
Abstract
The clinical management of a patient with adenomyosis in whom the levonorgestrel intrauterine release system was completely embedded in the myometrium is reported. The intrauterine device was located in the pelvis using qualitative imaging (plain abdominal X-ray, computed tomography, magnetic resonance imaging); localization (intraoperative ultrasound localization of the device within the myometrium of the anterior wall of the lower uterine segment); and definitive assessment (hysteroscopy to guide surgical manipulation and subsequent uterine suturing after removal of the device). The purpose of this article is to share our surgical procedure for removing an intrauterine device that has completely migrated into the myometrium using color Doppler ultrasound-guided hysteroscopy, thereby providing best practice for the management of complicated intrauterine device insertion and its prevention in clinical practice.
Keywords
Introduction
Adenomyosis (AM) is a common estrogen-dependent disease in women of childbearing age, characterized by invasion of endometrial glands and mesenchyme into the myometrium, with major clinical manifestations including heavy menstrual bleeding, progressive dysmenorrhea, and infertility. 1 The etiology and pathogenesis of adenomyosis remain unclear, and treatment options include pharmacologic, interventional, and surgical therapies, with hysterectomy considered the most effective treatment for adenomyosis. 2 As there is no curative pharmacologic therapy, nonsteroidal anti-inflammatory drugs, oral progestational agents, and gonadotropin-releasing hormone-a may be used for patients with mild symptoms, fertility preservation needs, or perimenopausal status; however, attention should be paid to adverse effects and recurrence after discontinuation. Levonorgestrel intrauterine release system (LNG-IUS) is also an effective treatment option for adenomyosis and can directly inhibit endometrial hyperplasia and decrease prostaglandin synthesis, thereby relieving dysmenorrhea and heavy menstrual bleeding, with a long duration of action in vivo.3,4
However, some patients treated with LNG-IUS may experience spotting, weight gain, breast tenderness, insomnia, depression, and headache. 5 The risk of dislodgement, migration, and embedment is significantly increased in patients with an enlarged uterus (uterine cavity depth >9 cm). 6 Although displacement of the intrauterine device (IUD) into the myometrium or outside the uterine cavity is a rare but well-documented complication, its incidence varies depending on device type, insertion technique, and patient-related factors such as uterine malformation, uterine leiomyoma, and adenomyosis. 7 Nonetheless, cases of adenomyosis with complete embedding of the LNG-IUS in the myometrium are extremely rare, with an incidence of <0.3%. 8 Herein, we report the case of a patient with adenomyosis in whom the LNG-IUS was completely embedded in the myometrium, was removed under color Doppler ultrasound-guided hysteroscopy, and replaced with a new LNG-IUS.
Case report
The reporting of this study conforms to the Case Report (CARE) guidelines. 9
General information
The patient, a female in her early 40s, G2P2, with a history of relatively normal menstrual cycles and severe dysmenorrhea, had an LNG-IUS ring placed following high-intensity focused ultrasound (HIFU) treatment for adenomyosis in 2019. Vaginal ultrasonography (January 2025) showed a posteriorly positioned uterus with an upper–lower diameter of 8.3 cm, anterior–posterior diameter of 6.9 cm, and transverse diameter of 8.0 cm. The endometrium was centrally located with homogeneous echogenicity and a thickness of 0.7 cm (bilayer), while the myometrial wall showed heterogeneous echogenicity, with some areas demonstrating a lumpy appearance. No definite lesion was identified in the bilateral adnexal regions. Emergency plain abdominal radiography and abdominal computed tomography (CT) revealed high-density pelvic shadows, raising suspicion of IUD ectopia or myometrial embedding (Figure 1). In January 2025, the patient underwent an outpatient hysteroscopic removal attempt; however, the device was not visualized intraoperatively. The operator considered the possibility of extrauterine migration of the IUD into the pelvis. The patient was subsequently admitted to Suining Central Hospital for surgical removal.
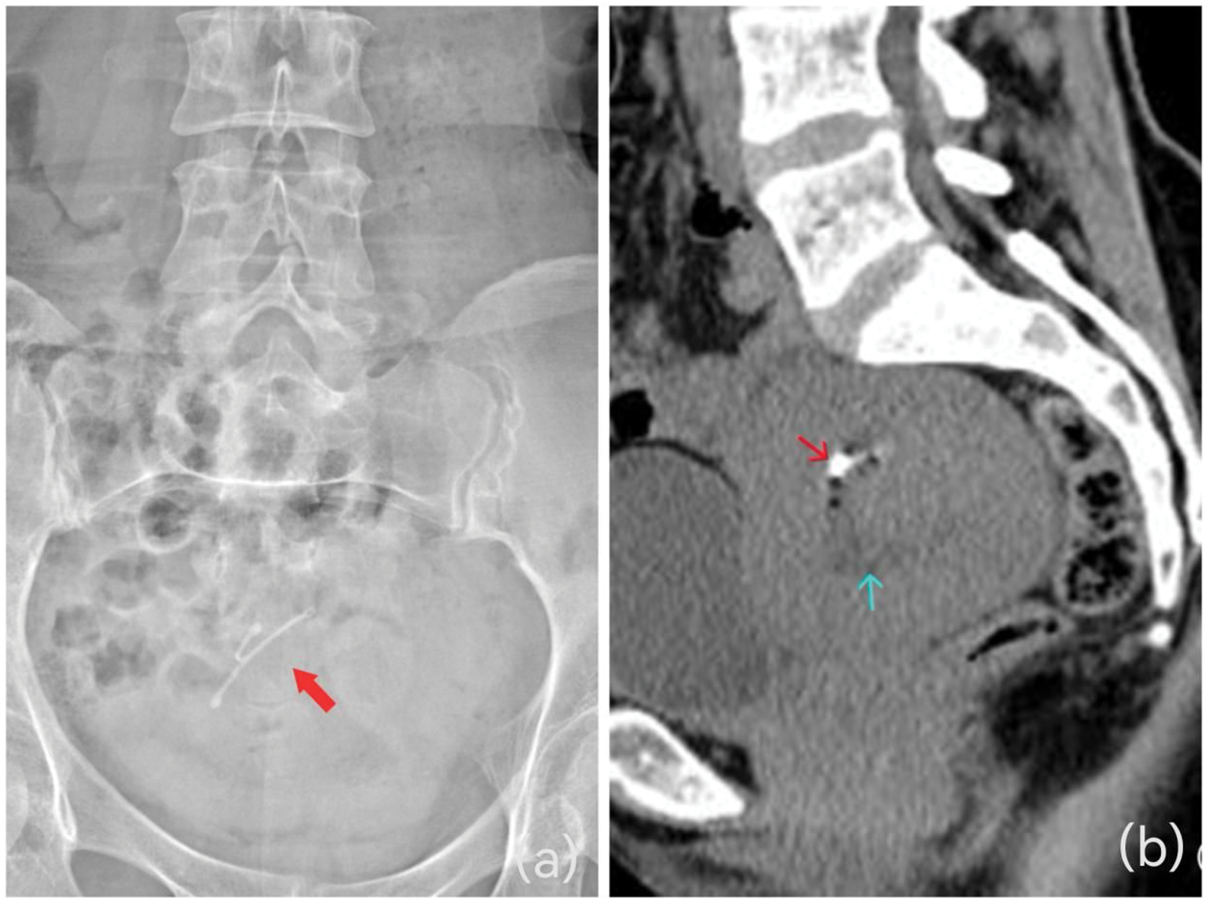
(a) The frontal plane view of the abdomen: the IUD is located in the pelvis; the red arrow indicates the IUD. (b) Noncontrast CT shows the IUD (red arrow, appearing hyperdense on sagittal noncontrast CT) within the myometrium, and the uterine cavity (blue arrow) appears hypodense. CT: computed tomography; IUD: intrauterine device.
Treatment process
The patient completed relevant preoperative examinations and had clear surgical indications with no contraindications for hysteroscopic retrieval of the IUD. The procedure was successfully completed in three main stages:
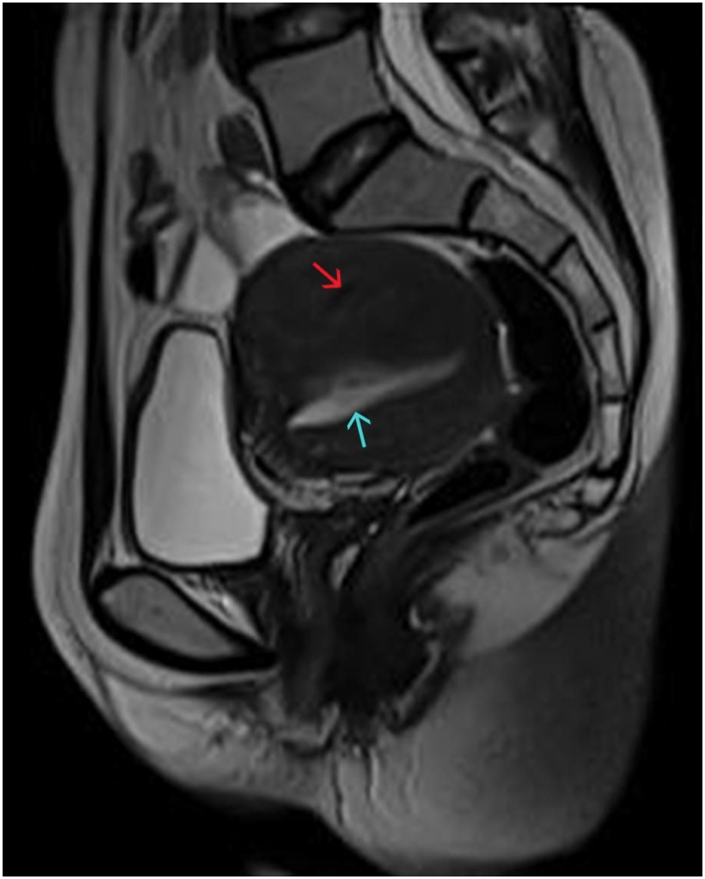
Pelvic magnetic resonance imaging shows the intrauterine device (red arrow), appearing hypointense on sagittal T2WI, within the myometrium, and the uterine cavity (blue arrow) appearing hyperintense on T2WI. T2WI: T2-weighted imaging.
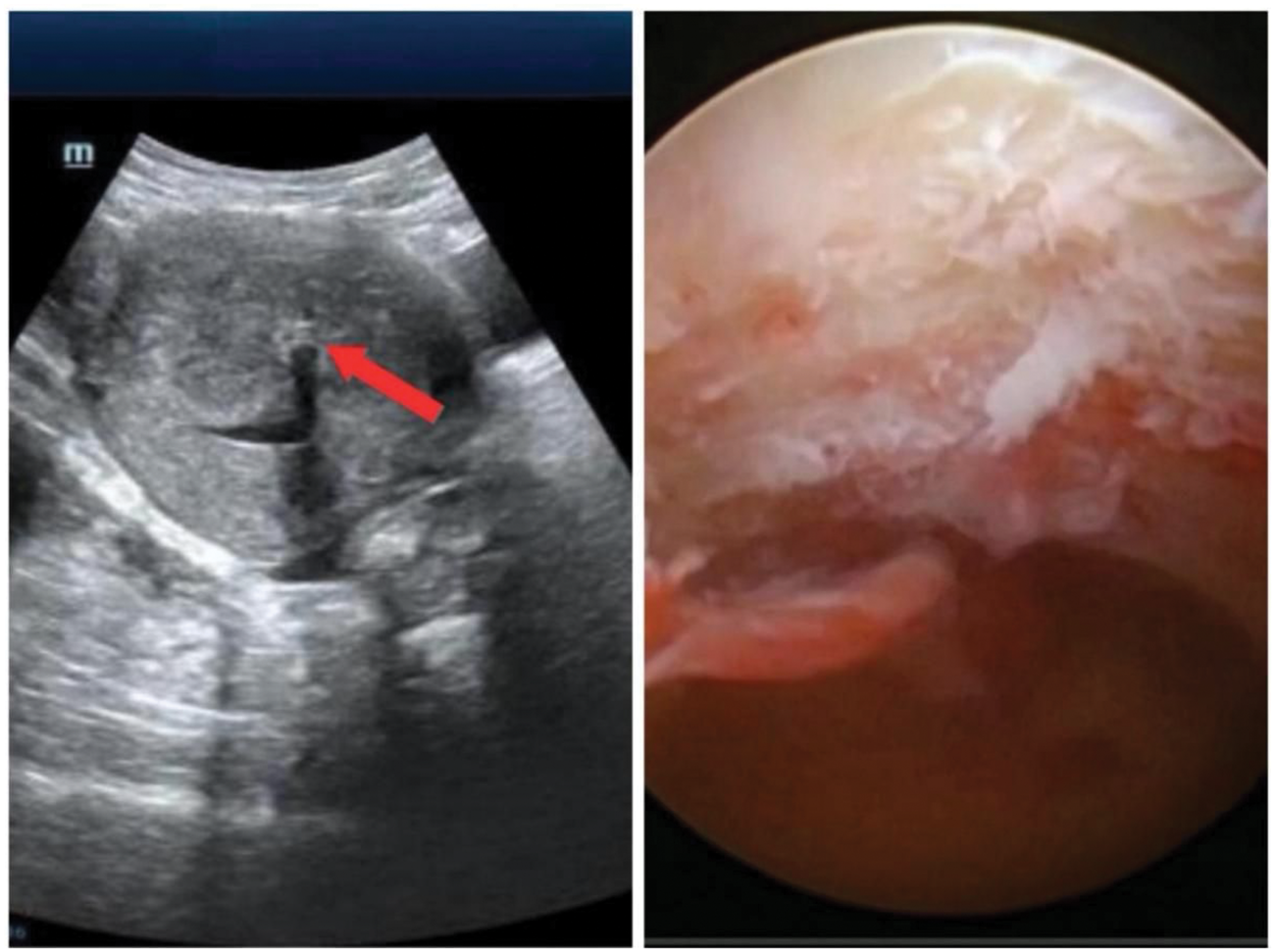
Intraoperative ultrasound localization. The IUD is located in the myometrium of the anterior uterine wall and the lower part of the uterine cavity, where fibrous encapsulation and inflammatory reactions can be observed. IUD: intrauterine device.
Specific key surgical steps
The surgeon first incised the scar-like tissue of the lower anterior uterine wall until the myometrium using scissors under hysteroscopy with color Doppler ultrasound guidance (Figure 4). A plasma electrosurgical loop was then used to longitudinally ablate the mucosal layer and superficial myometrium, exposing the proximal end of the IUD. The surrounding adherent tissue within approximately 1.3 cm of the myometrial layer was dissected to fully expose part of the device. The “Y”-shaped IUD was then grasped with the separating forceps and gently extracted toward the uterine cavity. After complete removal of the IUD, a new LNG-IUS was prepared by cutting the tail thread and securing the junction of the two arms and drug reservoir with 2-0 polyester nonabsorbable suture. One end of the suture needle was introduced into the uterine cavity under hysteroscopic guidance and grasped using a needle holder. The needle was passed through the myometrial layer at the posterior uterine fundus and then slowly retrieved through the cervix to draw the LNG-IUS into the uterine cavity. The suture was tied externally at the vaginal orifice, and a knot pusher was used to position the knot at the uterine cavity. The hysteroscope was reinserted to adjust the position of the suture knot to the bottom of the uterus, and 6–7 additional knots were tied in the same way. Each time a knot was tied, the hysteroscope was inserted and the position of the knot was adjusted to the bottom of the uterus. Finally, a new LNG-IUS was securely implanted and fixed to the posterior uterine wall.

(a) Under hysteroscopy, the scar-like tissue on the anterior wall of the lower uterine segment was slowly cut open with scissors to the myometrium. (b) The longitudinal resection of the uterine mucosa and the superficial myometrium was performed with the plasma electro-resection loop. A hard foreign body sensation was detected in the myometrium, and part of the IUD was gradually exposed. (c) The forceps were used to grasp the tail end of the IUD and slowly pull out a “Y”-shaped IUD toward the uterine cavity. (d) A new LNG-IUS ring was implanted and sutured to the posterior wall of the uterus. LNG-IUS: levonorgestrel intrauterine release system; IUD: intrauterine device.
The procedure was completed smoothly with an operative time of 25 min and intraoperative blood loss of 20 mL. Anesthesia was satisfactory, and the patient was discharged 4 h postoperatively.
Discussion
IUD embedment refers to partial or complete penetration of the IUD into the myometrium or even uterine wall penetration, which is one of the complications of IUD use. It may cause abdominal pain, irregular vaginal bleeding, reproductive tract inflammation, and, in severe cases, uterine perforation, with the probability of IUD-associated uterine perforation reported to be approximately 1.6/1000. 12 Commonly used IUDs include hormone-releasing devices (e.g. LNG-IUS ring) and copper-containing IUDs (Cu-IUD). The LNG-IUS ring is widely used as a safe and effective contraceptive method, used by 13.9% of the world’s 1.16 billion women of childbearing age, 13 and it also shows favorable efficacy in treating heavy menstrual bleeding and dysmenorrhea caused by adenomyosis as well as in preventing endometrial polyps. 14
Causes of IUD implantation
The occurrence of IUD embedment is associated with multiple factors, commonly including prolonged placement, mismatch between IUD type and size and uterine cavity, improper insertion, and development of inflammation. In the present case, the patient had adenomyosis with dysmenorrhea. According to Bourdon et al., 15 adenomyosis may induce a systemic or local inflammatory response, resulting in a disturbed immune environment in the endometrium and myometrium, accompanied by myometrial fibrosis and abnormal angiogenesis. This microenvironment may promote IUD embedment, which is consistent with intraoperative findings in this case. Additionally, the patient had undergone HIFU treatment prior to IUD placement, which may have induced localized tissue changes potentially contributing to subsequent IUD migration, although no direct causal relationship has been established in the literature. 16 Furthermore, multiple studies have shown that patients with adenomyosis have a higher risk of LNG-IUS expulsion and migration compared with the general population. Specifically, the reported expulsion rate is significantly elevated (15%–37.5%), whereas the rate in normal uteri is only 3%–10%.17,18 The possible reasons for this increased risk include disordered myometrial structure, abnormal uterine contractions, uterine cavity enlargement, and a chronic inflammatory microenvironment associated with adenomyosis, all of which may contribute to device displacement and embedment. 18 In addition, Gunardi et al. 19 reported a case of IUD loss in a patient with adenomyosis. Therefore, regular follow-up is recommended for patients with adenomyosis using IUDs to monitor device position and assess the risk of dislocation or misplacement.
Diagnosis of IUD insertion
For patients suspected of IUD embedment, a detailed history and comprehensive physical examination are essential. Ultrasonography is one of the most commonly used auxiliary diagnostic methods. However, for different types of IUDs—particularly the LNG-IUS ring—the T-shaped structure is composed of polyethylene and barium sulfate, making it impervious to radiation, and at the same time, the reservoir around the vertical stem is covered with a translucent silica gel (polydimethylsiloxane) film. The components of the LNG-IUS ring make ultrasound identification more challenging for LNG-IUS ring than for copper IUDs and often require careful identification by an experienced gynecologic ultrasonographer. 20 Moreover, there are limitations in embedding deep into the myometrium or even penetrating the serosal layer of the uterus into the pelvic tissues surrounding the uterus, which may require the use of radiographic imaging such as X-ray, CT, or MRI to characterize the presence of the ring, depth of the embedment, and severity of the embeddedness. 21
Methods of removing embedded IUDs
For embedded IUDs, appropriate methods should be selected based on the degree and location of embedment and the patient’s clinical condition. Partially embedded IUDs can usually be removed directly by conventional hysteroscopy. 22 However, for devices completely embedded in the myometrium or reaching the surface of the serosal membrane of the uterus, it is more difficult to remove it by simple hysteroscopy, and it is susceptible to complications such as uterine perforation and hemorrhage. Hysteroscopy combined with color Doppler ultrasound is a safe and effective method. Color Doppler ultrasound can monitor the operation process of hysteroscopy in real time, guide the removal instrument to reach the embedded site, avoid blind operation, and reduce the occurrence of complications. For IUDs that have migrated to the rectum, sigmoid colon, or bladder, alternative minimally invasive methods can be considered, such as removal under colonoscopy and cystoscopy.23,24 In cases of severe incarceration, high risk of perforation during IUD removal and migration to the peritoneum 25 or even to the bladder 26 should be considered for laparoscopic or open surgical removal. However, this type of surgery is more traumatic, and strict control of the indications is required. Conservative treatment may also be considered in a small number of asymptomatic patients. 27 Studies indicate that patients with adenomyosis have a higher incidence of LNG-IUS expulsion compared with the general population. 28 In addition, in the present case, given the depth of the patient’s uterine cavity, their previous 5-year placement of the LNG-IUS was effective in relieving the clinical symptoms. However, after 5 years, the ring was weakened and there was a need for reimplantation. Therefore, to avoid reimplantation, displacement, and dislodgement, the patient opted for nonabsorbable sutures to fix the LNG-IUS, thereby reducing the risk of device expulsion.
IUD insertion, ring removal, sharing
Before removing the ring, we need to determine the presence or absence of the ring, IUD type, and insertion details. Through qualitative analysis, the selection of tools and techniques can be targeted to reduce intraoperative complications. Accurate localization may require transvaginal ultrasonography combined with CT or MRI, which directly determines the choice of surgical procedures. For a shallowly embedded ring, hysteroscopy removal along the uterine curvature and device orientation may be required. For deeply embedded or perforating devices, ultrasound-guided hysteroscopic or laparoscopic surgery under direct visualization is recommended to avoid blind traction that may lead to uterine perforation or device rupture. 29 Finally, even when an appropriate surgical method is selected, suitable surgical instruments, such as metal rings, should be used flexibly and reasonably, or a lesser degree of incarceration should be prioritized for removal by cold hysteroscopic instruments (e.g. mini grasping forceps and scissors), which can avoid electrothermal damage and reduce the secondary damage caused by energy instruments to the myometrium. 30 When serious incarceration is found (e.g. ring breakage or penetration of the uterine wall) and when cold instruments are used in conjunction with energy instruments, the scope of action of energy instruments should be strictly controlled to avoid unintended conductive or thermal injury caused by contact with metal components. Alternative mechanical separation techniques, such as blunt dissection, may also be used. 31
Conclusion
For the removal of incarcerated IUDs, the diagnostic strategy of “characterization, localization, and method” can be followed. This approach is not only applicable to LNG-IUS rings but also to other types of IUDs (e.g. copper-containing metal devices). The specific procedure for IUD removal should be individualized according to the patient’s clinical condition.
Supplemental Material
sj-mp4-1-imr-10.1177_03000605261457785 - Supplemental material for A case report of removal and uterine suturing of an incarcerated intrauterine sterilization ring
Supplemental material, sj-mp4-1-imr-10.1177_03000605261457785 for A case report of removal and uterine suturing of an incarcerated intrauterine sterilization ring by Qingmei Wang, Zhuyang Liao, Ziyi Rao, Shuang Luo and Yanglu Liu in Journal of International Medical Research
Footnotes
Acknowledgments
We express our gratitude to the patient who kindly provided consent for this case to be presented in this report.
Data availability statement
The data supporting the findings of this study are included within the article and its supplementary materials.
Declaration of conflicting interests
The authors declare no conflict of interest.
Ethics statement and informed consent
Informed consent was obtained from the patient for publication of this case report and accompanying images. This report adheres to the Declaration of Helsinki, which emphasizes respect for participants’ rights, confidentiality, and informed consent. The institutional review board waived the requirement for ethical approval for this case report. All patient identifiers have been removed to ensure confidentiality.
Funding
This research received no external funding.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.