
Abstract
Objective
Ultrasound-guided percutaneous renal biopsy is a common diagnostic tool for renal disease. This study investigated the safety and efficiency of free-hand and puncture attachment approaches for ultrasound-guided percutaneous renal biopsy.
Methods
This retrospective, single-center study included 110 patients who underwent ultrasound-guided percutaneous renal biopsy. The patients were divided into the free-hand or puncture attachment group, depending on whether a puncture attachment was used.
Results
The number of glomeruli obtained in the free-hand group was similar to that in the puncture attachment group. Two patients had no glomeruli visible under the microscope and could not be diagnosed. The most common etiologies were immunoglobulin A nephropathy (42 patients; 38.2%) and hypertensive nephropathy (27 patients; 24.5%). Most participants received individual antihemorrhagic treatments. Only three patients had postoperative complications, including gross hematuria, perinephric hematoma, and transient fever, with no significant difference between the free-hand and puncture attachment groups. After biopsy, the number of urinary red blood cells rapidly increased during the first micturition and then decreased during the third micturition.
Conclusions
The rates of hematuria and glomerular yield after renal biopsy were similar between the free-hand and puncture attachment groups. The free-hand approach could be a safe and efficient technique for patients undergoing ultrasound-guided percutaneous renal biopsy without puncture attachment.
Introduction
Kidney biopsy is the “gold standard” for the diagnostic evaluation of glomerular diseases, 1 leading to a revolution in our understanding of glomerular disease pathology and pathogenesis. It enables the diagnosis of glomerulonephritis (GN), guiding treatment selection and long-term outcome prediction.2,3 According to the 2024 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guidelines, kidney biopsy is considered an acceptable and safe diagnostic test for evaluating the cause of kidney disease and guiding treatment decisions when clinically appropriate. 4 Percutaneous renal biopsy (PRB) is currently the standard method. Ultrasound (US)- and computed tomography (CT)–guided biopsies are performed with the patient in the prone position. 5 US-guided PRB is simple, rapid, and widely used; however, this procedure is associated with common post-biopsy complications, such as macroscopic and gross hematuria, perinephric hematomas, arteriovenous fistulas, and injuries to blood vessels and surrounding organs. 5
Given the vascularity of the kidney, bleeding is a substantial risk in patients undergoing renal biopsy, and efforts should be made to mitigate this risk. In a previous retrospective study, perirenal hematoma was detected in 89.9% of 138 patients (104 with native kidneys and 34 with grafts) who underwent kidney magnetic resonance imaging 36–48 h after PRB. 6 Furthermore, CT-guided biopsies are associated with higher complication rates than US-guided procedures.7,8 In a retrospective, single-center review conducted from January 1998 to December 2017, Pombas et al. found that the rate of complications after renal biopsy was 16.6%, and 1.5% were major complications requiring blood transfusion. 9 Schnuelle et al. found that bleeding is the most common complication after renal biopsy, occurring in 1.3%–18% of cases. 10 This study focused on balancing the need to obtain sufficient biopsy tissue with the goal of reducing the incidence of major complications during PRB procedures.
The body-surface projection of the renal biopsy site varies among individuals because of differences in embryonic development and the prone position. During PRB, the needle is advanced under direct, real-time US visualization. Depending on the operator’s preference, a puncture attachment may be used for this technique. A puncture attachment helps maintain stability during needle insertion into the kidney; however, the needle angle cannot be adjusted, and the prone position makes needle maneuvering challenging. The advantage of the free-hand technique, that is PRB without puncture attachment, is that the needle can be freely manipulated after insertion. Because the insertion angle is determined by the operator, needle stability within the body is limited, potentially leading to injury and bleeding. The differences in safety and efficiency between the free-hand and puncture attachment techniques remain unclear; thus, in this study, we evaluated whether the free-hand technique can serve as an alternative method for PRB, aiming to provide further evidence regarding the success and complication rates associated with PRB.
Methods
This retrospective study analyzed 110 renal biopsies performed between 1 March 2021 and 31 July 2025 at the Third People’s Hospital of Jingdezhen, Jiangxi Province, China. Data were collected from renal biopsy records and hospital medical records. All patient details were deidentified, and study reporting conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 11 The procedures and materials used in this study complied with the tenets of the Declaration of Helsinki, 1975, as revised in 2024.
The main indications for renal biopsy in this study were as follows: (a) age ≥18–80 years; (b) diagnosis of proteinuria and/or glomerular hematuria, acute kidney injury/rapidly progressive GN, or chronic kidney disease; 1 (c) written informed consent provided before renal biopsy; and (d) the patient’s ability to follow instructions. Participants with coagulation disorders, severe anemia, uncontrolled hypertension (>140/90 mmHg), small hyperechoic kidneys on US, skin infection over the biopsy area, active kidney infection/pyelonephritis or perirenal abscess, and other conditions inappropriate for PRB were excluded. 10
Assignment to the free-hand or puncture attachment group was based on operator preference. Written informed consent was obtained the day before the procedure and reconfirmed on the day of the procedure. All patients were scanned using the same color US diagnostic system (Wisonic Piloter; China) with a single 18-gauge (G) needle (Bard MC1816, Tempe; AZ, USA). US settings were not rigorously standardized throughout the study period. The US settings (depth, gain, and focus) were adjusted with minor variations among participants depending on operator preference. The US-guided renal biopsy procedure involved the following steps:12,13
(1) Preparation. (1) Anticoagulant or antiplatelet agents were discontinued at least 3 days before the biopsy. (2) Preoperative breathing training was provided to help patients cooperate during the procedure. (3) Routine blood, coagulation, and other standard laboratory tests were performed. (2) Procedure. (1) The patient was placed in the prone position with an elastic belt placed under the abdomen. (2) Aseptic and antiseptic preparation of the procedure site was performed. (3) Local anesthesia with 2% lidocaine was administered. (4) Color Doppler US was used (to characterize intrarenal vascular structures and reduce the risk of hemorrhagic complications) to identify the biopsy target region (posterior lower pole of the kidney). (5) The needle path was selected, and the entry site was marked on the skin. (6) The needle was inserted under real-time US guidance. (7) One to three tissue fragments were obtained by core biopsy using either the free-hand or puncture attachment technique. (8) Specimens were placed in appropriate containers for pathological analysis. (3) Postprocedure. Patients were kept on strict bed rest for 6 h. Blood pressure and heart rate were monitored every 30 min for the first 2 h, hourly for the next 4 h, and every 4 h for the subsequent 18 h. After biopsy, three consecutive urine samples were collected for urinalysis to evaluate urinary red blood cell (RBC) counts.
Antihemorrhagic agents were administered to prevent postoperative bleeding. The selection of agents was based on efficacy, safety, clinicians’ experience in similar cases, patient-specific factors (such as age, organ function, and comorbidities), cost-effectiveness, availability, patient preference, and regulatory and legal considerations. The agents used included desmopressin, carbazochrome sodium sulfonate, tranexamic acid, aminocaproic acid, etamsylate, and hemocoagulase.14–21 Treatment choices were determined according to the specialists’ clinical experience.
Adequate assessment of kidney biopsies included light microscopy, immunofluorescence, and electron microscopy. The postoperative urinary RBC count in high-power microscopic fields was recorded. The number of glomeruli was obtained from renal pathology reports.
Major complications were defined as those requiring intervention, such as a blood transfusion or an invasive radiologic or surgical procedure, or those resulting in severe hypotension, acute renal obstruction or failure, septicemia, readmission, surgery, arteriography, or nephrectomy. Minor complications were defined as arteriovenous fistula, gross hematuria, post-procedural hypotension, severe flank pain, gross hematuria, and/or perinephric hematoma that resolved spontaneously without the need for further intervention.22–24 Bleeding was assessed by ultrasonography within 24–72 h.
Statistical analysis
Continuous variables were reported as mean ± SD or median (quartile) and were compared using an independent t test or Mann–Whitney U test, as appropriate. The Wilcoxon paired test was used to compare preoperative and postoperative values. Categorical variables were expressed as frequencies (percentages) and were compared using the χ2 test or Fisher’s exact test, as appropriate. A univariate general linear model was used to examine the effects of hemostatic agents on postoperative urinary RBC counts, using Type III sum of squares. Bonferroni correction was applied for post hoc comparisons. Statistical significance was defined as a two-sided p-value <0.05. All analyses were performed using Statistical Package for the Social Sciences (SPSS) version 24 (IBM SPSS Statistics; Armonk, NY, USA).
Handling of missing data
The proportion of missing data among the 110 patients ranged from 0.9% to 21.8% across variables (Supplemental Table 2). The highest rates were observed for renal length and width (21.8% each), followed by preoperative RBC count (17.3%) and use of hemostatic drugs (11.8%). Missing data pattern analysis suggested that the data were not missing completely at random; therefore, complete-case analysis was considered inappropriate.
Multiple imputation was performed to maximize use of available data and reduce potential bias. The imputation model included all analytical variables: punctured renal length, punctured renal width, number of punctures, preoperative RBC count, preoperative and three postoperative urinary RBC count, hemoglobin, platelet count, serum creatinine, blood urea nitrogen, hypertension, diabetes mellitus, and antihemorrhagic agents. The original drug variable contained 10 categories, several of which had very low frequencies (<5). To reduce model complexity and improve stability, this variable was recorded into three clinically meaningful categories: (a) no drug; (b) single drug (desmopressin, ethamsylate, or aminomethylbenzoic acid); and (c) combination therapy (two or more drugs). Hypertension and diabetes were treated as binary variables, and all continuous variables were retained at their original scales. Multiple imputation was performed using the fully conditional specification (FCS) method with 10 iterations, generating 10 complete imputed datasets. Linear regression was used for continuous variables, and logistic regression was used for categorical variables. Sensitivity analysis using complete-case data yielded similar results, indicating the robustness of the multiple imputation approach.
Results
The baseline characteristics of patients who underwent renal biopsy are shown in Table 1. A total of 69 males and 41 females were enrolled in this study. The median age was 49.8 years in the free-hand group and 54.8 years in the puncture attachment group. Of the included participants, 62.9% had hypertension and fewer than 50% had diabetes mellitus. There were no significant differences in sex distribution, hypertension, or diabetes mellitus between the free-hand and puncture attachment groups. The median hemoglobin and platelet levels in both groups were 127.1 g/L and 233.1 × 109/L, respectively, with no significant differences between the groups. Serum creatinine and blood urea nitrogen levels were also comparable between the two groups.
Baseline characteristics of patients who underwent renal biopsy.

Data for 24 participants were not fully recorded. Their renal length and width measurements were missing. Underlying conditions were missing in five cases.
Most PRB procedures were performed on the right kidney, with the needle inserted medially three times. The median length and width of the punctured kidneys were 102.5 mm and 47.1 mm, respectively. The mean number of glomeruli obtained per biopsy sample was 19.2 ± 8.1. Twenty-seven patients had at least two types of pathological changes. Two patients had no visible glomeruli under the microscope and could not be diagnosed. The main etiologies were immunoglobulin A nephropathy (42 cases; 38.2%), hypertensive nephropathy (27 cases; 24.5%), membranous nephropathy (13 cases; 11.8%), diabetic nephropathy (11 cases; 10.0%), focal segmental glomerulosclerosis in (9 cases; 8.2%), acute tubular injury (5 cases; 4.5%), and minimal change disease and membranoproliferative GN (4 cases; 3.6%). Henoch–Schönlein purpura nephritis, renal amyloidosis, antineutrophil cytoplasmic antibody–associated vasculitis, lupus nephritis, and podocytosis were observed in one participant each (Table 2).
Pathological results of representative renal biopsies (n = 108).

Twenty-seven samples of representative renal biopsies represented at least two pathological findings. In 2 of 110 patients, no glomeruli was observed under the microscope.
IgA: immunoglobulin A.
After biopsy, 108 of the 110 patients received antihemorrhagic drugs to prevent bleeding. The antihemorrhagic treatments administered in both groups are shown in Table 3. Etamsylate and desmopressin were the most commonly used drugs. The proportions of different antihemorrhagic treatments were similar (p = 0.179). The proportions of desmopressin and etamsylate were higher in the puncture attachment group than in the free-hand group. The postoperative complication rate was 2.7% (n = 3), including gross hematuria, perinephric hematoma, and transient fever. None of the patients required blood transfusion.
Postoperative antihemorrhagic drugs in patients.

Null refers to data that were not obtained; None refers to patients who underwent percutaneous renal biopsy did not receive antihemorrhagic drugs.
Urinary RBC counts were significantly increased at first urination after biopsy in both the free-hand and puncture attachment groups and decreased substantially by the third urination (Figure 1). There were no significant differences in RBC counts either preoperatively or postoperatively between the two groups (Table 4).
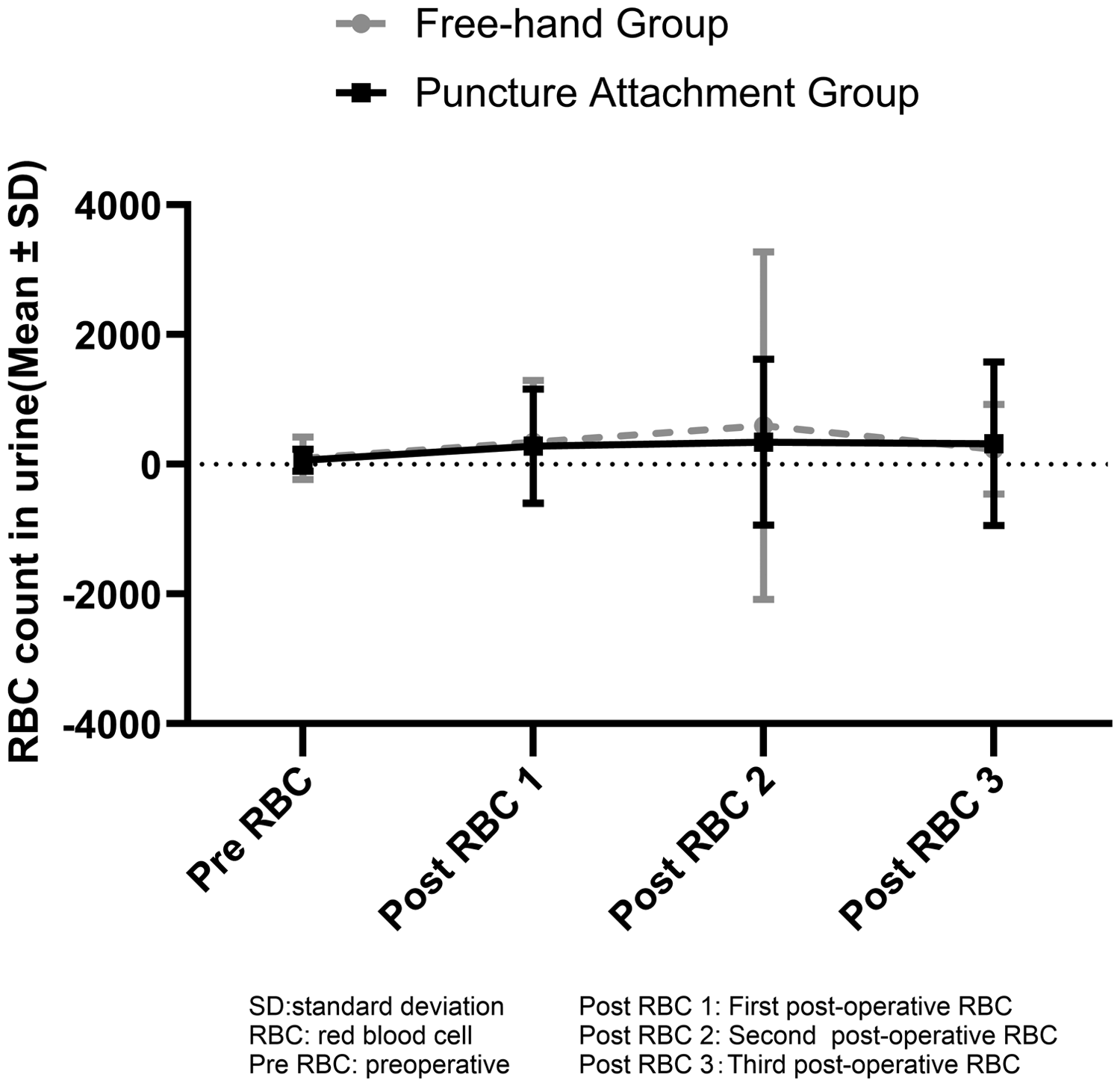
Change in mean urinary red blood cell count among different groups after biopsy.
Preoperative and postoperative urinary red blood cell counts.

Preoperative urinary RBC values were missing for 19 patients. First postoperative urinary RBC values were missing for 11 patients. Second postoperative urinary RBC values were missing for 12 patients. Third postoperative urinary RBC values were missing for 13 patients.
RBC: red blood cell.
The effect of antihemorrhagic drugs on postoperative hematuria exhibited significant time-specific characteristics (Table 5). Model 1 was not significant (F = 0.751, p = 0.770). A substantial proportion of variance was explained in Model 2 (adjusted R2 = 0.593, F = 6.382, p < 0.001) and Model 3 (adjusted R2 = 0.929, F = 46.890, p < 0.001). Significant predictors in Model 2 included age (F = 5.905, p = 0.018), first postoperative urine RBC count (F = 44.929, p < 0.001), and antihemorrhagic drug treatment (F = 6.975, p < 0.001). In the post hoc pairwise comparisons, the combination of hemocoagulase and etamsylate showed a significant difference compared with the other drugs (all p < 0.001; Supplemental Table 4). The third postoperative urinary RBC count was significantly associated with the first postoperative urine RBC count (F = 538.662, p < 0.001). Neither group assignment nor the interaction term contributed significantly to any of the models.
Multivariate analysis of variance for the effects of antihemorrhagic drugs on postoperative hematuria.

F values represent Type III sum of squares. Model 1 included age, sex, puncture number, comorbidities, platelet count, creatinine, medication, and preoperative urinary RBC count as covariates. Model 2 included all covariates from Model 1 plus the first postoperative urinary RBC count. Model 3 included all covariates from Model 2 plus the second postoperative urinary RBC count. Sex, puncture number, comorbidities, platelet count, and creatinine were not statistically significant in any the three models and are not shown in the table. Fixed factors and interaction terms were the same across all three models (antihemorrhagic treatment, group, group × antihemorrhagic interaction). Due to missing data, sample sizes for Models 1, 2, and 3 were 89, 88, and 87, respectively.
RBC: red blood cell.
Discussion
Renal biopsy, an essential tool in daily nephrological practice, is necessary to obtain a histological diagnosis and may impact therapeutic management. 12 The types of renal biopsy include open, percutaneous, laparoscopic, transjugular, and transurethral approaches. 5 US-guided PRB is superior to the blind technique, requiring fewer attempts and maintaining equivalent tissue adequacy and a similar bleeding complication rate. 25 PRB is the most widely used technique because it is simple and fast and has a high success rate with few complications; 5 however, severe complications, including death, can still occur. In our study, most participants underwent three right kidney punctures and experienced a transient increase in urinary RBCs. The postoperative complication rate was 2.7% in all patients, and no deaths or blood transfusions occurred.
Some patients have contraindications to PRB; in such cases, alternative renal biopsy methods have been attempted. Bolufer et al. found that transjugular renal biopsy enabled histological diagnosis in two-thirds of patients for whom percutaneous US-guided renal biopsy was contraindicated. 26 St. Jeor et al. reported that the incidence of bleeding complications across 15 articles with complete data was 202 of 892 procedures (22.6%), including 162 (18.2%) minor and 40 (4.5%) major events. This finding indicates that transjugular renal biopsy is a feasible procedure for obtaining renal tissue for diagnosis, with most complications being self-limiting. 27 Patients with systemic lupus erythematosus and antiphospholipid antibody syndrome may undergo transjugular renal biopsy, whereas transcutaneous renal biopsy is associated with an increased risk of bleeding. 28 Aoun et al. performed a matched-pair analysis (1:3 matching) of 40 patients who underwent transperitoneal laparoscopic renal biopsy and 120 who underwent PRB during the same period and found that the laparoscopic approach was associated with a significantly higher diagnostic yield (82.5% vs. 63.5%, p = 0.027) and a lower complication rate (0% vs. 4%, p < 0.001), particularly regarding the need for transfusion due to postprocedure bleeding (0% vs. 1.8%, p < 0.001), compared with the percutaneous approach. 29 Transperitoneal laparoscopic renal biopsy is considered a suitable option for patients with contraindications to PRB, as it is safer and more effective for diagnosing renal disease than other approaches.30,31
The most common complication of renal biopsy is bleeding. Reported frequencies of perirenal hematoma after US-guided renal biopsy in adults vary substantially across studies (1.1%–85%). 32 Poggio et al. conducted a random-effects meta-analysis including 118,064 biopsies; 33 hematomas were estimated to occur in 11% of cases, macroscopic hematuria in 3.5%, bleeding requiring blood transfusions in 1.6%, and interventions to control bleeding in only 0.3%. Corapi et al. summarized 34 studies comprising 9474 biopsies and reported a macroscopic hematuria rate of 3.5% and an erythrocyte transfusion rate of 0.9%. 34 Female sex, body mass index (BMI) ≥28 kg/m2, and immediate post-biopsy active bleeding have been identified as risk factors for perirenal hematoma after real-time US-guided PRB of native kidneys. 33 Factors associated with larger perirenal hematoma include needle gauge, number of passes, impaired renal function, coagulopathy, and certain histopathologies. 32 Jung et al. reported that older age, obesity, and smoking are independently associated with a lower risk of complications. 35 Furthermore, older age has been identified as an independent risk factor for blood transfusion requirement. 9 Major complications are most commonly associated with increased activated partial thromboplastin time and decreased baseline hemoglobin levels. 9 In our study, the first postoperative urinary RBC count was associated with the third measurement; thus, the first postoperative RBC count may be a predictor of postoperative hematuria.
Reasonable observation of patients after renal biopsy helps identify post-biopsy complications. In our study, all patients were closely monitored, underwent 6 h of bed rest, and were allowed to resume activity 24 h after biopsy to reduce the risk of postoperative complications and ensure timely management when needed. Trinh et al. suggested that a 4-h observation period may be safe and sufficient to detect most clinically significant complications within the first 24 h, potentially saving time and resources. 36 In Robert et al.’s retrospective study of 576 patients, a 3-h monitoring window before discharge was found to be safe, supporting more efficient resource utilization. 37 Lin et al. analyzed data from 10 eligible studies (1801 patients; 203 bleeding events), reporting similar rates of bleeding and major complications in outpatient and inpatient renal biopsy settings. 38 Further studies are needed to determine whether an optimal post-biopsy observation period exists for detecting complications and conserving resources, and if so, how it may vary across different patient populations.
Anticoagulants are typically used to prevent bleeding after biopsy. In our study, antihemorrhagic drugs were significantly associated with the second postoperative urinary RBC count. The management of antihemorrhagic drugs during renal biopsy may merit consideration as a factor influencing postoperative bleeding risk; however, this requires confirmation in other cohorts. Hemocoagulase is a detoxified and purified snake venom enzyme that has been reported to reduce post-renal biopsy hemoglobin decline and prevent post-renal biopsy bleeding without adverse events (e.g. thrombosis and anaphylactic shock). 17 Desmopressin reduces unplanned hospitalizations and bleeding interventions (angiography and embolization) after nonfocal renal biopsy without an observed increase in thromboembolism. 14 Tranexamic acid and etamsylate have been used to control bleeding in patients with autosomal dominant polycystic kidney disease presenting with persistent gross hematuria. 21 In our study, antihemorrhagic agents were administered in a non-standardized manner, with multiple regimens used across groups. We adjusted for this confounder in the general model, and the combination of hemocoagulase and etamsylate was associated with higher RBC counts compared with other treatments. This finding should be interpreted with caution given the very small sample size (n = 2). More evidence on the use of hemostatic agents in renal biopsy is needed before broad recommendations can be made.
The needle size was not uniform across renal biopsies. 10 Both 16-G and 18-G needles are widely used.39,40 In our study, the adequacy rate of renal biopsy was 98.2% using real-time US guidance with an 18-G automated needle, indicating a high procedural success rate. The 18-G needle is considered as effective as the 16-G needle for PRB and is associated with a lower risk of large hematoma and arteriovenous fistula formation. 40 Sousanieh et al. suggested that using a 16-G needle yields optimal samples from both native and transplanted kidneys; however, in transplant biopsies, the use of an 18-G needle may compromise diagnostic accuracy and does not necessarily improve safety. 39 Xie et al. found no significant differences in the number of glomeruli obtained, adequacy rates, or complication rates between 18-G or 16-G needles. They also reported that the use of an 18-G needle does not affect the pathological diagnosis or classification of immunoglobulin A nephropathy and lupus nephritis. 41 Korbet et al. reported that adequate tissue for diagnosis was obtained in 99% of 1055 adults who underwent renal biopsy using real-time US guidance and 14-G biopsy needles; moreover, 4.5% developed gross hematuria, and only one death (0.09%) resulted from post-PRB bleeding. 22 Nicholson et al. demonstrated that the use of a 14-G needle resulted in a significantly larger sample size (15 vs. 11 vs. 9 glomeruli, p < 0.05) and higher diagnostic success (85% vs. 76% vs. 53%, p < 0.05) than 16-G or 18-G needles. 42 Larger needles are more diagnostically useful because they yield more tissue and glomeruli; however, they are also associated with increased pain and a higher risk of bleeding. Further studies are needed to determine the optimal balance between diagnostic yield and complication risk when selecting needle size.
The safety of renal biopsy relies on appropriate patient selection, proper management of modifiable risk factors, adequate post-procedural monitoring, and the technique used to localize and puncture the kidney. Brardi et al. showed that US-guided PRB using a perforated probe and a perpendicular needle trajectory reduced the risk of post-biopsy bleeding. 43 A biopsy angle of approximately 60°, directed toward the poles and avoiding the medulla, has been associated with fewer inadequate samples and fewer bleeding complications. 44 Puncture attachment is useful for controlling the biopsy angle and reducing bleeding; however, the needle cannot be repositioned after insertion. The free-hand technique for US-guided PRB is simpler and more flexible than puncture attachment and requires fewer devices. In our study, the tissue yield and number of glomeruli obtained did not differ significantly between the free-hand and puncture attachment groups. The pathological diagnostic rates were similar between the two groups. Because the needle is manually controlled, the free-hand technique requires the operator to stabilize the needle angle individually, which may theoretically increase the risk of bleeding. In our study, no significant difference was observed in postoperative urinary RBC counts between the free-hand and puncture attachment groups, indicating that the bleeding risk was not increased with the free-hand approach. Generally, the safety of such procedures depends on the operator’s proficiency and cooperation. Boiled eggs have been proposed as useful simulation models for renal biopsy practice; 45 ultrasonographic evaluation shows a clear contrast between the egg yolk and white, mimicking the renal cortex and medulla. When access to puncture attachments or operator experience is limited, the free-hand technique may represent a feasible alternative for US-guided PRB.
Few postoperative complications were observed in the current study, potentially due to the small sample size and the use of a smaller needle, which is associated with a reduced risk of tissue damage. Furthermore, operators followed standard operating procedures, and all invasive procedures were performed under real-time US guidance. Adequate postoperative bed rest, observation, and administration of hemostatic medication were also provided, which may have contributed to reducing the risk of postoperative complications. Further studies are needed to confirm the impact of these factors on postoperative complication rates.
This study has several limitations. As a retrospective, single-center study with a limited sample size and a specific patient population, the generalizability of the findings is limited. Group allocation was not randomized, and some data were missing. US settings were not rigorously standardized across the study period; instead, depth, gain, and focus were adjusted according to operator preference. Statistical methods were applied to mitigate the influence of these limitations on the findings. Further prospective studies are required to validate the results of this study.
In conclusion, both free-hand and puncture attachment techniques in PRB of native kidneys in adults using real-time US guidance and an 18-G automated needle demonstrated a high success rate and a favorable safety profile in our study. The free-hand approach may be a feasible alternative for patients undergoing US-guided PRB without puncture attachment; however, these findings should be interpreted with caution and confirmed in prospective studies.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261455146 - Supplemental material for Ultrasound-guided percutaneous renal biopsy: Free-hand versus puncture attachment
Supplemental material, sj-pdf-1-imr-10.1177_03000605261455146 for Ultrasound-guided percutaneous renal biopsy: Free-hand versus puncture attachment by Yingzi Lv, Guizhen He, Liling Feng, Xiaokang Cheng, Jingyu Deng, Yingxin Zhu, Shuifa Wang, Guoan Yu, Qiang Tu, Xiaohui Yu, Yun Wu, Xianglan Zhang, Liwen Lai, Qingxiu Zhu and Yao Jiang in Journal of International Medical Research
Footnotes
Acknowledgment
Special thanks to the staff of the Department of Nephrology, The Third People’s Hospital of Jingdezhen, for their wonderful support with patient management.
Author contributions
Yingzi Lv: formal analysis, investigation, validation, data curation, writing—original draft, and writing—review and editing; Qingxiu Zhu: conceptualization, data curation, methodology, investigation, and funding acquisition; Guizhen He, Xiaokang Cheng, Jingyu Deng, Shuifa Wang, Guoan Yu, Qiang Tu, and Xiaohui Yu: data curation, investigation, and validation; Liling Feng, Yingxin Zhu, Yun Wu, and Xianglan Zhang: data curation and investigation; Liwen Lai: conceptualization ad methodology; Yao Jiang: conceptualization, formal analysis, investigation, data curation, validation, writing—original draft, writing—review and editing, and funding acquisition.
Data availability statement
All data generated or analyzed during this study are included in this article. Further inquiries can be directed to the corresponding authors.
Competing interests
The authors declare no competing interests.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Funding
This work was supported by the Jiangxi Province Administration of Traditional Chinese Medicine Program (2023A0084) and The Third People’s Hospital of Jingdezhen Science and Technology Program (2024YJYB09).
Statement of ethics
The study protocol was reviewed and approved by the Human Research Ethics Committee of The Third People’s Hospital of Jingdezhen (approval number: LL202408; date 29 March 2024). The procedures and materials used in this study complied with the Declaration of Helsinki, 1975, as revised in 2024. As the study involved only a review of electronic medical records, the requirement for written informed consent was waived.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.