
Abstract
Multisystem Inflammatory Syndrome in Children is a serious complication associated with coronavirus disease 2019 that commonly affects individuals under 19 years of age. This condition can present with a wide spectrum of clinical manifestations, some of which may be severe or life-threatening. Management can be challenging due to the variability in clinical presentation and response to therapy. This report describes the case of a toddler with no previously documented severe acute respiratory syndrome coronavirus 2 infection who presented with a 30-day relapsing fever that demonstrated partial response to antipyretics and was associated with gastrointestinal symptoms and a skin rash. Following extensive clinical and laboratory investigations, the patient was diagnosed with multisystem inflammatory syndrome in children and was successfully treated with intravenous immunoglobulin and corticosteroids.
Keywords
Introduction
Multisystem inflammatory syndrome in children (MIS-C) is a rare but serious complication that can develop 4–6 weeks after an initial infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). 1 Some data suggest that MIS-C is less common and less severe with the Omicron variant as compared with earlier variants. 2 In very young children, MIS-C can resemble other conditions such as Kawasaki disease (KD), toxic shock syndrome, or sepsis, making diagnosis challenging, especially when laboratory or coronavirus disease 2019 (COVID-19) testing are unavailable. Early recognition and prompt treatment with immune-modulating therapies are crucial to prevent serious complications. A major diagnostic challenge in MIS-C is distinguishing it from KD because of overlapping clinical features. Delays in diagnosis or treatment may result in severe cardiac or systemic complications. Herein, we present a rare case of MIS-C in a 1.7-year-old female from Hama, Syria, who presented with a 30-day history of recurrent fever and was partially responsive to antipyretics. This report discusses the diagnostic challenges, management strategies, and follow-up recommendations for this case.
Case presentation
A female toddler in her second year of life from Syria was admitted to Hama Maternity and Children’s Hospital, Syria, in August 2024 with a 30-day history of persistent recurrent fever and was partially responsive to antipyretics. Her parents reported that she had unusual fatigue, anorexia, repeated vomiting, and episodes of diarrhea. There was no cough, shortness of breath, or signs of meningitis. She had been healthy prior to this illness, with no significant medical or family history. All patient data have been anonymized to ensure privacy. On examination, the patient was hemodynamically stable but appeared pale and weak, with a body temperature of 39°C. Physical examination revealed a congested pharynx, a maculopapular rash over the trunk that persisted for 4 days, mild swelling of the hands and feet, and palpable splenomegaly (approximately 1 cm). There was no lymphadenopathy, respiratory distress, or neurological involvement. Laboratory investigations revealed anemia, with a hemoglobin level of 7.3 g/dL (normal range, 10.5–13.5 g/dL) and a mean corpuscular volume (MCV) of 76.6 fL (normal range, 80–100 fL) as well as mild thrombocytopenia, with a platelet count of 117 × 10³/µL (normal range, 150 × 10³/µL to 450 × 10³/µL). The white blood cell count was 5.2 × 10³/µL (normal range, 4 × 10³/µL to 11 × 10³/µL) with lymphocytosis. C-reactive protein (CRP) level was 18 mg/L (normal, <10 mg/L) on admission but later returned to normal levels. One week later, the hemoglobin was 6.9 g/dL. Lactate dehydrogenase (LDH) was markedly elevated at 1200 U/L (normal range, 150–500 U/L), and D-dimer was markedly elevated at 3440 ng/mL (normal, <250 ng/mL DDU). The coagulation profile demonstrated prolonged partial thromboplastin time (PTT). Procalcitonin was 1.8 ng/mL (normal, <0.05 ng/mL). COVID-19 immunoglobulin M was positive (1.1), whereas blood cultures and tests for Wright and Widal were negative. Echocardiography demonstrated normal cardiac function without coronary abnormalities. Abdominal ultrasonography showed no abnormalities. Cerebrospinal fluid (CSF) analysis was normal, and bone marrow aspiration revealed hypercellularity, consistent with a systemic inflammatory response, with no evidence of malignancy or hemophagocytosis. Based on these findings, the child was diagnosed with MIS-C related to COVID-19. Treatment included intravenous immunoglobulin (IVIG; 2 g/kg), methylprednisolone (30 mg/kg/day for 3 days), and low-dose aspirin (5 mg/kg/day). The fever subsided within 2 days, and the patient’s condition improved rapidly. Laboratory values, including D-dimer, gradually returned to normal (256 ng/mL after 15 days). Aspirin was subsequently discontinued. At follow-up, the child remained healthy and symptom-free, with normal cardiac and laboratory evaluations. Written informed consent was obtained from the patient’s legal guardians for both clinical treatment and publication of this case report.
This study’s reporting conforms to the Case Report (CARE) guidelines. 3
Discussion
MIS-C, a complication of COVID-19, is rarely reported in Syria, with very few cases published in PubMed-indexed literature. To the best of our knowledge, this is the first reported case from our city.
Severe acute respiratory syndrome coronavirus 2 is a viral infection that primarily affects the respiratory tract. According to the World Health Organization, MIS-C affects individuals aged 0–19 years. 4
In most cases, COVID-19 in children is asymptomatic or mild; however, in rare cases, it may progress to severe disease. 5 MIS-C is considered an uncommon complication of COVID-19, although its pathogenesis is not fully understood. Some studies suggest that it may represent a delayed response to COVID-19. 6
Clinically, MIS-C presents with a wide range of symptoms, including persistent fever, rash, gastrointestinal symptoms (e.g. abdominal pain, vomiting, and diarrhea), conjunctivitis, mucous membrane involvement, neurocognitive symptoms, respiratory symptoms, sore throat, myalgia, swelling of the hands and feet, and lymphadenopathy. Herein, we report a case of a 1.7-year-old female with a 30-day history of recurrent fever, consistent with MIS-C, along with other typical clinical features (Table 1).
MIS-A/MIS-C case definition and diagnostic criteria according to the Centers for Disease Control and Prevention compared with the present case.
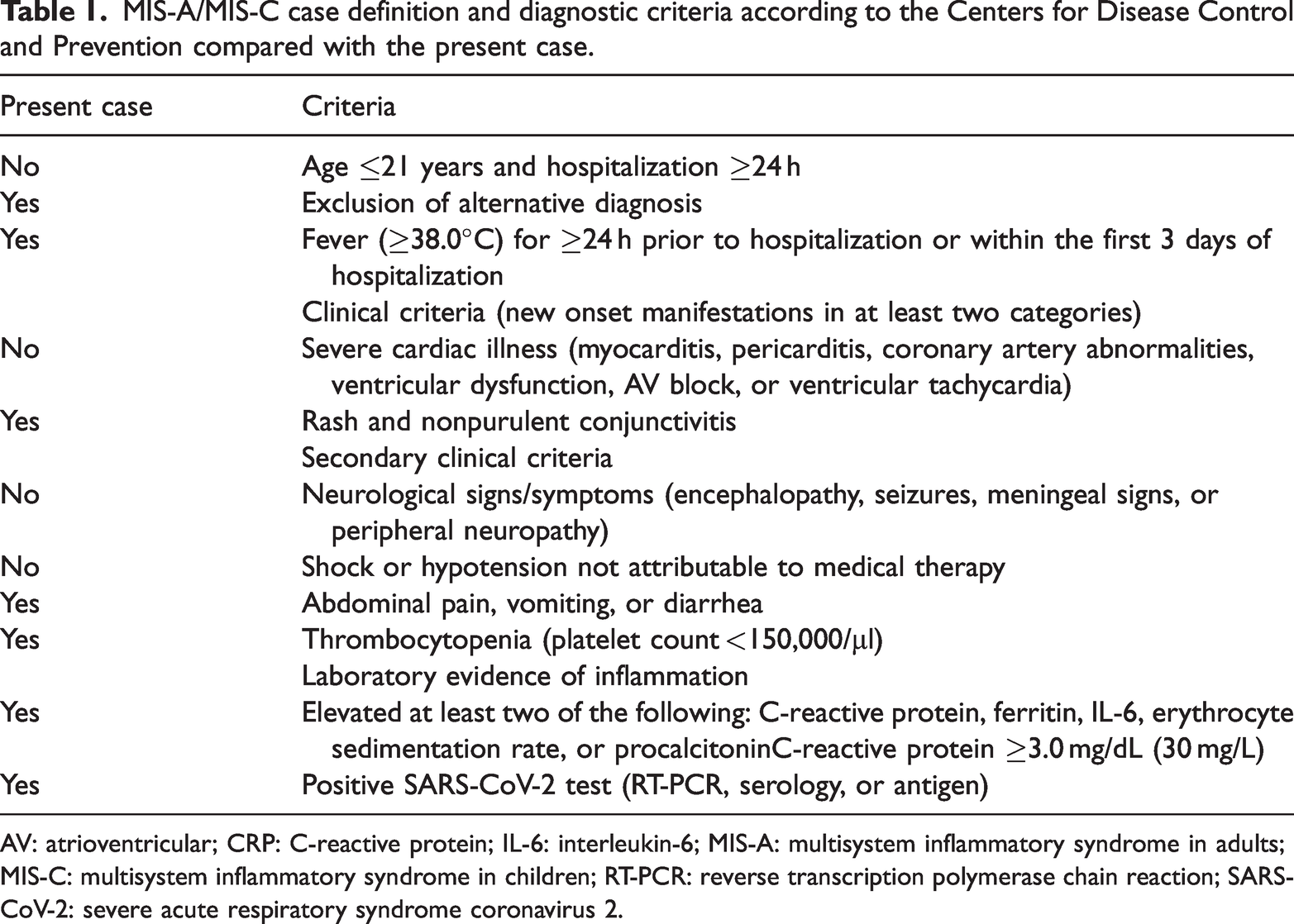
AV: atrioventricular; CRP: C-reactive protein; IL-6: interleukin-6; MIS-A: multisystem inflammatory syndrome in adults; MIS-C: multisystem inflammatory syndrome in children; RT-PCR: reverse transcription polymerase chain reaction; SARS-CoV-2: severe acute respiratory syndrome coronavirus 2.
Elevated inflammatory markers are clinical hallmarks essential for the diagnosis of MIS-C. According to Michael et al., 7 laboratory abnormalities frequently include elevated D-dimer (67%–100%), CRP (90%–100%), and LDH (10%–60%).
The laboratory profile of the present case is consistent with these findings, showing markedly elevated D-dimer and CRP levels. Notably, these markers demonstrated a favorable clinical course, returning to baseline within 2 weeks.
According to the Department of Pediatric Respiratory Diseases, Chongqing, 8 steroids combined with IVIG is standard treatment for most hospitalized patients with MIS-C unless contraindicated. Other therapeutic options include tocilizumab (an interleukin (IL)-6 (IL-6) inhibitor), which may be used in severe cases, and anakinra (an IL-1 inhibitor), which may be considered in IVIG-refractory cases. In patients with severe ventricular dysfunction and risk of thrombosis, heparin or low-molecular-weight heparin (LMWH) may be administered. In the absence of bleeding risk, low-dose aspirin is also recommended. In the present case, management was limited to IVIG, methylprednisolone, and aspirin, as there were no clinical indications for further therapeutic escalation.
Aspirin was administered at a low dose of 3–5 mg/kg/day, in line with established antiplatelet protocols for both MIS-C and KD. To mitigate the risk of Reye syndrome, the patient was screened for predisposing viral infections; influenza and varicella were excluded. The patient’s immunization history also confirmed prior vaccination against both pathogens.
Throughout aspirin therapy, close clinical monitoring was performed to detect any signs of neurological or hepatic compromise, including altered mental status, seizures, lethargy, somnolence, and jaundice. No clinical or laboratory evidence suggestive of Reye syndrome was observed.
Before diagnosing MIS-C, several alternative conditions were excluded. The patient presented with persistent fever, edema, rash, and laboratory evidence of inflammation, prompting consideration of a broad differential diagnosis. Sepsis was excluded based on negative blood cultures and laboratory investigations, as well as significant clinical improvement without antimicrobial therapy. Toxic shock syndrome was considered unlikely due to the absence of severe shock and characteristic skin findings and negative bacterial tests. KD was also considered; however, the patient’s age, thrombocytopenia, and normal echocardiography findings made this diagnosis less likely. Meningitis was excluded based on normal CSF analysis. Bone marrow aspiration ruled out hemophagocytic lymphohistiocytosis, macrophage activation syndrome, and malignancy. Following exclusion of these conditions and detection of COVID-19 antibodies, a diagnostic challenge was encountered, particularly given the absence of documented severe acute respiratory syndrome coronavirus 2 infections in the surrounding community. However, in the context of a compatible clinical presentation and a favorable response to IVIG and steroids, the diagnosis of MIS-C was confirmed. 9
Several biological markers can be used in follow-up monitoring. For example, Anita Bartha-Tatar 10 reported that IL-18 and tumor necrosis factor-alpha (TNF-α) have prognostic value in assessing disease severity. In the present case, D-dimer was used to monitor the patient’s clinical course.
Follow-up in MIS-C may vary depending on initial severity and clinical manifestations and in some cases may require a multidisciplinary team approach. According to Davis Health, 11 cardiological evaluation should be scheduled approximately 4 weeks after discharge, and infectious disease follow-up is recommended within 1 week after completion of steroid therapy; this approach was consistent with the management in our case.
Study limitations
This case report is limited by its focus on a single patient, which restricts the generalizability of the findings. Additionally, due to resource constraints in our clinical setting, advanced genetic testing was not available to definitively exclude other autoinflammatory conditions.
Conclusion
We present a rare case of MIS-C, one of the most uncommon cases reported in our country. Early diagnosis and treatment remain challenging due to overlapping clinical features with other differential diagnoses. MIS-C is a severe, delayed complication that can occur following severe acute respiratory syndrome coronavirus 2 infection in individuals under 19 years of age. Although COVID-19 is typically self-limiting in children, MIS-C may lead to critical, life-threatening complications. In this report, we describe a case of MIS-C in a 1.7-year-old female toddler following severe acute respiratory syndrome coronavirus 2 infection. Due to delayed diagnosis, the patient’s symptoms progressed; however, after administration of corticosteroids and IVIG, marked clinical improvement was observed, leading to complete recovery. This case highlights the importance of considering MIS-C in the differential diagnosis of pediatric patients presenting with vague, nonspecific symptoms, particularly those with a recent history of COVID-19 exposure or infection.
Footnotes
Acknowledgment
The authors used AI tools for language improvement and grammatical editing of this manuscript.
Author contribution
This case report was prepared as a team effort. All authors contributed equally to the collection of clinical information, literature review, case analysis, drafting of the manuscript, and final revision.
Declaration of conflicting interests
The authors declare no competing interests.
Ethics approval and consent to participate
Written informed consent was obtained from the patient’s parent for publication of this case report and any accompanying images. Our institution does not require formal ethics committee approval for case reports.
Funding
There was no funding for this study