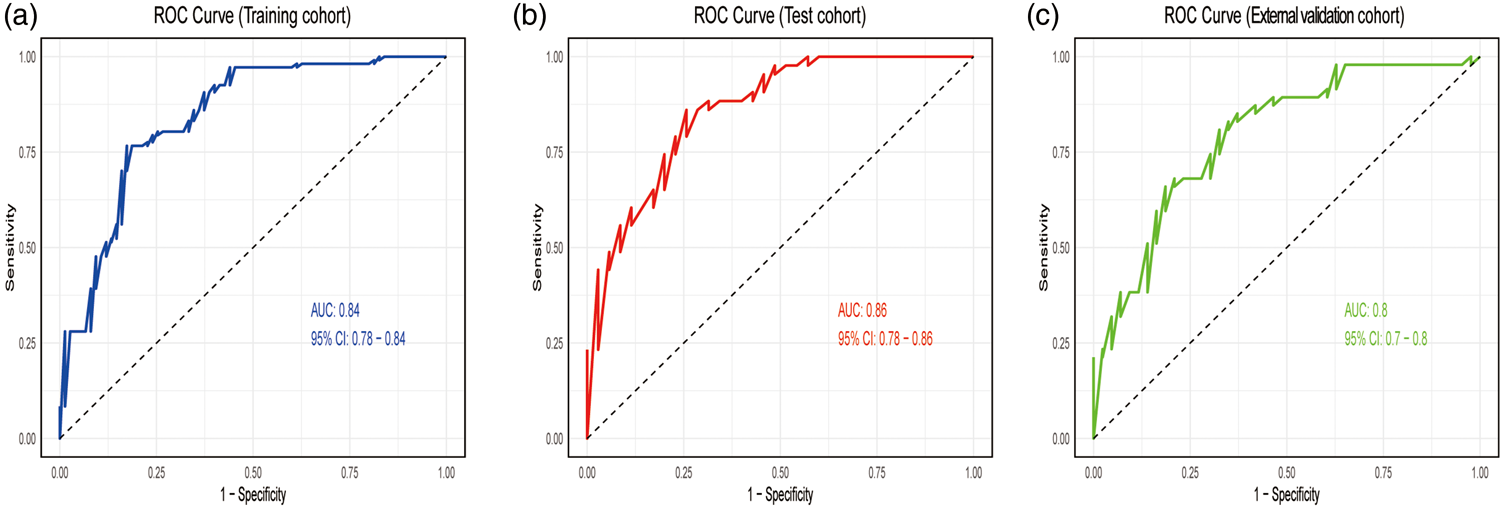
Receiver operating characteristic curves of the model in the training (a), test (b), and external validation (c) cohorts.
Calibration performance of the prediction model
Calibration performance was assessed in the test and external validation cohorts. As shown in Figure 5(a) and (b), the calibration curves demonstrated good agreement between predicted and observed probabilities in both cohorts. In the test cohort, the calibration slope, intercept, and Brier score were 0.993, −0.129, and 0.149, respectively, whereas in the external validation cohort, the corresponding values were 1.026, −0.742, and 0.204, respectively, thereby indicating satisfactory calibration. The calibration curve for the training cohort is provided in Supplementary Figure 1.

Calibration curves of the model in the test (a) and external validation (b) cohorts.
Clinical utility of the prediction model
DCA was performed to evaluate the clinical utility of the model. As shown in Figure 6(a) and (b), the model provided greater net benefit than the treat-all and treat-none strategies across a range of threshold probabilities in the test and external validation cohorts, respectively, suggesting potential clinical usefulness. The DCA results for the training cohort are shown in Supplementary Figure 2.

Decision curve analysis of the model in the test (a) and external validation (b) cohorts.
Sensitivity analysis
To evaluate the robustness of the primary findings, a sensitivity analysis was performed by reintroducing sICH into the model. As shown in Supplementary Table 2, the direction and magnitude of the main associations remained broadly consistent with those of the primary analysis. Model performance, assessed using AUC and Brier score across the training, test, and external validation cohorts, was also generally similar, supporting the robustness of the final model.
Discussion
Based on a multicenter retrospective cohort, this study systematically analyzed factors associated with FR after MT in patients with AIS and developed a clinical prediction model with good interpretability and potential clinical utility. Our findings demonstrated that FR remains relatively common among patients undergoing MT, highlighting that angiographic success alone does not necessarily translate into meaningful functional recovery. In the primary model, higher baseline NIHSS score, lower ASPECTS, elevated admission blood glucose levels, poor collateral circulation, and prolonged OTR were identified as independent predictors of FR. Notably, postoperative sICH was excluded from the primary model because it is considered a downstream postprocedural event rather than a routine predictor available for preoperative or perioperative risk stratification. However, sensitivity analysis including sICH yielded broadly consistent results. The final model demonstrated acceptable discrimination in the training, test, and external validation cohorts and satisfactory calibration, as assessed by calibration curves, slope, intercept, and Brier score. In addition, DCA indicated potential net clinical benefit across a range of threshold probabilities. Collectively, these findings provide a multidimensional framework for understanding determinants of functional outcome after MT and support a quantitative tool for risk assessment in patients undergoing MT.
From a pathophysiological perspective, the observed associations among higher baseline NIHSS scores, lower ASPECTS, and FR highlight the central role of baseline neurological deficit severity and ischemic core extent in post-thrombectomy functional outcomes. A higher NIHSS score generally reflects more severe neurological impairment and more extensive brain tissue involvement, whereas a lower ASPECTS indicates a larger ischemic core and reduced salvageable penumbral tissue. Under such conditions, even successful large vessel recanalization may fail to yield favorable functional recovery. These findings are consistent with prior studies reporting close associations between these parameters and poor neurological outcomes, and our multicenter analysis further supports their robustness and clinical relevance across different populations.14,15 In addition, OTR, modeled in the present study per 30-min increase, further reduces the potential benefits of reperfusion therapy when prolonged by accelerating the transition of ischemic penumbra to irreversible infarction, consistent with the well-established concept that “time is brain.” 16 Poor collateral circulation also emerged as a significant independent predictor of FR, suggesting that even after successful reopening of the occluded large vessel, impaired microcirculatory perfusion may limit effective tissue-level reperfusion. 17 Together, these findings indicate that FR is not driven by a single factor but rather results from the combined effects of baseline ischemic severity, reperfusion timeliness, and microvascular status, supporting the concept that angiographic recanalization does not necessarily equate to effective tissue reperfusion or functional recovery. 18
Beyond ischemic burden and reperfusion efficiency, metabolic status also plays an important role in the development of FR. In this study, elevated admission blood glucose levels were identified as an independent risk factor, consistent with evidence linking stress-induced hyperglycemia to unfavorable stroke outcomes. Hyperglycemia may exacerbate ischemia–reperfusion injury through multiple mechanisms, including enhanced oxidative stress, activation of inflammatory cascades, and disruption of blood–brain barrier integrity, thereby reducing cerebral tissue tolerance to reperfusion and impairing functional recovery despite successful vessel recanalization.19–22 Recent studies suggest that composite glycometabolic indicators, such as the glucose-to-glycated hemoglobin ratio, may provide additional prognostic information in patients with AIS undergoing reperfusion therapy.23–26 However, in this multicenter retrospective study, we prioritized routinely available and readily interpretable variables across centers. Therefore, admission glucose levels were retained as a pragmatic predictor in the final model, which is also consistent with recent registry-based evidence, suggesting that admission glucose levels may be a practical glucose measure for outcome prediction after endovascular therapy. 27 In contrast, although sICH was associated with worse outcomes in sensitivity analysis, it was intentionally excluded from the primary model because it represents a postprocedural event and may not be well-suited for preoperative or perioperative risk assessment. This distinction enhances the temporal interpretability and clinical applicability of the final model.
On the basis of identified risk factors, we further developed a nomogram prediction model integrating readily available clinical and imaging variables to facilitate individualized risk assessment of FR after MT. Compared with reliance on single indicators or subjective clinical judgment, the model offers improved interpretability and operational feasibility by integrating multiple key predictors into a user-friendly quantitative tool. Importantly, the added value of this study lies not only in model development but also in its multicenter design, independent external validation, and a more comprehensive performance evaluation, which includes discrimination, calibration, and DCA. The model may be applied in the preoperative or perioperative period to enable rapid risk stratification. Early identification of high-risk patients may support more cautious and individualized management strategies, such as stricter glucose and blood pressure control, optimization of reperfusion timing, and closer monitoring for adverse postprocedural complications, potentially reducing the risk of FR. Notably, the model maintained stable predictive performance in an independent external validation cohort, suggesting acceptable generalizability and potential value for broader clinical application. Overall, this model shifts the evaluation of MT success from a purely technical focus on recanalization toward a patient-centered assessment emphasizing functional outcome, thereby supporting more precise clinical decision making in acute stroke care.
Several limitations in this study should be acknowledged. First, the retrospective design introduces inherent risks of selection bias and information bias, and the findings require confirmation in prospective studies. Second, although multicenter data and external validation were included, the overall sample size remains relatively modest, particularly in the external validation cohort, and intercenter differences in patient characteristics and perioperative management strategies may have influenced model stability. Third, several variables that showed between-group differences or have been reported in previous studies, such as age, inflammatory markers, and lipid-related indicators, were not retained in the final model.10,28–31 This likely reflects limited incremental predictive value after adjustment for stronger predictors, potential collinearity, and sample size constraints rather than lack of clinical relevance. Fourth, certain potentially important prognostic factors, including perioperative hemodynamic parameters, quantitative imaging biomarkers, and advanced glycometabolic indicators (e.g. glucose-to-glycated hemoglobin ratio), were not included, limiting a more comprehensive mechanistic characterization of FR.25,32 Finally, it should be emphasized that the proposed model is intended for risk stratification in patients with AIS after MT and should not replace clinical judgment or be used as the sole determinant of treatment decisions. Future studies with larger sample sizes, broader geographic representation, and prospective designs are warranted, and incorporation of advanced imaging and dynamic clinical variables may further refine and enhance the model’s clinical utility.
Conclusions
Higher baseline NIHSS score, lower ASPECTS, poor collateral circulation, elevated admission blood glucose levels, and prolonged OTR were identified as independent predictors of FR after MT. The prediction model developed from these variables demonstrated acceptable discriminative ability, satisfactory calibration, and potential clinical utility across the training, test, and external validation cohorts. This model may support risk stratification and individualized perioperative management in patients with AIS undergoing MT.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261454832 - Supplemental material for Risk factors and predictive model for futile recanalization after mechanical thrombectomy in patients with acute ischemic stroke: A multicenter retrospective study
Supplemental material, sj-pdf-1-imr-10.1177_03000605261454832 for Risk factors and predictive model for futile recanalization after mechanical thrombectomy in patients with acute ischemic stroke: A multicenter retrospective study by Shuhong Mei, Fanghua Zhou, Xinhua Zhan, Bin Wu, Yiqin Zhang, Jianping Yang, Bin Li, Min Xu, Qian Wu, Fengda Li and Longyuan Gu in Journal of International Medical Research
Footnotes
Acknowledgments
The authors thank all participants and clinical staff involved in this study.
Author contributions
Shuhong Mei and Fanghua Zhou contributed to study design, data collection, statistical analysis, and manuscript drafting. Xinhua Zhan, Bin Wu, Yiqin Zhang, Jianping Yang, and Bin Li participated in patient screening, data collection, and data verification. Min Xu, Qian Wu, and Fengda Li contributed to data interpretation and critically revised the manuscript for important intellectual content. Longyuan Gu conceived and supervised the study, reviewed the results, and revised the manuscript. All authors read and approved the final manuscript and agree to be accountable for all aspects of the work.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request. Because the dataset contains patient-related clinical information, data sharing is subject to deidentification requirements, institutional regulations, and ethics approval where necessary.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Science and Technology Bureau of Ji’an City (No. 20244-049542) and the Science and Technology Program of the Jiangxi Provincial Health Commission (No. 202611641).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.