
Abstract
Objective
To describe individuals with differences in sex development presenting with a female phenotype and an absent uterus and identify specific diagnostic characteristics that improve diagnostic accuracy and optimize patient care.
Materials and Methods
This descriptive comparative study included retrospective and prospective clinical data collected between 2023 and 2025 at the Reproductive Medicine Center “Universe,” Tbilisi, Georgia. Among 233 individuals evaluated for primary amenorrhea, 26% with a female phenotype and an absent uterus who were evaluated for Complete Androgen Insensitivity Syndrome, Mayer–Rokitansky–Küster–Hauser syndrome, and ovotesticular disorder of sex development were included in the final sample. All participants underwent clinical, hormonal, genetic, and imaging assessment. Laparoscopy and histomorphological examination were performed when indicated.
Results
Mayer–Rokitansky–Küster–Hauser syndrome accounted for 57.4%, Complete Androgen Insensitivity Syndrome for 37.7%, and ovotesticular disorder of sex development for 4.9% of the cases. Complete Androgen Insensitivity Syndrome patients exhibited preserved breast development with absent or sparse pubic hair, whereas Mayer–Rokitansky–Küster–Hauser syndrome and ovotesticular disorder of sex development patients exhibited normal pubic hair and breast development. Vaginal length was shortest in patients with Mayer–Rokitansky–Küster–Hauser, intermediate in those with complete androgen insensitivity syndrome, and variable in patients with ovotesticular disorder of sex development. Complete Androgen Insensitivity syndrome patients demonstrated male-range testosterone levels; Mayer–Rokitansky–Küster–Hauser patients exhibited female-range hormone profiles, and ovotesticular disorder of sex development patients were observed to have nonspecific endocrine patterns. Ovotesticular disorder of sex development was confirmed histomorphologically.
Conclusion
An integrated diagnostic approach combining specific clinical features, hormonal profiles, imaging, karyotyping, and histomorphology enables accurate differentiation of Mayer–Rokitansky–Küster–Hauser, complete androgen insensitivity syndrome, and ovotesticular disorder of sex development.
Keywords
Introduction
Differences in sex development (DSD) encompass a heterogeneous group of congenital conditions characterized by discordance among chromosomal, gonadal, and phenotypic sex. These conditions result from variations in genetic, hormonal, and developmental factors, leading to atypical sexual differentiation.1–3
Individuals with DSD presenting with a female phenotype and absent uterus are often first identified during adolescence, primarily during clinical evaluation for primary amenorrhea (PA).4,5 This diagnosis can be emotionally and psychologically challenging, as affected individuals typically identify as female and have female secondary sexual characteristics but lack the corresponding internal genitalia. 6
Complete androgen insensitivity syndrome (CAIS), Mayer–Rokitansky–Küster–Hauser (MRKH) syndrome, and ovotesticular disorder of sex development (OT-DSD) are among the most common DSD conditions presenting with a female phenotype and absent uterus. Although these conditions share key clinical features, including a female external phenotype and uterine agenesis, they differ significantly in karyotype, developmental mechanisms, and hormonal profiles.3,7,8
CAIS
CAIS is a type of androgen insensitivity syndrome and is characterized by discordance between chromosomal and phenotypic sex.9,10 In CAIS, individuals with a male karyotype (46, XY) exhibit a female phenotype due to complete androgen receptor (AR) insensitivity despite male-range circulating androgen levels. Thus, individuals with CAIS develop female secondary sexual characteristics, including breast development and external female genitalia.9,11–13
Despite their female phenotype and female sex identity in most cases, individuals with CAIS lack internal female reproductive structures. This is due to the presence of functional testes, which secrete anti-Müllerian hormone (AMH), leading to Müllerian duct regression and, consequently, the absence of the uterus, cervix, and upper two-thirds of the vagina. Additionally, due to AR insensitivity, Wolffian duct differentiation is impaired, resulting in the absence of male internal genitalia. The testes are typically located intra-abdominally, within the inguinal canals, or in the labia majora.13–15
MRKH syndrome
MRKH syndrome is a disorder of sex development characterized by a normal female karyotype (46, XX) and female phenotype. Affected individuals have normally developed ovaries, which support the development of normal female secondary sexual characteristics. However, the defining feature of MRKH syndrome is defective Müllerian duct development, which results in the absence of the uterus, cervix, and upper two-thirds of the vagina. The exact cause of MRKH syndrome remains incompletely understood, with genetic and environmental factors likely contributing to its etiology.16–18
MRKH syndrome is classified into two types. Type 1 is characterized by variations in anatomy limited to the reproductive system, whereas Type 2 involves additional malformations in other organ systems.19,20
Ovotesticular disorder
Ovotesticular disorder is an extremely rare condition with wide clinical polymorphism and genetic variability. Affected individuals may present with a female, ambiguous, or male phenotype. In individuals with OT-DSD and a female phenotype, the uterus may be absent or present as remnants, and the vagina may be normally developed or exhibit vaginal atresia. Current evidence suggests that the etiology of OT-DSD is multifactorial and involves dysregulation of key genes responsible for sex determination and differentiation, resulting in the coexistence of both ovarian and testicular tissue. The phenotypic variability observed in OT-DSD reflects differences in the timing, distribution, and functional activity of these genetic and hormonal influences.21–23
In individuals with DSD presenting with a female phenotype and PA, the overlapping clinical features frequently pose significant diagnostic challenges, leading to delayed or incorrect diagnoses. Given the complexity of these conditions, accurate and timely diagnosis by a multidisciplinary team is essential to ensure appropriate clinical management and mitigate potential long-term complications, including an increased risk of gonadal malignancy in some cases.3,24 These challenges highlight the need for well-defined, differential diagnostic characteristics for standardized diagnostic criteria and management strategies, facilitating accurate differentiation among DSD types and optimizing patient care.
The aim of this study was to describe individuals with DSD presenting with a female phenotype and an absent uterus and identify specific diagnostic characteristics that improve diagnostic accuracy and optimize patient care.
Materials and methods
This study was a descriptive, comparative analysis based on clinical data collected both retrospectively and prospectively from patients evaluated between 2023 and 2025 at the Reproductive Medicine Center “Universe,” Tbilisi, Georgia. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 25
Among 233 individuals aged 16–41 years presenting with PA, 61 (26%) presented with a female phenotype, PA, and an absent uterus and were evaluated for MRKH syndrome, CAIS, and OT-DSD. This group comprised the final study sample. The remaining 172 (74%) individuals had other etiologies of PA and were excluded according to the exclusion criteria.
Inclusion criteria
Patients with a female phenotype, PA, and an absent uterus confirmed on pelvic ultrasound (US) and/or magnetic resonance imaging (MRI) were included.
Exclusion criteria
Individuals who exhibited any of the following were excluded: (a) Intersexual external genitalia; (b) short stature; (c) delayed pubertal development; (d) Tanner breast stage <3; (e) streak gonads and/or hypoplastic ovaries and uterus on US or MRI; (f) endocrine disorders, including pituitary hypogonadism, hyperprolactinemia, functional hypothalamic amenorrhea, severe hypothyroidism, uncontrolled diabetes mellitus, and congenital adrenal hyperplasia; and (g) use of sex steroid hormonal therapy prior to evaluation.
At study inclusion, participants underwent comprehensive diagnostic evaluation including medical, surgical, and family history taking; gynecologic examination; pelvic US; pelvic MRI (when indicated); hormonal evaluation; and karyotype assessment. A diagnostic laparoscopy with histomorphological assessment of the gonadal tissue and Müllerian remnants was performed for 11 participants with CAIS and 3 with OT-DSD, as clinically indicated.
Sexual maturation was assessed using the Tanner staging system (B1–B5 for breasts, P1–P5 for pubic hair, and Ax1–Ax5 for axillary hair) during standardized clinical examination.
The development of the labia majora and labia minora was assessed during gynecological examination. As no validated scoring system for labial development exists, the assessment was based on clinical appearance. Hypoplastic labia were defined as underdeveloped structures with reduced tissue volume, thin structure, diminished contour, and incomplete coverage of the vestibule, a pattern commonly seen in prepubertal girls.
Pelvic ultrasonography was performed using a Voluson E12 system (GE Healthcare; USA). Transvaginal US was performed for 10 sexually active participants, whereas transabdominal US was performed in 51 participants who had an underdeveloped vagina or were sexually inactive.
Pelvic MRI was performed when US findings were inconclusive or when further delineation of Müllerian structures and gonadal morphology was required. MRI was performed using a Siemens Vida 3 T system with T2-weighted coronal, sagittal, and axial sequences and T1-weighted fat-suppressed axial sequences.
Hormonal assays in the study group included measurement of follicle-stimulating hormone (FSH), luteinizing hormone (LH), total testosterone, and estradiol (E2) levels using enzyme-linked immunosorbent assay (ELISA) (Beckman Coulter, Irving, TX).
Cytogenetic testing was performed using G-banding of peripheral blood lymphocytes cultures to determine karyotype.
Statistical analyses were performed employing descriptive and comparative methods, using the Statistical Package for Social Sciences (SPSS) software (version 31). Continuous variables were summarized as mean ± SD and range values, as appropriate. Categorical variables were expressed as frequencies and percentages. Between-group comparisons for continuous variables were performed using the independent sample Student’s t test. Due to the small number of patients with OT-DSD, comparisons involving this group were interpreted with caution. A two-sided p-value <0.05 was considered statistically significant.
Ethics statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the Reproductive Medicine Center “Universe,” Tbilisi, Georgia (Approval Number: 1/1, Approval Date: 8 January 2023). Written informed consent was obtained from all adult participants and from the parents or legal guardians of adolescent participants prior to study inclusion. All data were anonymized to ensure participant confidentiality.
Results
Study group composition
Among 61 individuals presenting with a female phenotype, PA, and an absent uterus, the most frequent diagnosis was MRKH syndrome, observed in 35 patients (57.4%), followed by CAIS in 23 patients (37.7%), and OT-DSD in 3 patients (4.9%). Within the MRKH syndrome group, Type I accounted for 94.3% (n = 33) and Type II for 5.7% (n = 2).
Phenotype and stature
All participants demonstrated a female phenotype and overall feminine body habitus. Height differed across various groups. In patients with MRKH syndrome (n = 35), height ranged from 150 to 169 cm (mean 160.0 ± 4.95 cm). In those with CAIS (n = 23), height ranged from 163 to 180 cm (mean 172.2 ± 3.97 cm), and in patients with OT-DSD (n = 3), height was recorded at 164, 166, and 168 cm (mean 166.0 ± 2.0 cm). Between-group comparisons revealed that CAIS patients were significantly taller than those with MRKH syndrome (p < 0.001). The height of OT-DSD patients was significantly more than that of MRKH syndrome patients (p < 0.001) and lesser than that of CAIS patients. However, the comparison of the height between OT-DSD and CAIS patients did not yield statistically significant results (p = 0.091); this result should be interpreted with caution, given the small sample of OT-DSD patients (n = 3).
Breast development corresponded to advanced Tanner stages across groups. In patients with MRKH syndrome and OT-DSD, breast development was predominantly Tanner stage B4–B5, whereas patients with CAIS exhibited Tanner stage B4 breast development. Compared with patients with MRKH syndrome in whom areolar pigmentation and nipple morphology appeared typical for normal female development, CAIS participants exhibited pale areolae (n = 23, 100%) and inverted nipples (n = 9, 39%). Findings in OT-DSD patients were heterogeneous (pale areolae n = 1, 33.3%; inverted nipples n = 1, 33.3%).
Pubic hair intensity varied markedly across diagnoses. Patients with MRKH syndrome demonstrated a typical female pattern. Tanner stage P4 was observed in 7 patients (20%) and P5 in 28 patients (80%). In patients with CAIS, pubic hair was absent or sparse, corresponding to stages P1 in 19 patients (82.6%) and P2 in 4 patients (17.4%). In patients with OT-DSD, pubic hair was well-developed, corresponding to stages P4 in one patient (33.3%) and P5 in two patients (66.7%).
External genitalia were female-appearing in patients with MRKH syndrome and CAIS, without clitoromegaly. In patients with MRKH syndrome, the labia majora and minora were normally developed. In patients with CAIS, the labia minora were markedly hypoplastic, with typically developed labia majora. In patients with OT-DSD, both labia majora and minora were well-developed.
Vaginal length and sexual function
Probe-measured vaginal length differed across diagnostic groups. In MRKH syndrome participants, length ranged from 1 to 2 cm in 30 patients (85.7%), whereas 4 patients (11.4%) had a completely absent vaginal dimple, and one patient (2.9%) had a vaginal length of 3.5 cm. In CAIS participants, the vagina was short and blind-ending. Among sexually inactive participants, the vaginal length was 3–4 cm in 14 patients (60.9%), whereas in sexually active individuals it extended to 6–7 cm in 9 patients (39.1%). In OT-DSD patients, one patient (33.3%) had a vaginal length of 4 cm, one sexually active patient (33.3%) had a vaginal length of 6 cm, and one patient (33.3%) had no vaginal dimple or invagination.
Overall, vaginal length in this study group was shortest in those with MRKH syndrome, with longer lengths observed in sexually active patients with CAIS. Patients with OT-DSD showed heterogeneous findings. At the time of assessment, participants with MRKH syndrome were unable to participate in vaginal intercourse. In contrast, sexually active participants with CAIS and OT-DSD reported satisfactory sexual function.
Karyotype profile
Karyotyping demonstrated 46, XX in all participants with MRKH syndrome (n = 35, 100%) and 46, XY in all participants with CAIS (n = 23, 100%). Among OT-DSD patients, one exhibited a 46, XX karyotype (33.3%) and two demonstrated a 46, XY karyotype (66.7%).
Hormonal profile
MRKH syndrome
The total testosterone levels of most participants (n = 33, 94.3%) ranged from 0.22 to 0.5 ng/mL, values that were within the adult female reference interval (<0.6 ng/mL), whereas two patients (5.7%) showed borderline elevation in the levels (1.20 and 1.32 ng/mL).
FSH values ranged from 1.8 to 9.8 mIU/mL, within the adult female reference interval (1.8–11.0 mIU/mL), in all patients (n = 35, 100%).
LH values ranged from 4.4 to 8.5 mIU/mL in 33 patients (94.3%), falling within the adult female reference interval (1.1–8.7 mIU/mL). In two patients (5.7%) an isolated elevation was observed (22.9 and 25.0 mIU/mL).
E2 concentrations ranged from 39 to 132.5 pg/mL in all patients (n = 35), falling within the adult female reference interval (28.0–173.0 pg/mL).
CAIS
Total testosterone level ranged from 4.1 to 7.5 ng/mL in 15 patients (65.2%), falling within the adult male reference interval (3.5–8.6 ng/mL). However, 8 patients (34.8%) exhibited supraphysiologic levels (12.1–14.5 ng/mL).
FSH concentrations in 20 patients (86.7%) ranged from 2.5 to 9.6 mIU/mL and were within the adult male reference interval (1.0–14.0 mIU/mL). However, 3 patients (13.0%) exhibited values exceeding the upper limit (15.7–17.9 mIU/mL).
LH values ranged from 3.4 to 6.8 mIU/mL in 9 patients (39.1%) and were within the adult male reference interval (0.7–7.4 mIU/mL), whereas 14 patients (60.9%) demonstrated persistent elevations (12.5–36.8 mIU/mL).
E2 levels ranged from 45.0 to 78.2 pg/mL, exceeding typical adult male concentrations (10–40 pg/mL) and falling within the female early follicular range (28.0–173.0 pg/mL).
OT-DSD
The total testosterone level was mildly elevated in one patient with a 46, XY karyotype (33.3%) at 0.8 ng/mL, exceeding the female reference interval (<0.6 ng/mL), whereas the levels of the remaining two patients (66.7%) were within the normal range for women.
FSH levels ranged from 4.2 to 8.7 mIU/mL in all patients, falling within the adult female reference interval (1.8–11.0 mIU/mL).
LH elevation was observed in one patient (33.3%) at 40 mIU/mL, whereas the remaining two patients (66.7%) had values within the adult female range (4.5 IU/l, 7 IU/l).
E2 levels ranged from 31 to 45 pg/mL in all cases and were within the adult female reference interval.
Pelvic imaging findings
MRKH syndrome
Pelvic US and/or MRI confirmed complete uterine agenesis in all patients. Uterine remnants were identified in 33 patients (94.3%) without visualization of endometrial tissue. Notably, none of the patients with uterine rudiments reported cyclic pelvic pain.
Structurally normal ovaries were observed in all cases. Typical ovarian position was observed in 32 patients (91.4%), whereas 3 patients (8.6%) had ectopic ovaries at the level of the iliac crest.
Among these, two patients (5.7%) also exhibited renal anomalies (one case of unilateral renal agenesis and one case of renal ectopia). An isolated scoliosis was documented in one case (2.9%).
CAIS
The uterus was not visualized on US and/or MRI in any participant. Bilateral intra-abdominal gonads (undescended testes) were present in 15 patients (65.2%). In 8 patients (34.8%), gonads were asymmetrically positioned, with one intra-abdominal and the contralateral gonad located near the external inguinal ring or within the labia majora.
OT-DSD
Pelvic US and MRI revealed uterine remnants without a discernible endometrial cavity in all three patients. In the patient with a 46, XX karyotype, both gonads were orthotopically located within the pelvis at typical ovarian projection sites and contained follicle-like structures consistent with ovarian morphology. In the two patients with a 46, XY karyotype, one gonad in each demonstrated fluid inclusions.
Surgical management and histomorphology
CAIS
Diagnostic laparoscopy with gonadectomy was performed in 11 patients (47.8%) for intra-abdominally located gonads after completion of pubertal development. Histomorphology revealed testicular tissue without neoplasia in 10 patients (90.9%) and seminoma in one patient (9.1%), diagnosed at 19 years of age. Additionally, in a 41-year-old patient, excision of a gonad located within the labia majora revealed gonadoblastoma on histomorphological examination.
Following gonadectomy, out of the 11 patients, 10 received estrogen replacement therapy for maintenance of secondary sexual characteristics, bone health, and overall well-being; the patient with a seminoma was excluded from hormone therapy and was managed according to oncologic protocols.
OT-DSD
In both patients with 46, XY OT-DSD, laparoscopic evaluation followed by gonadectomy revealed testis on the right side, adjacent to a rudimentary fallopian tube with well-developed fimbrial structures. On the left side, an ovotestis was identified in both patients, which was also associated with a rudimentary fallopian tube. Histomorphological examination in both patients confirmed these findings. The right gonads contained hypoplastic testicular tissue with pronounced fibrosis, consistent with testicular dysgenesis. The left gonads demonstrated hypoplastic testicular tissue with ovarian structural elements and fibrotic changes, confirming the diagnosis of ovotestis. In addition, Müllerian duct remnants were identified as tubular structures lacking epithelial lining in both cases. All patients received estrogen therapy after the gonadectomy.
In the patient with 46, XX OT-DSD a diagnostic laparoscopy was performed because imaging suggested the presence of enlarged Müllerian remnants and atypical gonadal structures, requiring direct visualization and histological verification. During laparoscopy, a Müllerian remnant measuring approximately 2 cm was identified centrally, appearing as a fibrous cord continuous with bilateral Müllerian duct remnants. On the right side, the gonad had an atypical location, resembled an ovary, with visible small follicles, with hypoplastic fallopian tube. On the left side, a hypoplastic fallopian tube with recognizable ampulla and fimbria was observed together with a gonad containing small follicles. An extended biopsy of both gonads and Müllerian duct remnants was performed. Histomorphological examination demonstrated that the right gonad showed normal ovarian morphology, including stromal hyperplasia, a luteal cyst, and small follicles at different stages of development.
The left gonad contained both ovarian and testicular components, including small follicles, stromal hyperplasia, and small fragments of testicular tissue with tubular structures and polymorphic testicular stroma, confirming the diagnosis of ovotestis. Examination of the Müllerian remnants revealed fibrous tissue with smooth muscle fibers, whereas biopsy of the uterine remnant demonstrated small focal areas of endometrial tissue. No cellular atypia or malignancy was detected. Given the low oncologic risk, the presence of functional ovarian tissue, and the patient’s reproductive considerations, gonadectomy was deferred according to the patient's preference. Instead, neovaginal reconstruction was performed to enable sexual function. The patient remains under follow-up with periodic imaging, tumor marker monitoring, and fertility counseling.
Based on integrated clinical, laboratory, imaging, and histomorphological findings, specific distinct diagnostic characteristics were identified to differentiate MRKH syndrome, CAIS, and OT-DSD in individuals presenting with a female phenotype and absent uterus (Table 1).
Differential diagnostic characteristics of MRKH syndrome, CAIS, and OT-DSD in individuals with a female phenotype and an absent uterus.
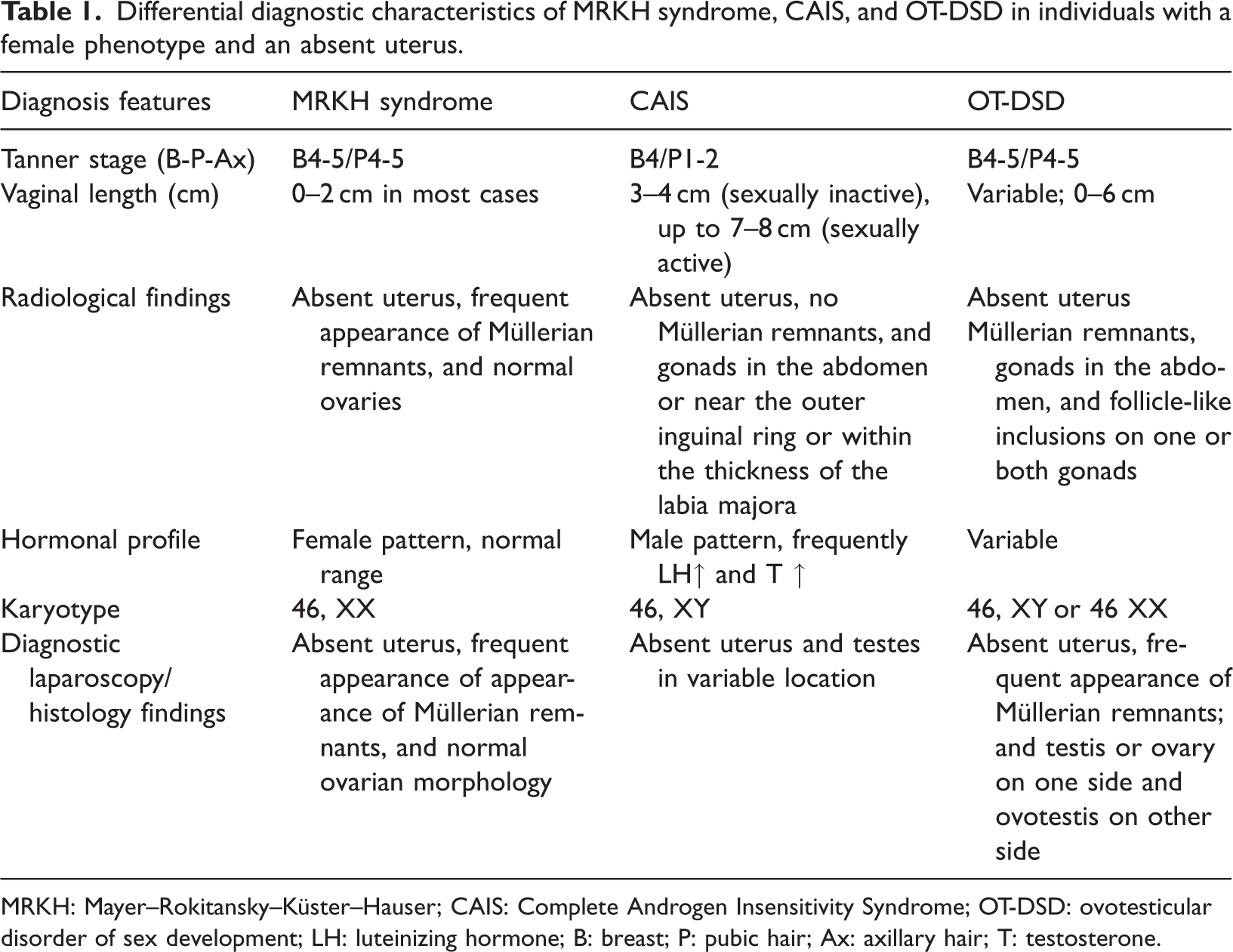
MRKH: Mayer–Rokitansky–Küster–Hauser; CAIS: Complete Androgen Insensitivity Syndrome; OT-DSD: ovotesticular disorder of sex development; LH: luteinizing hormone; B: breast; P: pubic hair; Ax: axillary hair; T: testosterone.
Discussion
Disorders of sex development presenting with a female phenotype, PA, and absent uterus include MRKH syndrome, CAIS, and OT-DSD. Although these conditions may share overlapping clinical features, they differ fundamentally in embryology, endocrine signatures, and karyotype, which are central to accurate diagnosis and counseling.3,24
Population-based estimates place MRKH syndrome at approximately 1 in 4500–5000 female births; CAIS at 1 in 20,000–100,000 46, XY births; and OT-DSD as markedly rarer (1 in 100,000 births).9,17,26 In our study group of individuals with a female phenotype, PA, and absent uterus, MRKH syndrome, predominantly Type I, was present in >50% of all cases, whereas CAIS, despite its rarity, accounted for nearly one-third of cases, consistent with published data.27,28
Phenotypic measures such as stature and secondary sexual characteristics helped discriminate diagnoses but require cautious interpretation. Height data in our study group mirrored literature expectations. MRKH syndrome patients demonstrated typical female stature, whereas CAIS patients had intermediate height, greater than the average for females but below those for males, reflecting complete androgen resistance despite a 46, XY karyotype and elevated androgen levels, with growth additionally influenced by Y-linked regulatory genes.13,17,29,30 OT-DSD cases exhibited variable stature, consistent with mixed gonadal influence.31,32 Given genetic and population variabilities, stature alone should not be used diagnostically.
In contrast, secondary sexual characteristics were more informative for differential diagnosis. In our study group, breast development was advanced in both MRKH syndrome and CAIS patients, reflecting functional ovarian estrogen production in MRKH syndrome and peripheral aromatization of androgens to estrogens in CAIS. Subtle qualitative differences, including nipple inversion and pale areolae in CAIS, may reflect tissue-level androgen insensitivity.13,15,17
Secondary sexual hair development provided one of the most reliable clinical discriminators. Patients with CAIS consistently exhibited sparse or absent pubic and axillary hair due to complete androgen resistance, whereas those with MRKH syndrome or OT-DSD generally demonstrated normal hair development.13,15,30 This feature represents a readily observable and clinically valuable diagnostic marker.
In distinguishing CAIS from 46, XY complete gonadal dysgenesis (Swyer syndrome), secondary sexual characteristics are particularly important. Unlike individuals with CAIS, patients with Swyer syndrome typically lack breast development due to nonfunctional streak gonads, whereas pubic and axillary hair development is usually present because of adrenal androgen production. 33
Vaginal length reflected embryologic development and further aided differentiation. In our study group, findings paralleled the literature, with MRKH syndrome patients exhibiting the shortest vaginal length, often 1–2 cm or absent and CAIS patients demonstrating a blind-ending vagina measuring 3–4 cm in sexually inactive individuals, which extended to 6–7 cm with sexual activity due to dilation.9,13–15,18,30,34 OT-DSD patients showed variable findings, reflecting gonadal heterogeneity. 32 These observations highlight the importance of accounting for sexual activity when interpreting vaginal measurements. Notably, MRKH syndrome patients unlike those with CAIS were unable to achieve vaginal intercourse, emphasizing the functional significance of these anatomic differences and the importance of individualized counseling on reconstructive or conservative management options.9,17
Hormonal assessment remains a cornerstone of DSD evaluation. In our study group, as in previous studies, endocrine profiles largely corresponded to the underlying chromosomal sex, limiting direct intergroup comparisons.3,4
In our CAIS study group, testosterone levels consistently fell within or exceeded the male reference range, reflecting intact testicular steroidogenesis and impaired AR–mediated feedback.13,35 Gonadotropin elevations, particularly LH, were frequently observed, consistent with compensatory pituitary stimulation.9,35 Isolated hormonal abnormalities, however, lacked diagnostic specificity.
Participants with MRKH syndrome demonstrated female-range sex steroids and gonadotropins, confirming preserved ovarian function despite Müllerian agenesis. Mild elevations in the total testosterone levels in two patients (5.7%) align with reported associations between MRKH syndrome and hyperandrogenism, including the potential involvement of WNT4 variants.17,36–38 OT-DSD endocrine profiles were heterogeneous, precluding the identification of a characteristic hormonal pattern. Notably, in OT-DSD patients with a 46, XY karyotype, total testosterone levels were within the female reference range in one case and mildly elevated in the other. These findings may be explained by the presence of hypoplastic testes, with severely expressed fibrosis, which likely resulted in reduced androgen production. This also explains the absence of virilization during puberty in these individuals. 32
Radiological evaluation plays a critical role in the differential diagnosis of DSD. Diagnostic challenges often arise when distinguishing an extremely hypoplastic uterus associated with gonadal dysgenesis from streak-like uterine remnants observed in MRKH syndrome. In such complex cases, ovarian morphology provides key discriminatory value. Gonadal dysgenesis typically presents with an extremely hypoplastic uterus and streak gonads, reflecting absent or severely impaired ovarian development, which is expressed by the incomplete development of secondary sexual characteristics. In contrast, MRKH syndrome is characterized by normal-sized, morphologically typical ovaries, consistent with preserved endocrine function and normal secondary sexual characteristics, along with an underdeveloped or absent uterus.39,40 Recognition of these radiologic and morphologic distinctions is essential for accurate diagnosis and management planning.
Our MRKH syndrome study group predominantly demonstrated functional ovaries. Although polycystic ovarian morphology has been described in MRKH syndrome, we did not observe this finding.17,40–42 Ectopic ovaries were identified in three patients at the level of the iliac crest, with associated renal anomalies in two patients. The relationship between ovarian ectopy and renal malformations remains insufficiently understood; however, our findings are consistent with limited reports in the literature.28,43 Recognition of normal ovarian morphology remains a critical diagnostic indicator.44,45
MRI remains the gold standard for gonadal localization and structural assessment in CAIS and OT-DSD and is particularly valuable in detecting fluid inclusions. 46 In our study group, MRI findings of gonadal fluid inclusions in a 46, XY patient with female-range hormones raised a suspicion for OT-DSD, which was subsequently confirmed using laparoscopy and histological analysis. Histomorphological examination remains the definitive diagnostic tool for OT-DSD.
Additionally, radiological identification of Müllerian remnants supports the diagnosis of OT-DSD, unlike for CAIS, where such structures are absent according to both our data and the literature. Furthermore, MRI does not always reveal fragments of the endometrial tissue in Müllerian remnants.32,47 Notably, in our study group, in OT-DSD patients, MRI failed to detect endometrial tissue within uterine remnants that were later identified using diagnostic laparoscopy. Histomorphological evaluation revealed small foci of the endometrial tissue, underscoring the limitations of imaging and reinforcing the importance of combined radiological and surgical–histologic assessment.
Our patients with OT-DSD and MRKH syndrome who exhibited uterine remnants did not report cyclic pelvic pain, suggesting incomplete or nonfunctional endometrial tissue. Nevertheless, the literature documents patients with MRKH syndrome who experienced cyclic pelvic pain and secondary endometriosis, likely resulting from functioning endometrial implants or obstructed Müllerian remnants. 48
In our study group, MRKH syndrome and CAIS demonstrated consistent 46, XX and 46, XY karyotypes, respectively, whereas OT-DSD showed marked karyotypic heterogeneity. In our study, two of the three patients with OT-DSD had a 46, XY karyotype, whereas one had a 46, XX karyotype. However, this distribution does not reflect the pattern reported in the literature, where 46, XX karyotype is more common among individuals with OT-DSD. The difference observed in our study group is most likely attributable to the very small number of OT-DSD cases included in the study. Therefore, karyotype interpretation must be integrated with clinical, hormonal, and imaging findings to establish diagnostic certainty.9,10,20,21,26,35,36
Oncologic risk remains a major management concern. Published estimates place germ-cell tumor risk in retained gonads in patients with CAIS at <1% during childhood, which increases up to 3.6%–33% during adulthood, with the highest risk for intra-abdominal gonads. Malignancy risk rises with age.9,49 Our series reflects this spectrum; one seminoma occurred in a 19-year-old patient with intra-abdominally located gonads, and one gonadoblastoma occurred in a 41-year-old patient with gonads located within the labium majus, despite the typically lower associated risk. 50 These findings underscore the importance of individualized counseling regarding the need for gonadectomy in CAIS and highlight importance of a vigilant long-term surveillance if the gonads are retained.
Although optimal timing of gonadectomy remains debated, most current recommendations support surgery after puberty to permit spontaneous pubertal development, with surveillance beginning at puberty. 51 Age-appropriate involvement of patients and families is essential for patient- and family-centered care. Hormone replacement therapy following gonadectomy is essential to maintain bone, cardiovascular, and sexual health.9,13,52
Thus, the integration of clinical, endocrine, radiologic, genetic, and histomorphologic data enables accurate differentiation of MRKH syndrome, CAIS, and OT-DSD in individuals with a female phenotype and absent uterus. Early and precise diagnosis is essential not only for guiding management and malignancy risk reduction but also for addressing sexual function, reproductive counseling, and long-term psychosocial well-being. Comprehensive management of DSD requires not only accurate diagnosis but also structured psychological evaluation and ongoing psychosocial support as integral components of multidisciplinary, patient-centered care.
Our specific diagnostic framework integrates multimodal data to streamline evaluation and shared decision-making; comprehensive counseling on sexual function and reproductive options remains a central component of care.
This study has certain limitations. First, advanced genetic investigations, including whole-exome sequencing, chromosomal microarray analysis, and targeted single-gene testing, were not available for all participants, which may have limited precise molecular characterization of the underlying disorders. In particular, molecular confirmation of CAIS through AR gene mutation analysis and measurement of dihydrotestosterone (DHT) levels were not performed in this study, which may limit diagnostic precision and raises the possibility of overlap with conditions such as 5α-reductase deficiency. Second, the number of patients with OT-DSD was small, reflecting the rarity of the condition and limiting subgroup analysis. Finally, the single-center design may have limited the generalizability of the findings.
Footnotes
Acknowledgments
The authors are grateful to the participants for their cooperation and thank the Shota Rustaveli National Science Foundation of Georgia for supporting this research.
Author contributions
Ana Jibladze conducted the study, performed data collection, managed software and resources, carried out the literature review, contributed to data interpretation, and drafted the manuscript. Elene Asanidze contributed to study design and methodology, data collection, data curation, analysis and interpretation, and manuscript writing and review. Alla Vash-Margita contributed to data analysis, supervised manuscript preparation, and participated in manuscript review and editing. Jenaro Kristesashvili conceptualized and designed the study, developed the methodology, supervised the research, contributed to data collection and analysis, and participated in manuscript writing, review, and editing. All authors critically revised the manuscript, approved the final version, and agree to be accountable for all aspects of the work.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request and with approval from the relevant ethics committee.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Ethics statement
This study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was reviewed and approved by the Ethics Committee of the Reproductive Medicine Center “Universe,” Tbilisi, Georgia (Approval No. 1/1, 8 January 2023). Written informed consent was obtained from all adult participants and from the parents or legal guardians of adolescent participants prior to study inclusion. All data were anonymized to ensure participant confidentiality.
Funding
This research (Grant Number: PHDF-24-1369) has been supported by Shota Rustaveli National Science Foundation of Georgia (SRNSFG).