
Abstract
Sacral epidural cavernous hemangioma involving the intervertebral foramen is exceptionally rare and may closely mimic more common benign nerve sheath tumors on magnetic resonance imaging. We report the case of a woman in her mid-50s who presented with a 1-month history of nocturnal left lower-extremity pain and mild weakness. Contrast-enhanced lumbar magnetic resonance imaging revealed a strongly enhancing nodular lesion in the left S2 foraminal region, and schwannoma was considered preoperatively. The patient underwent microsurgical resection through a posterior midline approach. Intraoperatively, the lesion was dark red, soft, and hypervascular, raising suspicion for a vascular malformation rather than schwannoma. Frozen-section analysis suggested hemangioma, and postoperative histopathology confirmed cavernous hemangioma. The patient experienced marked postoperative relief of radicular pain, and follow-up analysis indicated complete symptom resolution without radiological evidence of residual lesion. This case emphasizes that cavernous hemangioma should be included in the differential diagnosis of sacral foraminal masses. Purely epidural cavernous hemangiomas centered in the sacral foramen are particularly rare and frequently misdiagnosed preoperatively as schwannoma; thus, careful preoperative planning, anticipation of intraoperative hypervascularity, and frozen-section histology may help guide safe resection.
Introduction
Purely epidural cavernous hemangiomas centered in the sacral foramen are particularly rare and frequently misdiagnosed preoperatively as schwannoma; this case highlights the value of anticipating intraoperative hypervascularity and using frozen-section histology to guide resection. Cavernous hemangioma, currently classified by the International Society for the Study of Vascular Anomalies within the spectrum of venous malformations, 1 is a benign vascular lesion composed of dilated, thin-walled vascular channels lined by endothelium. 2 However, the term “cavernous hemangioma” remains widely used in radiology, pathology, and neurosurgery. Spinal epidural cavernous hemangiomas are rare, particularly sacral lesions.1,3 Because their symptoms and magnetic resonance imaging features are often nonspecific, they are frequently misdiagnosed before surgery, especially when they extend into the neural foramen and simulate schwannoma or other dumbbell-shaped tumors. 4
We describe a rare cavernous hemangioma centered in the left S2 sacral foramen. The case is notable because the lesion presented as a foraminal mass with radicular symptoms, was initially diagnosed as schwannoma, and required intraoperative reassessment due to unexpected hypervascularity. In addition to documenting the clinical course, this report emphasizes practical lessons regarding imaging interpretation, differential diagnosis, surgical planning, histopathological confirmation, and postoperative assessment for neurosurgeons managing sacral foraminal tumors.
Case presentation
The reporting of this study conforms to the Case Report (CARE) guidelines. 5 We have de-identified all details to protect patient anonymity. A woman in her mid-50s was admitted to the Department of Neurosurgery, The First Affiliated Hospital of Wannan Medical College, Yijishan Hospital of Wannan Medical College, Wuhu, Anhui, China, in July 2025, with a 1-month history of left lower-extremity pain that was more severe at night. Neurological examination revealed preserved lumbar motion, no spinal tenderness, left lower-extremity strength of 4/5, and right lower-extremity strength of 5/5. Muscle tone was normal. Bilateral patellar reflexes were symmetric, whereas both Achilles tendon reflexes were decreased.
Contrast-enhanced lumbar magnetic resonance imaging revealed mild straightening of the physiological lumbar curvature and a nodular lesion in the left S2 foraminal region with obvious heterogeneous enhancement (Figure 1(A) to (C)). Based on the lesion location and imaging appearance, a sacral schwannoma was considered the leading preoperative diagnosis.
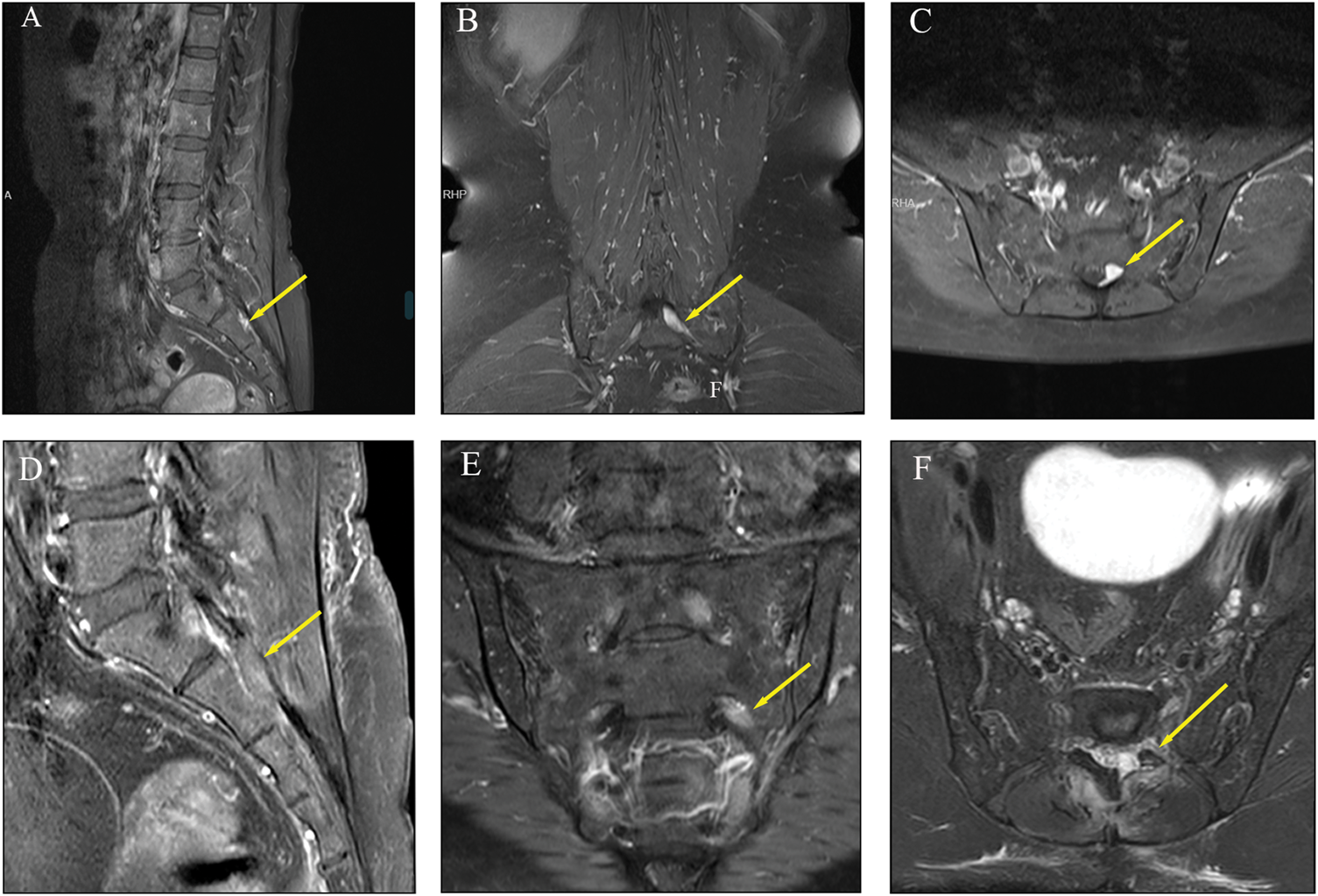
Preoperative contrast-enhanced magnetic resonance imaging showing the lesion in the left S2 foraminal region on (A) sagittal, (B) coronal, and (C) axial images. Postoperative magnetic resonance imaging on (D) sagittal, (E) coronal, and (F) axial views shows no definite residual lesion after resection.
The patient underwent microsurgical resection of the intra- and extraspinal S2 lesion with neural decompression via a posterior midline approach under general anesthesia. Intraoperative fluoroscopy was used to localize the S2 level. After exposure of the left S2 lamina, a high-speed drill was used to open the lamina. The lesion appeared dark red, soft, and distinctly hypervascular and compressed the adjacent sacral nerve root. Because the operative findings were inconsistent with a typical schwannoma, frozen-section examination was requested intraoperatively, which suggested hemangioma (Figure 2(A) and (B)). Tumor resection was then performed carefully and progressively to avoid abrupt decompression and possible traction or ischemia–reperfusion injury to the sacral nerve root. The resected specimen measured approximately 1.5 × 1.0 × 1.0 cm. Adequate hemostasis was achieved after removal of the lesion. Written informed consent for surgical treatment was obtained from the patient before the procedure.
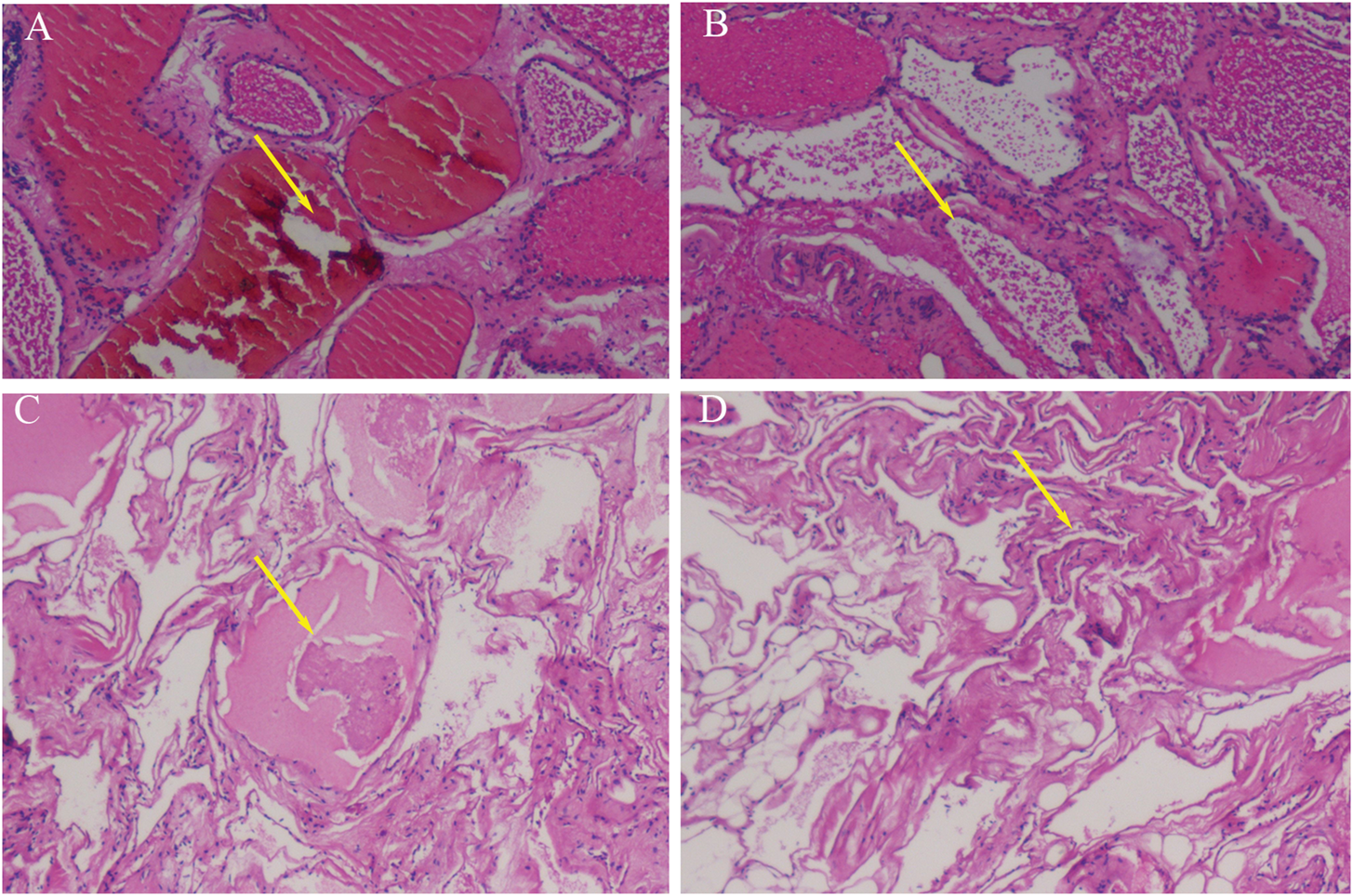
(A and B) Intraoperative frozen sections and (C and D) postoperative hematoxylin-eosin staining showing characteristic pathological features of cavernous hemangioma. Arrows indicate dilated blood-filled vascular spaces lined by flattened endothelial cells (original magnification 200×).
Definitive histopathological examination confirmed cavernous hemangioma, showing dilated vascular spaces lined by flattened endothelial cells (Figure 2(C) and (D)). Postoperatively, the patient’s left lower-extremity pain and fatigue improved substantially. Motor function and muscle tone were normal, bilateral straight-leg-raising tests were negative, and no pathological reflexes were elicited. Follow-up magnetic resonance imaging showed no residual lesion Figure 1(D) to (F)), and telephone follow-up at 3–6 months confirmed complete symptom resolution. Written informed consent for publication of the clinical details and imaging findings was also obtained from the patient.
Discussion
Spinal epidural cavernous hemangiomas account for only a small fraction of spinal vascular lesions, and localization to the sacral region is particularly unusual. 1 Lesions centered in the neural foramen are even more diagnostically challenging because they can resemble schwannoma, neurofibroma, meningioma, metastasis, lymphoma, or other epidural masses. 6 In this patient, the foraminal location and enhancing appearance strongly suggested schwannoma before surgery. This pattern of misclassification is consistent with prior reports showing that purely epidural cavernous hemangiomas are often not definitively identified until pathological examination.4,7 To the best of our knowledge, this is the first reported case of sacral foraminal cavernous hemangioma confirmed by intraoperative frozen section; previous reports have described only isolated epidural cases, with none specifically centered at the S2 foramen.
The clinical presentation of spinal epidural cavernous hemangioma depends mainly on the lesion size, site, and degree of neural compression. 4 Radicular pain, sensory disturbance, weakness, and gait dysfunction are common. 8 Some patients show slowly progressive symptoms, whereas others develop intermittent or acute neurological deterioration related to thrombosis or intralesional hemorrhage.4,7,9 Our patient presented mainly with radicular pain and mild unilateral weakness, which are not specific and therefore do not help reliably distinguish this entity from a nerve sheath tumor. The relatively short symptomatic history in the present case may reflect the confined foraminal space, where even a modest increase in lesion volume can produce clinically significant compression of the exiting sacral nerve root.
Anatomically, the sacral foraminal region deserves special attention when discussing these lesions. A mass at the S2 foramen may affect not only the adjacent sensory fibers responsible for radicular pain but also motor and autonomic pathways, depending on the degree and direction of compression. Although our patient did not present with bowel or bladder dysfunction, the proximity of the lesion to functionally important sacral roots increased the operative stakes. This anatomical context helps explain why apparently small lesions in the sacrum can cause disproportionate symptoms and why surgical decompression should be undertaken with careful respect for neural tissue.
Although magnetic resonance imaging is the most useful preoperative tool, misdiagnosis is common. 4 Typical lesions are iso- to hypointense on T1-weighted imaging, hyperintense on T2-weighted imaging, and strongly enhanced after gadolinium administration.4,10 However, these features overlap with those of schwannoma. 6 In practice, several clues may suggest a vascular lesion: relatively intense and sometimes homogeneous enhancement, a lobulated epidural mass, evidence of adjacent venous channels, and intraoperative hypervascularity that is out of proportion to the expected appearance of a schwannoma. In our case, the diagnosis became more plausible only after direct inspection of the lesion and frozen-section analysis. In addition, the differential diagnosis should extend beyond benign nerve sheath tumors to include malignant lesions such as metastatic disease, lymphoma, and malignant peripheral nerve sheath tumor, particularly when enhancement is heterogeneous, bony erosion is present, or the lesion demonstrates aggressive extension beyond the neural foramen. Although imaging overlap is substantial, the combination of lesion morphology, pattern of enhancement, osseous involvement, and intraoperative vascular appearance may help raise suspicion for a vascular malformation rather than a malignant neoplasm. Similar diagnostic challenges have been described in other uncommon cavernous hemangiomas, in which accurate diagnosis often depends on integrating radiologic assessment with intraoperative findings and histopathological confirmation. 11
Complete microsurgical resection is the treatment of choice for symptomatic lesions.7,9 The most important operative issues are accurate localization, early recognition of the vascular nature of the lesion, gentle manipulation of sacral nerve roots, and meticulous hemostasis. Unlike schwannoma, cavernous hemangioma may bleed readily, and unprepared resection can obscure the operative field. In the sacral foramen, excessive traction or rapid decompression may also endanger the nerve root because of the limited corridor and intimate tumor–nerve relationship. The favorable postoperative course in our patient underscores the value of cautious stepwise decompression. Recurrence after gross-total resection of spinal epidural cavernous hemangioma appears to be uncommon, although the true rate is difficult to define because most published evidence consists of isolated case reports and small series with limited follow-up. This underscores the importance of postoperative imaging surveillance, particularly in unusual sacral lesions where the operative corridor is narrow and complete assessment of residual disease may be challenging.
The technical principles of surgery for sacral epidural cavernous hemangioma differ subtly but importantly from those used for many other benign foraminal lesions. Accurate level localization is essential because the sacral lamina and foramina provide limited visual landmarks, and unnecessary bone removal may destabilize local anatomy or enlarge the operative corridor more than necessary. After exposure, the surgeon should identify the relationship between the mass and the sacral root before aggressive manipulation. Because these lesions may bleed readily, maintaining a clean field through bipolar coagulation, careful piecemeal resection, and patient hemostatic preparation is critical. In addition, rapid decompression should be avoided when the root is chronically compressed, because abrupt change in local tension may increase the risk of postoperative neural irritation. The favorable postoperative course in our patient suggests that cautious microsurgical handling can achieve both gross-total removal and neurological preservation.
Histopathological confirmation remains the diagnostic gold standard. In the present case, definitive examination showed dilated vascular spaces lined by flattened endothelial cells, consistent with cavernous hemangioma. This finding is important because the distinction from schwannoma is not merely semantic; it explains the lesion’s operative appearance, vascular behavior, and potential pitfalls in preoperative imaging interpretation. The pathology also reinforces the point that rare sacral masses should be approached with a broad differential diagnosis, especially when radiology and intraoperative findings are not fully concordant.
Outcome after resection of symptomatic spinal epidural cavernous hemangioma is generally favorable when decompression is timely and complete.9,10 Our patient experienced marked relief of radicular pain, recovery of strength, and no residual lesion on postoperative imaging. Although the follow-up duration in this report was limited, the early result supports existing evidence that surgery can be both diagnostic and therapeutic. In rare sacral lesions, successful treatment also provides reassurance that the functional risks associated with operating near the sacral roots can be minimized when microsurgical principles are followed.
This case also offers a broader lesson for interdisciplinary management. Radiologists should be aware that strongly enhancing sacral foraminal lesions are not always schwannomas, especially if the lesion appears unusually lobulated or vascular. Pathologists should consider vascular malformation when frozen sections show blood-filled spaces lined by inconspicuous endothelial cells rather than spindle-cell proliferation. Surgeons should anticipate the possibility of brisk bleeding and prepare accordingly. In selected anatomically complex or diagnostically uncertain cases, multidisciplinary discussion may also help guide the need for additional imaging, operative planning, and postoperative surveillance. Thus, even a single case can carry educational value when it illustrates an uncommon but reproducible diagnostic pitfall.
The main strengths of this report are the unusual location and the clear intraoperative discrepancy between the expected diagnosis and the actual vascular lesion. Its limitations are the single-case design and the relatively short follow-up interval. Nevertheless, the case carries practical value because it broadens the differential diagnosis of sacral foraminal tumors and may help reduce preoperative misclassification.
Conclusion
Cavernous hemangioma should be included in the differential diagnosis of enhancing sacral foraminal masses. Recognition of this entity preoperatively, combined with careful microsurgical technique, enables safe resection and excellent neurological recovery. Although rare, this lesion deserves awareness among neurosurgeons, radiologists, and pathologists because earlier diagnostic suspicion may improve operative preparation and reduce the likelihood of intraoperative surprise.
Footnotes
Acknowledgements
The authors used an AI-assisted language tool only for language improvement during manuscript preparation. The authors take full responsibility for the content of the manuscript.
Author contributions
Zixiao Li and Changli Han drafted the manuscript. Zhang Xiong, Zhichun Wang, Mingze Tan, Jiajia Yu, Mengwei Ma, Weicheng Wang, and Yuqing Wang collected the clinical data and assisted with image and pathological interpretation. Guangfu Di and Xiaochun Jiang supervised the study, critically revised the manuscript, and approved the final version. All authors read and approved the final manuscript.
Data availability
No datasets were generated or analyzed during the current study.
Declaration of conflicting interests
The authors declare that there are no competing interests.
Ethics approval and consent
According to institutional practice, ethics committee approval was not required for this single anonymized case report. Written informed consent for surgical treatment was obtained from the patient, and separate written informed consent for publication of the clinical details and images was also obtained. All patient details have been de-identified to protect anonymity.
Funding
Anhui Provincial University Research Program (2024AH040241); Anhui Provincial Health Research Program (2024Ab0097); Anhui Provincial University Research Program (2024AH040236); Anhui Provincial University Research Program (2024AH051901).