
Abstract
Objective
Emerging evidence suggests a potential role for soluble triggering receptor expressed on myeloid cells 2 (sTREM2) in cardiovascular pathophysiology. However, plasma sTREM2 levels in patients with acute decompensated heart failure and their possible association with adverse clinical outcomes have not been fully characterized.
Methods
In this retrospective cohort study, we enrolled patients with acute decompensated heart failure between 2020 and 2023 and defined a composite endpoint comprising all-cause mortality and heart failure–related readmission. Baseline plasma sTREM2 levels were compared across clinical categories and acute decompensated heart failure phenotypes using appropriate statistical tests. The prognostic value of sTREM2 was evaluated using Kaplan–Meier survival curves, restricted cubic splines, and Cox proportional hazards regression models. Model calibration was validated using bootstrap-corrected plots with 1000 resamples. Furthermore, time-dependent receiver operating characteristic curves, net reclassification improvement, and integrated discrimination improvement were used to assess the incremental predictive value of sTREM2 over N-terminal pro-B-type natriuretic peptide. Finally, subgroup analyses were performed to assess the robustness of the findings.
Results
A total of 128 patients (median age, 75.5 years) were enrolled, with 58 (45.3%) reaching the composite endpoint during follow-up. Plasma sTREM2 levels were significantly higher in patients with acute decompensated heart failure than in healthy controls (P < 0.001) and showed a progressive increase with worsening New York Heart Association functional class. Multivariable Cox regression analysis demonstrated that each 50 pg/mL increment in sTREM2 was independently associated with an increased risk of the composite endpoint (adjusted hazard ratio: 1.594; 95% confidence interval: 1.170–2.173) and heart failure–related readmission (adjusted hazard ratio: 1.802; 95% confidence interval: 1.310–2.480). Restricted cubic spline analysis confirmed a linear association between sTREM2 levels and clinical outcomes (all P for nonlinear > 0.05). Although adding sTREM2 to N-terminal pro-B-type natriuretic peptide did not significantly increase the area under the curve, it provided incremental predictive value for heart failure–related readmission. Subgroup analyses revealed no significant interactions (all P for interaction > 0.05).
Conclusion
Our findings demonstrate that sTREM2 is a potential biomarker in acute decompensated heart failure. Elevated sTREM2 levels are independently associated with an increased risk of adverse clinical outcomes, particularly heart failure–related readmission, underscoring its potential utility in risk stratification and clinical management of acute decompensated heart failure.
Keywords
Introduction
Over recent decades, the global incidence of heart failure (HF) has been rising. 1 Acute decompensated heart failure (ADHF), a clinical syndrome that includes both de novo HF and acute exacerbation of chronic HF, remains a major cause of emergency department visits and hospital admissions. Patients hospitalized with this condition experience risks of early readmission and other adverse post-discharge outcomes. 2 This clinical burden places significant burden on healthcare systems. 3 Although management strategies continue to evolve, early identification of patients at risk for readmission may improve long-term prognosis and optimize healthcare resource management. Current prognostic assessments rely on clinical indicators, including B-type natriuretic peptide (BNP) levels, hyponatremia, anemia, and changes in renal function.4,5 However, there is a lack of clinical tools specifically designed for managing ADHF. 6 These limitations in risk assessment indicate that more precise stratification protocols and personalized management strategies may improve ADHF care.7,8
sTREM2, the soluble form of triggering receptor expressed on myeloid cells 2 (TREM2), is generated through proteolytic cleavage of the extracellular domain and subsequently released into the systemic circulation. 9 Although extensive studies have focused on the role of sTREM2 in neurodegenerative diseases,10–12 emerging evidence suggests its potential involvement in cardiovascular pathophysiology. Elevated sTREM2 concentrations have been associated with atherosclerosis, 13 coronary artery disease, 14 and acute ischemic stroke. 15 These findings indicate a possible role for sTREM2 in cardiovascular disorders. We hypothesized that quantification of plasma sTREM2 levels may provide novel prognostic insights for patients with ADHF.
Methods
Study population
This study consecutively enrolled 158 patients diagnosed with ADHF at the China-Japan Friendship Hospital between November 2020 and December 2023. The diagnosis of ADHF was established according to the 2021 European Society of Cardiology (ESC) Guidelines. 16 Exclusion criteria were as follows: (a) active infection; (b) current or prior malignancy; and (c) end-stage hepatic or renal dysfunction. End-stage hepatic dysfunction was defined as Child–Pugh class C liver cirrhosis or advanced hepatic failure, whereas end-stage renal dysfunction was defined as chronic kidney disease (CKD) stage 5, characterized by an estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2. Following this screening process, 128 eligible participants were included in the final analysis. Additionally, 90 relatively healthy individuals were recruited from the health examination center of the same hospital to serve as a control group. Baseline data were systematically collected.
The reporting of this study adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 17 The study was conducted in accordance with the Declaration of Helsinki, as revised in 2024. The study protocol was approved by the Institutional Review Board of China-Japan Friendship Hospital (Approval Number: 2020-94-K58) in October 2020. To maintain participant confidentiality, all personal data were deidentified throughout the research process.
Sample collection and laboratory measurements
Standardized fasting peripheral blood samples were collected from all enrolled patients within 24 h of hospital admission. For the control group, fasting plasma samples were obtained from residual blood following routine clinical monitoring on the day of physical examination. Using aseptic techniques, 10 mL blood samples were drawn into lithium heparin vacutainer tubes and processed within 2 h of collection. Plasma was separated by centrifugation at 3000 ×g for 10 min at 4°C, and the resulting supernatant was aliquoted into 2 mL cryogenic vials. These aliquots were then stored at −80°C in a monitored ultra-low-temperature freezer until batch analysis. Plasma sTREM2 concentrations were quantified using a commercial enzyme-linked immunosorbent assay (ELISA) kit (Human sTREM2 ELISA Kit, Cusabio; Wuhan, China). All assays were performed by experienced laboratory technicians in accordance with the manufacturer’s instructions.
Follow-up and clinical endpoints
A comprehensive follow-up assessment conducted in March 2024 evaluated the clinical outcomes of all participants. Standardized telephone interviews were conducted and supplemented by a systematic review of hospital admission records. The observation period, starting at the time of discharge, had a median duration of 420 days (interquartile range (IQR): 227–1038 days). The composite endpoint of this study was defined as all-cause mortality and HF-related readmission.
Statistical analysis
Continuous variables were presented as mean ± SD or median (IQR), depending on their distribution, whereas categorical variables were expressed as frequencies and percentages. Between-group comparisons were performed using Student’s t-test, the Mann–Whitney U test, the chi-squared test, or one-way analysis of variance (ANOVA), as appropriate. For multigroup comparisons of sTREM2 levels across New York Heart Association (NYHA) functional classes, the Kruskal–Wallis test followed by Dunn’s post hoc test was employed. Spearman’s rank correlation was used to assess the association between sTREM2 and clinical biomarkers. To ensure robust statistical inference and adhere to the 10 events per variable (EPV) principle, covariates for regression were carefully selected. Multicollinearity was assessed using variance inflation factors (VIF), with all values <1.4 (range: 1.018–1.358), indicating no significant bias. Prognostic associations were evaluated using Cox proportional hazards models with two adjustment sets. Model 1 was adjusted for age, body mass index (BMI), left ventricular ejection fraction (LVEF), and NYHA class (dichotomized as II vs. III–IV). Model 2 was further adjusted N-terminal pro-B-type natriuretic peptide (NT-proBNP) and eGFR. Model calibration was assessed using bootstrap-corrected calibration plots (1000 resamples). Survival outcomes were compared between high- and low-sTREM2 groups (stratified by the median value of 179.6 pg/mL) using Kaplan–Meier curves and log-rank tests. Potential nonlinear relationships between sTREM2 and outcomes were examined using restricted cubic spline (RCS) regression. Prognostic performance was evaluated using time-dependent receiver operating characteristic (ROC) curves, with area under the curve (AUC) differences compared with NT-proBNP. The incremental value of sTREM2 was further quantified using net reclassification improvement (NRI) and integrated discrimination improvement (IDI). All analyses were conducted using R software (version 4.3.2) and Statistical Package for the Social Sciences (SPSS) (version 26.0), with a two-tailed P-value <0.05 considered statistically significant.
Results
Baseline characteristics
The final analytical cohort consisted of 128 patients diagnosed with ADHF (Figure 1). During the follow-up period, 58 patients (45.3%) reached the composite endpoint, including 6 all-cause mortality events, 50 HF-related readmissions, and 2 patients who experienced both outcomes.
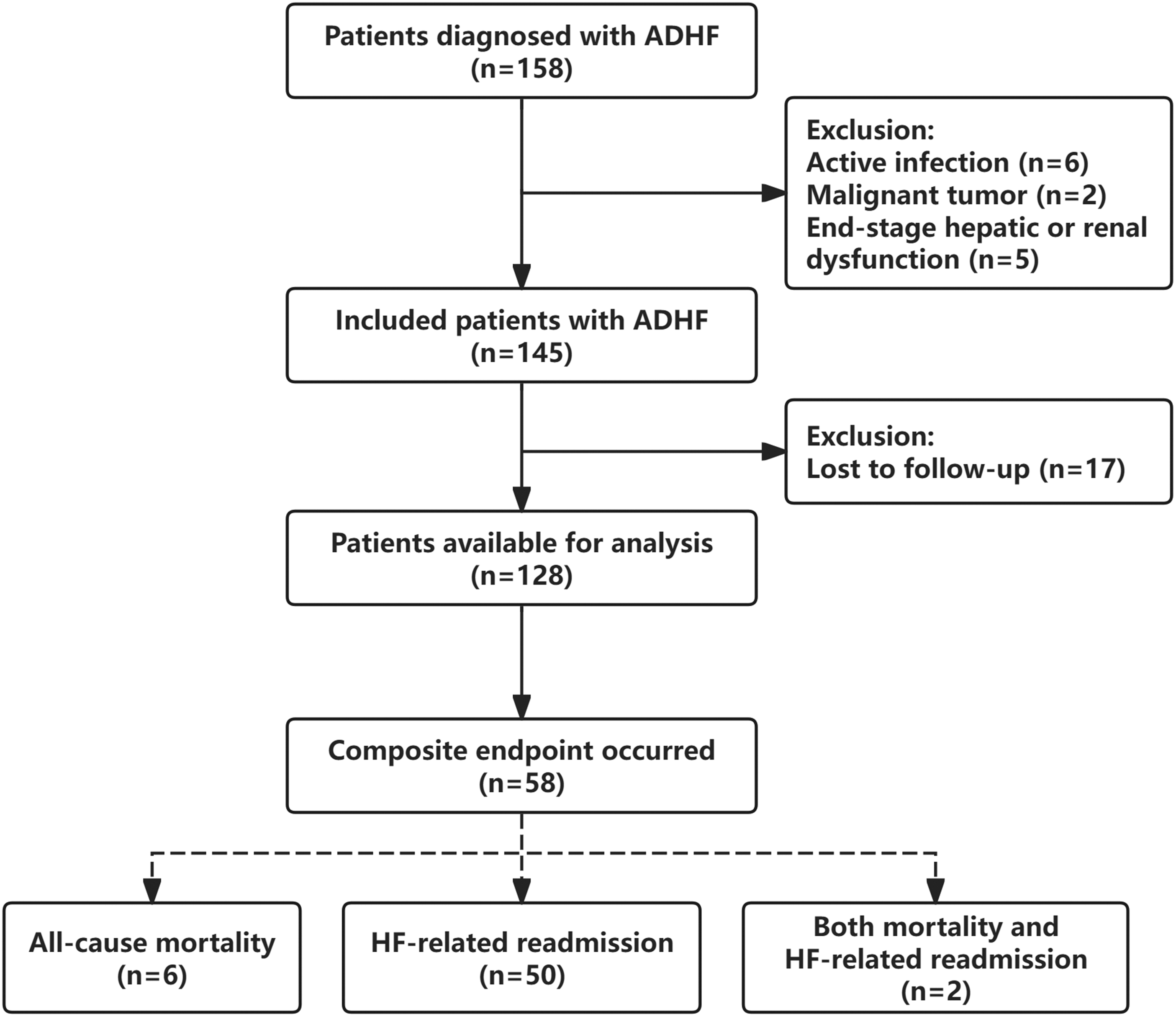
Flowchart illustrating the inclusion and exclusion of study participants. A total of 158 patients diagnosed with ADHF were screened. Of these, 13 patients were excluded based on pre-specified clinical criteria, and 17 were lost to follow-up. The final analysis cohort consisted of 128 patients. The composite endpoint (n = 58) included all-cause mortality and HF-related readmission. End-stage hepatic dysfunction was defined as Child–Pugh class C liver cirrhosis or advanced hepatic failure. End-stage renal dysfunction was defined as chronic kidney disease stage 5 (eGFR < 15 mL/min/1.73 m2). ADHF: acute decompensated heart failure; HF: heart failure; eGFR: estimated glomerular filtration rate.
As summarized in Table 1, the study population had a median age of 75.5 years (IQR: 64.0–83.0), with females comprising 37.5% of participants. Regarding HF phenotypes, 63.4% (n = 78) of patients were classified as having heart failure with preserved ejection fraction (HFpEF), whereas 36.6% (n = 45) had heart failure with reduced ejection fraction (HFrEF). Patients were stratified into two groups based on the median sTREM2 level (179.6 pg/mL): a low sTREM2 group (median, 135.6 pg/mL) and a high sTREM2 group (median, 206.1 pg/mL). Demographic characteristics, including age, sex, and BMI, were comparable between the two groups. However, patients in the high sTREM2 group tended to exhibit a more advanced NYHA functional class (P < 0.001) and a higher prevalence of HFrEF (P = 0.047) than those in the low sTREM2 group. Correspondingly, diuretic use was more frequent in the high sTREM2 group (P = 0.013). Biochemical profiling further indicated that the high sTREM2 group had elevated levels of NT-proBNP (P = 0.003), cardiac troponin T (cTnT; P = 0.004), and blood urea nitrogen (BUN; P = 0.036). No statistically significant differences were observed between the two groups regarding other laboratory measurements or echocardiographic parameters. Compared with the control group, patients with ADHF exhibited higher age, higher BMI, and elevated high-sensitivity C-reactive protein (hs-CRP) levels (all P < 0.001, Supplementary Table S1).
Baseline characteristics of the study population according to plasma sTREM2 levels.
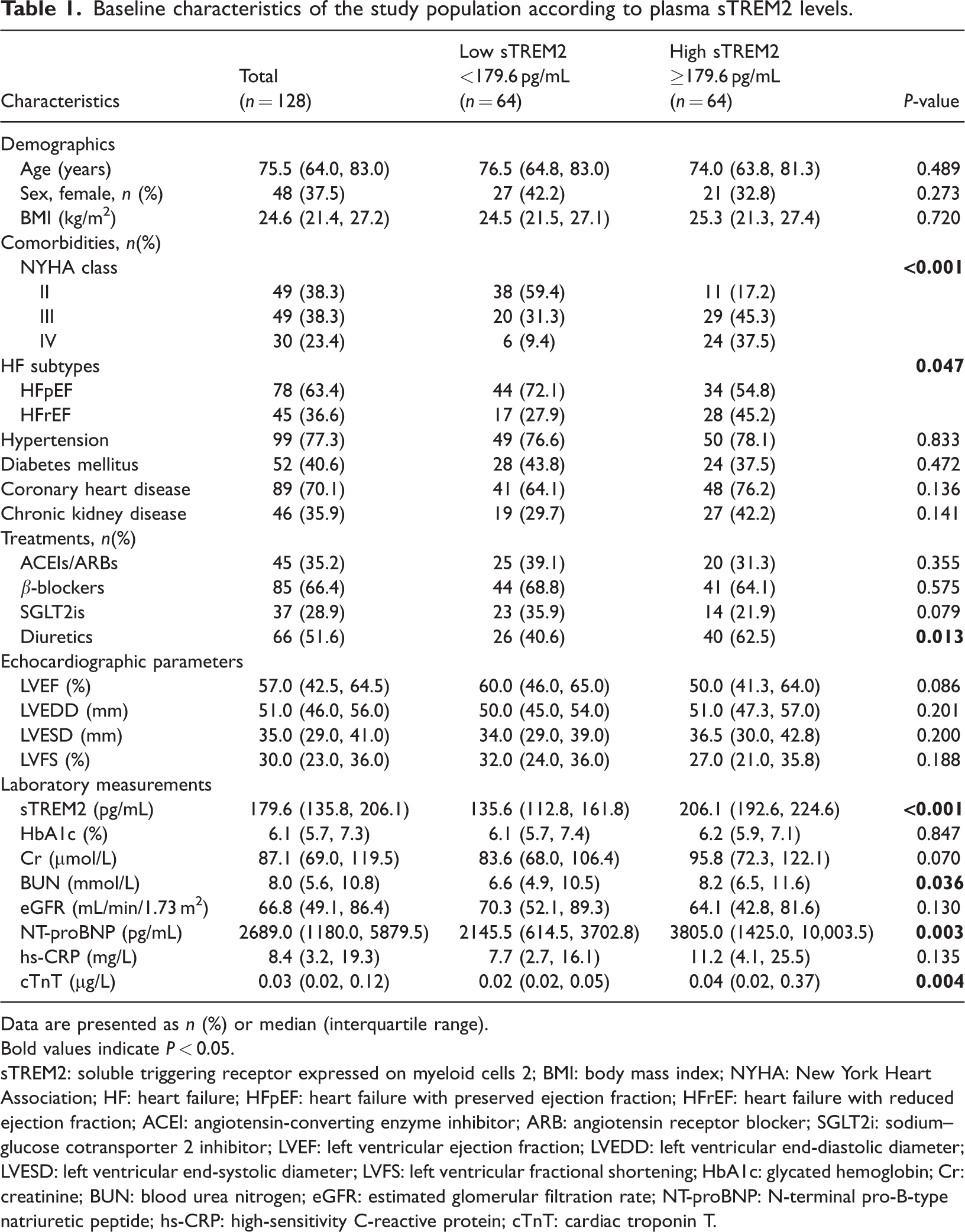
Data are presented as n (%) or median (interquartile range).
Bold values indicate P < 0.05.
sTREM2: soluble triggering receptor expressed on myeloid cells 2; BMI: body mass index; NYHA: New York Heart Association; HF: heart failure; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; SGLT2i: sodium–glucose cotransporter 2 inhibitor; LVEF: left ventricular ejection fraction; LVEDD: left ventricular end-diastolic diameter; LVESD: left ventricular end-systolic diameter; LVFS: left ventricular fractional shortening; HbA1c: glycated hemoglobin; Cr: creatinine; BUN: blood urea nitrogen; eGFR: estimated glomerular filtration rate; NT-proBNP: N-terminal pro-B-type natriuretic peptide; hs-CRP: high-sensitivity C-reactive protein; cTnT: cardiac troponin T.
Plasma sTREM2 levels across clinical categories and their correlation with biomarkers
Patients with ADHF exhibited significantly higher circulating sTREM2 levels than healthy controls (P < 0.0001, Figure 2(a)). Within the ADHF cohort, sTREM2 concentrations also tended to be higher in patients with HFrEF compared with those with HFpEF (P < 0.05, Figure 2(b)).
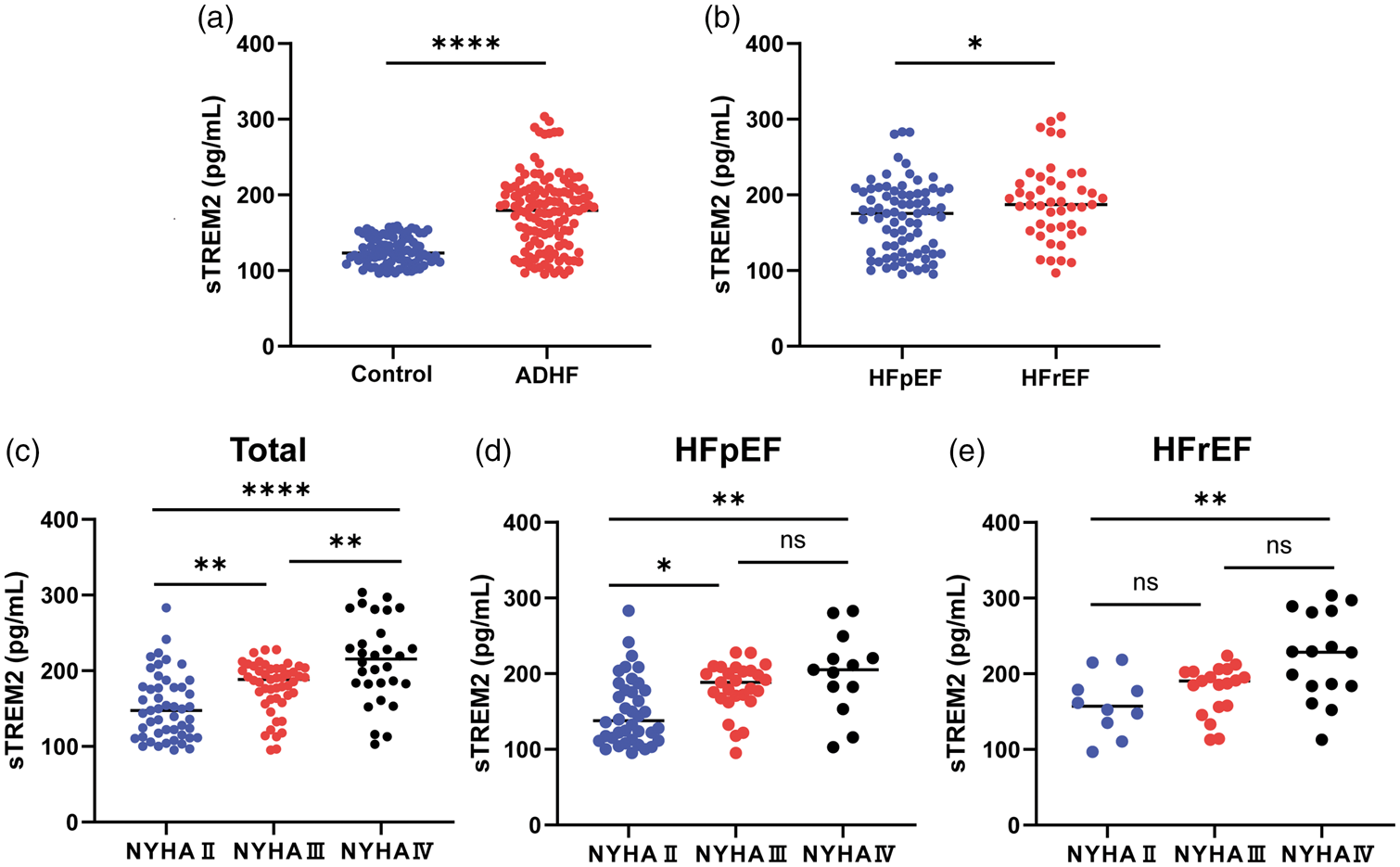
Plasma sTREM2 concentrations across different clinical categories and heart failure phenotypes. (a) Comparison of plasma sTREM2 levels between healthy controls and patients with ADHF; (b) distribution of plasma sTREM2 levels in patients with ADHF stratified by ejection fraction; (c) plasma sTREM2 levels according to NYHA functional classification (II, III, and IV) in the total ADHF cohort; (d and e) subgroup analysis of sTREM2 levels across NYHA classes within the HFpEF (d) and HFrEF (e) populations. Data are presented as scatter dot plots, with horizontal lines representing median values. *P < 0.05, **P < 0.01, ****P < 0.0001; ns, non-significant. sTREM2: soluble triggering receptor expressed on myeloid cells 2; ADHF: acute decompensated heart failure; HFpEF: heart failure with preserved ejection fraction; HFrEF: heart failure with reduced ejection fraction; NYHA: New York Heart Association functional classification.
Furthermore, a graded increase in sTREM2 concentrations was observed with advancing NYHA functional classes. This positive association between sTREM2 levels and clinical severity of HF symptoms remained consistent across the entire ADHF population as well as within the HFpEF and HFrEF subgroups (Figure 2(c) to (e)). These findings suggest that sTREM2 concentrations may be associated with the clinical severity of ADHF.
As illustrated in Supplementary Figure S1, plasma sTREM2 levels showed positive correlations with log2-transformed NT-proBNP (R = 0.249, P = 0.005), cTnT (R = 0.271, P = 0.002), and BUN (R = 0.186, P = 0.036). However, no significant association was observed between sTREM2 and hs-CRP levels (R = 0.121, P = 0.212).
Association between plasma sTREM2 and clinical outcomes
The potential associations between plasma sTREM2 levels and clinical outcomes were evaluated using Cox proportional hazards regression models (Table 2). In the unadjusted model, each 50 pg/mL increase in sTREM2 was associated with a higher risk of the composite endpoint (hazard ratio (HR): 1.552, 95% confidence interval (CI): 1.197–2.013, P < 0.001) and HF-related readmission (HR: 1.623, 95% CI: 1.233–2.136, P < 0.001). After adjusting for age, BMI, LVEF, NYHA class, NT-proBNP, and eGFR (Model 2), sTREM2 levels remained significantly associated with the composite endpoint (HR: 1.594, 95% CI: 1.170–2.173, P = 0.003) and HF-related readmission (HR: 1.802, 95% CI: 1.310–2.480, P < 0.001). Calibration analysis further confirmed that Model 2 demonstrated good predictive accuracy with a low risk of overfitting (Supplementary Figure S2).
Association between plasma sTREM2 levels and clinical outcomes in patients with ADHF.
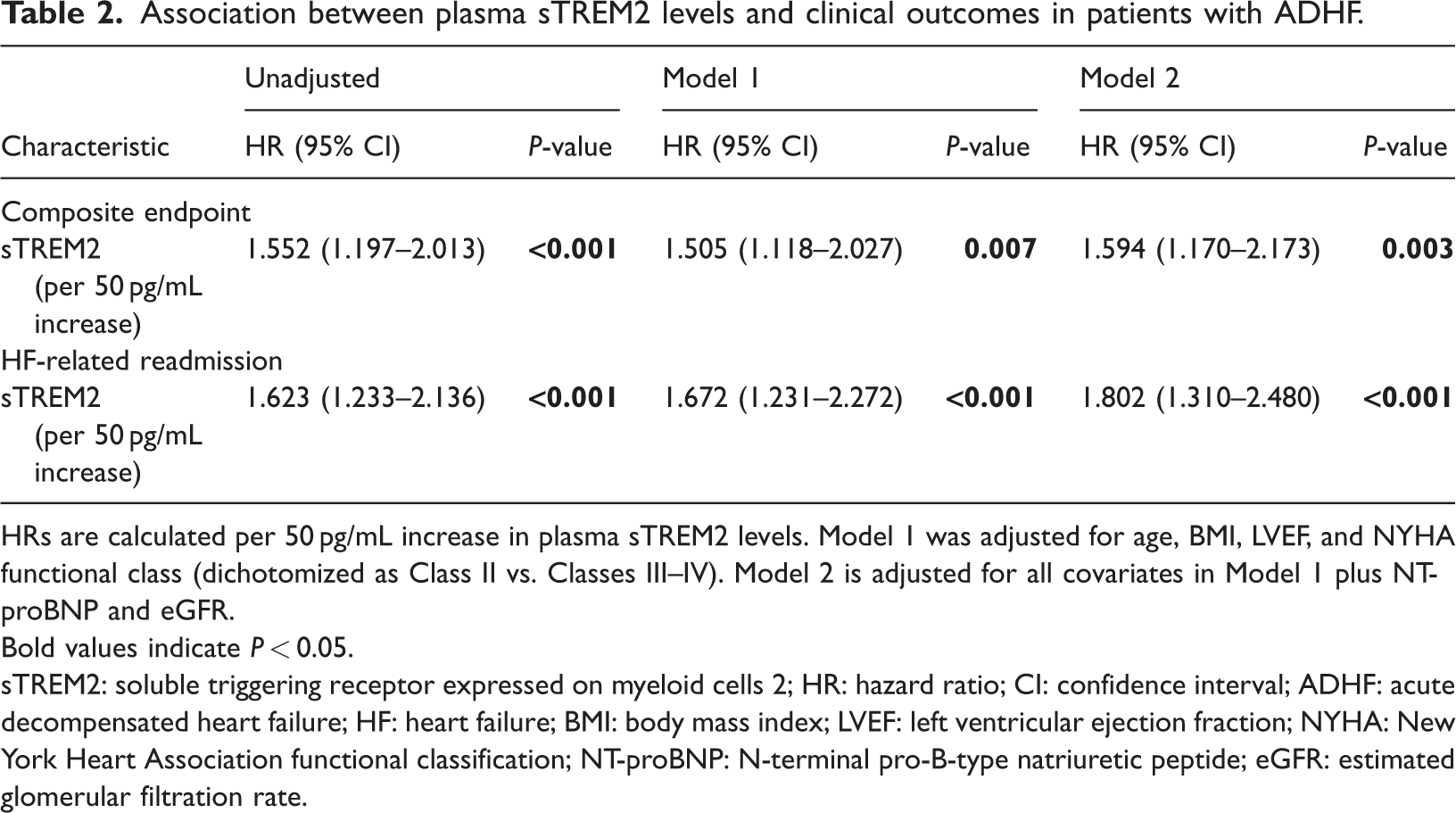
HRs are calculated per 50 pg/mL increase in plasma sTREM2 levels. Model 1 was adjusted for age, BMI, LVEF, and NYHA functional class (dichotomized as Class II vs. Classes III–IV). Model 2 is adjusted for all covariates in Model 1 plus NT-proBNP and eGFR.
Bold values indicate P < 0.05.
sTREM2: soluble triggering receptor expressed on myeloid cells 2; HR: hazard ratio; CI: confidence interval; ADHF: acute decompensated heart failure; HF: heart failure; BMI: body mass index; LVEF: left ventricular ejection fraction; NYHA: New York Heart Association functional classification; NT-proBNP: N-terminal pro-B-type natriuretic peptide; eGFR: estimated glomerular filtration rate.
Kaplan–Meier survival analysis indicated that the high sTREM2 group had lower event-free survival rates compared with the low sTREM2 group. These differences were statistically significant for both the composite endpoint (P = 0.024; Figure 3(a)) and HF-related readmission (P = 0.018; Figure 3(b)). Additionally, multivariable-adjusted RCS analysis suggested a linear relationship between sTREM2 levels and the risk of both the composite endpoint (P for nonlinearity = 0.325; Figure 3(c)) and HF-related readmission (P for nonlinearity =0.450; Figure 3(d)).

Relationship between plasma sTREM2 levels and clinical outcomes. (a and b) Unadjusted Kaplan–Meier survival curves of sTREM2 levels (stratified by the median) for (a) the composite endpoint and (b) HF-related readmission; (c and d) multivariable-adjusted restricted cubic spline analyses of sTREM2 for (c) the composite endpoint and (d) HF-related readmission, adjusted for age, BMI, LVEF, NYHA class (dichotomized as Class II vs. Classes III–IV), eGFR, and NT-proBNP. sTREM2: soluble triggering receptor expressed on myeloid cells 2; HF: heart failure; BMI: body mass index; LVEF: left ventricular ejection fraction; NYHA: New York Heart Association functional classification; eGFR: estimated glomerular filtration rate; NT-proBNP: N-terminal pro-B-type natriuretic peptide.
Prognostic performance and incremental value of sTREM2 for clinical outcomes
For predicting the composite endpoint, the AUC for NT-proBNP was 0.617, whereas the AUC for sTREM2 was 0.642. Although the combination of sTREM2 and NT-proBNP yielded a numerically higher AUC of 0.679, this increase was not statistically significant compared with NT-proBNP alone (P = 0.262; Supplementary Figure S3A). Similar results were observed for HF-related readmission, where the combined model achieved an AUC of 0.682 (Pvs. NT-proBNP =0.104; Supplementary Figure S3B).
For the composite endpoint, the addition of sTREM2 to Model 1 (comprising age, BMI, LVEF, and NYHA class) and Model 2 (which further included NT-proBNP and eGFR) resulted in a modest increase in AUC, with ΔAUC values of 0.059 (P = 0.171) and 0.070 (P = 0.062), respectively. Although these increments suggest a trend toward improved discrimination, the improvements in both NRI and IDI did not reach statistical significance for this endpoint (all P > 0.05). In contrast, sTREM2 demonstrated statistically significant incremental value for predicting HF-related readmission. Its incorporation into Model 1 significantly enhanced the AUC (ΔAUC = 0.114, P = 0.040), accompanied by improvements in reclassification (NRI = 0.546, P = 0.037) and discrimination (IDI = 0.097, P = 0.046). These robust improvements were maintained when sTREM2 was added to the comprehensive Model 2 (ΔAUC = 0.115, P = 0.026; NRI =0.416, P = 0.029; IDI = 0.102, P = 0.034). Overall, these data indicate that sTREM2 provides significant prognostic information specifically for HF-related readmission.
Subgroup analyses
Subgroup analyses are presented in Supplementary Figure S4. The association between sTREM2 (per 50 pg/mL increase) and clinical outcomes was generally consistent across all strata. No significant interactions were observed in any of the tested subgroups (Supplementary Figures S4A and S4B).
Discussion
This study evaluated the prognostic significance of plasma sTREM2 levels in patients with ADHF, yielding three primary findings. First, circulating sTREM2 levels were significantly elevated in patients with ADHF compared with healthy controls. Second, sTREM2 concentrations progressively increased with advancing NYHA functional class, suggesting a potential association between this biomarker and clinical disease severity. Third, after adjusting for established risk factors, elevated sTREM2 levels remained independently associated with adverse clinical outcomes, particularly HF-related readmission. These findings highlight the potential of sTREM2 as a valuable complementary biomarker for risk stratification in the acute clinical setting.
To the best of our knowledge, this study represents a preliminary effort to evaluate plasma sTREM2 levels in patients with ADHF and their potential association with adverse clinical outcomes. To account for significant differences in baseline age and BMI between groups, these variables were included as covariates in the multivariable Cox proportional hazards models (Model 1 and Model 2). The results demonstrated that the prognostic value of sTREM2 for both the composite endpoint and HF-related readmission remained independent of these baseline characteristics.
TREM2 is a transmembrane receptor involved in cell activation and phagocytosis. 18 It releases its soluble isoform, sTREM2, upon cleavage by ADAM proteases. 19 Recent studies suggest that sTREM2 may serve as a potential biomarker for atherosclerotic cardiovascular disease, 20 coronary heart disease, 14 and coronary microvascular dysfunction. 21 These findings indicate that the role of sTREM2 in the cardiovascular system warrants further investigation. In the context of HF, elevated plasma sTREM2 levels have been significantly associated with cognitive impairment in patients with chronic HF. 22 In our cohort, the median sTREM2 level was 179.6 pg/mL, which differs substantially from previous reports in chronic HF (16.6 ng/mL) 22 and HFpEF (35 ng/mL). 23 These discrepancies likely arise from differences in the assays used, highlighting the need for further standardization to enable direct comparisons across studies. 24 Additionally, we observed higher sTREM2 levels in HFrEF compared with HFpEF, possibly due to the more pronounced hemodynamic instability and systemic inflammation characteristic of acute decompensated HFrEF. 25 These factors may be associated with endothelial dysfunction, 26 which may further influence the shedding of sTREM2.
Our study identified positive correlations between plasma sTREM2 levels and established biomarkers, including NT-proBNP, cTnT, and BUN. Although NT-proBNP and cTnT are established biomarkers for the diagnosis of HF and myocardial injury,27–29 the correlation with BUN suggests possible renal involvement. Interestingly, the lack of a significant correlation between sTREM2 and hs-CRP indicates that sTREM2 may reflect the local myocardial microenvironment and macrophage activation rather than the overall systemic inflammatory burden.22,30 These findings underscore the potential clinical value of sTREM2 as a complementary biomarker for comprehensive assessment of ADHF.
Immune and inflammatory mechanisms play a significant role in the pathophysiology of acute HF. 31 Although inflammatory markers may be low in chronic HF, they typically surge during acute decompensation.32,33 These inflammatory profiles, assessed through routine peripheral blood testing, may provide a practical and valuable approach for risk stratification in this patient population. 34 Recent immune profiling has further identified TREM2 as a novel mediator in hypertensive HF models. 23 Based on previous experimental evidence, sTREM2 may interact with the NF-κB signaling pathway 35 or influence macrophage polarization, 20 theoretically exacerbating myocardial injury. Although these pathways provide a biologically plausible framework for our findings, they remain hypothesis-generating. Further mechanistic studies are essential to determine whether these pathological cascades are directly mediated by sTREM2 in the clinical setting of ADHF.
Several limitations of this study warrant consideration. First, the healthy control group, recruited from a physical examination center, differed significantly in age and BMI compared with the patients with ADHF due to practical constraints in enrollment. Although these variables were adjusted for in our multivariable models to mitigate potential confounding, this baseline imbalance may still introduce some degree of selection bias. Second, the single-center design and relatively modest sample size may limit the generalizability of our findings; therefore, further validation in larger, multicenter cohorts is essential to confirm these results. Finally, as serial plasma sTREM2 measurements were not performed, we were unable to evaluate the dynamic prognostic value of this biomarker or its fluctuations throughout the clinical course.
Conclusion
This exploratory study highlights the potential of plasma sTREM2 as a novel prognostic biomarker in patients with ADHF. Our findings demonstrate that elevated sTREM2 levels are independently associated with adverse clinical outcomes, particularly HF-related readmissions. Although these preliminary results require validation in larger, multicenter cohorts, they provide valuable insights that may contribute to the development of more refined risk stratification strategies for this complex clinical syndrome.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605261456984 - Supplemental material for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study
Supplemental material, sj-pdf-1-imr-10.1177_03000605261456984 for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study by Jie Li, Mengyu Wang, Jing Ma, Shuwen Zheng, Yinong Chen, Furong Yang, Yingying Xie, Wenjing Wu, Mengwen Yan, Peiran Yang, Zhenguo Zhai and Yihong Sun in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605261456984 - Supplemental material for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study
Supplemental material, sj-pdf-2-imr-10.1177_03000605261456984 for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study by Jie Li, Mengyu Wang, Jing Ma, Shuwen Zheng, Yinong Chen, Furong Yang, Yingying Xie, Wenjing Wu, Mengwen Yan, Peiran Yang, Zhenguo Zhai and Yihong Sun in Journal of International Medical Research
Supplemental Material
sj-pdf-3-imr-10.1177_03000605261456984 - Supplemental material for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study
Supplemental material, sj-pdf-3-imr-10.1177_03000605261456984 for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study by Jie Li, Mengyu Wang, Jing Ma, Shuwen Zheng, Yinong Chen, Furong Yang, Yingying Xie, Wenjing Wu, Mengwen Yan, Peiran Yang, Zhenguo Zhai and Yihong Sun in Journal of International Medical Research
Supplemental Material
sj-pdf-4-imr-10.1177_03000605261456984 - Supplemental material for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study
Supplemental material, sj-pdf-4-imr-10.1177_03000605261456984 for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study by Jie Li, Mengyu Wang, Jing Ma, Shuwen Zheng, Yinong Chen, Furong Yang, Yingying Xie, Wenjing Wu, Mengwen Yan, Peiran Yang, Zhenguo Zhai and Yihong Sun in Journal of International Medical Research
Supplemental Material
sj-pdf-5-imr-10.1177_03000605261456984 - Supplemental material for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study
Supplemental material, sj-pdf-5-imr-10.1177_03000605261456984 for Plasma soluble triggering receptor expressed on myeloid cells 2 levels and clinical outcomes in acute decompensated heart failure: A retrospective cohort study by Jie Li, Mengyu Wang, Jing Ma, Shuwen Zheng, Yinong Chen, Furong Yang, Yingying Xie, Wenjing Wu, Mengwen Yan, Peiran Yang, Zhenguo Zhai and Yihong Sun in Journal of International Medical Research
Footnotes
Acknowledgments
We are grateful to all the participants in the study as well as to the dedicated clinical and research teams and nursing staff.
Author contributions
Jie Li conceptualized and designed the study. Jing Ma and Shuwen Zheng performed data extraction and conducted the initial analysis. Mengyu Wang, Yinong Chen, and Furong Yang assisted in data cleaning, proofreading, and statistical analysis. Wenjing Wu and Mengwen Yan contributed to the preparation of the figures. Jie Li and Yingying Xie prepared the initial manuscript draft. Mengyu Wang, Peiran Yang, Zhenguo Zhai, and Yihong Sun participated in the critical revision of the manuscript for important intellectual content. All authors participated in editing, reviewing, and approving the final version of the manuscript.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declare no conflicts of interest in this work.
Funding
This study was funded by the National Science and Technology Major Project on Prevention and Treatment of Cancer, Cardiovascular and Cerebrovascular Diseases, Respiratory Diseases and Metabolic Diseases (2025ZD0546100); the National Natural Science Foundation of China (82270062); the Natural Science Foundation of Beijing (7242096); and the Non-Profit Central Research Institute Fund of the Chinese Academy of Medical Sciences (2021RC310016).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.