
Abstract
Objective
Unexplained recurrent spontaneous abortion is a multifactorial condition with an unclear etiology. This study aimed to investigate the relationship between liver function biomarkers and unexplained recurrent spontaneous abortion and explore interactions with tobacco exposure and body mass index.
Methods
A retrospective case–control study was conducted on 2126 pregnant women, including 602 with unexplained recurrent spontaneous abortion and 1524 who served as controls. Liver enzyme indicators (alanine aminotransferase, aspartate aminotransferase, gamma-glutamyl transferase, and alkaline phosphatase) were assessed, and multivariate logistic regression models were applied to analyze their association with unexplained recurrent spontaneous abortion. Interaction analyses were performed to evaluate combined effects of liver enzyme abnormalities, tobacco exposure, and body mass index.
Results
Liver enzyme abnormalities (alanine aminotransferase level >32 U/L or aspartate aminotransferase level >28 U/L) were significantly associated with increased unexplained recurrent spontaneous abortion risk (adjusted odds ratio = 2.15, 95% confidence interval: 1.68–2.76). A significant interaction between alanine aminotransferase elevation and tobacco exposure was observed (p < 0.001). Among non-exposed women, elevated alanine aminotransferase levels were associated with an odds ratio of 1.8 (95% confidence interval: 1.2–2.7), whereas among tobacco-exposed women, the odds ratio was 5.2 (95% confidence interval: 3.1–8.7) (p for interaction <0.001). However, these interaction results warrant cautious interpretation due to the absence of quantitative tobacco exposure metrics. The alanine aminotransferase–body mass index interaction was not significant (p = 0.179).
Conclusions
Elevated alanine aminotransferase and aspartate aminotransferase levels are independently associated with unexplained recurrent spontaneous abortion, and tobacco exposure significantly strengthened this association. These findings suggest that liver function abnormalities and tobacco exposure are associated with unexplained recurrent spontaneous abortion risk. However, given the limitations associated with tobacco exposure measurement, these findings should be interpreted with caution.
Keywords
Introduction
Recurrent spontaneous abortion (RSA) is a significant clinical issue in obstetrics and gynecology, defined as the occurrence of two or more consecutive pregnancy failures, affecting approximately 2.5% of women of reproductive age. 1 Known causes include chromosomal abnormalities, uterine structural defects, endocrine disorders, immune factors, and thrombophilia. However, approximately 50% of RSA cases remain unexplained and are classified as “unexplained recurrent spontaneous abortion (URSA).” 2 This diagnostic gap not only places a heavy psychological burden on patients but also presents a challenge for clinicians in developing effective treatment strategies.
In recent years, as research on the mechanisms of pregnancy maintenance has deepened, the association between maternal systemic diseases and pregnancy outcomes has gained increasing attention. The liver is a key metabolic organ. Liver dysfunction can disrupt estrogen metabolism, induce coagulation abnormalities, and cause inflammatory imbalance. These disturbances may subsequently affect embryo implantation and placental development.3–8 Studies have shown that abnormal liver enzyme levels are associated with adverse pregnancy outcomes. For example, a large retrospective cohort study of 10,175 pregnant women in Shanghai confirmed that abnormal liver function in early pregnancy increases the risk of spontaneous abortion by 55% (adjusted relative risk (aRR) = 1.55, 95% confidence interval (CI): 1.26–1.92), furthermore, each 1-SD increase in gamma-glutamyl transferase (GGT) and alkaline phosphatase (ALP) levels was linearly associated with a rise in abortion risk. 9 However, research on URSA remains limited. In particular, the dose–response relationship between liver function markers and RSA risk as well as the underlying mechanisms has been rarely investigated. URSA may be related to maternal microenvironment disturbances, including oxidative stress, chronic inflammation, and metabolic dysregulation. In this context, liver enzymes such as GGT and alanine aminotransferase (ALT) can serve as serum biomarkers for these subclinical states to identify high-risk populations.10–12 Furthermore, liver enzyme levels are also influenced by external environmental factors such as smoking, a well-recognized inducer of oxidative stress and inflammation. 13 These factors can cause liver injury and elevated liver enzymes via induction of hepatic oxidative stress and lipid peroxidation, 14 thereby potentially affecting pregnancy outcomes via pathways similar to or synergistic with those of abnormal liver enzymes. Nevertheless, large-scale studies systematically examining the interactions among these factors and their combined effects on RSA risk are still lacking.
To address this research gap, the present study utilized a large-scale clinical dataset. We applied multivariable logistic regression and stratified analysis to systematically explore the relationship between liver function markers and RSA risk. The study specifically focused on the following aspects. First, we analyzed the independent association between liver enzyme levels and RSA risk. Second, we investigated the interactions between liver function markers and other risk factors (e.g. tobacco exposure and body mass index (BMI)). The findings are expected to provide new perspectives for etiological research on RSA and offer scientific evidence for clinical risk assessment and preventive strategy development.
By deeply exploring the relationship between liver function and RSA, this study not only contributes to refining the etiological framework of RSA but may also provide important guidance for the development of new prevention and intervention measures. For patients with URSA, liver function assessment may become an important component of routine clinical diagnosis and treatment, offering new insights for personalized treatment and precision medicine.
Methods
Study design and participants
This study employed a retrospective case–control design, with data sourced from the electronic medical record (EMR) system of the Department of Obstetrics and Gynecology at Renmin Hospital of Wuhan University, from January 2018 to December 2024. According to the guidelines provided by the European Society of Human Reproduction and Embryology and American Society for Reproductive Medicine (ASRM), RSA is defined as two or more consecutive or non-consecutive miscarriages, including biochemical pregnancies and pregnancies of unknown location.15,16
Cases were identified from the EMR by searching for discharge diagnoses of recurrent miscarriage, followed by manual verification of two or more consecutive pregnancy losses before 20 weeks and documented exclusion of known causes. Exclusion of known causes required documented normal results of the following: (a) parental or product karyotyping; (b) pelvic ultrasound (including adnexa) or hysterosalpingography/hysteroscopy; (c) thyroid function; (d) glucose tolerance test; (e) antiphospholipid antibodies; (f) lupus anticoagulant test; (g) thrombophilia panel (coagulation function test and protein C/S); and (h) toxoplasmosis, other agents, rubella, cytomegalovirus, and herpes simplex virus (TORCH)/syphilis/Human Immunodeficiency Virus (HIV)/hepatitis screening.
The following inclusion criteria were applied for the case group: (a) two or more consecutive spontaneous miscarriages before 20 weeks of gestation; (b) systematic examination to exclude known causes (including chromosomal abnormalities in both partners, uterine anatomical defects, endocrine disorders, autoimmune diseases, thrombophilia, and infections); (c) complete clinical records; and (d) exclusion of organic liver disease.
The inclusion criteria for the control group were as follows: (a) normal pregnancy with no history of miscarriage; (b) no pregnancy-related complications; (c) no major medical or surgical comorbidities; (d) normal perinatal outcomes; and (e) exclusion of organic liver disease. Controls were frequency-matched to cases by age (±3 years) and gestational age at blood sampling (±2 weeks).
In total, 2126 participants were included in the study. All patients meeting the eligibility criteria during the study period were consecutively included; no random or selective sampling was applied. Although no a priori sample size calculation was performed due to the retrospective design, the achieved sample size (602 cases and 1524 controls) exceeded the minimum required based on a post‑hoc calculation (204 cases and 408 controls) for detecting an odds ratio (OR) of 2.0 with 80% power at α of 0.05.
Data collection and processing
Data were collected from the hospital’s EMR system, with independent dual entry to ensure accuracy. Miscarriage history was extracted from the documented obstetric history (gravidity and parity records), and tobacco exposure was retrieved from clinicians’ notes recorded during routine prenatal visits. With respect to the timing of blood sample collection, for cases, blood samples were collected at the time of hospital admission for the miscarriage event (before any medical or surgical intervention). For controls, blood samples were collected during routine first‑trimester prenatal visits (gestational weeks 6–12). The collected variables included the following: (a) Basic clinical information. Demographic characteristics such as age (years), height (m), weight (kg), and calculation of BMI (kg/m2); (b) Pregnancy-related information. Gravidity (total number of pregnancies) and parity (number of live births ≥28 weeks); (c) Lifestyle factors. Tobacco exposure (defined as smoking ≥1 cigarette per day or exposure to secondhand smoke ≥3 times per week for ≥30 min per session); (d) Menstrual history. Age at menarche (years) and menstrual cycle regularity (a cycle length of 21–35 days was considered regular); (e) Laboratory parameters. Liver function tests for ALT, aspartate aminotransferase (AST), GGT, and ALP levels measured using a Hitachi 7600 automatic biochemistry analyzer (all blood samples were collected after an overnight fast); and (f) Bilirubin metabolism markers. Total bilirubin (TBIL), direct bilirubin (DBIL), and calculated indirect bilirubin (IBIL) levels. Patient records were anonymized and deidentified prior to analysis.
Variable definitions and grouping
Liver enzyme levels and tobacco exposure were the primary study variables. Liver enzyme abnormalities were defined based on previous studies; the normal range for ALT during early pregnancy was 6–32 U/L and that for AST was 10–28 U/L. 17 Abnormal liver enzyme levels were classified as ALT >32 U/L and AST >28 U/L. Tobacco exposure was categorized as no exposure (0) and exposure (1). Menstrual cycle regularity was classified as regular (0) and irregular (1). The outcome variable, RSA, was defined as a binary classification variable (0 = control group, 1 = case group).
Statistical analyses
There were no missing data for the main variables (age, BMI, tobacco exposure, gravidity, ALT level, and AST level) in the final dataset. Descriptive statistical analyses were performed for all variables; means, SD, medians, and interquartile ranges were calculated. Normally distributed variables were summarized using mean and SD values, whereas non-normally distributed variables were presented as medians and interquartile ranges. Normality was tested using the Shapiro–Wilk test. To assess multicollinearity between liver function indicators, Pearson’s correlation coefficients were calculated for ALT, AST, GGT, ALP, TBIL, DBIL, and IBIL levels. Variance inflation factors (VIFs) were calculated for all covariates in the full model; all VIF values were <2, indicating no significant multicollinearity. All covariates (age, BMI, tobacco exposure, gravidity, and in sensitivity analyses, age at menarche, and menstrual cycle regularity) were selected a priori based on clinical knowledge and prior literature. No stepwise or data‑driven variable selection was performed. To assess the relationship between liver function indicators and RSA, multivariable logistic regression models were constructed. Two main models were fitted. Model 1 included ALT and AST levels as continuous variables; Model 2 replaced continuous ALT and AST with dichotomized abnormal indicators (ALT > 32 U/L, AST > 28 U/L). Both models were adjusted for the same set of covariates selected a priori based on clinical knowledge and prior literature as follows: age, BMI, tobacco exposure, and gravidity. All models were fitted using binary logistic regression to calculate adjusted odds ratios (aORs) and 95% CIs. To address potential small sample bias or extreme estimates due to complete separation, Firth’s penalized likelihood method was applied (‘logistf’ package). To further explore dose–response relationships, ALT and AST levels were additionally analyzed by quartiles. Interaction terms (e.g. ALT level × tobacco exposure, ALT level × BMI, AST level ×tobacco exposure, and AST level × BMI) were introduced to examine effect modification. The significance of each interaction was assessed using the likelihood ratio test, comparing the model with the interaction term to the model without it. A p‑value <0.05 was considered statistically significant.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement for case–control studies. 18
Software and tools
The following R packages were used for analysis: (a) ‘tidyverse’ (1.3.0) for data processing; (b) ‘rms’ (6.2.0) and ‘logistf’ (1.24) for statistical modeling; (c) ‘ggplot2’ (3.3.5) and ‘ggpubr’ (0.4.0) for visualization; and (d) ‘interactions’ (1.1.0) for interaction testing.
Results
Characteristics of the study population
In total, 2126 pregnant women were included in this study, with 602 in the RSA group (28.3%) and 1524 in the control group (71.7%). A comparison of the baseline characteristics between the two groups is presented in Table 1. The RSA group had a significantly higher average BMI than the control group (24.26 ± 4.09 vs. 22.27 ±3.72 kg/m2) and higher gravidity (2.20 ±1.20 vs. 1.81 ± 0.95). In terms of lifestyle factors, the RSA group had a significantly higher tobacco exposure rate (49.2% vs. 16.7%, p < 0.001) and a higher proportion of women with irregular menstrual cycles (54.3% vs. 31.4%, p < 0.001). There were no significant differences between the two groups in terms of age, gestational age, parity, and age at menarche.
Characteristics of the URSA case and control groups.

URSA: unexplained recurrent spontaneous abortion; BMI: body mass index.
Comparison of liver function indicators between the two groups
To examine the differences in liver function indicators between the RSA and control groups, we employed a combination of normality and non-parametric tests. The Shapiro–Wilk test indicated that some liver function indicators were not normally distributed; therefore, the Wilcoxon test was used for variables that did not meet the normality assumption. The median ALT level of the RSA group was significantly higher than that of the control group (21.40 vs. 15.03 U/L, p < 0.001). The median AST level of the RSA group was significantly higher than that of the control group (28.59 U/L vs. 24.66 U/L, p < 0.001). These differences showed strong statistical significance. For other liver function indicators such as GGT, ALP, TBIL, DBIL, IBIL, and bile acids, no significant differences were observed between the two groups (p > 0.05). Tables S1/S2 summarize the comparison of liver function indicators between the two groups, and Figure 1 illustrates the comparison of liver function indicators between the RSA and control groups.

Comparison of liver function indicators between the two groups.
Multivariable logistic regression analysis: The relationship between liver function indicators and URSA
In this study, two multivariable logistic regression models were constructed to evaluate the association between liver function indicators and URSA. Model 1 included liver function indicators (ALT and AST) as continuous variables along with age, BMI, tobacco exposure, and gravidity. Model 2 replaced continuous ALT and AST with dichotomized abnormal indicators (ALT > 32 U/L, AST > 28 U/L) using the same covariates. Both models were fitted using Firth’s penalized likelihood method to address potential separation issues.
To assess dose–response patterns, ALT and AST levels were first analyzed as continuous variables. In Model 1, each 1-U/L increase in the ALT level was associated with a 3% increase in the URSA odds (aOR = 1.03, 95% CI: 1.02–1.04, p < 0.001), and each 1-U/L increase in the AST level was associated with a 2% increase (OR = 1.02, 95% CI: 1.01–1.03, p = 0.002). To examine potential nonlinear patterns, both enzymes were categorized into quartiles based on the distribution of the study population (Table 2). Using the lowest quartile as a reference, ALT levels showed a progressive risk increase: Q2 (10.96–19.44 U/L): OR = 2.03 (1.47–2.80); Q3 (19.44–28.05 U/L): OR = 2.06 (1.49–2.85); and Q4 (>28.05 U/L): OR = 3.90 (2.86–5.32); p for trend < 0.001. In contrast, AST levels plateaued after mild elevation: Q2 (15.73–27.30 U/L): OR = 1.77 (1.31–2.40); Q3 (27.30–37.32 U/L): OR = 1.87 (1.37–2.55); and Q4 (>37.32 U/L): OR = 1.87 (1.37–2.56); all p < 0.001, with the overall trend driven primarily by the Q1-to-Q2 increase.
Quartile analysis of ALT and AST levels in relation to URSA risk.

ALT: alanine aminotransferase; AST: aspartate aminotransferase; URSA: unexplained recurrent spontaneous abortion; OR: odds ratio; CI: confidence interval; Q1: quartile 1; Q2: quartile 2; Q3: quartile 3; Q4: quartile 4.
For clinical interpretability, we also analyzed liver enzyme abnormalities using dichotomized cutoff values. The results of Model 2 (liver enzyme abnormality model) showed that abnormal ALT levels (OR = 1.85, 95% CI: 1.32–2.59, p < 0.001), abnormal AST levels (OR = 1.58, 95% CI: 1.20–2.08, p = 0.001), BMI (OR = 1.14, 95% CI: 1.08–1.20, p < 0.001), tobacco exposure (OR = 5.57, 95% CI: 4.10–7.56, p < 0.001), and gravidity (OR = 1.38, 95% CI: 1.18–1.61, p < 0.001) were significantly associated with URSA risk (Figure 2, Table S3). Age was not significantly associated (p = 0.592). Firth-corrected estimates remained consistent (Table S4).

Multivariate logistic regression of risk factors for URSA presented as a forest plot. URSA: unexplained recurrent spontaneous abortion.
Interaction between liver function indicators and URSA risk
To assess whether the association between liver enzymes and URSA risk is modified by lifestyle factors, we tested for multiplicative interactions between ALT/AST and tobacco exposure as well as BMI in the logistic regression models.
A statistically significant interaction was observed between ALT level and tobacco exposure (p for interaction < 0.0001). This indicates that the strength of the association between ALT level and URSA risk differed significantly between women with and without tobacco exposure. To illustrate the clinical implication of this interaction, we calculated the odds ratios for URSA comparing participants with normal and elevated ALT levels, stratified by tobacco exposure status. Among women without tobacco exposure, elevated ALT levels were associated with an OR of 1.8 (95% CI: 1.2–2.7). In contrast, among women with tobacco exposure, elevated ALT levels were associated with a substantially greater OR of 5.2 (95% CI: 3.1–8.7). This pattern is visually presented in the interaction plot (Figure 3), which clearly shows that the positive slope between ALT level (as a continuous variable) and the predicted probability of URSA is steeper in the tobacco exposure group. No significant interaction was found between ALT levels and BMI (p for interaction = 0.179).

Interaction effects of ALT levels with tobacco exposure and BMI on URSA risk. (a) Interaction between ALT levels and tobacco exposure in relation to URSA risk; (b) Interaction between ALT levels and BMI in relation to URSA risk. Tobacco exposure was assessed as a binary variable; results regarding the intensity of exposure should be interpreted with caution. ALT: alanine aminotransferase; BMI: body mass index; URSA: unexplained recurrent spontaneous abortion.
Similarly, a significant multiplicative interaction was found between AST levels and tobacco exposure (p for interaction = 0.018) and between AST levels and BMI (p for interaction = 0.0049). The interaction plot (Figure 4) demonstrates that tobacco exposure also amplifies the association between AST levels and URSA risk. Furthermore, the positive relationship between AST and URSA risk was strengthened at higher BMIs.
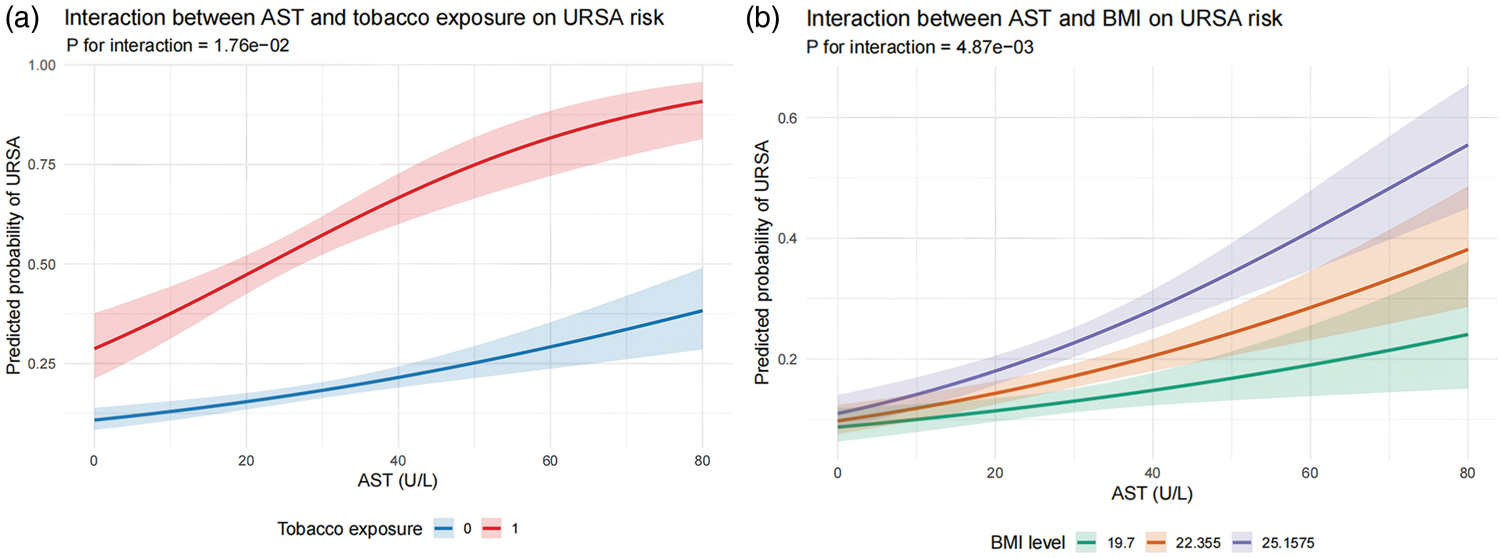
Interaction effects of AST levels with tobacco exposure and BMI on URSA risk. (a) Interaction between AST level and tobacco exposure in relation to URSA risk; (b) Interaction between AST levels and BMI in relation to URSA risk. Tobacco exposure was assessed as a binary variable; results regarding the intensity of exposure should be interpreted with caution. AST: aspartate aminotransferase; BMI: body mass index; URSA: unexplained recurrent spontaneous abortion.
Thus, our analysis using multiplicative interaction models revealed that tobacco exposure significantly modified the association of both ALT and AST levels with URSA risk, acting as an effect modifier that amplifies the risk associated with elevated liver enzymes. BMI plays a similar modifying role specifically with respect to AST levels. These findings underscore the necessity of considering lifestyle factors, particularly tobacco exposure, when evaluating liver function biomarkers in the context of URSA risk assessment. Although these multiplicative interactions are statistically significant, it is noteworthy that the binary classification of tobacco exposure (presence/absence) without accounting for exposure intensity suggests that these interaction effects should be interpreted with due caution.
Sensitivity analyses
We also focused on examining multicollinearity among liver enzyme indicators and performed corresponding model optimization to ensure the stability and accuracy of the final model. First, we calculated the Pearson correlation coefficients for the included liver function-related indicators (ALT, AST, GGT, ALP, TBIL, and bile acids levels). The overall correlations were weak, and no highly correlated variable pairs were detected (all |r| < 0.7). A correlation heatmap has been depicted in Figure 5 and Table S6.

Evaluation of collinearity and model stability using liver enzyme correlation and variance inflation factor (VIF) analysis. (a) The liver enzyme correlation heatmap displays the correlations between ALT, AST, GGT, ALP, total bilirubin, and bile acids levels; (b) VIF analysis chart presents the VIF values for each variable, assessing potential multicollinearity issues within the model. ALT: alanine aminotransferase; AST: aspartate aminotransferase; GGT: gamma-glutamyl transferase; ALP: alkaline phosphatase.
In the complete binary logistic model, which included ALT level, AST level, age, BMI, tobacco exposure, gravidity, age at menarche, and regular menstrual cycle, the VIF ranged from 1.02 to 1.21 (ALT level: 1.09, AST level: 1.21, BMI: 1.02, tobacco exposure: 1.18, gravidity: 1.11, age at menarche: 1.06, regular menstrual cycle: 1.12, age: 1.06). All VIF values were well below the commonly used thresholds (3 or 5), indicating that multicollinearity was minimal, and no further adjustments were necessary (Figure 5(b) and Table S7). Based on these findings, we retained the full model as the final model.
Thus, there was no evidence in favor of removing or combining variables due to multicollinearity in the current data. The final model was stable, with good interpretability and discrimination.
Discussion
This is the first large-scale, case–control study to investigate the association of liver enzyme abnormalities with URSA risk and their interaction with tobacco exposure. Our findings indicate that liver enzyme abnormalities, especially elevated ALT and AST levels, are independently associated with URSA risk. Furthermore, a significant interaction between liver dysfunction and tobacco exposure was observed. This discovery not only provides new insights into the etiology of URSA but also offers novel directions for risk assessment and clinical management.
The liver, as the metabolic hub of the body, plays a crucial role in maintaining pregnancy. We found a significant association between liver dysfunction, particularly the elevation of ALT and AST levels, and the occurrence of URSA. Traditionally, the liver is viewed as the core organ for metabolism and detoxification; however, its role in reproductive health, especially in pregnancy maintenance, has not been sufficiently explored. Our findings align with emerging research indicating that hepatic metabolic diseases, such as nonalcoholic fatty liver disease (NAFLD), are associated with an increased risk of adverse pregnancy outcomes, including gestational diabetes and preeclampsia.19,20 Elevated liver enzymes may reflect underlying subclinical liver inflammation or oxidative stress.21,22 This chronic low-grade inflammatory state could disrupt immune tolerance at the maternal–fetal interface through the release of pro-inflammatory cytokines (such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6)), impairing placental formation and function, which may ultimately lead to pregnancy loss.23–26 Additionally, liver dysfunction could impact hormone metabolism, leading to hormonal imbalances, 27 which in turn could affect endometrial receptivity and embryo implantation. Therefore, the liver may act as a critical link between metabolic health and reproductive failure.
An especially novel and important finding is the significant interaction between liver dysfunction and tobacco exposure. This suggests that individuals with both elevated liver enzymes and tobacco exposure exhibit a synergistically increased risk of URSA compared with those who have a single risk factor. Tobacco smoke contains numerous hepatotoxic compounds (such as nicotine and polycyclic aromatic hydrocarbons) that require metabolism via the cytochrome P450 enzyme system in the liver.28,29 This process may exacerbate the liver’s metabolic burden, inducing oxidative stress and inflammatory responses.30–33 When a liver already in a subclinical inflammatory state (indicated by elevated liver enzymes) is further exposed to tobacco as an external stressor, its function may decompensate rapidly, releasing additional inflammatory mediators and oxidative products, thereby intensifying the toxic environment for embryo implantation and fetal development. This finding emphasizes the importance of considering both endogenous physiological status and external environmental exposures when assessing the risk of URSA.
From a clinical perspective, our study holds dual significance. First, at the etiological level, it provides a potential explanation for some cases of URSA. In routine screening, patients without obvious anatomical, endocrine, immune, or genetic abnormalities are often diagnosed with URSA. Our study suggests that liver health should be regarded as a new, assessable risk dimension. Second, in terms of prevention and management, liver function markers (such as ALT and AST) are simple, cost-effective, and routinely tested clinical items. Incorporating these into the regular screening panel for URSA patients could help identify high-risk individuals. These findings suggest that for those with both elevated liver enzymes and tobacco exposure, smoking cessation and lifestyle modifications may be beneficial; however, this interpretation requires prospective validation and may provide new avenues for the development of personalized prevention and treatment of URSA.
Interaction analysis revealed complex relationships between ALT levels and tobacco exposure as well as ALT levels and BMI. Our results suggest that tobacco exposure significantly amplifies the association between ALT levels and URSA risk; among non-exposed women, elevated ALT levels were associated with an OR of 1.8, whereas among exposed women, the OR was 5.2, indicating that tobacco exposure may affect RSA occurrence by exacerbating hepatic oxidative stress and other mechanisms. In contrast, the interaction between BMI and ALT levels did not show statistical significance, which may be attributed to the limitations in BMI distribution within the data. To better understand the impact of BMI on liver function and URSA risk, future studies could further explore the potential biological mechanisms between BMI and liver function, particularly in populations with higher BMI, through broader sample data.
In this study, although some variables (such as age) did not show significant correlations in multivariable regression analysis (p = 0.5916), it does not imply that their influence can be disregarded. Age is a known risk factor for recurrent miscarriages, 34 and although it did not reach statistical significance in our current model, it has been considered a potential risk factor for RSA in other studies. Therefore, we suggest that future studies further explore the impact of age, in conjunction with other factors such as genetics and lifestyle, on RSA, and employ finer age stratification or subgroup analysis to reveal its potential effects. Additionally, despite the lack of statistical significance for some variables, they may still hold clinical relevance. For example, smoking exposure in our study demonstrated a significant impact, with an OR value of 5.57, indicating that smoking exposure is a strong risk factor for RSA and warrants special attention in clinical interventions.
Several important potential confounders were not available in our EMR data, including alcohol consumption, pre-existing NAFLD, and use of hepatotoxic or hormonal medications. These unmeasured factors may influence both liver enzyme levels and pregnancy outcomes, and residual confounding cannot be ruled out. Future prospective studies should collect detailed information on these variables to better isolate the association between liver enzyme abnormalities and URSA. Although our study had a sufficient sample size, we did not adequately discuss the representativeness of the sample. Specifically, it remains unclear whether the sample represents the broader pregnant female population. Factors such as race, region, age, and other socioeconomic factors could influence the external validity of our results. Future studies could consider validating our findings in multicenter, multiethnic populations to enhance the generalizability of the results. A notable limitation remains regarding the definition of tobacco exposure. The current binary classification combined active and passive exposure without quantitative assessments (e.g. intensity or duration), which may lead to exposure misclassification. Such misclassification can potentially bias the interaction findings. Therefore, although our statistical models show a significant synergistic effect, the results regarding the interaction between liver enzymes and tobacco exposure must be interpreted with appropriate caution. Future multicenter prospective studies should employ detailed quantitative metrics, such as pack-years for active smoking and specific exposure durations for passive smoking, to validate these findings and further clarify the underlying biological mechanisms.
Thus, this observational study suggests that liver enzyme abnormalities, especially elevated ALT and AST levels, are associated with URSA risk, and that tobacco exposure may amplify this association. Although the interaction findings require cautious interpretation due to measurement limitations, these findings may offer new perspectives for risk assessment and hypothesis generation. Future prospective studies are needed to confirm these observations.
Footnotes
Acknowledgments
The authors used DeepSeek (a large language model) for language polishing and grammar improvement. No AI tools were used for data analysis, interpretation, or scientific conclusions.
Author contributions
Xue Xiaolei designed the study, analyzed the data, and wrote the manuscript. Fang Congcong performed the statistical analyses and interpreted the data. Zhou Huan and Zhou Hanjing contributed to data collection. Li Wei and Lei Di contributed to study conceptualization and critical revision of the manuscript. All authors read and approved the final manuscript.
Consent to participate
The need for informed consent was waived by the Ethics Committee of Renmin Hospital of Wuhan University due to the retrospective design and the use of deidentified medical records.
Consent to publish
Not applicable.
Data availability statement
Data pertaining to this study will be made available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare that they have no competing interests.
Ethics approval
This study was approved by the Ethics Committee of Renmin Hospital of Wuhan University (Wuhan, China; approval No. WDRY2025-K015, dated 5 January 2025). The committee granted a waiver of informed consent due to the retrospective nature of the study. All study procedures were performed in accordance with the relevant guidelines and regulations, and the study was conducted in accordance with the Declaration of Helsinki (1975, revised in 2024).
Funding
This research was funded by NSFC Navigation Program of the Fifth Affiliated Hospital of Xinjiang Medical University (XYDWFY-GOH-2024-01-21) and Natural Science Foundation of Xinjiang Uygur Autonomous Region (2025D01C223).
Supplemental material
Supplemental material for this article is available online.